
Abstract
Purpose
Besides mortality, the patient-reported outcome (PRO) in survivors of multiple trauma is of increasing interest. So far, no data on patient-reported outcome measures (PROMs) after multiple trauma from an entire trauma network are available. Within this study, the course of the PRO over time and differences between level I and level II trauma centers within an entire trauma network was evaluated.
Methods
Multiple injured patients, treated in a rural trauma network over 2 years, were prospectively included in this study. After 6, 12 and 24 months the results of the European Quality of Life (EuroQoL) EQ-5D outcome instrument were evaluated. To adjust for differences in trauma severity between level I and level II centers, the Revised Injury Severity Classification II (RISC II) and the Functional Capacity Index (FCI) were used to adjust the life-quality results of patients.
Results
501 patients were included, 118 patients with an ISS < 16 points, 383 patients reached 16 points or more. Despite a steady increase of EQ-5D index over time (6 months: 0.71 ± 0.31; 12 months: 0.74 ± 0.28; 24 months: 0.76 ± 0.27; p < 0.001), the values of a reference population could not be reached even 2 years after trauma (EQ-5D reference population: 0.9). After adjustment for trauma severity, no significant differences in PROMs between level I and level II centers could be detected (p = 0.188).
Conclusion
The consistently low EQ-5D index relative the reference population and the lack of a difference between level I and II centers suggest that improved strategies for polytrauma aftercare are called for.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Purpose
Multiple trauma is one of the most common causes of death worldwide [1]. The continuous development of medical care and technical achievements has led to a significant reduction in trauma associated mortality over the past years in high income countries [2]. In this context, many countries established trauma networks to optimize the structural requirements in order to minimize mortality rates after trauma, especially in rural areas. A recently published study could show that mortality rates between level I and level II trauma centers within a rural trauma network are comparable [3]. Despite the reduction in mortality, survivors frequently suffer from physical, social and psychological sequels of trauma [4]. Therefore, the outcome after survived trauma, especially the patient-reported outcome (PRO) in survivors is of increasing interest. While many single-center studies show an initial, considerable deterioration of life quality compared to a reference-based population after trauma followed by a steady increase over time [4,5,6,7,8,9,10,11,12], no data concerning the PRO of an entire trauma network are available.
Within this article, we present the first results concerning the trauma-related quality of life of an entire trauma network. The goal of this study was to analyze data on PROs over time and to compare PRO results between level I and level II trauma centers.
Methods
Study design and study population
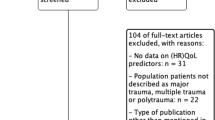
This was a longitudinal study that comprised a cohort of 2596 patients that were treated in the Trauma Network of Eastern Bavaria over a period of 24 months (01.03.2012–28.02.2014). This trauma network includes 25 hospitals (2 level I centers, 8 level II centers and 15 level III centers) [3]. In 585 patients the EuroQol-5 Dimension questionnaire could be collected prospectively after 6, 12 and 24 months [13]. Patients younger than 18 years and patients treated in a local trauma center (level III center) were excluded. In total 501 patients met the inclusion and exclusion criteria and were included into this study (Fig. 1).

Flowchart of case inclusion and exclusion
Data collection
Data of the quality management questionnaire of the TraumaRegister DGU® (40 parameters, www.traumaregister-dgu.de) were prospectively collected in each case. Next to the Abbreviated Injury Scale (AIS) [14], the Injury Severity Score (ISS) was assessed [15]. The RISC II, a tool to calculate the expected mortality in multiple injured patients, was used [16]. Additionally, the FCI, which reflects the expected levels of reduced functional capacity 1 year after injury depending on the injury pattern, was calculated [17]. Since differences in trauma severity between level I and level II centers within this network are known [3], RISC II and the lowest FCI values were used to adjust the life-quality results of the patients depending on the expected lethality and functional capacity. EQ-5D PROs were collected via a telephone interview between the study physician and the patient 6, 12 and 24 months after trauma.
Patient-reported outcome measures (PROMs)
The patient-related outcome and quality of life were assessed using interview version of the EuroQol-5D medical outcome score EQ-5D medical outcome score [13]. The EQ-5D consists of five questions concerning the following functional domains: mobility, self-care, everyday life activities, pain/discomfort and anxiety/depression [18]. These five items were transformed into individual health status profiles (range = 11111 [best] to 55555 [worst]) and then, using German norm data weights, converted into a single EQ index (range = − 0.21 [worst] to 1.00 [best]).
