
Abstract
Heart failure (HF) is a structural or functional cardiac abnormal syndrome characterized with series of symptoms and signs such as breathlessness, fatigue, pulmonary crackles, and peripheral edema. Being a terminal phase of most myocardial lesions, HF has become a leading cause of mobility and mortality worldwide, associated with heavy clinical burden and economic costs affecting over 23 million people [14]. There is an increase to 5.5% with systolic dysfunction and an increase to 36.0% with diastolic dysfunction in people 60 years or older [85]. The costs accompanied with heart failure stand 2–3% of the total healthcare system expenditure in high-income countries and are expected to increase >2-fold in the next 2 decades [34].
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


1 Introduction
Heart failure (HF) is a structural or functional cardiac abnormal syndrome characterized with series of symptoms and signs such as breathlessness, fatigue, pulmonary crackles, and peripheral edema. Being a terminal phase of most myocardial lesions, HF has become a leading cause of mobility and mortality worldwide, associated with heavy clinical burden and economic costs affecting over 23 million people [14]. There is an increase to 5.5% with systolic dysfunction and an increase to 36.0% with diastolic dysfunction in people 60 years or older [85]. The costs accompanied with heart failure stand 2–3% of the total healthcare system expenditure in high-income countries and are expected to increase >2-fold in the next 2 decades [34].
The pathological mechanisms of HF include hemodynamic abnormalities, neuroendocrine cytokine system over-activation, bioenergetics defects, signal transduction pathway dysfunction, and abnormal calcium homeostasis [54]. In addition, oxidative stress and inflammatory disorders also contribute to the pathogenic process [58, 87]. HF is caused by multiple different etiologies; however, all causes have final common pathways, at least in part, independent of the original cause. Based on previous clinical trials of neurohormonal therapies, neurohormonal activation plays a pivotal role in its pathophysiology [56, 57]. Any cardiovascular diseases can cause cardiac injury; as a consequence, myocyte cells loss and the remaining myocytes become eccentric hypertrophy. Followed by neurohormonal activation, the left ventricle changes from elliptical to spherical and is characterized by functional mitral regurgitation. Afterward, left ventricular remodeling occurs with fibrosis and ventricular dilatation in which process myocardial oxygen consumption increases and myocardial contraction efficiency reduces [10, 69]. As the course progresses, concomitant renal dysfunction and gut congestion cause reduced response to diuretics and inflammatory activation, leading to worse outcomes [58, 84]. Existing therapies including angiotensin-converting enzyme (ACE) inhibitors, angiotensin receptor blockers (ARBs), β-blockers, mineralocorticoid receptor antagonists, and advanced device therapies provide symptomatic and clinical benefits; however, they do not completely solve the molecular abnormalities. Thus, it is urgent to find other effective therapeutic targets.
Recently, energetic impairment in the pathophysiology and progression of HF has caused lots of interest. Mitochondria accounts for 30% of the volume of cardiomyocytes whose dysfunction has been recognized as the key link in the development of heart failure [69]. Mitochondrial dysfunctions cover altered utilization of metabolic substrates, increased formation of reactive oxygen species, impaired mitochondrial electron transport chain activity, abnormal mitochondrial dynamics, and altered ion homeostasis [4]. In view of the above evidences, mitochondria appear to be the main target for direct improvement of cardiac function. Acetaldehyde dehydrogenase 2 (ALDH2) is firstly regarded as an alcohol metabolism enzyme, which mainly distributed in the mitochondria. Increasing evidences have supported its important cardioprotective role [44, 53, 61]. In the following review, we will summarize its beneficial role and novel insights in heart failure due to different etiologies, as well as the potential therapeutic measures.
2 Characteristics of ALDH2
Acetaldehyde dehydrogenase (ALDH) is an enzyme superfamily responsible for the catalytic oxidation of acetaldehyde to acetic acid both physiologically and pathologically [38]. It has been identified 19 isozymes till now. ALDH2 is the most active isozyme and its molecule form is a 56 kDa tetramer. The precursor protein of ALDH2 encodes from chromosome 12, enters the mitochondria under the guidance of the signal peptide, and cleaves off the signal peptide to locate in mitochondria [28]. ALDH2 is widely distributed in human liver, kidney, heart, lung, brain, and other tissues. It contains three domains including coenzyme-binding or NAD+-binding domain, catalytic domain, and oligomerization domain [61]. ALDH2 also processes three kinds of enzyme activities including dehydrogenase, esterase, and reductase activities detoxifying aldehyde, 4-nitrophenyl acetate, and nitroglycerin, respectively [55].
A total of 84 single nucleotide polymorphism (SNP) loci have been found on human ALDH2 gene [46]. The foremost is rs671 G > A mutation which presents in exon 12 and results in amino acid substitutions of p.Glu504Lys [74]. The genotypes of ALDH2 comprise wild homozygous (GG also known as ALDH2 *1/*1), owning normal catalytic activity of the enzyme; mutant heterozygous (GA also known as ALDH2 *1/*2), processing a decrease in enzyme catalytic activity with only 10%–45% of the wild homozygous; and mutant homozygotes (AA type also known as ALDH2 *2/*2) having only 1%–5% enzyme catalytic activity of the wild homozygous [15]. In general, the prevalence of the genetic polymorphism (ALDH2 *2/*2) is found in nearly 8% of world populations and 40% of East Asian population [103].
3 Beneficial Role and Mechanisms of ALDH2 in Heart Failure
Experimental and clinical studies have proved that ALDH2 plays a pivotal role in heart failure via maintaining cellular homeostasis [13, 17]. Evidences from our group and others have verified ALDH2 is closely related to various etiologies of heart failure, such as coronary artery disease (CAD) [80], hypertension [71], alcoholism [73], and other susceptibilities [102, 106]. Next we will review the pathological role and underlying mechanisms of ALDH2 involved in heart failure.
