
Abstract
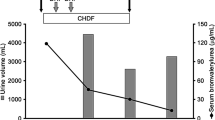
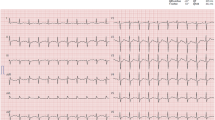
Two to twelve hours after suicidal ingestion of an estimated dose of 10 g chlorprothixene, a 31-year-old female was admitted to the emergency ward of the clinic with cardiorespiratory arrest. After successful resuscitation, the further clinical course was complicated by persistent ventricular extrasystoles and ventricular fibrillation which necessitated repeated defibrillation. Since the patient did not respond satisfactorily to supportive treatment, a combined hemoperfusion/hemodialysis was performed. Under extracorporeal detoxication, elimination of chlorprothixene from plasma was accompanied by substantial improvement of the patient's estimated dose had been removed. This case seems to indicate that evaluation of the therapeutic efficacy of hemoperfusion should not be based exclusively on the relation of the amount of the eliminated drug to total absorbed dose.
Article PDF
Similar content being viewed by others

Avoid common mistakes on your manuscript.
References
Baselt RC (1981) Disposition of drugs and chemicals in man. Biomedical Publications, Davis (CA), pp 173
Christensen H (1974) Chlorprothixene and its metabolites in blood, liver, and urine from fatal poisoning. Acta Pharmacol Toxicol 34:16
Crome P, Widdop B (1980) Resin hemoperfusion in tricyclic antidepressant poisoning. Lancet 1:306
Harms D, Singer H (1975) Vergiftungsbild und Therapie der Chlorprothixen-Intoxikation. Anästh Praxis 10:101
Raaflaub J (1975) On the pharmacokinetics of chlorprothixene in man. Experientia 31:557
Author information
Authors and Affiliations
Rights and permissions
About this article
Cite this article
Köppel, C., Schirop, T., Ibe, K. et al. Hemoperfusion in severe chlorprothixene overdose. Intensive Care Med 13, 358–360 (1987). https://doi.org/10.1007/BF00255795
Received:
Accepted:
Issue Date:
DOI: https://doi.org/10.1007/BF00255795