
Abstract
Objectives
Due to a lack of longitudinal studies on health in immigrants, the purpose of the present study is to investigate trajectories of health-related quality of life (HRQoL) in immigrants and non-immigrants in Germany by considering the impact of immigration-related factors.
Methods
Based on longitudinal SOEP data from 2002 to 2012, the trajectories of the mental (MCS) and physical component (PCS) of HRQoL (assessed with SF-12v2) were analyzed in 8546 subjects, including 1064 immigrants by conducting hierarchical linear models.
Results
MCS remains stable over time, whereas PCS shows a decrease, influenced by increasing age. There were no differences between immigrants and non-immigrants concerning PCS trajectories as well as no influence of immigration-related factors on it. In contrast, MCS trajectories were influenced by immigration-related factors: 2nd-generation immigrants, participants from Turkey or Southern Europe and those who immigrated at young age show a slight decrease in MCS over time.
Conclusions
The results show negative association between MCS and time in different groups of immigrants. Future research is needed for better conceptualization of the complex interplay between health and migration over time to identify subgroups at greater risk for mental distress.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
One of the most controversially discussed issues western high-income countries are currently dealing with is best described by immigration processes and its consequences in different areas of public life in these host countries. Consequently, in the last decades immigration has become an important topic of public health and social development, especially in the European countries (Westphal 2016; Schenk 2007; Brzoska et al. 2015). Germany, being described as the main destination within Europe (Federal Office for Migration and Refugees 2016) is a case in point. In 2016, more than one-fifth (18.6 million; 22.5%) of the general population in Germany were persons with a migration background, including immigrants of the 1st generation (two-thirds of all immigrants) as well as German-born individuals with at least one parent who immigrated to Germany, so-called 2nd-generation immigrants (Federal Statistics 2017a). In general, immigrants in Germany are younger than natives, they live less often without a partner, are more likely to be unemployed, and more than half of them are born in or live over 20 years in Germany (Federal Statistics 2017a).
The relationship between immigration as a multidimensional, critical life event with long-term consequences and mental as well as physical health outcomes has been demonstrated in numerous studies (e.g., Bhugra et al. 2014; Nesterko et al. 2013; Glaesmer et al. 2011). There is consensus that experiences caused by migration have an impact on health status, even though direction, type and intensity of this relationship remain unanswered up to now (Glaesmer et al. 2011). Some studies found that immigrants enjoy better or similar health compared to the native population (Glaesmer et al. 2011; Razum and Zeeb 2004), whereas other studies reported worse health status among different immigrant groups (Beutel et al. 2016; Brzoska et al. 2015). So the findings are often contradictory, which is mainly attributable to the characteristics of the sample from which the data has been collected, the methods which were used, as well as the outcome variables which were analyzed (Nesterko et al. 2013). Accordingly, there are different theoretical approaches addressing the relationship between health and immigration-related processes. The idea of positive selection of immigrants before the immigration, best described by the so-called healthy migrant effect (Razum et al. 1998), was widely supported in studies from different host countries (e.g., in Europe—Rivera et al. 2016; Wengler 2013; in USA—Argeseanu et al. 2008; in Canada—Vang et al. 2015; and in Australia—Biddle et al. 2007) showing better health and lower mortality among immigrants compared to natives. Thus, individuals who are more vigorous and less affected by health problems are more likely to migrate (Westphal 2016). On the other hand, it was shown that such health advantages among immigrants decrease over time (Westphal 2016). In addition, a possible source of bias is unregistered return migration, causing underestimation of mortality rates among immigrants, which may also affect the results supporting the “healthy migrant effect” (Turra and Elo 2008). Focussing on immigration as a long-term process and its impact on health over time, the “double jeopardy hypothesis” (Down and Bengston 1978) might be of interest. The hypothesis states that age-related health disadvantages are cumulatively compounded by minority status: elderly immigrants might be at double risk to become ill. Because of a lack of longitudinal data from immigrant populations, the empirical evidence for the “double jeopardy hypothesis” is mixed and fragmental (Carreon and Noymer 2011). However, some studies support the assumption of increased health risks in elderly immigrants due to double stigmatization (Carreon and Noymer 2011; Wengler 2013), some other found no evidence for the interaction between higher age and minority status over time (Ferraro and Farmer 1996). According to the assumption that immigrants are a quite heterogeneous group, a theoretical concept for the examination of the complex interplay between health status and immigration process addressing immigrations-related characteristics in more detail was suggested by Schenk (2007). In her model, three levels of investigations are proposed: On the population-based level (level I), comparisons between immigrants and natives are of interest. More detailed exploration of the impact of immigration is defined by contrasting different groups of immigrants, e.g., by comparing one homogenous group with one or more other homogenous group or groups of immigrants living in the same host country (level II). On this level, immigration-related characteristics such as age at immigration, length of stay or country/region of origin are examined to characterize different groups of immigrants. Moreover, the country of origin is the basis for comparisons within homogeneous groups of immigrants (level III). On this level, comparisons of samples from the same country of origin or of samples from the same country of origin, but from different host countries, are of specific interest. The vast majority of evidence on health status in immigrants in different host countries is based on level I and/or level II analyses almost always analyzing cross-sectional data. As far as we know there has only been little research examining health status in immigrants on level I and/or level II using longitudinal data.
