
Abstract
Purpose
Multi-modal brain imaging provides different in vivo windows into the human brain and thereby different ways to characterize brain disorders. Particularly, resting-state functional magnetic resonance imaging facilitates the study of macroscopic intrinsic brain networks, which are critical for development and spread of neurodegenerative processes in different neurodegenerative diseases. The aim of the current study is to present and highlight some paradigmatic findings in intrinsic network-based pathophysiology of neurodegenerative diseases and its potential for new network-based multimodal tools in imaging diagnostics.
Methods
Qualitative review of selected multi-modal imaging studies in neurodegenerative diseases particularly in Alzheimer’s disease (AD).
Results
Functional connectivity of intrinsic brain networks is selectively and progressively impaired in AD, with changes likely starting before the onset of symptoms in fronto-parietal key networks such as default mode or attention networks. Patterns of distribution and development of both amyloid-β plaques and atrophy are linked with network connectivity changes, suggesting that start and spread of pathology interacts with network connectivity. Qualitatively similar findings have been observed in other neurodegenerative disorders, suggesting shared mechanisms of network-based pathophysiology across diseases.
Conclusion
Spread of neurodegeneration is intimately linked with the functional connectivity of intrinsic brain networks. These pathophysiological insights pave the way for new multi-modal network-based tools to detect and characterize neurodegeneration in individual patients.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Multi-modal brain imaging provides distinct in vivo windows into the human brain and thereby specific ways to characterize brain disorders. Different methods range from structural magnetic resonance imaging (MRI), revealing volumetric aspects of brain tissue, to diffusion-weighted MRI, detecting water diffusion along brain fibers and thereby structural connectivity, to functional MRI, being sensitive to blood oxygenation changes caused indirectly by regional brain activity. When using multi-modal neuroimaging to characterize brain disorders, the variety of distinct brain aspects calls for integrating pathophysiological models. Macroscopic intrinsic brain networks represent a fundamental large-scale organization of the mammalian brain, which can be detected in vivo by resting-state functional MRI [1]. Intrinsic brain networks are characterized by coherent ongoing blood oxygenation-dependent activity that fluctuates at about 0.1 Hz, and are consistently found in different species [2], along the whole human ontogenetic trajectory [3], and across different states of consciousness [4]. Critically, since intrinsic networks are sensitive to different brain disorders’ changes via altered coherence in ongoing activity, they offer a pathophysiological framework to characterize brain disorders and to integrate different types of brain changes. The aim of the current paper is to present and highlight some paradigmatic findings in intrinsic network-based pathophysiology of neurodegenerative diseases and its potential role for new network-based multimodal tools in imaging diagnostics.
Since already excellent reviews about intrinsic network-centered multi-modal connectivity changes in neurodegenerative disorders exist [5, 6], we focused our review on few selected studies which we found appropriate for our study’s focus on network-based pathophysiology and the role of those intrinsic networks in multi-modal imaging. The selection of previous literature is biased in two ways: firstly it is centered on Alzheimer’s disease (AD), since most work has been done in this field; secondly, we place emphasis on studies of our own research laboratory due to the aim of the journal’s special issue, that is, to present distinct neuroradiology departments of 50 years Deutsche Gesellschaft für Neuroradiologie. This means formally, we performed a qualitative review of author-biased selected studies about neurodegenerative diseases and intrinsic brain networks. In the beginning, we reported about selective and progressive changes in intrinsic networks in neurodegenerative disorders, then how these changes link with neurodegenerative processes as revealed by multi-modal imaging. After that functional changes in intrinsic connectivity were linked with changes in structural connectivity; this allows us in the end to mention some relevant points about network- or connectivity-based multi-modal imaging tools for the characterization of neurodegeneration.