Funding and regulatory aspects
The Polytrauma Health Care Quality Outcome (POLYQUALY) Study (“Outcome after major trauma in a certified trauma network: comparing standard vs. maximum care facilities”) was funded by the German Federal Ministry of Education and Research in the context of a funding program on health services research (01GY1153).
The study was approved by the Ethics Committee of the University of Regensburg (number 10-101-0077). Written informed consent was obtained from all patients who participated in this study.
The study is registered in the data base of the German Network for Healthcare Research (VfD_Polyqualy_12_001978) and in the German Register for Clinical Studies (number DRKS00010039). The study protocol has been published [20].
Statistical analysis
Data are presented as mean (SD) for continuous variables and as absolute and relative frequencies for categorical data. Linear mixed models with patients as random factor were used to compare the EQ-5D index value over time and between groups (ISS < 16 vs ISS ≥ 16 and level I vs level II). The effect between level I and level II hospitals was further adjusted by RISC II and FCI with multiple linear regression models. For all models, estimated marginal means with corresponding 95% confidence intervals (95% CI) are presented as effect estimates. A p value < 0.05 was considered statistically significant. The results were compared with normative data from Germany [20]. All analyses were performed by using SAS 9.4 (SAS Institute, Cary NC) and IBM SPSS Statistics 22.0 (IBM Corp. Released 2013. IBM SPSS Statistics for Windows, Version 22.0. Armonk, NY: IBM Corp.). All graphics were created with SPSS Statistics 22.0 (IBM Corp. Released 2013. IBM SPSS Statistics for Windows, Version 22.0. Armonk, NY: IBM Corp.).
Results
Study population and demographics
In total 501 patients, who responded to the EQ-5D questionnaire at any of the three assessment points, were included into this prospective cohort study (Fig. 1). Demographic characteristics of all patients treated within the Trauma Network Eastern Bavaria (TNO) and patients included into this study are shown in Table 1.
Within the study group (n = 501) 118 patients showed an ISS < 16 points, while in 383 patients the ISS reached 16 points or more.
213 patients were treated in a level I center, 288 in a level II center with significant differences concerning age and FCI (p < 0.05) (Table 2).
EQ-5D: course over time
In total, 501 patients responded to EQ-5D questionnaire at any of the three assessment points. 458 patients completed the EQ-5D score 6 months after trauma (level I centers: n = 194; level II centers: n = 264), for 469 patients the EQ-5D questionnaire was available after 12 months (level I centers: n = 201; level II centers: n = 267) and for 427 patients after 24 months (level I centers: n = 183; level II centers: n = 244; Table 3). In 78% (389/501) all three measuring times were eligible for evaluation. Table 3 indicates that respondents with complete and incomplete follow-ups did not differ with regard to various measures of injury severity.
Overall, the EQ-5D index showed a steady increase over time (6 months: 0.71 ± 0.31; 12 months: 0.74 ± 0.28; 24 months: 0.76 ± 0.27). Nevertheless, the value of a healthy German reference population (EQ-5D index of 0.9) could not be reached, even 24 months after trauma (Fig. 2).

EQ-5D index value: course over time; *p < 0.001
EQ-5D: relation to injury severity
Patients with a high injury severity (ISS ≥ 16) showed significantly lower EQ-5D index scores at all 3 measurement points compared to patients with an ISS < 16 (Table 4). Nevertheless, in patients with high injury severity (ISS ≥ 16) a significant increase in life quality over time could be detected (p < 0.001), whereas the increase of the EQ-5D index in patients with lower injury severity (ISS < 16) was not significant (p = 0.348) (Fig. 3).

EQ-5D index value in relation to injury severity: ISS Injury Severity Score, *p < 0.001
EQ-5D: relation to the trauma level of the clinic
Life quality of severely injured patients (ISS ≥ 16: n = 383) was evaluated according to the trauma level of the clinic (level I center vs. level II center). Within these patients, 152 (40%) were treated in a level I center, 231 (60%) in a level II trauma center.