In their population-based, longitudinal study investigating HRQoL in children and adolescents (aged 11–17 years) in Germany, Otto et al. (2017) demonstrated that immigration status was related to lower HRQoL at baseline, and there was no significant interaction with time. Browne et al. (2017) investigated emotional problems among immigrants in Canada 6 months after arrival and followed them up two and 4 years later showing refugee status, female gender, lower income and visible minority status as predictors for higher levels of emotional problems over time. Based on longitudinal survey data, Montazer and Wheaton (2017) showed an increase in distress over time among immigrants in Canada from lower national product origin countries for the first 5 years after arrival, followed by a decline among all immigrants, regardless of their country of origin. Looking at the demographic changes caused by rising numbers of immigrants in different western countries, this limited empirical evidence underlines the need for research on the possible interplay between immigration-related factors and health status prospectively. Thus, the present study compares HRQoL in immigrants and non-immigrants in Germany (level I analysis) and investigates the impact of immigration-related factors as suspected determinants of trajectories of HRQoL in immigrants (level II analyses) in a longitudinal population-based survey in Germany in six two-year interval assessments between 2002 and 2012. The following questions guide the research presented below:
-
1.
Are there differences in the trajectories of HRQoL between immigrants and non-immigrants living in Germany?
-
2.
Are there influences of immigration-related factors—age at immigration and country/region of origin—on trajectories of HRQoL of immigrants in Germany?
Methods
Dataset and study population
Our analyses are based on a dataset from the German Socio-Economic Panel (SOEP), a representative longitudinal study of private households of the German general population carried out by the German Institute for Economic Research (Wagner et al. 2007). Each year since 1984 around 14,000 households and about 30,000 individuals have been surveyed by the SOEP’s fieldwork organization (Kroh et al. 2015). In every first survey wave a face-to-face interview with the participants was conducted by trained interviewers, and for each following survey year the participants completed the questionnaire independently in a paper–pencil or computer-based version. Detailed information on response rates and survey stability for each year is reported by Britzke and Schupp (2016). For our analyses we compiled a dataset out of the SOEP-Health Survey collected in 2-year time intervals from 2002 to 2012 including HRQoL as one key variable. Moreover, this dataset includes socio-demographic information as well as immigration-related characteristics such as age at immigration and country/region of origin. Between 2002 and 2012, data of 9611 (100%) individuals about their health status was available. A total of 8546 subjects (52.5% female; aged between 17 and 92 years at baseline) completed the self-rating questionnaire about their HRQoL each survey wave. Immigration status was assessed according to the recommendations of Schenk (2007), including information about country of origin, year of immigration to Germany, the legal status of the participants as well as their parents. For our analyses we differentiated between immigrants of the 1st and the 2nd generation and non-immigrants (German natives) and created an algorithm for each group. All participants who immigrated to Germany after 1949 are classified as 1st-generation immigrants. All those who reported being born in Germany and having at least one parent who immigrated to Germany after 1949 are classified as 2nd-generation immigrants. Based on this algorithm, we classified 1064 subjects (12.4% of the sample) as immigrants, of which 754 (8.8%) were of the 1st generation and 310 (3.6%) of the 2nd generation. Because of the heterogeneity of the 1st-generation immigrant sample due to their country of origin, which consequently leads to small subgroup sizes, we merged participants to groups of geographic regions (Table 1), with exception of participants from Turkey and Poland.
