
Abstract
Purpose
Ideally, preoxygenation is performed using a tight fitting mask either by breathing normally for three to five minutes or with four to eight vital capacity (VC) breaths in 0.5 to one minute, but in practice leaks are frequent and sometimes unavoidable. This study was designed to determine which breathing method provided the best oxygenation in the presence of leak.
Methods
Twenty volunteers were instructed to breathe from a circle circuit supplied with 6 L·min-1 of fresh oxygen. Each subject was tested under four situations selected in random order: 1) normal breathing for three minutes without leak; 2) normal breathing for three minutes with a leak; 3) four VCs in 30 sec without a leak; and 4) four VCs in 30 sec with a leak. The leak was created by a piece of size 18 French nasogastric tube, 5 cm long, taped under the face mask. Inspired and expired O2 and CO2 were sampled at the nostrils.
Results
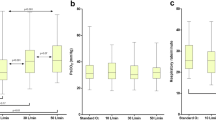
In the absence of a leak, the end-tidal oxygen fraction (FEO2) was greater after three minutes of tidal breathing (89 ± 3%; mean ± SD) in comparison with the response to four VCs (76 ± 7%; P < 0.001). Introduction of a leak decreased the FEO2 significantly (P < 0.001). With a leak, the FEO2 was similar with normal breathing (61 ± 8%) and after four VCs (59 ± 11%).
Conclusion
Preoxygenation with tidal volume breathing for three minutes yields higher FEO2 in comparison to four VCs. If a small leak (4 mm internal diameter) is introduced, the FEO2 decreases significantly with both breathing methods to approximately 60%.
Résumé
Objectif
Idéalement la préoxygénation est effectuée avec un masque étanche selon deux techniques; soit en respirant normalement pendant trois à cinq minutes ou en prenant quatre à huit respirations à capacité vitale (CV) en 0,5 à une minute. En pratique, les fuites sont fréquentes et quelquefois incontournables. Cette étude fut réalisée pour déterminer quelle méthode produit la meilleure préoxygénation en présence de fuite.
Méthode
Vingt volontaires ont respiré dans un circuit en cercle fournissant 6 L·min-1 ďoxygène frais. Chaque sujet fut soumis à quatre situations sélectionnées de façon aléatoire: 1) respiration normale pour trois minutes sans fuite; 2) respiration normale pour trois minutes avec fuite; 3) quatre CV en 30 sec sans fuite; 4) quatre CV en 30 sec avec fuite. La fuite a été créée avec un segment de tube nasogastrique de taille 18, long de 5 cm, fixé sous le masque. Les fractions inspirées et expirées ďO2 et de CO2 ont été mesurées aux narines.
Résultats
En ľabsence de fuite, la fraction expirée ďoxygène (FEO2) est plus grande avec trois minutes de respiration normale (89 ± 3%; moyenne ± ET) qu’avec quatre CV (76 ± 7%, P < 0,001). Avec une fuite, la FEO2 diminue significativement (P < 0,001). En présence ďune fuite, la FEO2 est la même avec respiration normale (61 ± 8%) qu’avec quatre respirations profondes (59 ± 11%).
Conclusion
Une préoxygénation avec respiration normale pour trois minutes donne une FEO2 plus élevée qu’avec quatre C V. Si une petite fuite (4 mm de diamètre interne) est présente, la FEO2 s’abaisse de façon significative à environ 60 % avec les deux méthodes de préoxygénation.
Article PDF
Similar content being viewed by others

Avoid common mistakes on your manuscript.
References
Drummond GB, Park GR. Arterial oxygen saturation before intubation of the trachea. An assessment of oxygenation techniques. Br J Anaesth 1984; 56: 987–93.
Baraka AS, Taha SK, Aouad MT, El-Khatib MF, Kawkabani NI. Preoxygenation. Comparison of maximal breathing and tidal volume breathing techniques. Anesthesiology 1999; 91: 612–6.
Nimmagadda U, Chiravuri SD, Salem MR, et al. Preoxygenation with tidal volume and deep breathing techniques: the impact of duration of breathing and fresh gas flow. Anesth Analg 2001; 92: 1337–41.
Dillon JB, Darsie ML. Oxygen for acute respiratory depression due to administration of thiopental sodium. JAMA 1955; 12: 1114–6.
Norris MC, Dewan DM. Preoxygenation for cesarean section: a comparison of two techniques. Anesthesiology 1985; 62: 827–9.
Valentine SJ, Marjot R, Monk CR. Preoxygenation in the elderly: a comparison of the four-maximal-breath and three-minute techniques. Anesth Analg 1990; 71: 516–9.
Gold MI, Duarte I, Muravchick S. Arterial oxygenation in conscious patients after 5 minutes and after 30 seconds of oxygen breathing. Anesth Analg 1981; 60: 313–5.
Goldberg ME, Norris MC, Larijani GE, Marr AT, Seltzer JL. Preoxygenation in the morbidly obese: a comparison of two techniques. Anesth Analg 1989; 68: 520–2.
Berthoud M, Read DH, Norman J. Pre-oxygenationhow long? Anaesthesia 1983; 38: 96–102.
Hamilton WK, Eastwood DW. A study of denitrogenation with some inhalation anesthetic systems. Anesthesiology 1955; 16: 861–7.
Russell GN, Smith CL, Snowdon SL, Bryson TH. Preoxygenation and the parturient patient. Anaesthesia 1987; 42: 346–51.
McGowan P, Skinner A. Preoxygenation—the importance of a good face mask seal. Br J Anaesth 1995; 75: 777–8.
Berry CB, Myles PS. Preoxygenation in healthy volunteers: a graph of oxygen “washin” using end-tidal oxygraphy. Br J Anaesth 1994; 72: 116–8.
Machlin HA, Myles PS, Berry CB, Butler PJ, Story DA, Heath BJ. End-tidal oxygen measurement compared with patient factor assessment for determining preoxygenation time. Anaesth Intensive Care 1993; 21: 409–13.
Grippi MA. Pulmonary Pathophysiology. Philadelphia: J.B. Lippincott Company; 1995.
Campbell IT, Beatty PC. Monitoring preoxygenation (Editorial). Br J Anaesth 1994; 72: 3–4.
Gambee AM, Hertzka RE, Fisher DM. Preoxygenation techniques: comparison of three minutes and four breaths. Anesth Analg 1987; 66: 468–70.
McCrory JW, Matthews JN. Comparison of four methods of preoxygenation. Br J Anaesth 1990; 64: 571–6.
McCarthy G, Elliott P, Mirakhur RK, McLoughlin C. A comparison of different pre-oxygenation techniques in the elderly. Anaesthesia 1991; 46: 824–7.
Hirsch J, Fuhrer I, Kuhly P, Schaffartzik W. Preoxygenation: a comparison of three different breathing systems. Br J Anaesth 2001; 87: 928–31.
Ooi R, Pattison J, Joshi P, Chung R, Soni N. Pre-oxygenation: the Hudson mask as an alternative technique. Anaesthesia 1992; 47: 974–6.
Author information
Authors and Affiliations
Corresponding author
Additional information
An erratum to this article is available at http://dx.doi.org/10.1007/BF03021640.
Rights and permissions
About this article
Cite this article
Gagnon, C., Fortier, LP. & Donati, F. When a leak is unavoidable, preoxygenation is equally ineffective with vital capacity or tidal volume breathing. Can J Anesth 53, 86–91 (2006). https://doi.org/10.1007/BF03021532
Accepted:
Issue Date:
DOI: https://doi.org/10.1007/BF03021532