
Abstract
Background and Purpose:
High-dose irradiation to the pulmonary hilar region is generally considered to be of high risk in causing bronchial injury. The aim of this retrospective study is to investigate the safety and efficacy of stereotactic body radiotherapy (SBRT) for patients with lung tumors in the pulmonary hilum.
Patients and Methods:
21 patients who underwent SBRT for lung tumors within 2 cm from a major bronchus were retrospectively analyzed. The total biologically effective doses ranging from 50.7 to 157.5 Gy (median, 100 Gy) were given to the tumors by SBRT.
Results:
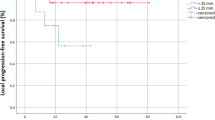
The overall survival rates at 1 and 2 years after SBRT were 90.0% and 62.2%, respectively. Nine patients were alive and 15 irradiated tumors were controlled during the follow-up period of 10–54 months (median, 20 months). Nine patients died of tumor progression and one patient each died of hemoptysis, infectious pneumonia, and epidural hemorrhage. Severe late toxicity (≥ grade 3) was seen in three patients of whom two had previously received repeated radiotherapy.
Conclusion:
SBRT for lung tumors located in the pulmonary hilar region may be tolerable and acceptable, if multiple treatments to the same major bronchus are avoided, and irradiated volumes are carefully taken into consideration.
Zusammenfassung
Hintergrund und Ziel:
Die hochdosierte Bestrahlung der Lungenhilusregion gilt im Allgemeinen als großes Risiko in Bezug auf die Verursachung von Bronchialverletzungen. Ziel dieser retrospektiven Studie ist die Untersuchung der Sicherheit und Wirksamkeit der stereotaktischen Strahlentherapie bei Patienten mit Lungentumoren im Hilum pulmonis.
Patienten und Methodik:
21 Patienten, die sich einer stereotaktischen Bestrahlung von Lungentumoren im Abstand von bis zu 2 cm zu einem Hauptbronchus unterzogen, wurden retrospektiv analysiert. Die Tumoren wurden mit biologisch wirksamen Gesamtdosen im Bereich von 50,7 bis 157,5 Gy (Median: 100 Gy) bestrahlt.
Ergebnisse:
Die Gesamtüberlebensraten 1 und 2 Jahre nach der stereotaktischen Strahlentherapie lagen bei 90,0% bzw. 62,2%. Während des Nachuntersuchungszeitraums von 10–54 Monaten (Median: 20 Monate) waren neun Patienten am Leben, und 15 bestrahlte Tumoren wurden kontrolliert. Neun Patienten starben aufgrund von Tumorprogression und je ein Patient starb infolge von Hämoptysis, infektiöser Pneumonie und epiduraler Blutung. Schwere Spättoxizität (≥ Grad 3) wurde bei drei Patienten beobachtet, von denen sich zwei in der Vergangenheit mehreren Strahlentherapien unterzogen hatten.
Schlussfolgerung:
Eine stereotaktische Strahlentherapie bei Lungentumoren in der Gegend des Lungenhilus ist möglicherweise verträglich und vertretbar, wenn mehrere Behandlungen des gleichen Hauptbronchus vermieden und bestrahlte Volumen sorgfältig berücksichtigt werden.
Article PDF
Similar content being viewed by others


Avoid common mistakes on your manuscript.
References
Chang JY, Balter PA, Dong L, et al. Stereotactic body radiation therapy in centrally and superiorly located stage I or isolated recurrent non-small-cell lung cancer. Int J Radiat Oncol Biol Phys 2008;72:967–971.
Cox JD, Stetz J, Pajak TF. Toxicity criteria of the Radiation Therapy Oncology Group (RTOG) and the European Organization for Research and Treatment of Cancer (EORTC). Int J Radiat Oncol Biol Phys 1995;31:1341–1346.
Ernst-Stecken A, Lambrecht U, Mueller R, et al. Hypofractionated stereotactic radiotherapy for primary and secondary intrapulmonary tumors: first results of a phase I/II study. Strahlenther Onkol 2006;182:696–702.
Fowler JF, Tome WA, Fenwick JD, Mehta MP. A challenge to traditional radiation oncology. Int J Radiat Oncol Biol Phys 2004;60:1241–1256.
Graham MV, Purdy JA, Emami B, et al. Clinical dose-volume histogram analysis for pneumonitis after 3D treatment for non-small cell lung cancer (NSCLC). Int J Radiat Oncol Biol Phys 1999;45:323–329.
Hara R, Itami J, Komiyama T, et al. Serum levels of KL-6 for predicting the occurrence of radiation pneumonitis after stereotactic radiotherapy for lung tumors. Chest 2004;125:340–344.
Hara R, Itami J, Kondo T, et al. Stereotactic single high dose irradiation of lung tumors under respiratory gating. Radiother Oncol 2002;63:159–163.
Hara R, Itami J, Kondo T, et al. Clinical outcomes of single-fraction stereotactic radiation therapy of lung tumors. Cancer 2006;106:1347–1352.
Hui Z, Zhang X, Starkschall G, et al. Effects of interfractional motion and anatomic changes on proton therapy dose distribution in lung cancer. Int J Radiat Oncol Biol Phys 2008;72:1385–1395.