Measures
HRQoL was measured with SF-12v2—SOEP version. The SF-12 was constructed as a short version of SF-36 Health Survey, reflecting the physical (PCS) and mental (MCS) component summaries of the original scale (Daig and Lehmann 2007). The SF-12v2 consists of 12 items. It has been validated in a number of countries and several languages (Daig und Lehmann 2007). The validation of SF-12v2 in a representative sample of the German population is based on SOEP data from 2004 (Nübling et al. 2006). To calculate PCS-12 and MCS-12 scores, the items (PCS: two items for physical fitness and for role physical each, one item for general health and for bodily pain each; MCS: two items for mental health and for role emotional each, one item for social functioning and vitality with each) are scored and normalized via a standardized algorithm. The scores range from 0 to 100 (with a mean score of 50 and a standard deviation of 10), with higher scores indicating better functioning (Nübling et al. 2006).
Analytic plan and statistics
The objectives of the present study were to analyze the trajectories of HRQoL in a representative German general population sample with a specific focus on immigrant populations between 2002 and 2012. Longitudinal hierarchical linear modeling (HLM, Bryk and Raudenbush 1992) was employed to investigate changes in HRQoL scores for non-immigrants, the 1st- and the 2nd-generation immigrants. To examine the first research question, two-level HLMs, separate for MCS and PCS, were used with level 1 time (from assessment 1(2002) to assessment 6 (2012) reflecting intraindividual changes), and level 2 individual [e.g., age (grand mean centering at baseline, according to Field et al. 2012), gender, and immigration status/generation at baseline reflecting interindividual changes]. The models were used as follows, with MCS as an example:
with MCS = mental component of HRQoL, T = time, G = gender, A = age, ImS = immigration status.
When analyzing the second research question, two-level HLMs, separate for MCS and PCS were used with level 1 time (assessment 1 (2002)–6 (2012) reflecting intraindividual changes), and level 2 individual (age (grand mean centering at baseline, according to Field et al. 2012), gender, and immigration-related factor, separate models for (1) country/region of origin and (2) age at the immigration at baseline reflecting interindividual changes). The models used as follows with MCS and CoO as an example:
with MCS = mental component of HRQoL, T = time, G = gender, A = age, CoO = country of Origin.
Before proceeding with detailed analyses described above, we ran an empty model when predicting HRQoL (the effects of age and gender not included) to confirm the justification for two-level HLM modeling using intraclass correlation (Hosoya et al. 2014), \(ICC =\sigma^{2}_{{\nu0}} / \, (\sigma^{2}_{{\nu0}} +\sigma^{2}_{\varepsilon} )\) within the model:
For MCS, level 1 variance (intrapersonal changes) was \(\sigma^{2}_{\varepsilon} = \, 50.99\) and level 2 variance (interpersonal changes) \(\sigma^{2}_{{\nu0}} = \, 44.59\), the ICC was .47, which justified 2-level HLM for MCS. For PCS, level 1 variance (intrapersonal changes) was \(\sigma^{2}_{\varepsilon} = \, 34.21\) and level 2 variance (interpersonal changes) \(\sigma^{2}_{{\nu0}} = \, 59.60\), the ICC was .635, which justified two-level HLM for PCS.
Data were analyzed using SPSS Version 20 and R 1.2.3.
Results
Descriptive and immigration-related characteristics
Descriptive statistics of the sample including immigration-related characteristics of the 1st- and 2nd-generation immigrants are shown in Table 1. The vast majority of immigrants (70.9%) are 1st-generation immigrants. In 2002, about half of them (48.2%) had been living in Germany for more than 20 years, 35.1% of them came to Germany under the age of 18 years, 16.2% of 1st-generation immigrants were originally from Turkey, 17.1% came from the Former Soviet Union (FSU), 20.8% were from other Eastern European countries.
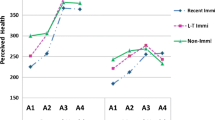
Mental (MCS) as well as physical (PCS) components of HRQoL were measured in two-year intervals from 2002 to 2012, resulting in 6 assessments. The mean scores of MSC and PCS for German natives, 1st- and 2nd-generation immigrants are displayed in Fig. 1.

