
Abstract
Purpose
To estimate the pooled PDRs (preventable death rates) with articles being published since 1990, and compare the differences of PDRs over time and according to the evaluation approaches to determine preventable deaths.
Methods
Articles concerning preventable deaths of trauma patients published between 1990 and 2013 were systematically reviewed, and the pooled PDRs with 95 % confidence intervals were estimated using meta-analysis. It was also observed whether the PDRs differed over time and according to the evaluation approaches employed for determining preventable deaths.
Results
Twenty seven articles were identified through bibliographic searches using PUBMED with the keywords of ‘preventable deaths’, ‘the cause of deaths’ and ‘trauma’. Mean ages of the trauma patients in the selected articles ranged from 32.9 to 58 years old and 72 % were male on average. The pooled PDR was estimated as 0.20 with 95 % CI (0.16, 0.25) with a p-value of 0.0001, and the differences of PDRs over time and according to the employed approaches were not statistically significant with p-values of 0.06 and 0.99, respectively. However, PDRs determined by statistical approaches alone showed greater dispersion in comparison with the ‘panel review approach’.
Conclusions
This article provided some insights about the trauma care system by computing the pooled estimate of PDRs over the past 23 years as an indicator. The pooled PDR was estimated as approximately 20 %, with no statistical significance of differences in PDRs over time or by the evaluation methods employed. That left us still room for improvement in trauma care system despite our efforts to reduce PDRs. In addition, when ‘statistical approaches’ are applied alone to estimate PDRs, we recommend that statistical methods should be applied with caution when the characteristics of trauma patients are heterogeneous. The optimal approach might be to combine both statistical and panel review approaches instead of employing a single approach.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Trauma is one of the leading causes of deaths worldwide [23]. As a result, many physicians are aware of the importance of the trauma care system, and study the causes of deaths in order to improve outcomes in the traumatic care setting. Preventable deaths imply that the patient could have survived under optimal treatment conditions in the optimal trauma care system. However, it is difficult to define the optimal care and to determine ‘avoidable’ or ‘preventable’ deaths. Generally, deaths resulting from trauma are classified as ‘immediate death’, ‘early death’, and ‘late death’ according to the time from the occurrence of trauma to the time of death. Among these, preventable death seems to be most closely related to ‘early death’ where early death occurs in the first 6 h as a result of evolving conditions or complications such as hemorrhagic injuries [9, 23]. Accordingly, preventable deaths can occur in either the pre-hospital stage or hospital stage. Physicians report preventable death rates (PDRs) in an attempt to diagnose or improve the trauma care system including the emergency care system. However, PDRs vary widely among articles. We systematically reviewed articles about PDRs published for the period of 1990–2013, and estimated the pooled PDRs. In addition, we provided some insights about PDRs by statistically analyzing the studies on the selected articles using meta-analysis.
Methods
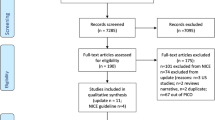
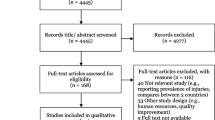
As shown by Fig. 1, articles were identified through bibliographic searches using PUBMED based on the following inclusion criteria: articles were restricted to those published in English since 1990 reporting preventable deaths with trauma patients; trauma, preventable, deaths and cause of deaths were used as keywords; clinical articles using animals and articles relating to combat were excluded; and book chapters and literature reviews were also excluded.

Article selection procedure
According to systematic searches in Fig. 1, a total of 27 articles were selected which were published in 14 different countries, and they are summarized in Table 1. Most studies (85.2 %) involved the collection of data retrospectively, and common sources of data were pre-hospital records, hospital medical records and autopsy results. The target populations of all articles except one were adult trauma patients whose mean ages ranged from 32.9 to 58 years old. The average proportion of male patients in the studies was about 72 %, and the sample sizes were distributed from 13 to 2,081. The study periods ranged from three months to nine years. Preventable deaths were evaluated by multidisciplinary panel review (55.6 %), statistical approaches such as Ps (probability of survival) (3.7 %; [21]) and mixed approaches of those two. The trauma patients in [21], which only used Ps, were solely based on severe brain injury patients. Some articles (29.6 %) evaluated the preventability of traumatic deaths using panel reviews but also computed Ps using TRISS [trauma and Injury severity score (ISS)] [13, 20, 26, 27] or ASCOT (A severity characterization of trauma) [27]. Boman et al. [2], Ince et al. [15] and Ashour et al. [1] used the ISS or AIS (abbreviated injury scale) scale instead. In Table 2, the PDRs were computed by dividing the number of preventable deaths by the number of total deaths, and the counts of the preventable deaths in this article were computed by adding the counts of ‘preventable death’ to the counts of ‘potentially preventable death’.