Altered Intrinsic Brain Networks in Neurodegenerative Diseases
Intrinsic networks are measured by patterns of functional connectivity in resting-state functional magnetic resonance imaging (fMRI) data, that is, spatial patterns of correlated fMRI signals [1]. Specific patterns of such stationary correlated blood oxygenation level-dependent (BOLD) signal time courses define specific intrinsic networks. Examples for such networks are the default mode or attention networks as well as primary sensory or sensori-motor networks. In 2004, Greicius et al. [7] were the first showing that a brain disorder has an impact on an intrinsic brain network. They demonstrated that patients with AD dementia had reduced functional connectivity in the default mode network particularly in parietal and hippocampal sub-regions. In 2007, we found that in patients with mild cognitive impairment being at increased risk for AD, reduced functional connectivity was present only in selected intrinsic networks, namely the medial fronto-parietal default mode and lateral attention network [8]. Other networks such as primary sensory and motor networks were unchanged, and connectivity changes were independent from structural changes, that is, atrophy mainly in medial temporal lobes. Agosta et al. [9] found in a similar way that such patterns of selected intrinsic network changes proceed and extend from patients with mild cognitive impairment to patients with AD dementia, suggesting progressive and selective changes in functional connectivity across intrinsic networks along the course of the disease. Recently, Lim et al. [10] found both reduced and increased functional connectivity in the default mode and lateral attention networks in cognitively normal people but with significant amyloid-β plaque load as measured by in vivo Pittsburgh-compound-B (PiB) positron emission tomography (PET); amyloid-β pathology is assumed to be the critical causal agent in AD pathogenesis [11]. This finding suggests both a preclinical start of aberrant intrinsic network connectivity in AD and a link between aberrant intrinsic connectivity and AD’s molecular key pathology, that is, amyloid-β deposition.
Even though less examined than in AD, other neurodegenerative diseases such as fronto-temporal lobar degenerations or Parkinson’s disease show similar patterns of progressive network changes (for review [6]). For example, in patients with behavioral variant fronto-temporal dementia, functional connectivity of the salience network including anterior cingulate and insula is primarily disrupted [12], while in patients with Parkinson’s disease, intrinsic connectivity between cortical-thalamic-cerebellar networks is preferentially altered [13]. For comprehensive review of intrinsic network changes across different neurodegenerative disorders see [6].
Characteristically Altered Intrinsic Networks and Their Link with Neurodegeneration
Given such trajectories of intrinsic network changes, two questions arise: are changes in functional connectivity specific for distinct neurodegenerative diseases, and how do these changes link with patterns of neurodegeneration? Concerning the first question, Zhou et al. [12] demonstrated that in patients with behavioral variant fronto-temporal dementia, impaired functional connectivity was preferentially found in the salience network in sharp contrast to patients with AD dementia, whose strongest affected intrinsic network was the default mode network. More generally, Seeley et al. [14] demonstrated that spatial patterns of atrophy across distinct neurodegenerative disorders (i.e., AD, semantic dementia, behavioral variant fronto-temporal dementia, progressive non-fluent aphasia, and corticobasal degeneration) resembles distinct intrinsic networks in healthy people in a way that suggests a preferential impact of distinct diseases on specific intrinsic networks: for example, while AD preferentially impacts the default mode network, behavioral variant fronto-temporal dementia affects particularly the salience network and progressive nonfluent aphasia a left lateralized fronto-parieto-temporal network comprising Broca’s and Wernicke’s area.
Concerning the question about the link between network changes and neurodegeneration, Zhou et al. demonstrated in an elegant graph-based approach that in different neurodegenerative diseases (i.e., the same as in the study by Seeley et al. [14]), the detailed spatial pattern of atrophy can be explained by specific patterns of intrinsic connectivity in healthy controls [15]: starting from the center of atrophy, graded volume reduction corresponds with graded functional connectivity, suggesting that the spread of neurodegeneration is associated with intrinsic functional connectivity.