Mean scores for mental (MCS) and physical (PCS) components of health-related quality of life of German natives, 1st- and 2nd-generation immigrants between 2002 and 2012 in Germany
Both the MCS and PCS scores of HRQoL were found to be within the mean range of the measurement scales in all three groups. Non-immigrant participants showed constant values over time in MCS, whereas a slight decrease was observed in the 1st- and 2nd-generation immigrants. All groups showed similar baseline values of MCS. With PCS, a decrease was observed over time for all three groups, but the baseline levels were different for each group with higher level for 2nd-generation immigrants and lower level for 1st-generation immigrants compared to non-immigrants.
Differences between German natives and immigrants in HRQoL over time
The results of HLMs testing Time and Immigration Status as predictors for MCS and PCS are displayed in Table 2. For MCS, there were no differences between non-immigrants and 1st-generation immigrants, although significant differences between 2nd-generation immigrants and non-immigrants (higher scores for 2nd-generation immigrants) were found at baseline. In addition, a significant interaction between time and 2nd-generation immigrants was found. This indicates a decrease in MCS in this group of immigrants over time.
For PCS, differences between 1st-generation immigrants and non-immigrants were found with higher scores for non-immigrants at baseline. However, there were no differences between immigrants of the 2nd generation and non-immigrants as well as no significant interactions of immigration status with Time.
Impact of immigration-related factors on HRQoL in immigrants over time
Country/region of origin
When testing the impact of country/region of origin on HRQoL, data of six participants with invalid information about their origin were excluded. In addition, the group of participants of countries “other” (N = 59) was also excluded from the analysis because of heterogeneity within the group. The model was ran with N = 8481 participants. The results are presented in Table 3.
For MCS, there were differences between immigrants from the FSU and non-immigrants only, with higher rates for immigrants from the FSU at baseline. Significant interactions were found between Time and Turkish immigrants as well as Time and immigrants from Southern European countries, indicating a decrease in MCS in both groups over time. For PCS, immigrants from Turkey, Poland and other Eastern European countries reported lower scores compared to non-immigrants at baseline. There were no significant interactions in PCS scores between country/region of origin and Time.
Age at immigration
Data from 36 participants were excluded from the analysis due to invalid information about age at immigration. The results of the model testing the impact of the age at the immigration on HRQoL are displayed in Table 4.
For MCS, there were differences between non-immigrants and immigrants who came to Germany between the age of 13 and 19 years with higher scores for immigrants at baseline. In addition, significant interaction between this group of immigrants and Time was found, indicating MCS decrease over time. For PCS, immigrants who came to Germany between the age of 13 and 19 years as well as between 20 and 30 years reported lower scores compared to non-immigrants at baseline. There were no significant interactions in PCS scores between age at the immigration and Time.
Discussion
Using a population-based approach, in the present study trajectories of HRQoL across 10 years were analyzed in immigrants of the 1st and 2nd generation as well as in non-immigrants in Germany. In addition, the impacts of immigration-related characteristics such as age at immigration and country/region of origin on HRQoL were investigated.
Concerning the total sample, the findings indicate a decrease of physical health status on the one hand, and stability of mental health status on the other hand, which is in line with previous research (Ellert and Kurth 2013; Nesterko et al. 2013). However, there are differences between immigrants and non-immigrants for mental as well as physical HRQoL at baseline: immigrants of the 2nd generation show higher mental health scores compared to both non-immigrants and the 1st-generation immigrants; and immigrants of the 1st generation show lower physical health scores compared to both non-immigrants and the 2nd-generation immigrants. Higher levels of mental health in the 2nd-generation compared to the 1st-generation immigrants were also shown in some recently published studies (Beutel et al. 2016; Liddell et al. 2016) indicating higher level of acculturation in terms of better language skills, more frequent contacts with native peers and/or less proportion of unemployed participants of the 2nd-generation compared to 1st-generation immigrants. Lower levels of physical health status in the 1st-generation immigrants might be explained by usually adverse, low-income working conditions or employment situation of this group in Germany during the last 30 years (Seifert 1997). Regarding the trajectories of physical HRQoL, the results indicate no differences between immigrants and non-immigrants. Moreover, age was the best predictor for physical health trajectories in all three groups. Looking at the trajectories of mental health status, a stronger decrease was found for immigrants of the 2nd-generation immigrants. Due to the higher rates at baseline and younger age compared to 1st-generation immigrants and non-immigrants, we assume that 2nd-generation immigrants as a group of immigrants “in-between” (higher level of acculturation within the native majority and close connections to the community of origin at the same time) might be the group of higher negative impact of political and economic changes during the observed period of time. Some of these challenges can be seen as a result of intensified public debates about differences between cultural, ethnic and religious groups in pluralistic western societies and in its consequence by increased expectations on integration efforts of immigrants on the one hand and rising rates on perceived discrimination on the other hand (Decker et al. 2016). In future research, these possible interpretations should be investigated in more detail as well as in collaboration with experts from other fields, e.g., economists, political scientists.