3.1 ALDH2 and Ischemic Heart Failure
Numerous studies have shown that ALDH2 has cardioprotective effects in ischemic with or without reperfusion myocardial injury. The expression of ALDH2 was found decreased in infarction border zone [90]. Cardiac function deteriorated in ALDH2 knockout posts myocardial infarction (MI) mice as evidenced by increased left ventricle (LV) cavity, LV end-diastolic pressure, and infarct size [80]. Meanwhile, there were more apoptotic cells in the non-infarcted LV region as compared with wild-type (WT) MI mice. In contrast, overexpression of ALDH2 in the heart could alleviate these injures. Ma, et al. found that ALDH2 induced autophagy during ischemia and inhibited autophagy during reperfusion which reduced hypoxic and reoxygenation cell death [53]. These data demonstrated that ALDH2 deficiency aggravated mitochondrial dysfunction and increased cardiomyocyte apoptotic cell death.
DNA methylation is a process adding methyl groups to cytosine residues into DNA sequences, which can prevent transcription factors from entering the gene regulatory region, thereby inhibiting gene transcription [65]. Increasing studies indicated that DNA methylation provided a potential molecular basis on energy metabolism between environmental and genetic factors interaction and might contribute to myocardial injury [40]. We also found DNA methylation at CpG sites (CpG1, CpG2, and CpG7) in the upstream sequence of ALDH2 promoter was upregulated post MI. These abnormal hypermethylations at the CpG sites downregulated ALDH2 enzyme activity and aggravated ischemic damages [90]. DNA methylation reflected the upstream mechanism of ALDH2 regulating cardiac function after ischemia.
We also demonstrated the downstream mechanisms of ALDH2 in protecting cardiac from ischemic injures. ALDH2 could increase the intracellular levels of 4-HNE, which could exacerbate apoptosis by inhibition of HSP70, phosphorylation of JNK, and activation of p53 [80]. 4-HNE is also a diffusible product of membrane lipid peroxidation and relates to oxidative stress-induced cell death [70]. Mitochondrial-derived ROS also attacked polyunsaturated fatty acids, leading to membrane lipid peroxidation, thereby increasing reactive aldehydes [7, 8]. We demonstrated both experimentally and clinically that ALDH2 was vital in regulating microenvironment homeostasis. ALDH2 could promote angiogenesis post chronic ischemia. ALDH2 deficiency inhibited tubelike construction formation of hypoxia endothelial cell through HIF-1α/VEGF pathway, deteriorating perfusion recovery in ischemia tissue, while overexpression of ALDH2 promoted angiogenesis. Furthermore, clinical data suggested that the dysfunction of ALDH2 due to gene variant was an unfavorable factor for revascularization in patients with chronic total occlusion (CTO). Therefore, targeting ALDH2 activity may be a potential therapeutic strategy for chronic ischemic heart failure, and we have used this achievement to guide clinical decision-making [49].
3.2 ALDH2 and Stress-Induced Heart Failure
Endoplasmic reticulum (ER) stress refers to an increase in unfolded and misfolded proteins in the ER that disrupts the homeostasis in response to cellular stressors, such as heat, hypoxia, metabolic starvation, angiotensin II, and tumor necrosis factor-α [29, 42]. Substantial evidences indicated ES stress as important target for the treatment of cardiovascular disease, including ischemia/reperfusion injury, atherosclerosis, cardiac hypertrophy, and heart failure [29, 82]. Our results suggested that ALDH2 deficiency aggravated cardiac contractile dysfunction following activation of ES stress, manifested as descend of ejection fraction and fractional shortening. NADPH oxidase (p47phox subunit) increased in ALDH2 knockout mice, suggesting that ALDH2 might regulate Akt signaling pathway through p47phox NADPH oxidase-dependent manner against ER stress and ER stress-induced apoptosis [47].
Persistent pressure overload such as refractory hypertension is a significant risk factor for heart failure and sudden death. Series of pathological cardiac remodeling were characterized by increased myocardial cells, “fetal gene program” activation, cytoskeletal reorganization, and irreversible systolic dysfunction [35, 51]. Autophagy is an important homeostatic pathway in degrading damaged proteins and intracellular organelles [24]. It has been found to be involved in pressure-induced heart failure [22]. Autophagy-related signaling pathways involved in pressure overload included the classic AMPK-mTOR-autophagy, Beclin-1-dependent pathway, Akt/mTOR/FoxO3a signal pathway, and PI3K/Akt signaling [48, 89, 96, 98]. In early compensated cardiac hypertrophy after transverse aortic constriction (TAC), autophagy played an adverse role with worse cardiac function and severer mitochondria damage. In this process, ALDH2 acted through the regulation of PI3K/PTEN/Akt signaling [95]. Besides, ALDH2 deficiency further inhibited autophagy during decompensated cardiac hypertrophy accompanied with inactive Beclin-1-dependent autophagy signaling [71]. Therefore, autophagy works in both early stage and late stage of ALDH2 regulation in pressure-overload adaptive response.
3.3 ALDH2 and Alcoholic Heart Failure
Alcoholic cardiomyopathy is characterized by a dilated left ventricle and reduced myocardial contractility due to a long-term history of heavy alcohol consumption. It was estimated that about one-third of alcoholics suffered from varying degrees of alcoholic cardiomyopathy and approximately half of them resulted in death within 4 years [43, 101]. Mitochondrial defects, cell death, heart rate variability, and cardiac remodeling would eventually result in heart failure [31].