Regardless of differences in injury severity, patients treated in a level II trauma center showed significantly higher EQ-5D index values compared to those who were treated in a level I center at all 3 measurement times (p < 0.001) (Fig. 4). The mean 2-year EQ-5D index for patients treated in a level II center reached 0.72 ± 0.29 compared to 0.69 ± 0.32 in level I centers (p < 0.001). Looking at the subdimensions of EQ-5D 2 years after trauma, the patients showed limited results especially in mobility, everyday life activities and pain/discomfort. Comparing level I and level II trauma centers, significant differences regarding mobility, self-care and everyday life activities could be detected (p < 0.001) (Fig. 5).

Unadjusted EQ-5D index value of severe injured patients (ISS ≥ 16) in relation trauma level of the clinic; *p < 0.001

Subdimension of unadjusted EQ-5D of severe injured patients (ISS ≥ 16) after 24 months; *p < 0.001
Adjusted EQ-5D
To get further information about the PRO after severe trauma and differences between level I and level II centers within the same trauma network an adjustment is necessary to level different patient groups, especially concerning the injury severity. After adjustment, no significant differences in EQ-5D values could be detected at any time (Fig. 6). After adjustment, the 2-year EQ-5D index in a level I center was 0.71 (0.66–0.76) and in level II centers 0.75 (0.71–0.79) (p = 0.188).

Adjusted EQ-5D index value of severe injured patients (ISS ≥ 16) in relation to trauma level of the clinic: adjustment was performed using the RISC II and the FCI
The same analyses were conducted for EQ 5D-VAS and yielded comparable results (data not shown).
Discussion
The key findings of the present study are:
-
1.
Patients reported a considerably lower Quality of Life (QoL) compared to an age-matched reference population 2 years after trauma.
-
2.
Our results show an improvement in QoL over time, while patients with an ISS ≥ 16 are more impaired compared to those with a lower injury severity (ISS < 16), even 2 years after trauma.
-
3.
After adjustment, no significant differences in QoL between level I and level II trauma centers could be detected.
While previously published outcome studies after multiple trauma are single-center evaluations [4,5,6,7,8,9,10,11,12], an outstanding feature of the present investigation is the evaluation of an entire trauma network. Especially in rural areas, rather decentralized trauma networks with a large number of included hospitals (level I and level II) are necessary to ensure trauma treatment across a wide area. The trauma network evaluated in the present study is described in detail in a previous published investigation [3].
Regardless of injury severity, patients reported worse QoL compared to an age-matched reference population 2 years after trauma. We could find impairments after multiple trauma in all functional domains similar to previously published single-center studies [4, 10,11,12].
Our results show that injury severity influences the long-term functional outcome of the survivors. Patients with an ISS ≥ 16 are more impaired compared to those with a lower injury severity (ISS < 16), even 2 years after trauma.
While some studies did not observe any further improvement of QoL 6 months or 1 year after trauma [6, 11], our results show an improvement even after 2 years. This finding emphasizes the need for a good aftercare and proper long-term rehabilitation after completion of acute treatment, especially in severely injured patients.
In a previous study we could find equivalent results with regard to mortality rates between level I and level II centers within the evaluated trauma network [3]. Nevertheless, next to mortality rates, the QoL in survivors and potential differences depending on the trauma level of the clinic are of increasing interest. Within the present study 60% of the included severely injured patients were treated in level II centers. The overall QoL after 2 years is significantly higher in patients treated in level II centers compared to those treated in level I centers. However, there are significant differences in injury severity (ISS), expected mortality (RISC II) and the expected levels of reduced functional capacity (FCI). Therefore, an adjustment of the EQ-5D values, using the RISC II and the lowest FCI values, were performed to get comparable information about the QoL after trauma within the network.
After the adjustment, significant differences could not be detected anymore. Nevertheless, a trend towards superior PROs in level II centers could still be seen. Our findings complement the results of the previous study mentioned above, where the effectiveness and high functionality of the considered trauma network could be verified [3]. For the first time, the present study shows the possibility to evaluate the PRO of survivors after polytrauma within a multicenter study based on the Trauma Register DGU®.