Consequently and with respect to a possible theoretical framework describing the interplay of health status and immigration mentioned in the introduction section, there is also no evidence for “healthy migrant effect” as for “double jeopardy hypothesis” according to the data analyzed in the present study.
For a more detailed examination of possible immigration-related influences on health status, HLMs predicting trajectories of HRQoL by country/region of origin and age at immigration were run. There are differences within immigrants of different origins with respect to mental as well as physical health at baseline: whereas immigrants from the FSU reported higher scores on mental health compared to non-immigrants and other immigrant groups, immigrants from Turkey, Poland and other Eastern European countries reported lower scores on physical HRQoL compared to non-immigrants and immigrants of another origin. Higher levels of mental health in participants from the FSU might be related to general reservation with respect to mental health care services and in consequence much stronger societal taboo due to mental health disorders being often reported for Russian speaking immigrants in previous research (Ditte et al. 2006). Worse physical health in Turkish, Polish and immigrants from other Eastern European countries verify lower scores for physical health in 1st-generation immigrants, which is likely to be related to mostly adverse employment situations as result of labor immigration waves to Germany during the 1960s (Seifert 1997). In addition, the results indicate a decrease in mental health status over time for Turkish immigrants and immigrants from Southern European countries, including Italy, Greece, Spain and Portugal—the great majority of labor immigrants who came to Germany in 1960s–1970s. Rather unexpected results in mental and physical health scores were found when testing the impact of age at immigration: compared to non-immigrants and other immigrants, participants who immigrated to Germany at the age of 13–19 years reported higher mental health on the one hand and lower physical health on the other hand. Moreover, there was a decrease in mental health status, whereas no significant changes were found for physical health in this immigrant group. Thus, as mentioned in previous cross-sectional research (Glaesmer et al. 2011; Nesterko et al. 2013), the results of this study suggest that immigration-related factors like country/region of origin or age at immigration seem to be important determinants of HRQoL among immigrants.
Although the present study has some major strengths (e.g., population-based approach, large sample size, longitudinal design, inclusion of immigration-related factors), some limitations of this approach should be mentioned. First, the dataset is supposed to be representative for the German general population, but the proportion of immigrants is in fact lower than in the general population of Germany (12.4. vs. 19.2% in 2012, Federal Statistics 2017b). Moreover, this study includes mainly immigrants with good German language skills who have been living in Germany for years or since their birth, which leads to an underrepresentation of refugee populations or of regular immigrants who have recently arrived and/or are unable to speak and understand German. Thus, the interpretation of the presented results may not be generalizable to all immigrants, particularly with regard to groups in greater need of psychosocial support. Secondly, some important socio-demographic as well as immigration-related characteristics were not considered. For example, we did not control for socio-economic status or perceived discrimination as well-known predictors of HRQoL because of invalid and/or inconsistent data. Third, when using HLM for modeling longitudinal trajectories, only linear functions were assumed. Future research is needed to test alternative trajectory mapping (e.g., quadratic and/or cubic functions). Nevertheless, our study, as far as we know, represents the first population-based longitudinal study including a large and heterogeneous sample of immigrants.
To sum up, some conclusions from this longitudinal study should be drawn. First, focusing on HRQoL trajectories, additional attention should be paid to the mental component, especially in immigrants of the 2nd generation. Second, in the light of the methodological limitations of the present study, the impact of immigration-related characteristics should be studied in more detail in future research for better identification of specific subgroups of immigrants with decreased HRQoL. Third, when analyzing long-term effects of immigration processes having impact on health status, more specific theoretical conceptualization of the complex interplay between immigration and health is needed in the future. Finally, there is an urgent need for research focusing on possible clinical implications and/or health care services targeting different groups of immigrants.