As early as the twentieth century, it was found about 50% of Asians had facial flushing after drinking alcohol, and these individuals were tested having an inactive form of mitochondrial ALDH2 [88]. rs671 in ALDH2 gene was the most influential genetic variant linked to alcohol consumption [83]. ALDH2 deficiency aggravated alcoholic myocardiopathy by weakening acetaldehyde-biogenic amine condensation products detoxification, breaking intracellular Ca2+ homeostasis, increasing apoptosis, upregulating autophagy, as well as impairing mitochondrial function [52, 66, 72, 73, 101]. Besides, our study explored the role of ALDH2 in low-to-moderate alcohol consumption. On one hand, we confirmed the cardioprotective effects of low-to-moderate alcohol consumption which manifested by elevated HDL-c levels and upregulated HO-1 expression in the myocardium. However, the benefits were disrupted when ALDH2 was deficient, possibly by activating ROS-dependent apoptosis and RIP1/RIP3/MLKL-mediated necrosis [73]. A Guangzhou biobank cohort study genotyped rs671 of ALDH2 in 4867 men. Diastolic blood pressure and HDL cholesterol which associated with ALDH2 variants were attenuated after adjusting for alcohol use. The result suggested the apparent associations between physical activity and alcohol use in ALDH2 variants population [3]. Even moderate alcohol use was found associated with subclinical adverse effects with greater left ventricle mass and more impaired diastolic functions in subjects carrying ALDH2 variants, especially among East Asians [36]. Individuals with inactive isoforms of ALDH2 should be warned to avoid drinking alcohol, even for social or occupational promotion.
3.4 ALDH2 and Diabetes Mellitus-Related Heart Failure
The increasing morbidity and mortality of heart failure are related to the increase in aging, obesity, and diabetes mellitus in a large part. The prognosis of heart failure in patients with diabetes is much worse than that in patients without diabetes. The early symptom of diabetic cardiomyopathy is diastolic dysfunction and can gradually develop into systolic dysfunction. Metabolic disorder is an important feature of diabetic cardiomyopathy, manifested as reduced glucose uptake and increased fatty acid utilization accompanied by oxidative stress, inflammation, cardiomyocyte apoptosis, and myocardial fibrosis [37]. Beyond these, mitochondrial dysfunction, impaired mitochondrial and cardiomyocyte calcium handling, endoplasmic reticulum stress, and reduced nitric oxide bioavailability were also implicated in the development and progression of diabetic cardiomyopathy [39].
A genome-wide association study contained 12,720 participants found rs671 (ALDH2) was associated with metabolic syndrome (MetS) in Han Chinese. What’s more, the effects of rs671 on metabolic components were significantly correlated with drinking [108]. Previous studies showed that ALDH2 improved the contractile function of advanced diabetic cardiomyopathy by regulating Ca2+ homeostasis and autophagy [32, 104]. Our data found that ALDH2 deficiency impaired diastolic function in early stage of diabetic cardiomyopathy, while cardiac contractile function remained normal. In this stage, ALDH2 deficiency disrupted energy metabolism with increased AMP/ATP and ADP/ATP and decreased PCr/ATP ratio, which in turn induced activation of energy regulatory LKB1/AMPK pathway. The progressive accumulation of phosphatidylcholine and phosphatidylinositol in heart tissue induced metabolic homeostasis disequilibrium and led to deterioration of diastolic function [20, 91].
3.5 ALDH2 and Aging-Related Heart Failure
Aging is an irreversible biological process. In the cardiovascular area, age-dependent increases include left ventricular hypertrophy, diastolic dysfunction, atrial fibrillation, as well as vascular intimal thickening and vessel stiffness. Aging-related cardiac dysfunction is characterized with loss of cardiac contractile reserve, increased fibrosis and remodeling, impaired cardiomyocyte proteostasis, and loss of autophagy [21, 50]. Heart failure can be regarded as an aging-related phenotype. Aging-associated cardiac pathological changes involve oxidative stress, short telomere defect, mitochondrial damage, intracellular Ca2+ mishandling, etc. [2, 99].
Numerous studies suggested ALDH2 participated in the process of aging and age-related cardiovascular diseases [18, 106]; however, whether ALDH2 is beneficial or detrimental is still controversial. Wu found that ALDH2 ablation led to cardiac aging and sustained usage of Alda-1 (a specific activator of ALDH2) abrogated the aging effect [94]. ALDH2 activity was discovered to be significantly decreased in aged hearts which also demonstrated the benefits of activation of ALDH2 on retarding the aging process. In the meantime, ALDH2 was also discovered to exert age-dependent vasoprotective effects with decreased mitochondrial ROS formation and oxidative mtDNA damage [92]. On the contrary, our lab found ALDH2 overexpression such as using Alda-1 accentuated aging-related cardiomyocyte. The dysfunction was characterized by increased contractile dysfunction, oxidative stress, intracellular Ca2+ mishandling, and mitochondrial injury [105]. Moreover, AMPK/Sirt1 signaling cascades were found taken part in ALDH2-accenuated cardiac aging [106]. In the light of the debates, further epidemiological of different races or experimental studies will be needed to provide more evidence about the effect of ALDH2 in aging.
3.6 ALDH2 and Drug-Induced Heart Failure
Several chemical agents and drugs could impair cardiac mitochondrial function via destroying mitochondrial respiratory chain (e.g., uncoupling) or inhibiting mitochondrial enzymes. The most common agents are anticancer drugs such as anthracycline doxorubicin (DOX), cisplatin, and Trisenox; antiviral compound azidothymidine (AZT zidovudine); and several oral antidiabetic drugs such as Avandia [86].
The chemotherapy drug DOX is frequently found in inducing cardiotoxic. Left ventricular systolic pressure would significantly reduce, and left ventricular end-diastolic pressure would overtly increase after DOX treatment. ALDH2 attenuated this cardiotoxicity by inhibiting oxidative stress, decreasing the expression and activity of NADPH oxidase 2, and reducing myocardial apoptosis. In addition, DOX-induced myocardial dysfunction was severer with increased levels of 4-HNE and autophagy in ALDH2 knockout mice. Besides, these symptoms could be improved when ALDH2 activity was restored, suggesting that inhibition of 4-HNE and autophagy may be the possible mechanisms of ALDH2 against DOX-induced cardiac dysfunction [79].
Oxidative stress-induced cardiomyocyte apoptosis is also a main part in the pathogenesis of heart failure [59]. ROS production and accumulation caused intracellular redox imbalance, leading to mitochondrial dysfunction and decreased production of ATP [26]. We elucidated the relationship between ALDH2 deficiency and oxidative stress-induced apoptosis in an antimycin-induced heart failure model. Inhibiting ALDH2 activity by daidzin increased intracellular ROS levels and apoptosis in which associated with the upregulated phosphorylation of ERK1/2, JNK, and p38-MAPK [102]. Thus, these data suggested the beneficial role of ALDH2 in drug-induced heart failure.