Results
Pooled estiamtes of PDRs
In Table 2, PDRs were widely distributed from 2.5 to 58.5 %, and sample sizes varied from 13 to 2,081. McDermott et al. [20] compared two datasets having separate study periods of (1997–1998) and (2002–2004), and we considered PDRs associated with each study period separately in data synthesis, marked as McDermott et al.1 and McDermott et al.2 in Fig. 2. Considering all 28 studies, we estimated the pooled PDR by meta-analysis. The estimated pooled PDR was 0.20 with a 95 % confidence interval (0.16, 0.25) based on the random effect model to take into consideration the variability of the studies. The pooled variance between the studies (τ2) was computed by DerSimonian and Lairds estimation. Z-statistics to test the significance of the estimated PDR and determined it to be statistically significant with the p-value of less than 0.0001.

Pooled PDRs
Difference of PDRs over time
Boman et al. [2] determined the decrease in PDRs over time using the proportion of preventable deaths during the period of 1988–1996 in Sweden. We studied whether the same trend existed in the selected articles. Two articles whose study periods were unavailable [19, 33] were excluded from this analysis. Accordingly, 26 studies were categorized into two groups based on the median years of the study periods. The first group consisted of 15 articles (57.7 %) with a median study years of 1990–2000. The other 11 articles (42.3 %) were assigned to the second group whose median study years were 2000–2013. We statistically tested whether the PDRs were different between these two groups: the PDRs were estimated to be 0.24 with 95 % CI (0.01, 0.18) for the first group and 0.16 with 95 % CI (0.09, 0.22) for the second group (Fig. 3). The results showed that the PDRs were lower in the more recent studies, but the difference was not statistically significant with a p-value of 0.06 by Q-test. We also tested the time effect on PDRs using a regression approach and found that the effect was not statistically significant with a p-value of 0.77.

Difference of PDRs by years
Difference in PDRs related to the employed evaluation approaches
Three approaches were employed to determine preventable deaths in the selected articles: (1) expert panel review, (2) statistical methods, and (3) a mixed approach which used both (1) and (2) together. More than half of the articles (57.1 %) chose a panel review approach to identify the preventable deaths, and the panels were generally composed of multidisciplinary team members including two to three trauma surgeons. The second most frequent approach (28.6 %) was the mixed approach combining a panel review with any type of statistical method. However, preventable deaths were typically determined by panel review on the mixed approach, and the statistical methods were employed to filter the deaths which were examined. The remaining articles (14.3 %) applied any type of statistical methods to define the preventable deaths such as TRISS, ASCOT or ISS severity score. We categorized the articles into two groups: the first group included the articles using either ‘panel review approach’ or ‘mixed approach’, and the second group included those using the ‘statistical approach’. The pooled PDRs were estimated as 0.21 with a 95 % CI (0.16, 0.26) for the first group and as 0.19 with a 95 % CI (0.07, 0.32) for the second group. The difference in PDRs between the two groups was tested using Q-test and found to be not statistically significant with a p-value of 0.99. However, it should be noted that the dispersion of PDRs was approximately three times wider in the statistical approach group than in the panel review group shown by Fig. 4.

Difference of PDRs by the evaluation methods
Discussion
Some articles differentiated ‘preventable deaths’ from ‘potentially preventable deaths’ according to the severities of the injuries [11, 14], but we treated them collectively as ‘preventable deaths’ in the analysis. The preventable deaths were conditioned on two in [11]: (1) injuries or sequelae considered (severe but) survivable or (2) (suspected) errors in care which implicated directly or indirectly in the patient‘s demise. Reported factors contributing to preventable deaths were diverse according to the mechanisms of the injuries. Most categories referred to in preventable deaths were diagnostic errors, missed injuries, delay in transfer or inadequate care [14]. Accordingly, the PDRs might be regarded as an indicator of the quality of the trauma care system. However, the range of PDRs across articles varied widely, and the evaluation approaches, sample size, study locations and study periods were also significantly different across the studies. These factors led us to question the external validity of PDRs. Because of these reasons, we systematically searched articles being published since 1990 through PubMed, and selected 27 articles for further studies. With the selected articles, we examined: (1) the representative measure of PDRs; (2) whether PDRs changed over time; and (3) whether PDRs were affected by the evaluation approach which was employed to determine the preventable deaths. We addressed these questions by conducting meta-analysis of the article data and testing for statistical significance controlling alpha at a level of 0.05. The pooled estimate of the PDRs was approximately 20 % on average over the period 1990–2013. When we compared the difference in PDRs between the periods of (1990–2000) and (2000–2013), the difference was not statistically significant with a p-value of 0.06 although the proportion of preventable deaths was lower in more recent years (which was similar to [2]). To eliminate the evaluation approach as a confounder in our analysis, the difference was also analogously tested with articles which only used the ’panel review approach’; however, the test result did not change with a p-value of 0.17. The analysis results implied that there might still be room for improvement in the trauma care system despite significant efforts. The difference in PDRs using different evaluation approaches was not statistically significant with p-value of 0.98. Namely, PDRs were not affected by the employed approach to identify the preventable deaths. Some articles favored the ‘panel review approach’ over the ‘statistical approach’, but panel review could over-inflate the PDRs [16]. In the panel review approach, there was no gold standard for the optimal make up of panels or ‘how to reach a decision evaluating preventable deaths’. However, most articles using a panel review approach constitued 'multidisciplinary team', and some even used autopsy reports to make a decision. Those efforts might prevent PDRs from over-flating by incorporating various points of views in a panel review approach. Some articles criticized ‘statistical approach’. TRISS was prevalently used, but it was criticized because of its wide variation in mortality prediction when the trauma types were broad [4, 6, 7, 8]. Conversely, Moon et al. [21] supported the use of Ps in mortality using TRISS. When we compared the difference in PDRs according to the employed approach, PDRs estimated by the ‘statistical approach’ were about three times wider in dispersion compared with the ‘panel review approach’. The wider dispersion of PDRs could be attributed to the variability of trauma deaths across the studies in agreement with the findings about the ‘statistical approach’ of Cayten et al. [5]. It is also plausible that Moon et al. [21] applied TRISS to predict the mortality with only neuro-trauma patients, and TRISS worked well. Yet, Shanti et al. [26] demonstrated that the ‘statistical approach’ resulted in a consistent trend: the higher Ps, the more likely the death was found to be preventable. It appeared that there was no superior approach for PDR estimation. Thus, we need to select the evaluation approach with caution. In the case of a panel review approach, it is important to carefully select the make up of the multidisciplinary panel to determine the preventable deaths without bias. When a ‘statistical approach’ was applied as a stand-alone method, we need to first consider the types of trauma patients evaluated so as not to broaden the dispersion of PDRs. If the majority of trauma patients had multiple injuries or trauma characteristics are heterogeneous, a ‘statistical approach’ might serve as a good diagnostic filter within a ‘panel review approach’, but the estimate of PDR might not be accurate enough to make an inference because of the higher dispersion. Generally, it might be more suitable to combine a ‘panel review’ with a ‘statistical approach’ rather than to choose either one.
Conclusion
As an indicator to diagnose the quality of the trauma care system, we estimated the pooled PDR with articles published from 1990 to 2013 using meta-analysis. As a result, the estimate of PDRs was computed as about 20 %. More recent articles reported slightly lower PDRs, but the decrease in PDRs over time was not significant, which suggests that additional effort is needed to reduce PDRs by improving the trauma care system. In addition, we tested the difference in PDRs according to the selected evaluation approach and also determined that the differences were not significant. However, we need to carefully consider the most accurate approach to determine preventable deaths. When applying a ‘panel review approach’, we need to carefully select a multidisciplinary panel so that various viewpoints are reflected. When a ‘statistical approach’ is applied, we need to select patients whose trauma types are as similar as possible to avoid broadening the confidence intervals of PDRs. Most of all, it might be optimal to find the cross-point of the two approaches by combining both approaches instead of choosing a single approach.
References
Ashour A, Cameron P, Bernard S et al. (2007) Could bystander first-aid prevent trauma deaths at the scene of injury?. EMA. 19:163–68.
Boman H, Bjornstig U, Hedelin A et al. (1999) Avoidable deaths in two areas of Sweden-analysis of deaths in hospital after injury. Eur J Surg. 165:828–33.
Caldwell M, McGovern E. Fatal trauma: a five year review in a Dublin hospital. LJMS. 1993;309–12.
Cayten CG, Stahl WM, Agarwal N et al. (1991) Analysis of preventable deaths by mechanism of injury among 13,500 trauma admissions. Annual meeting of the American surgical association 4:510–20.
Cayten CG, Stahl WM, Murphy JG et al. (1991) Limitation of TRISS method for interhospital comparisons: a multihospital study. J Trauma. 31:471–82.
Champion HR, Sacco WJ, Copes WS et al. (1989) A revision of the trauma score. J Trauma. 29:623–29.
Champion HR, Copes WS, Sacco WJ et al. (1990) A new characterization of injury severity. J Trauma. 30(5):539–46.
Champion HR, Copes WS, Sacco WJ et al. (1996) Improved predications from a severity characterization of trauma (ASCOT) over trauma and injury severity score. J Trauma. 40:42–48.