James K, Eisenhauer E, Christian M, et al. Measuring response in solid tumors: unidimensional versus bidimensional measurement. J Natl Cancer Inst 1999;91:523–528.
Jereczek-Fossa BA, Kowalczyk A, D’Onofrio A, et al. Three-dimensional conformal or stereotactic reirradiation of recurrent, metastatic or new primary tumors. Analysis of 108 patients. Strahlenther Onkol 2008;184:36–40.
Joyner M, Salter BJ, Papanikolaou N, Fuss M. Stereotactic body radiation therapy for centrally located lung lesions. Acta Oncol 2006;45:802–807.
Kaplan EL, Meier P. Nonparametric estimation from incomplete observations. J Am Stat Assoc 1958;31:457–481.
Koto M, Takai Y, Ogawa Y, et al. A phase II study on stereotactic body radiotherapy for stage I non-small cell lung cancer. Radiother Oncol 2007;85:429–434.
McGarry RC, Papiez L, Williams M, et al. Stereotactic body radiation therapy of early-stage non-small-cell lung carcinoma: phase I study. Int J Radiat Oncol Biol Phys 2005;63:1010–1015.
Miller KL, Shafman TD, Anscher MS, et al. Bronchial stenosis: an underreported complication of high-dose external beam radiotherapy for lung cancer? Int J Radiat Oncol Biol Phys 2005;61:64–69.
Mirri MA, Arcangeli G, Benassi M, et al. Hypofractionated conformal radiotherapy (HCRT) for primary and metastatic lung cancers with small dimension. Efficacy and toxicity. Strahlenther Onkol 2009;185:27–33.
Oken MM, Creech RH, Tormey DC, et al. Toxicity and response criteria of the Eastern Cooperative Oncology Group. Am J Clin Oncol 1982;5:649–655.
Onishi H, Araki T, Shirato H, et al. Stereotactic hypofractionated high-dose irradiation for stage I nonsmall cell lung carcinoma: clinical outcomes in 245 subjects in a Japanese multiinstitutional study. Cancer 2004;101:1623–1631.
Seppenwoolde Y, Shirato H, Kitamura K, et al. Precise and real-time measurement of 3D tumor motion in lung due to breathing and heartbeat, measured during radiotherapy. Int J Radiat Oncol Biol Phys 2002;53:822–834.
Sibley GS. Radiotherapy for patients with medically inoperable stage I nonsmall cell lung carcinoma: smaller volumes and higher doses — a review. Cancer 1998;82:433–438.
Sobin LH, Wittekind C, eds. Classification of malignant tumors, 6th edn. New York: Wiley-Liss, 2002.
Speiser BL, Spratling L. Remote afterloading brachytherapy for the local control of endobronchial carcinoma. Int J Radiat Oncol Biol Phys 1993;25:579–587.
Speiser BL, Spratling L. Radiation bronchitis and stenosis secondary to high dose rate endobronchial irradiation. Int J Radiat Oncol Biol Phys 1993;25:589–597.
Takayama K, Nagata Y, Negoro Y, et al. Treatment planning of stereotactic radiotherapy for solitary lung tumor. Int J Radiat Oncol Biol Phys 2005;61:1565–1571.
Timmerman R, McGarry R, Yiannoutsos C, et al. Excessive toxicity when treating central tumors in a phase II study of stereotactic body radiation therapy for medically inoperable early-stage lung cancer. J Clin Oncol 2006;24:4833–4839.
Tinnel B, Mendonca MS, Henderson M, et al. Pulmonary hilar stereotactic body radiation therapy in the rat. Technol Cancer Res Treat 2007;6:425–431.
Trotti A, Colevas AD, Setser A, et al. CTCAE v3.0: development of a comprehensive grading system for the adverse effects of cancer treatment. Semin Radiat Oncol 2003;13:176–181.
Wang C, Nakayama H, Sugahara S, et al. Comparisons of dose-volume histograms for proton-beam versus 3-D conformal X-ray therapy in patients with stage I non-small cell lung cancer. Strahlenther Onkol 2009;185:231–234.
Wara WM, Phillips TL, Margolis LW, Smith V. Radiation pneumonitis: a new approach to the derivation of time-dose factors. Cancer 1973;32:547–552.
Wiehle R, Koth HJ, Nanko N, et al. On the accuracy of isocenter verification with kV imaging in stereotactic radiosurgery. Strahlenther Onkol 2009;185:325–330.
Wu J, Li H, Shekhar R, et al. An evaluation of planning techniques for stereotactic body radiation therapy in lung tumors. Radiother Oncol 2008;87:35–43.
Wulf J, Haedinger U, Oppitz U, et al. Stereotactic radiotherapy of targets in the lung and liver. Strahlenther Onkol 2001;177:645–655.
Wulf J, Haedinger U, Oppitz U, et al. Stereotactic radiotherapy for primary lung cancer and pulmonary metastases: a noninvasive treatment approach in medically inoperable patients. Int J Radiat Oncol Biol Phys 2004;60: 186–196.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Oshiro, Y., Aruga, T., Tsuboi, K. et al. Stereotactic Body Radiotherapy for Lung Tumors at the Pulmonary Hilum. Strahlenther Onkol 186, 274–279 (2010). https://doi.org/10.1007/s00066-010-2072-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00066-010-2072-y