4 ALDH2-Related Therapy
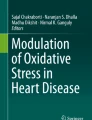
The following mediators have been reported mediating the cardiac dysfunction in ALDH2 deficiency: (1) ROS and toxic aldehydes [53]; (2) apoptosis pathways [80], involving caspase 3, Bcl- 2; (3) oxidative stress signaling cascade [1], involving MAP kinase cascades ERK1/2, SAPK/JNK, and p38 MAP kinase; and (4) autophagy [1], involving Beclin-1 and AMPK-mTOR. The indispensable role of ALDH2 in the pathogenesis of heart failure sheds light on the development of potential therapeutic target of it (Fig. 1). Here we summarized activators of ALDH2 and several other aspects which have already been proved to have therapeutic effects or just have a therapeutic potential on heart failure.

A scheme depicting how ALDH2 plays the protective role in heart failure. ALDH2 protects myocardium by maintaining myocardial cell survival and angiogenesis. At the same time, ALDH2 can determine the efficacy of stem cell transplantation by increasing the quality of seed stem cells and metabolic microenvironment
4.1 ALDH2 Activator
Alda-1, a small molecule activator of ALDH2, is a potential new therapeutic candidate. Alda-1 was reported to exert its cardioprotective effect through reducing oxidative stress, restoring calcium and CaMKII homeostasis, and detoxifying O2 •– induced reactive aldehydes to less reactive acids [16, 93]. It was also been reported to ameliorate pulmonary vascular remodeling in pulmonary arterial hypertension and inhibit atherosclerosis in apolipoprotein E-knockout mice [76, 97]. In addition, it played a protective role in cardiac dysfunction induced by abnormal glucose and lipid metabolism as well as DOX or 4-HNE-induced autophagic reduction and cell death [30, 79]. However, the efficiency of the activation by Alda-1 is variant, for example, Alda-1 increases acetaldehyde oxidation in wild-type ALDH2 (ALDH2*1) and East Asian variant of ALDH2 (ALDH2*2) approximately 1.5- and 6-fold, respectively [6]. Thus, the patients undergoing pathological processes such as cardiac ischemia with wild type or mutant ALDH2 might gain more benefits with the treatment of pharmacologic enhancement of ALDH2 activity [16]. Belmont conducted kinetic experiments to characterize Alda-1 on the properties of ALDH2 and found it was a complex behavior, where Alda-1 acted as inhibitor in low concentrations of aldehyde and as an activator in high concentrations [5]. Moreover, Alda-1 has exogenous and toxic characters. All factors should be taken into consideration when considering Alda-1 as an exogenous stimulator of ALDH2, including the working concentration, half-life period, continuity of stimulation, toxic, and side effects.
Protein kinase C ε (PKCε) has been found as another ALDH2 activator via direct phosphorylation. In vitro, phosphorylation of wild-type ALDH2 recombinant protein was reported increased its enzymatic activity [16]. The enzymatic activity of the phosphorylated ALDH2*2 is 270% of the non-phosphorylated ALDH2*2 [60]. Following phosphorylation by recombinant εPKC, there was an increase of 70% of the ALDH2 activity. Similar to Alda-1, the effect of εPKC phosphorylation was more pronounced on ALDH2*2 mutant enzyme. T185E, S279E, and T412E were three common phosphomimetic mutations sites by εPKC in the protection of ALDH2 against reactive aldehydes. Treatment with PKC activator upregulated ALDH2 activity, while applying PKC inhibitor had the opposite effect. Some study demonstrated that PKCε-ALDH2 interaction had disincentive effects in 4-HNE-induced aberrant PPARγ regulation, which suggest that PKCε-ALDH2 regulatory axis may be a therapeutic target for treating metabolic syndrome [100].
4.2 MicroRNAs
MicroRNAs are a class of endogenous interfering RNAs whose primary function are regulating the expression of genes. Evidences indicated that microRNAs could participate in diverse pathophysiological processes of cardiovascular disease, including hypertrophy, apoptosis, cardiac conduction, fibrosis, and angiogenesis [25, 75]. MiR-34a has been elucidated in many cell lines and was found related to apoptosis, energy metabolism, lipid metabolism, aging, and stem cell division [12, 33]. Bioinformatics analysis produced a protein-protein interaction network in HepG2 cells and revealed that ALDH2 was a potential target of miR-34a [19]. Our study found that increased circulating miR-34a could decrease ALDH2 activity and increase cardiomyocyte apoptosis post-MI injury [23]. Although miR-34a is not a cardiac-specific miRNA, the expression abundance of miR-34a in myocardium ranks third in all tissues [9], and it is reasonable to regard miR-34a as a diagnostic marker for MI. MiR-28 could also promote ischemia via inhibition of ALDH2 expression in myocardium [45]. In addition, Shen predicted ALDH2 as target genes of miR-224 [72]. The target sites existed in 3’UTR of ALDH2 suggesting that miR-224 downregulated the expressions of ALDH2 and finally regulated target genes in lipid metabolism. MicroRNAs might be new diagnostic indicators and therapeutic targets for heart failure patients. But it requires further studies in large cohort to assess the specificity and sensitivity of them.