Our study has several limitations. One limitation is the relatively low follow-up rate of 19.3%. We have to consider three reasons: (1) the high mortality rate (19%) in the patient sample under investigation; (2) the posttraumatic distress of the patients after severe trauma, and (3) the difficulty tracking of patients within the entire trauma network, which covers an area of about 20,000 km2 and has approximately 2.3 million inhabitants.
On the positive side, our total of patients included in the follow-up QoL assessments was n = 501, and thus markedly higher than sample sizes of previously published single-center studies, with study samples ranging from 53 to 397 patients [4,5,6,7,8,9,10,11,12]. Nevertheless, the results can only be applied to the entire trauma network to a limited extent, since the injury severity of the patients included differs significantly from that of the entire trauma network.
The present study used RISC II and FCI for the first time to adjust the quality of life of different injury severities. It has been shown that these adjusters can be used to assess quality of life after trauma, although further experience with these adjusters is still needed.
Overall the present study shows for the first time that within an entire working trauma network the PRO is comparable to previously published single-center studies. To compare the outcome of level I and level II centers an adjustment is necessary to level differences in patients’ and injury characteristics. After adjustment, no significant differences between level I and level II centers within the trauma network concerning the PRO could be detected. The next step should be the evaluation of the PRO within the entire TraumaRegister DGU®. Therefore, the TraumaRegister DGU® was recently expanded as part of a pilot project, to include a special category concerning outcome and quality of life. Therefore, further experience must be gained with regard to the adjustment of the quality of life.
Conclusion
Even though, patients showed an improvement in life quality 2 years after multiple trauma, the PROMs remained considerably lower compared to a reference population. No differences between level I and level II centers within a rural trauma network could be detected. Improved strategies for aftercare of polytraumatized patients are called for.
References
World Health Organization. The Global Burden of Disease: 2004 Update. 2008. http://www.who.int/healthinfo/global_burden_disease/2004_report_update/en/. Accessed 20 Jan 2019.
Ruchholtz S, Lefering R, Paffrath T, Oestern H-J, Neugebauer E, Nast-Kolb D, et al. Reduction in mortality of severely injured patients in Germany. Dtsch Arztebl Int. 2008;105:225–31.
Ernstberger A, Koller M, Zeman F, Kerschbaum M, Hilber F, Diepold E, et al. A trauma network with centralized and local health care structures: evaluating the effectiveness of the first certified Trauma Network of the German Society of Trauma Surgery. PloS one. 2018;13:e0194292.
Kaske S, Lefering R, Trentzsch H, Driessen A, Bouillon B, Maegele M, et al. Quality of life two years after severe trauma: a single-centre evaluation. Injury. 2014;45(Suppl 3):S100–5.
Ahmed W, Alwe R, Wade D. One-year functional outcomes following major trauma: experience of a UK level 1 major trauma centre. Clin Rehabil. 2017;31:1646–52.
Larsen P, Goethgen CB, Rasmussen S, Iyer AB, Elsoe R. One-year development of QOL following orthopaedic polytrauma: a prospective observational cohort study of 53 patients. Arch Orthop Trauma Surg. 2016;136:1539–46.
Marasco S, Lee G, Summerhayes R, Fitzgerald M, Bailey M. Quality of life after major trauma with multiple rib fractures. Injury. 2015;46:61–5.
Simmel S, Drisch S, Haag S, Bühren V. Long-term results after multiple trauma with ISS ≥ 25. Chirurg. 2013;84:771–9.
von Rüden C, Woltmann A, Röse M, Wurm S, Rüger M, Hierholzer C, et al. Outcome after severe multiple trauma: a retrospective analysis. J Trauma Manag Outcome. 2013;7:973.
Holtslag HR, van Beeck EF, Lindeman E, Leenen LPH. Determinants of long-term functional consequences after major trauma. J Trauma Inj Infect Crit Care. 2007;62:919–27.
Soberg HL, Bautz-Holter E, Roise O, Finset A. Long-term multidimensional functional consequences of severe multiple injuries two years after trauma: a prospective longitudinal cohort study. J Trauma Inj Infect Crit Care. 2007;62:461–70.
Dimopoulou I, Anthi A, Mastora Z, Theodorakopoulou M, Konstandinidis A, Evangelou E, et al. Health-related quality of life and disability in survivors of multiple trauma one year after intensive care unit discharge. Am J Phys Med Rehabil. 2004;83:171–6.