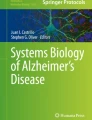
While the studies of Seeley and Zhou focused on general signs of neurodegeneration across different diseases, that is, atrophy, each neurodegenerative disease is characterized by more specific molecular pathways, for example, amyloid-β pathology in AD. Concerning AD, aberrant functional connectivity of intrinsic networks has been shown to link intimately with AD’s amyloid-β pathology [16]. Using PiB-PET and resting-state fMRI in asymptomatic and mildly cognitive impaired elderly with amyloid-β positivity, Drzezga et al. [17] found that a high amyloid-β plaque load is associated with a reduction of global centrality of parietal cortical hubs (centrality measures for each voxel its degree of functional connectivity with all other voxels of the brain). More specifically, we found in individual patients of prodromal AD (i.e., predementia AD) that for several networks such as default mode and different attention networks, spatial distributions of plaques and network functional connectivity were highly correspondent, suggesting that plaque spread is linked with networks’ connectivity [18]. Furthermore, in network centers of high connectivity and high plaque load, this relationship changes in the opposite direction, that is, the more plaques the more connectivity is impaired, indicating the detrimental effect of amyloid pathology on intrinsic functional connectivity when certain levels of pathology are overstepped (see Fig. 1). Complementary to these empirical findings, three very recent studies using advanced mathematical modeling of pathology expansion demonstrated prion-like spread of pathological agents along brain network connectivity in patients with AD and fronto-temporal dementia [19–21]. Taken together, these results demonstrate convincingly the relevance of intrinsic brain networks for molecular pathophysiology and pathogenesis of AD particularly in early stages of the disease.

Model of graded spread of amyloid-β pathology along intrinsicbrain networks. a Over the course of time amyloid-β pathology follows functional connectivity across intrinsic networks, typically starting in the default mode network and then affecting different lateral attention networks. b Within networks, cores of highest levels of functional connectivity are affected first, later pathology spreads to the network’s periphery. Figure is modified from [18]
Altered Intrinsic Networks and Disrupted Structural Connectivity in AD and Other Neurodegenerative Diseases
How do such changes in intrinsic functional connectivity link with structural connectivity in neurodegenerative diseases? Both empirical findings and computational modeling demonstrate that tract-based structural connectivity is a key factor in shaping intrinsic functional connectivity [22, 23]. Recently, we found that selective and progressive disruptions in intrinsic network functional connectivity were mirrored by similar selective and progressive disruptions in structural connectivity of the same networks (i.e., default mode and lateral attention networks in patients with mild cognitive impairment and AD dementia) [24]. This finding indicates that AD has a selective and progressive substantial (i.e., structural) impact on intrinsic networks beyond its degrading effect on functional organization. However, we found in addition that structural connectivity changes were beyond within-network changes but affected the whole structural connectome. This result emphasizes the central role of fronto-parietal key networks for the whole cortex activity due to their highest degrees of connectivity with other regions, and that AD impacts specifically these so-called hubs of the brain [25].
Concerning other neurodegenerative diseases, comparable findings were reported, that is, impaired intrinsic functional connectivity is accompanied by disrupted structural connectivity, whereas the overlap between aberrant functional and structural connectivity is not as perfect as in AD [6]. For example, in patients with behavioral variant fronto-temporal dementia, Zhang et al. [26] found strongly disrupted tract-based structural connectivity in the frontal lobes (beyond the salience network) being in sharp contrast to impaired structural connectivity of patients with AD showing changes preferential in the posterior brain (beyond the default mode network). For review of structural connectivity changes in further neurodegenerative diseases see [6].
Connectivity-Based Tools in Neurodegeneration Diagnostics and Caveats
In summary, these findings suggest intrinsic brain networks as a key component in the pathophysiology of neurodegenerative diseases. For example in AD, spread and detrimental effects of amyloid-β pathology on brain activity is intimately linked with the spatial layout of default mode and attention networks [18], suggesting that coherent intrinsic activity is both a initiator of amyloid-β pathology and a target of degrading effects. Due to this pathophysiological significance, network- and connectivity-based tools are promising candidates for imaging tools in neurodegenerative diagnostics particularly when integrating with other imaging modalities. For example, intrinsic network-based structural connectivity allowed us to separate patients with mild cognitive impairment into those who converted later to AD dementia and those that did not [24]. Furthermore, using whole brain structural connectivity and pattern recognition-based machine learning techniques, individual patients with prodromal or dementia AD were very robustly separated from healthy controls with accuracy values of more than 90 % [27]. Wee et al. [28] improved such accuracy values to more than 95 % by integrating structural and intrinsic functional connectivity to separate patients with mild cognitive impairment from healthy controls; however, Dybra et al. [29] were not able to replicate these findings, indicating some caveats for connectivity, particularly intrinsic connectivity-based methods for the use in diagnostics.