4.3 Mesenchymal Stem Cell (MSC) Therapy
Mesenchymal stem cell (MSC) therapy is a promising approach in alleviating ischemic injury and promoting tissue regeneration [64]. A present meta-analysis including 64 studies strongly supported the potential of MSCs therapy for ischemic stroke [68]. Up to now, various strategies have been used to increase transplant effects in ischemic diseases, including tissue engineering scaffolds, genetic modification, and hypoxia-based pretreatment [27]; however, implanted cell dysplasia is still a problem [78]. Many factors could affect the efficiency including regenerative cell source, injectable delivery vehicles, and microenvironmental signals [67, 77]. Our results showed that host ALDH2 affected the survival of transplanted MSCs. Protein array analysis also revealed that ALDH2−/− tissues expressed low levels of angiogenic factors, including cysteine-rich angiogenic inducer 61, endoglin, epidermal growth factor, fibroblast growth factor-1, angiopoietin-1, matrix metallopeptidase-3/-9, and insulin-like growth factor binding protein, all of which could enhance the tolerance of engrafted MSCs during vasculogenesis in hypoxia injury [107]. Thus, ALDH2 may be regarded as a homeostatic mediator of microenvironment by increasing local capillary density and energy supply and decreasing oxidative stress after ischemia.
4.4 ALDH Bright Cells
Autologous bone marrow-derived aldehyde dehydrogenase bright (ALDHbr) cells isolated by flow sorting express high activity of ALDH [41]. They have been applied in clinical practice to repair tissue damage and have been proven safe and efficient in patients with chronic myocardial ischemia [62]. Our observations supported the effective therapeutic effect of ALDHbr cells on ischemic myocardium; in addition, we demonstrated ALDH2 as a key mediator in the process [81]. Weakened glycolysis, mitochondrial respiratory abnormalities, and increased mitochondrial ROS gave rise to the diminished therapeutic efficacy of ALDHbr cells in ALDH2 deficiency mice rather than oxidative phosphorylation impairment. The results gave us a hint that ALDH2 activity was a pivotal precondition in the efficacy of ALDHbr cell therapy; therefore individuals with loss of ALDH2 function are unsuitable for ALDHbr cell therapy. However, recently a clinical trial didn’t find significant positive outcomes of ALDHbr cells in patients with peripheral artery disease [63]. Future investigational trial tests about cell therapy should be carried out to find new anatomic and perfusion insights.
5 Conclusion
Just as Braunwald said, heart failure is the last battle of cardiovascular diseases [11]. It is urgent to find a novel prospective to illustrate the mechanism of heart failure and to improve the prognosis. This review summarizes the roles of ALDH2 gene polymorphisms and ALDH2 enzyme activity in heart failure induced by multiple causes, such as ischemic injury, hypertension, alcohol, diabetes, and aging. Except the controversial role of ALDH2 in aging-related cardiac dysfunction, studies have suggested a cardioprotective role of ALDH2 to counteract cardiac dysfunction due to different etiologies. Emerging evidences provided new insight in understanding the epigenetic and transcriptional regulation of ALDH2 as well as the effect of ALDH2 in stem cell transplantation. Strategies aim to enhancing ALDH2 activity or expression, as well as improving mitochondrial function, will bring novel prospects for the treatment of heart failure.
References
Adameova A, Goncalvesova E, Szobi A, Dhalla NS (2016) Necroptotic cell death in failing heart: relevance and proposed mechanisms. Heart Fail Rev 21(2):213–221. https://doi.org/10.1007/s10741-016-9537-8
Armanios M, Blackburn EH (2012) The telomere syndromes. Nat Rev Genet 13(10):693–704. https://doi.org/10.1038/nrg3246
Au YS, Jiang C, Cheng KK, Liu B, Zhang W, Lam TH, Leung GM, Schooling CM (2013) Is aldehyde dehydrogenase 2 a credible genetic instrument for alcohol use in Mendelian randomization analysis in southern Chinese men? Int J Epidemiol 42(1):318–328. https://doi.org/10.1093/ije/dys221
Bayeva M, Gheorghiade M, Ardehali H (2013) Mitochondria as a therapeutic target in heart failure. J Am Coll Cardiol 61(6):599–610. https://doi.org/10.1016/j.jacc.2012.08.1021
Belmont-Diaz JA, Yoval-Sanchez B, Calleja-Castaneda LF, Pardo VJ, Rodriguez-Zavala JS (2016) Alda-1 modulates the kinetic properties of mitochondrial aldehyde dehydrogenase (ALDH2). FEBS J 283(19):3637–3650. https://doi.org/10.1111/febs.13833
Beretta M, Gorren AC, Wenzl MV, Weis R, Russwurm M, Koesling D, Schmidt K, Mayer B (2010) Characterization of the east Asian variant of aldehyde dehydrogenase-2: bioactivation of nitroglycerin and effects of Alda-1. J Biol Chem 285(2):943–952. https://doi.org/10.1074/jbc.M109.014548
Bhatnagar A (1995) Electrophysiological effects of 4-hydroxynonenal, an aldehydic product of lipid peroxidation, on isolated rat ventricular myocytes. Circ Res 76(2):293–304