Brooks R. EuroQol: the current state of play. Health Policy. 1996;37:53–72.
States JD. The abbreviated and the comprehensive research injury scales. SAE Tech Paper. 1969. https://doi.org/10.4271/690810.
Baker SP, OʼNeill B, Haddon WJR, Long WB. The injury severity score. J Trauma Inj Infect Crit Care. 1974;14:187–96.
Lefering R, Huber-Wagner S, Nienaber U, Maegele M, Bouillon B. Update of the trauma risk adjustment model of the TraumaRegister DGU™: The Revised Injury Severity Classification, version II. Crit Care. 2014;18:476.
Palmer CS, Cameron PA, Gabbe BJ. A review of the revised Functional Capacity Index as a predictor of 12 month outcomes following injury. Injury. 2017;48:591–8.
Hinz A, Kohlmann T, Stöbel-Richter Y, Zenger M, Brähler E. The quality of life questionnaire EQ-5D-5L: psychometric properties and normative values for the general German population. Qual Life Res. 2013;23:443–7.
Koller M, Ernstberger A, Zeman F, Loss J, Nerlich M, Trauma Network Eastern Bavaria (TNO). Outcome after polytrauma in a certified trauma network: comparing standard vs. maximum care facilities concept of the study and study protocol (POLYQUALY). BMC Health Serv Res. 2016;16:242.
Szende A, Janssen B, Cabases J, editors. Self-reported population health: an international perspective based on EQ-5D. Dordrecht: Springer Netherlands; 2014.
Acknowledgements
The project is funded by a grant from the German Federal Ministry of Education and Research (reference number 01GY1153) in the context of the funding initiative Health Services Research. On behalf of the Trauma Network Eastern Bavaria (TNO): Klinikum Amberg, Dr. Bauer; Krankenhaus Bogen, Dr. Lehner; Krankenhaus Burglengenfeld, Dr. Cedl; Krankenhaus Cham, Dr. Walter; Klinikum Deggendorf, Prof. Schandelmaier; Krankenhaus Dingolfing, Dr. Maurer; Krankenhaus Eggenfelden, Prof. Wick; Krankenhaus Freyung, Dr. Barz; Krankenhaus Kelheim, Dr. Obermeier; Krankenhaus Landshut-Achdorf, PD Ganslmeier; Krankenhaus Marktredwitz, Dr. Bay, OA Hoffmann; Krankenhaus Mallersdorf, Dr. Mehlhorn; Klinikum Neumarkt, Dr. Schmickal; Klinikum Passau, Dr. Obernhuber; Klinik der Barmherzigen Brüder Regensburg, Prof. Füchtmeier; Krankenhaus St. Josef Regensburg, Prof. Nerlich; Krankenhaus Schwandorf, Dr. Schneider; Klinikum Straubing, Prof. Oedekoven; Krankenhaus Viechtach, Dr. Schäfer; Krankenhaus Vilsbiburg, Dr. Albersdörfer; Krankenhaus Vilshofen, Dr. Rieger; Krankenhaus Waldkrichen, Dr. Schmid; Klinikum Weiden, Dr. Neubaruer- Grartzke; Krankenhaus Zwiesel, Dr. Walter.
Funding
This study is part of the Polytrauma Health Care Quality Outcome (POLYQUALY) Study (“Outcome after major trauma in a certified trauma network: comparing standard vs. maximum care facilities”) and was funded by the German Federal Ministry of Education and Research in the context of a funding program on health services research (01GY1153).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
All the authors declare that they have no conflicts of interests.
Ethical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. The study was approved by the Ethics Committee of the University of Regensburg (number 10-101-0077). The study is registered in the data base of the German Network for Healthcare Research (VfD_Polyqualy_12_001978) and in the German Register for Clinical Studies (number DRKS00010039).
Informed consent
Informed consent was obtained from all individual participants included in the study.
Rights and permissions
About this article

Cite this article
Angerpointner, K., Ernstberger, A., Bosch, K. et al. Quality of life after multiple trauma: results from a patient cohort treated in a certified trauma network. Eur J Trauma Emerg Surg 47, 121–127 (2021). https://doi.org/10.1007/s00068-019-01160-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00068-019-01160-y