With respect to fMRI-based intrinsic functional connectivity, both the low signal-to-noise ratio and the nonquantitative nature of fMRI signals (i.e., BOLD signal) have substantial constrains for individual reliable diagnostics [30]. For example, Biswal et al. [31] demonstrated significant center effects on ongoing fMRI activity in a huge sample of more than 1400 subjects collected across 35 centers. The authors identified several factors underlying such center effects and which have to be carefully controlled for across-subject and across-center comparisons in a diagnostic context such as scanner type, sequence specifications, instructions to participants, and degree of participant’s wakefulness). Quantitative BOLD imaging and new data acquisition techniques (e.g., multi-band fMRI) producing much more data in a comparable amount of time to increase the power of data analysis might be helpful for future approaches [32].
Beyond such methodological considerations, how can in general intrinsic network-based pathophysiology contribute to multi-modal imaging tools for diagnostics in neurodegeneration? We like to mention some ideas: (I) Intrinsic network-based pathophysiology may provide—in its simplest form—regional priors for other brain modalities. For example, preferential impact of different neurodegenerative diseases [14] may define characteristic regional ensembles whose distinct brain parameters (such as volumetry, metabolism etc.) serve as measures used for differential or early stage diagnostics. (II) Disease specific regions may provide multi-modal “fingerprints”. (III) Disease specific regions define functional and structural connectivity scores, which may be used for diagnostics. (IV) Such connectivity-based scores could be integrated with further multi-modal imaging aspects in multi-modal connectivity-based scores: in the form of multi-modal patterns such as used in pattern classification [28] or as integrated scalars (e.g., via spatial correlation between connectivity scores and scores of another modality see [28]). In summary, a lot of new options for network-based diagnostics are available. Coming years will show how successful such approaches could be.
Conclusion
Alterations in intrinsic brain networks are essential in the pathophysiology of neurodegenerative diseases. Therefore, intrinsic connectivity might provide promising network-based imaging tools, which integrate multi-modal imaging data and advance diagnostics in neurodegeneration.
Conflict of Interest
The authors declare to have no conflict of interest.
References
Fox MD, Raichle ME. Spontaneous fluctuations in brain activity observed with functional magnetic resonance imaging. Nat Rev Neurosci. 2007;8:700–11.
Vincent JL, Patel GH, Fox MD, Snyder AZ, Baker JT, Van Essen DC, Zempel JM, Snyder LH, Corbetta M, Raichle ME. Intrinsic functional architecture in the anaesthetized monkey brain. Nature. 2007;447:83–6.
Doria V, Beckmann CF, Arichi T, Merchant N, Groppo M, Turkheimer FE, Counsell SJ, Murgasova M, Aljabar P, Nunes RG, Larkman DJ, Rees G, Edwards AD. Emergence of resting state networks in the preterm human brain. Proc Natl Acad Sci U S A. 2010;107:20015–20.
Smith SM, Fox PT, Miller KL, Glahn DC, Fox PM, Mackay CE, Filippini N, Watkins KE, Toro R, Laird AR, Beckmann CF. Correspondence of the brain’s functional architecture during activation and rest. Proc Natl Acad Sci U S A. 2009;106:13040–5.
Pievani M, De Haan W, Wu T, Seeley WW, Frisoni GB. Functional network disruption in the degenerative dementias. Lancet Neurol. 2011;10:829–43.
Pievani M, Filippini N, Van Den Heuvel MP, Cappa SF, Frisoni GB. Brain connectivity in neurodegenerative diseases—from phenotype to proteinopathy. Nat Rev Neurol. 2014;10:620–33.
Greicius MD, Srivastava G, Reiss AL, Menon V. Default-mode network activity distinguishes Alzheimer’s disease from healthy aging: evidence from functional MRI. Proc Natl Acad Sci U S A. 2004;101:4637–42.