Boldogh I, Bacsi A, Choudhury BK, Dharajiya N, Alam R, Hazra TK, Mitra S, Goldblum RM, Sur S (2005) ROS generated by pollen NADPH oxidase provide a signal that augments antigen-induced allergic airway inflammation. J Clin Invest 115(8):2169–2179. https://doi.org/10.1172/JCI24422
Bommer GT, Gerin I, Feng Y, Kaczorowski AJ, Kuick R, Love RE, Zhai Y, Giordano TJ, Qin ZS, Moore BB, MacDougald OA, Cho KR, Fearon ER (2007) 53-mediated activation of miRNA34 candidate tumor-suppressor genes. Curr Biol 17(15):1298–1307. https://doi.org/10.1016/j.cub.2007.06.068
Braunwald E (2013) Heart failure. JACC Heart Fail 1(1):1–20. https://doi.org/10.1016/j.jchf.2012.10.002
Braunwald E (2015) The war against heart failure: the lancet lecture. Lancet 385(9970):812–824. https://doi.org/10.1016/S0140-6736(14)61889-4
Bu P, Wang L, Chen KY, Srinivasan T, Murthy PK, Tung KL, Varanko AK, Chen HJ, Ai Y, King S, Lipkin SM, Shen X (2016) A miR-34a-numb feedforward loop triggered by inflammation regulates asymmetric stem cell division in intestine and Colon cancer. Cell Stem Cell 18(2):189–202. https://doi.org/10.1016/j.stem.2016.01.006
Budas GR, Disatnik MH, Mochly-Rosen D (2009) Aldehyde dehydrogenase 2 in cardiac protection: a new therapeutic target? Trends Cardiovasc Med 19(5):158–164. https://doi.org/10.1016/j.tcm.2009.09.003
Bui AL, Horwich TB, Fonarow GC (2011) Epidemiology and risk profile of heart failure. Nat Rev Cardiol 8(1):30–41. https://doi.org/10.1038/nrcardio.2010.165
Chen Z, Foster MW, Zhang J, Mao L, Rockman HA, Kawamoto T, Kitagawa K, Nakayama KI, Hess DT, Stamler JS (2005) An essential role for mitochondrial aldehyde dehydrogenase in nitroglycerin bioactivation. Proc Natl Acad Sci U S A 102(34):12159–12164. https://doi.org/10.1073/pnas.0503723102
Chen CH, Budas GR, Churchill EN, Disatnik MH, Hurley TD, Mochly-Rosen D (2008) Activation of aldehyde dehydrogenase-2 reduces ischemic damage to the heart. Science 321(5895):1493–1495. https://doi.org/10.1126/science.1158554
Chen CH, Sun L, Mochly-Rosen D (2010) Mitochondrial aldehyde dehydrogenase and cardiac diseases. Cardiovasc Res 88(1):51–57. https://doi.org/10.1093/cvr/cvq192
Chen CH, Ferreira JC, Gross ER, Mochly-Rosen D (2014) Targeting aldehyde dehydrogenase 2: new therapeutic opportunities. Physiol Rev 94(1):1–34. https://doi.org/10.1152/physrev.00017.2013
Cheng J, Zhou L, Xie QF, Xie HY, Wei XY, Gao F, Xing CY, Xu X, Li LJ, Zheng SS (2010) The impact of miR-34a on protein output in hepatocellular carcinoma HepG2 cells. Proteomics 10(8):1557–1572. https://doi.org/10.1002/pmic.200900646
Christoffersen C, Bollano E, Lindegaard ML, Bartels ED, Goetze JP, Andersen CB, Nielsen LB (2003) Cardiac lipid accumulation associated with diastolic dysfunction in obese mice. Endocrinology 144(8):3483–3490. https://doi.org/10.1210/en.2003-0242
Cuervo AM, Bergamini E, Brunk UT, Droge W, Ffrench M, Terman A (2005) Autophagy and aging: the importance of maintaining “clean” cells. Autophagy 1(3):131–140
Delbridge L, Mellor KM, Taylor DJ, Gottlieb RA (2017) Myocardial stress and autophagy: mechanisms and potential therapies. Nat Rev Cardiol 14(7):412–425. https://doi.org/10.1038/nrcardio.2017.35
Fan F, Sun A, Zhao H, Liu X, Zhang W, Jin X, Wang C, Ma X, Shen C, Zou Y, Hu K, Ge J (2013) MicroRNA-34a promotes cardiomyocyte apoptosis post myocardial infarction through down-regulating aldehyde dehydrogenase 2. Curr Pharm Des 19(27):4865–4873
Galluzzi L, Baehrecke EH, Ballabio A, Boya P, Bravo-San PJ, Cecconi F, Choi AM, Chu CT, Codogno P, Colombo MI, Cuervo AM, Debnath J, Deretic V, Dikic I, Eskelinen EL, Fimia GM, Fulda S, Gewirtz DA, Green DR, Hansen M, Harper JW, Jaattela M, Johansen T, Juhasz G, Kimmelman AC, Kraft C, Ktistakis NT, Kumar S, Levine B, Lopez-Otin C, Madeo F, Martens S, Martinez J, Melendez A, Mizushima N, Munz C, Murphy LO, Penninger JM, Piacentini M, Reggiori F, Rubinsztein DC, Ryan KM, Santambrogio L, Scorrano L, Simon AK, Simon HU, Simonsen A, Tavernarakis N, Tooze SA, Yoshimori T, Yuan J, Yue Z, Zhong Q, Kroemer G (2017) Molecular definitions of autophagy and related processes. EMBO J 36(13):1811–1836. https://doi.org/10.15252/embj.201796697
Ghildiyal M, Zamore PD (2009) Small silencing RNAs: an expanding universe. Nat Rev Genet 10(2):94–108. https://doi.org/10.1038/nrg2504
Giordano FJ (2005) Oxygen, oxidative stress, hypoxia, and heart failure. J Clin Invest 115(3):500–508. https://doi.org/10.1172/JCI24408
Gnecchi M, He H, Liang OD, Melo LG, Morello F, Mu H, Noiseux N, Zhang L, Pratt RE, Ingwall JS, Dzau VJ (2005) Paracrine action accounts for marked protection of ischemic heart by Akt-modified mesenchymal stem cells. Nat Med 11(4):367–368. https://doi.org/10.1038/nm0405-367
Goedde HW, Agarwal DP (1990) Pharmacogenetics of aldehyde dehydrogenase (ALDH). Pharmacol Ther 45(3):345–371