Abbreviations
- HRQoL:
-
Health-related quality of life
- MCS:
-
Mental health component summary scale of the SF-12v2
- PCS:
-
Physical health component summary scale of the SF-12v2
- SOEP:
-
Socio-Economic Panel
- FSU:
-
Former Soviet Union
References
Argeseanu CS, Ruben JD, Narayan KMV (2008) Health of foreign-born people in the United States: a review. Health Place 14:623–635
Beutel ME, Jünger C, Klein EM et al (2016) Depression, anxiety and suicidal ideation among 1(st) and 2(nd) generation migrants—results from the Gutenberg health study. BMC Psychiatry 16:288
Bhugra D, Gupta S, Schouler-Ocak M et al (2014) EPA guidance mental health care of migrants. Eur Psychiatry 29:107–115
Biddle N, Kennedy S, McDonald JT (2007) Health assimilation patterns amongst Australian immigrants. Econ Rec 83:16–30
Britzke J, Schupp J (2016) SOEP wave report 2016. https://www.diw.de/documents/publikationen/73/diw_01.c, 560446. Accessed 18 April 2018
Browne DT, Kumar A, Puente-Duran A et al (2017) Emotional problems among recent immigrants and parenting status: findings from a national longitudinal study of immigrants in Canada. PLoS ONE 12:1–14
Bryk A, Raudenbush SW (1992) Hierarchical linear models for social and behavioral research: applications and data analysis methods. Sage, Newbury Park
Brzoska P, Ellert U, Kimil A, Razum O, Sass A-C, Salman R, Zeeb H (2015) Reviewing the topic of migration and health as a new national health target for Germany. Int J Public Helath 60:13–20
Carreon D, Noymer A (2011) Health-related quality of life in older adults: testing the double jeopardy hypothesis. J Aging Stud 25:371–379
Daig I, Lehmann A (2007) Verfahren zur Messung der Lebensqualität. Zeitschrift für Medizinische Psychologie 16:5–23
Decker O, Kiess J, Braehler E (2016) Die enthemmte Mitte. Autoritäre und rechtsextreme Einstellung in Deutschland. Die Leipziger Mitte-Studie 49–58
Ditte D, Schulz W, Schmid-Ott G (2006) Einstellung gegenüber der Psychotherapie in der russischen Bevölkerung und in der Bevölkerung mit einem russischen/sowjetischen kulturellen Hintergrund in Deutschland. Eine Pilotstudie. Der Nervenarzt 77:64–72
Dowd JJ, Bengtson VL (1978) Aging in minority populations: an examination of the double jeopardy hypothesis. J Gerontol 33:427–436
Ellert U, Kurth BM (2013) Gesundheitsbezogene Lebensqualität bei Erwachsenen in Deutschland: ergebnisse der Studie zur Gesundheit Erwachsener in Deutschland (DEGS1). Bundesgesundheitsblatt, Gesundheitsforschung, Gesundheitsschutz 56:643–649
Federal Office for Migration and Refugees (BAMF) (2016) Migration report 2015. http://www.bamf.de/SharedDocs/Anlagen/EN/Publikationen/Migrationsberichte/migrationsbericht-2015-zentrale-ergebnisse.pdf?__blob=publicationFile. Accessed 7 December 2017
Federal Statistics (2017a) Migration report 2016. https://www.destatis.de/DE/Publikationen/Thematisch/Bevoelkerung/MigrationIntegration/Migrationshintergrund2010220167004.pdf?__blob=publicationFile. Accessed 18 April 2018
Federal Statistics (2017) Migration report 2012. https://www.destatis.de/DE/Publikationen/Thematisch/Bevoelkerung/MigrationIntegration/Migrationshintergrund2010220127004.pdf?__blob=publicationFile. Assessed 19 April 2018
Ferraro KF, Farmer MM (1996) Double jeopardy to health hypothesis for African Americans: analysis and critique. J Health Soc Behav 37:27–43
Field A, Miles J, Field Z (2012) Discovering statistics using R. Sage publications, Thousand Oaks
Glaesmer H, Witting U, Braehler E et al (2011) Health care utilisation of first and second generation immigrants and the native population—a population based study in Germany. Int J Public Health 56:541–548
Hosoya G, Koch T, Eid M (2014) Längsschnittdaten und Mehrebenenanalyse. Kölner Zeitschrift für Soziologie und Sozialpsychologie 66:189–218