Sorg C, Riedl V, Mühlau M, Calhoun VD, Eichele T, Läer L, Drzezga A, Förstl H, Kurz A, Zimmer C, Wohlschläger AM. Selective changes of resting-state networks in individuals at risk for Alzheimer’s disease. Proc Natl Acad Sci U S A. 2007;104:18760–5.
Agosta F, Pievani M, Geroldi C, Copetti M, Frisoni GB, Filippi M. Resting state fMRI in Alzheimer’s disease: beyond the default mode network. Neurobiol Aging. 2012;33:1564–78.
Lim HK, Nebes R, Snitz B, Cohen A, Mathis C, Price J, Weissfeld L, Klunk W, Aizenstein HJ. Regional amyloid burden and intrinsic connectivity networks in cognitively normal elderly subjects. Brain. 2014;137:3327–38.
Hardy J, Selkoe DJ. The amyloid hypothesis of Alzheimer’s disease: progress and problems on the road to therapeutics. Science. 2002;297:353–6.
Zhou J, Greicius MD, Gennatas ED, Growdon ME, Jang JY, Rabinovici GD, Kramer JH, Weiner M, Miller BL, Seeley WW. Divergent network connectivity changes in behavioural variant frontotemporal dementia and Alzheimer’s disease. Brain. 2010;133:1352–67.
Luo C, Song W, Chen Q, Zheng Z, Chen K, Cao B, Yang J, Li J, Huang X, Gong Q, Shang HF. Reduced functional connectivity in early-stage drug-naive Parkinson’s disease: a resting-state fMRI study. Neurobiol Aging. 2014;35:431–41.
Seeley WW, Crawford RK, Zhou J, Miller BL, Greicius MD. Neurodegenerative diseases target large-scale human brain networks. Neuron. 2009;62:42–52.
Zhou J, Gennatas ED, Kramer JH, Miller BL, Seeley WW. Predicting regional neurodegeneration from the healthy brain functional connectome. Neuron. 2012;73:1216–27.
Sperling RA, Laviolette PS, O'Keefe K, O'Brien J, Rentz DM, Pihlajamaki M, Marshall G, Hyman BT, Selkoe DJ, Hedden T, Buckner RL, Becker JA, Johnson KA. Amyloid deposition is associated with impaired default network function in older persons without dementia. Neuron. 2009;63:178–88.
Drzezga A, Becker JA, Van Dijk KR, Sreenivasan A, Talukdar T, Sullivan C, Schultz AP, Sepulcre J, Putcha D, Greve D, Johnson KA, Sperling RA. Neuronal dysfunction and disconnection of cortical hubs in non-demented subjects with elevated amyloid burden. Brain. 2011;134:1635–46.
Myers N, Pasquini L, Göttler J, Grimmer T, Koch K, Ortner M, Neitzel J, Mühlau M, Förster S, Kurz A, Förstl H, Zimmer C, Wohlschläger AM, Riedl V, Drzezga A, Sorg C. Within-patient correspondence of amyloid-beta and intrinsic network connectivity in Alzheimer’s disease. Brain. 2014;137:2052–64.
Iturria-Medina Y, Sotero RC, Toussaint PJ, Evans AC. Epidemic spreading model to characterize misfolded proteins propagation in aging and associated neurodegenerative disorders. PLoS Comput Biol. 2014;10:e1003956.
Raj A, Kuceyeski A, Weiner M. A network diffusion model of disease progression in dementia. Neuron. 2012;73:1204–15.
Raj A, Locastro E, Kuceyeski A, Tosun D, Relkin N, Weiner M; for the Alzheimer’s Disease Neuroimaging Initiative (ADNI). Network diffusion model of progression predicts longitudinal patterns of atrophy and metabolism in Alzheimer’s disease. Cell Rep. 2015; 10:359–69.
Deco G, Jirsa VK, Mcintosh AR. Resting brains never rest: computational insights into potential cognitive architectures. Trends Neurosci. 2013;36:268–74.
