
Abstract
Background: It is unknown whether fluid resuscitation with colloid or crystalloid in patients with severe sepsis or septic shock is associated with an improvement in clinical outcome. This randomized controlled trial determined the feasibility of conducting a large trial testing resuscitation with pentastarchvs normal saline in early septic shock, powered for a difference in mortality.
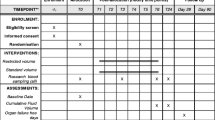
Methods: At three Canadian and one New Zealand academic centre, 40 patients with early septic shock defined by at least two systemic inflammatory response syndrome criteria, infectious source, and persistent hypotension after ≥ 1 L of crystalloid fluid were recruited. Feasibility measures were patient recruitment, blinding of the study fluids, and acceptability of the goal directed algorithms. Boluses of blinded normal saline or pentastarch (500 mL − maximum 3 L or 28 mL·kg−1) were administered within goal directed care for the first 12 hr.
Results: Of 161 patients screened, 121 were excluded and 40 patients were enrolled, for a recruitment rate of 0.75 patients/ site/month. Only 57% of physicians and 54% of nurses correctly guessed the study fluid (P = 0.46 andP = 0.67, respectively). The goal directed algorithms were acceptable to 97% of physicians.
Conclusion: The ability to recruit patients in this pilot randomized controlled trial was below expectations. Blinding of study fluids was adequate, and resuscitation algorithms were acceptable to most physicians. Methods to improve recruitment are required to enhance the feasibility of conducting a multicentre fluid resuscitation trial in early septic shock.
Résumé
Contexte: Nous ne savons pas si la réanimation liquidienne avec des colloïdes ou des cristalloïdes chez les patients présentant un sepsis grave ou un choc septique est associée à un devenir clinique meilleur. Cette étude randomisée contrôlée a déterminé la faisabilité d’une étude d’envergure testant la réanimation avec le pentastarch par rapport au sérum physiologique en début de choc septique, avec pour objectif primaire de détecter une différence dans les taux de mortalité.
Methode: Quarante patients en début de choc septique, défini comme au moins deux critères du syndrome de réaction inflammatoire, une source d’infection et une hypotension persistante après ≥ 1 L de cristalloïde ont été recrutés dans trois centres universitaires canadiens et un centre néo-zélandais. Les mesures de faisabilite étaient: le recrutement des patients, le masquage des liquides à l’étude, et I’acceptabilité des algorithmes dirigés vers des objectifs. Des bolus de normal sal in ou de pentastarch (500 mL — maximum 3 L ou 28 mL·kg−1) ont été administrés en aveugle dans le cadre de soins guidés dirigés vers des objectifs durant les 12 premieres heures.
Resultats: Sur 161 patients dépistés, 121 ont été exclus et 40 patients recrutés dans le cadre de I’étude, avec un taux de recrutement de 0,75 patient/site/mois. Seulement 57 % des médecins et 54 % des infirmières ont réussi à deviner correctement le type de liquide à I’étude (P = 0,46 etP = 0,67, respectivement). Les algorithmes ont été jugés acceptables par 97 % des médecins.
Conclusion: La capacité à recruter des patients pour cette étude pilote randomisée contrôlée était moins importante qu’attendue. Le masquage des liquides était satisfaisant, et les algorithmes de réanimation ont été jugés acceptables par la majorité des médecins. Des méthodes dans le but d’améliorer le recrutement sont nécessaire pour accroître la faisabilité d’une étude multicentrique sur la réanimation liquidienne en début de choc septique.
Article PDF
Similar content being viewed by others


Avoid common mistakes on your manuscript.
References
Marik PE, Varon J. Sepsis: state of the art. Dis Mon 2001; 47: 465–532.
Hollenberg SM, Ahrens TS, Annane D, et al. Practice parameters for hemodynamic support of sepsis in adult patients: 2004 update. Crit Care Med 2004; 32: 1928–48.
Vincent JL, Gerlach H. Fluid resuscitation in severe sepsis and septic shock: an evidence-based review. Crit Care Med 2004; 32(11 Suppl): S451–4.
Finfer S, Bellomo R, Boyce N, et al. A comparison of albumin and saline for fluid resuscitation in the intensive care unit. N Engl J Med 2004; 350: 2247–56.
Brunkhorst F, Engel C, Bloos F, et al. Intensive insulin therapy and pentastarch resuscitation in severe sepsis. N Engl J Med 2008; 358: 125–39.
Marik PE, Iglesias J. Would the colloid detractors please sit down! Crit Care Med 2000; 28: 2652–4.
Vercueil A, Grocott MP, Mythen MG. Physiology, pharmacology, and rationale for colloid administration for the maintenance of effective hemodynamic stability in critically ill patients. Transfus Med Rev 2005; 19: 93–109.
Ernest D, Belzberg AS, Dodek PM. Distribution of normal saline and 5% albumin infusions in septic patients. Crit Care Med 1999; 27: 46–50.
Mcintyre L, Hebert PC, Ferguson D, et al. A survey of Canadian intensivists’ resuscitation practices in early septic shock. Crit Care 2007; 11: R74.
Weil MH, Henning RJ. New concepts in the diagnosis and fluid treatment of circulatory shock. Thirteenth Annual Becton, Dickinson and Company Oscar Schwidetsky Memorial Lecture. Anesth Analg 1979; 58: 124–32.
Vincent JL, Weil MH. Fluid challenge revisited. Crit Care Med 2006; 34: 1333–7.
Vincent JL, de Mendonca A, Cantmine F, et al. Use of the SOFA score to assess the incidence of organ dysfunction/failure in intensive care units: results of a multicenter, prospective study. Working group on «sepsis-related problems» of the European Society of Intensive Care Medicine. Crit Care Med 1998; 26: 1793–800.
Rivers E, Nguyen B, Havstad MA, et al. Early goal-directed therapy in the treatment of severe sepsis and septic shock. N Engl J Med 2001; 345: 1368–77.
Micbard F, Teboul JL. Predicting fluid responsiveness in ICU patients: a critical analysis of the evidence. Chest 2002; 121: 2000–8.
Bland RD, Clarke TL, Harden LB. Rapid infusion of sodium bicarbonate and albumin into high-risk premature infants soon after birth: a controlled, prospective trial. Am J. Obstet Gynecol 1976; 124: 263–7.
Ernest D, Hartman NG, Deane CP, Belzberg AS, Dodek PM. Reproducibility of plasma and extracellular fluid volume measurements in critically ill patients. J Nucl Med 1992; 33: 1468–71.
Dellinger RP, Carlet JM, Masur H, et al. Surviving sepsis campaign guidelines for management of severe sepsis and septic shock. Crit Care Med 2004; 32: 858–73.
Author information
Authors and Affiliations
Consortia
Corresponding author
Additional information
Sources of funding and conflicts of interest: Dr. McIntyre has received unrestricted funds from Bristol Myers Squibb and Edwards Life Sciences to conduct this trial. She has also received unrestricted funds from Abbott Laboratories.
Rights and permissions
About this article
Cite this article
McIntyre, L.A., Fergusson, D., Cook, D.J. et al. Fluid resuscitation in the management of early septic shock (FINESS): a randomized controlled feasibility trial. Can J Anesth 55, 819–826 (2008). https://doi.org/10.1007/BF03034053
Accepted:
Issue Date:
DOI: https://doi.org/10.1007/BF03034053