Kroh M, Siegers R, Kühne S (2015) Gewichtung und Integration von Auffrischungsstichproben am Beispiel des Sozio-oekonomischen Panels (SOEP). Nonresponse Bias. Springer, Wiesbaden, pp 409–444
Liddell BJ, Nickerson A, Sartor L et al (2016) The generational gap: mental disorder prevalence and disability amongst first and second generation immigrants in Australia. J Psychiatr Res 83:103–111
Montazer S, Wheaton B (2017) Economic conditions in countries of origin and trajectories in distress after migration to canada: results from the national population health survey. Soc Ment Health 7:1–20
Nesterko Y, Braehler E, Grande G et al (2013) Life satisfaction and health-related quality of life in immigrants and native-born Germans: the role of immigration-related factors. Qual Life Res 22:1005–1013
Nübling M, Andersen HH, Mühlbacher A (2006) Entwicklung eines Verfahrens zur Berechnung der körperlichen und psychischen Summenskalen auf Basis der SOEP–Version des SF-12 (Algorithmus). Deutsches Institut für Wirtschaftsforschung. Data Documentation 16. https://www.diw.de/documents/publikationen/73/diw_01.c.44987.de/diw_datadoc_2006-016.pdf. Accessed 7 Dec 2017
Otto C, Haller AC, Klasen F (2017) Risk and protective factors of health-related quality of life in children and adolescents: results of the longitudinal BELLA study. PLoS ONE 12:1–17
Razum O, Zeeb H (2004) Inequity, acculturation and the „Mediterranean paradox”. Int J Epidemiol 33:1411–1412
Razum O, Zeeb H, Akgün HS et al (1998) Low overall mortality of Turkish residents in Germany persists and extends into a second generation: merely a healthy migrant effect? Trop Med Int Health 3:297–303
Rivera B, Casal B, Currais L (2016) The healthy immigrant effect on mental health: determinants and implications for mental health policy in Spain. Adm Policy Ment Health 43:616–627
Schenk L (2007) Migration und Gesundheit- Entwicklung eines Erklärungs- und Analysemodells für epidemiologische Studien. Int JPublic Health 52:87–96
Seifert W (1997) Occupational and economic mobility and social integration of Mediterranean migrants in Germany. Eur J Popul 13:1–16
Turra CM, Elo IT (2008) The impact of salmon bias on the Hispanic mortality advantage: new evidence from social security data. Popul Res Policy Rev 27:515–530
Vang Z, Sigouin J, Flenon A et al (2015) The healthy immigrant effect in Canada: a systematic review. Population Change and lifecourse strategic knowledge cluster discussion paper series volume 3: issue 1, article 4. http://ir.lib.uwo.ca/pclc/vol3/iss1/4. Accessed 7 Dec 2017
Wagner GG, Frick J, Schupp J (2007) The German socio-economic panel study (SOEP)—scope, evolution and enhancements. Schmollers Jahrbuch J Appl Soc Sci Stud 127:139–169
Wengler A (2013) Ungleiche Gesundheit. Zur Situation türkischer Migranten in Deutschland. Campus Verlag, Frankfurt
Westphal C (2016) Healthy migrants? Health selection of internal migrants in Germany. Eur J Popul 32:703–730
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Ethical statements
As our study has involved only a secondary analysis of anonymized data, an ethics approval was not required. Detailed information on ethical clearance and informed consent given by the participants can be found on Research Infrastructure “Socio-Economic Panel (SOEP) via internet (https://www.diw.de/soep).
Additional information
This article is part of the special issue “Environmental and health equity”.
Rights and permissions
About this article

Cite this article
Nesterko, Y., Turrión, C.M., Friedrich, M. et al. Trajectories of health-related quality of life in immigrants and non-immigrants in Germany: a population-based longitudinal study. Int J Public Health 64, 49–58 (2019). https://doi.org/10.1007/s00038-018-1113-7
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00038-018-1113-7