Chiara O, Scott J, Cimbanassi S et al. (2002) Trauma deaths in an Italian urban area: an audit of pre-hospital and in-hospital trauma care. Injury. 33(7):553–62.
Chua WC, DAmours SK, Sugrue M et al. (2009) Performance and consistency of care in admitted trauma patients: our next great opportunity in trauma care?. ANZ J Surg. 79:443–48.
Davis J, Hoyt D, McArdle S et al. (1991) The significance of critical care errors in causing preventable death in trauma patients in a trauma system. J Trauma. 31(6):813–19.
Esposito T, Sanddal N, Dean M et al. (1999) Analysis of preventable pediatric trauma deaths and inappropriate trauma care in Montana. J Trauma. 47(2):243–53.
Gorman D, Teanby D, Shinha M et al. (1996) Preventable deaths among major trauma patients in Mersey Region, North Wales and the Isle of Man. Injury. 27(3):189–92.
Iau P, Ong C, Chan S (1998) Preventable trauma deaths in Singapore. Aust N Z J Surg. 68:820–25.
Ince H, Ince N, Taviloglu K et al. (2006) A different approach to trauma scoring. Turkish J Trauma Emerg Surg. 12(3):195–200.
Kelly A, Epstein J (1997) Preventable death studies: an inappropriate tool for evaluating trauma systems. Aust N Z J Surg. 67:591–92.
Kleber C, Giesecke T, Tsokos M et al. (2013) Trauma-related preventable deaths in Berlin 2010: need to change prehospital management strategies and trauma management education. World J Surg. 37(5):1154–161.
Maio R, Burney R, Gregor M et al. (1996) A study of preventable trauma mortality in rural Michigan. J Trauma. 41(1):83–90.
Martine B, Fallon W, Palmieri P et al (2007) Autopsy data in the peer review process improves outcomes analysis. J Trauma. 62:69–73.
McDermott F, Cordner S, Cooper D et al. (2007) Management deficiencies and death preventability of road traffic fatalities before and after a new trauma care system in Victoria, Australia. J Trauma. 63:331–38.
Moon J, Seo B, Jang J et al. (2013) Evaluation of probability of survival using trauma and injury severity score method in severe neurotrauma patients. J Korean Neurosurg Soc. 54:42–46.
Papadopoulos I, Bukis D, Karalas E et al. (1996) Preventable prehospital trauma deaths in a hellenic urban health region: an audit of prehospital trauma care. J Trauma. 41(5):864–69.
Pfeifer R, Tarkin I, Rocos B et al. (2009) Patterns of mortality and causes of death in polytrauma patients-has anything changed?, Injury. 40(9):907–11.
Saltzherr T, Wendt K, Nieboer P et al. (2011) Preventability of trauma deaths in a Dutch level-1 trauma centre. Injury. 42:870–73.
Sanddal T, Esposito T, Whitney J et al. (2011) Analysis of preventable trauma deaths and opportunities for trauma care improvement in Utah. J Trauma. 70(4):970–77.
Shanti C, Tyburski J, Rishell K et al. (2003) Correlation of revised trauma score and injury severity score (TRISS) predicted probability of survival with peer-reviewed determination of trauma deaths. Am Surg. 69(3):257–60.
Sugrue M, Seger M, Sloane D et al. (1996) Trauma outcomes: a death analysis study. IJMS. 4:99–104.
Teixeira P, Inaba K, Hadjizacharia P et al. (2007) Preventable or potentially preventable mortality at a mature trauma center. J Trauma. 63:1338–347.
Thoburn E, Norris P, Flores R et al. (1993) System care improves trauma outcome: patient care errors dominate reduced preventable death rate. JEM. 11:135–39.
Tien H, Spencer F, Tremblay L et al. (2007) Preventable deaths from hemorrhage at a level 1 Canadian trauma center. J Trauma. 62:142–46.
Wilson J, Herbella F, Takassi G et al. (2011) Fatal trauma injuries in a Brazilian big metropolis: a study of autopsies. Rev Col Bras Cir. 38(2):122–26.
Yates D, Woodford M, Hollis S (1993) Trauma audit: clinical judgement or statistical analysis?. Ann R Coll Surg Engl. 75:321–24.
Zafarghandi M, Modaghegh M, Roudsari B (2003) Preventable trauma death in Tehran: an estimate of trauma care quality in teaching hospitals. J Trauma. 55:459–65.
Conflict of interest
None.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Kwon, A.M., Garbett, N.C. & Kloecker, G.H. Pooled preventable death rates in trauma patients. Eur J Trauma Emerg Surg 40, 279–285 (2014). https://doi.org/10.1007/s00068-013-0364-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00068-013-0364-5