Honey CJ, Kotter R, Breakspear M, Sporns O. Network structure of cerebral cortex shapes functional connectivity on multiple time scales. Proc Natl Acad Sci U S A. 2007;104:10240–5.
Hahn K, Myers N, Prigarin S, Rodenacker K, Kurz A, Förstl H, Zimmer C, Wohlschläger AM, Sorg C. Selectively and progressively disrupted structural connectivity of functional brain networks in Alzheimer’s disease—revealed by a novel framework to analyze edge distributions of networks detecting disruptions with strong statistical evidence. Neuroimage. 2013;81:96–109.
Buckner RL, Sepulcre J, Talukdar T, Krienen FM, Liu H, Hedden T, Andrews-Hanna JR, Sperling RA, Johnson KA. Cortical hubs revealed by intrinsic functional connectivity: mapping, assessment of stability, and relation to Alzheimer’s disease. J Neurosci. 2009;29:1860–73.
Zhang Y, Schuff N, Du AT, Rosen HJ, Kramer JH, Gorno-Tempini ML, Miller BL, Weiner MW. White matter damage in frontotemporal dementia and Alzheimer’s disease measured by diffusion MRI. Brain. 2009;132:2579–92.
Shao J, Myers N, Yang Q, Feng J, Plant C, Böhm C, Förstl H, Kurz A, Zimmer C, Meng C, Riedl V, Wohlschläger A, Sorg C. Prediction of Alzheimer’s disease using individual structural connectivity networks. Neurobiol Aging. 2012;33:2756–65.
Wee CY, Yap PT, Zhang D, Denny K, Browndyke JN, Potter GG, Welsh-Bohmer KA, Wang L, Shen D. Identification of MCI individuals using structural and functional connectivity networks. Neuroimage. 2012;59:2045–56.
Dyrba M, Grothe M, Kirste T, Teipel SJ. Multimodal analysis of functional and structural disconnection in Alzheimer’s disease using multiple kernel SVM. Hum Brain Mapp. 2015;6:2118–31.
Fox MD, Greicius M. Clinical applications of resting state functional connectivity. Front Syst Neurosci. 2010;4:19.
Biswal BB, Mennes M, Zuo XN, Gohel S, Kelly C, Smith SM, Beckmann CF, Adelstein JS, Buckner RL, Colcombe S, Dogonowski AM, Ernst M, Fair D, Hampson M, Hoptman MJ, Hyde JS, Kiviniemi VJ, Kötter R, Li SJ, Lin CP, Lowe MJ, Mackay C, Madden DJ, Madsen KH, Margulies DS, Mayberg HS, McMahon K, Monk CS, Mostofsky SH, Nagel BJ, Pekar JJ, Peltier SJ, Petersen SE, Riedl V, Rombouts SA, Rypma B, Schlaggar BL, Schmidt S, Seidler RD, Siegle GJ, Sorg C, Teng GJ, Veijola J, Villringer A, Walter M, Wang L, Weng XC, Whitfield-Gabrieli S, Williamson P, Windischberger C, Zang YF, Zhang HY, Castellanos FX, Milham MP. Toward discovery science of human brain function. Proc Natl Acad Sci U S A. 2010;107:4734–9.
Smith SM, Beckmann CF, Andersson J, Auerbach EJ, Bijsterbosch J, Douaud G, Duff E, Feinberg DA, Griffanti L, Harms MP, Kelly M, Laumann T, Miller KL, Moeller S, Petersen S, Power J, Salimi-Khorshidi G, Snyder AZ, Vu AT, Woolrich MW, Xu J, Yacoub E, Uğurbil K, Van Essen DC, Glasser MF; WU-Minn HCP Consortium. Resting-state fMRI in the human connectome project. Neuroimage. 2013;80:144–68.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Sorg, C., Göttler, J. & Zimmer, C. Imaging Neurodegeneration: Steps Toward Brain Network-Based Pathophysiology and Its Potential for Multi-modal Imaging Diagnostics. Clin Neuroradiol 25 (Suppl 2), 177–181 (2015). https://doi.org/10.1007/s00062-015-0438-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00062-015-0438-3