Groenendyk J, Sreenivasaiah PK, Kim DH, Agellon LB, Michalak M (2010) Biology of endoplasmic reticulum stress in the heart. Circ Res 107(10):1185–1197. https://doi.org/10.1161/CIRCRESAHA.110.227033
Gu X, Fang T, Kang P, Hu J, Yu Y, Li Z, Cheng X, Gao Q (2017) Effect of ALDH2 on high glucose-induced cardiac fibroblast oxidative stress, apoptosis, and fibrosis. Oxid Med Cell Longev 2017:9257967. https://doi.org/10.1155/2017/9257967
Guo R, Ren J (2010) Alcohol and acetaldehyde in public health: from marvel to menace. Int J Environ Res Public Health 7(4):1285–1301. https://doi.org/10.3390/ijerph7041285
Guo Y, Yu W, Sun D, Wang J, Li C, Zhang R, Babcock SA, Li Y, Liu M, Ma M, Shen M, Zeng C, Li N, He W, Zou Q, Zhang Y, Wang H (2015) A novel protective mechanism for mitochondrial aldehyde dehydrogenase (ALDH2) in type i diabetes-induced cardiac dysfunction: role of AMPK-regulated autophagy. Biochim Biophys Acta 1852(2):319–331. https://doi.org/10.1016/j.bbadis.2014.05.017
Han HS, Choi BH, Kim JS, Kang G, Koo SH (2017) Hepatic Crtc2 controls whole body energy metabolism via a miR-34a-Fgf21 axis. Nat Commun 8(1):1878. https://doi.org/10.1038/s41467-017-01878-6
Heidenreich PA, Albert NM, Allen LA, Bluemke DA, Butler J, Fonarow GC, Ikonomidis JS, Khavjou O, Konstam MA, Maddox TM, Nichol G, Pham M, Pina IL, Trogdon JG (2013) Forecasting the impact of heart failure in the United States: a policy statement from the American Heart Association. Circ Heart Fail 6(3):606–619. https://doi.org/10.1161/HHF.0b013e318291329a
Hein S, Arnon E, Kostin S, Schonburg M, Elsasser A, Polyakova V, Bauer EP, Klovekorn WP, Schaper J (2003) Progression from compensated hypertrophy to failure in the pressure-overloaded human heart: structural deterioration and compensatory mechanisms. Circulation 107(7):984–991
Hung CL, Chang SC, Chang SH, Chi PC, Lai YJ, Wang SW, Wu YJ, Yeh HI, Lin SJ, Chen CH, Mochly-Rosen D, Wang LY (2017) Genetic polymorphisms of alcohol metabolizing enzymes and alcohol consumption are associated with asymptomatic cardiac remodeling and subclinical systolic dysfunction in Large community-dwelling Asians. Alcohol Alcohol 52(6):638–646. https://doi.org/10.1093/alcalc/agx049
Isfort M, Stevens SC, Schaffer S, Jong CJ, Wold LE (2014) Metabolic dysfunction in diabetic cardiomyopathy. Heart Fail Rev 19(1):35–48. https://doi.org/10.1007/s10741-013-9377-8
Jackson B, Brocker C, Thompson DC, Black W, Vasiliou K, Nebert DW, Vasiliou V (2011) Update on the aldehyde dehydrogenase gene (ALDH) superfamily. Hum Genomics 5(4):283–303
Jia G, Hill MA, Sowers JR (2018) Diabetic cardiomyopathy: an update of mechanisms contributing to this clinical entity. Circ Res 122(4):624–638. https://doi.org/10.1161/CIRCRESAHA.117.311586
Jiang Y, Xia W, Yang J, Zhu Y, Chang H, Liu J, Huo W, Xu B, Chen X, Li Y, Xu S (2015) BPA-induced DNA hypermethylation of the master mitochondrial gene PGC-1alpha contributes to cardiomyopathy in male rats. Toxicology 329:21–31. https://doi.org/10.1016/j.tox.2015.01.001
Jones RJ, Barber JP, Vala MS, Collector MI, Kaufmann SH, Ludeman SM, Colvin OM, Hilton J (1995) Assessment of aldehyde dehydrogenase in viable cells. Blood 85(10):2742–2746
Kim I, Xu W, Reed JC (2008) Cell death and endoplasmic reticulum stress: disease relevance and therapeutic opportunities. Nat Rev Drug Discov 7(12):1013–1030. https://doi.org/10.1038/nrd2755
Laonigro I, Correale M, Di Biase M, Altomare E (2009) Alcohol abuse and heart failure. Eur J Heart Fail 11(5):453–462. https://doi.org/10.1093/eurjhf/hfp037
Li Y, Zhang D, Jin W, Shao C, Yan P, Xu C, Sheng H, Liu Y, Yu J, Xie Y, Zhao Y, Lu D, Nebert DW, Harrison DC, Huang W, Jin L (2006) Mitochondrial aldehyde dehydrogenase-2 (ALDH2) Glu504Lys polymorphism contributes to the variation in efficacy of sublingual nitroglycerin. J Clin Invest 116(2):506–511. https://doi.org/10.1172/JCI26564
Li SP, Liu B, Song B, Wang CX, Zhou YC (2015) miR-28 promotes cardiac ischemia by targeting mitochondrial aldehyde dehydrogenase 2 (ALDH2) in mus musculus cardiac myocytes. Eur Rev Med Pharmacol Sci 19(5):752–758
Li R, Zhao Z, Sun M, Luo J, Xiao Y (2016) ALDH2 gene polymorphism in different types of cancers and its clinical significance. Life Sci 147:59–66. https://doi.org/10.1016/j.lfs.2016.01.028
Liao J, Sun A, Xie Y, Isse T, Kawamoto T, Zou Y, Ge J (2012) Aldehyde dehydrogenase-2 deficiency aggravates cardiac dysfunction elicited by endoplasmic reticulum stress induction. Mol Med 18:785–793. https://doi.org/10.2119/molmed.2011.00466
Lin H, Li HF, Chen HH, Lai PF, Juan SH, Chen JJ, Cheng CF (2014) Activating transcription factor 3 protects against pressure-overload heart failure via the autophagy molecule Beclin-1 pathway. Mol Pharmacol 85(5):682–691. https://doi.org/10.1124/mol.113.090092
Liu X, Sun X, Liao H, Dong Z, Zhao J, Zhu H, Wang P, Shen L, Xu L, Ma X, Shen C, Fan F, Wang C, Hu K, Zou Y, Ge J, Ren J, Sun A (2015) Mitochondrial aldehyde dehydrogenase 2 regulates revascularization in chronic ischemia: potential impact on the development of coronary collateral Circulation. Arterioscler Thromb Vasc Biol 35(10):2196–2206. https://doi.org/10.1161/ATVBAHA.115.306012
Lopez-Otin C, Blasco MA, Partridge L, Serrano M, Kroemer G (2013) The hallmarks of aging. Cell 153(6):1194–1217. https://doi.org/10.1016/j.cell.2013.05.039
Lorell BH, Carabello BA (2000) Left ventricular hypertrophy: pathogenesis, detection, and prognosis. Circulation 102(4):470–479
Ma H, Li J, Gao F, Ren J (2009) Aldehyde dehydrogenase 2 ameliorates acute cardiac toxicity of ethanol: role of protein phosphatase and forkhead transcription factor. J Am Coll Cardiol 54(23):2187–2196. https://doi.org/10.1016/j.jacc.2009.04.100
Ma H, Guo R, Yu L, Zhang Y, Ren J (2011) Aldehyde dehydrogenase 2 (ALDH2) rescues myocardial ischaemia/reperfusion injury: role of autophagy paradox and toxic aldehyde. Eur Heart J 32(8):1025–1038. https://doi.org/10.1093/eurheartj/ehq253
Mann DL, Bristow MR (2005) Mechanisms and models in heart failure: the biomechanical model and beyond. Circulation 111(21):2837–2849. https://doi.org/10.1161/CIRCULATIONAHA.104.500546
Matsumoto A (2016) Fundamental Properties of Aldehyde Dehydrogenase 2 (ALDH2) and the Importance of the ALDH2 Polymorphism. Nihon Eiseigaku Zasshi 71(1):55–68. https://doi.org/10.1265/jjh.71.55
McMurray JJ (2015) Neprilysin inhibition to treat heart failure: a tale of science, serendipity, and second chances. Eur J Heart Fail 17(3):242–247. https://doi.org/10.1002/ejhf.250
McMurray JJ, Packer M, Desai AS, Gong J, Lefkowitz MP, Rizkala AR, Rouleau JL, Shi VC, Solomon SD, Swedberg K, Zile MR (2014) Angiotensin-neprilysin inhibition versus enalapril in heart failure. N Engl J Med 371(11):993–1004. https://doi.org/10.1056/NEJMoa1409077
Metra M, Teerlink JR (2017) Heart failure. Lancet 390(10106):1981–1995. https://doi.org/10.1016/S0140-6736(17)31071-1
Munzel T, Gori T, Keaney JJ, Maack C, Daiber A (2015) Pathophysiological role of oxidative stress in systolic and diastolic heart failure and its therapeutic implications. Eur Heart J 36(38):2555–2564. https://doi.org/10.1093/eurheartj/ehv305
Nene A, Chen CH, Disatnik MH, Cruz L, Mochly-Rosen D (2017) Aldehyde dehydrogenase 2 activation and coevolution of its epsilonPKC-mediated phosphorylation sites. J Biomed Sci 24(1):3. https://doi.org/10.1186/s12929-016-0312-x
Pang J, Wang J, Zhang Y, Xu F, Chen Y (2017) Targeting acetaldehyde dehydrogenase 2 (ALDH2) in heart failure-recent insights and perspectives. Biochim Biophys Acta 1863(8):1933–1941. https://doi.org/10.1016/j.bbadis.2016.10.004
Perin EC, Silva GV, Zheng Y, Gahremanpour A, Canales J, Patel D, Fernandes MR, Keller LH, Quan X, Coulter SA, Moore WH, Herlihy JP, Willerson JT (2012) Randomized, double-blind pilot study of transendocardial injection of autologous aldehyde dehydrogenase-bright stem cells in patients with ischemic heart failure. Am Heart J 163(3):415–421. https://doi.org/10.1016/j.ahj.2011.11.020
Perin EC, Murphy MP, March KL, Bolli R, Loughran J, Yang PC, Leeper NJ, Dalman RL, Alexander J, Henry TD, Traverse JH, Pepine CJ, Anderson RD, Berceli S, Willerson JT, Muthupillai R, Gahremanpour A, Raveendran G, Velasquez O, Hare JM, Hernandez SI, Kasi VS, Hiatt WR, Ambale-Venkatesh B, Lima JA, Taylor DA, Resende M, Gee AP, Durett AG, Bloom J, Richman S, G'Sell P, Williams S, Khan F, Gyang RE, Santoso MR, Goldman J, Leach D, Handberg E, Cheong B, Piece N, DiFede D, Bruhn-Ding B, Caldwell E, Bettencourt J, Lai D, Piller L, Simpson L, Cohen M, Sayre SL, Vojvodic RW, Moye L, Ebert RF, Simari RD, Hirsch AT (2017) Evaluation of cell therapy on exercise performance and limb perfusion in peripheral artery disease: the CCTRN PACE trial (patients with intermittent claudication injected with ALDH bright cells). Circulation 135(15):1417–1428. https://doi.org/10.1161/CIRCULATIONAHA.116.025707
Ranganath SH, Levy O, Inamdar MS, Karp JM (2012) Harnessing the mesenchymal stem cell secretome for the treatment of cardiovascular disease. Cell Stem Cell 10(3):244–258. https://doi.org/10.1016/j.stem.2012.02.005
Rau CD, Vondriska TM (2017) DNA methylation and human heart failure: mechanisms or prognostics. Circulation 136(16):1545–1547. https://doi.org/10.1161/CIRCULATIONAHA.117.029840
Ren J (2007) Acetaldehyde and alcoholic cardiomyopathy: lessons from the ADH and ALDH2 transgenic models. Novartis Found Symp 285:69–76, 76–79, 198–199
Russo V, Young S, Hamilton A, Amsden BG, Flynn LE (2014) Mesenchymal stem cell delivery strategies to promote cardiac regeneration following ischemic injury. Biomaterials 35(13):3956–3974. https://doi.org/10.1016/j.biomaterials.2014.01.075
Sarmah D, Agrawal V, Rane P, Bhute S, Watanabe M, Kalia K, Ghosh Z, Dave KR, Yavagal DR, Bhattacharya P (2017) Mesenchymal stem cell therapy in ischemic stroke: a meta-analysis of preclinical studies. Clin Pharmacol Ther. https://doi.org/10.1002/cpt.927
Shah AM, Mann DL (2011) In search of new therapeutic targets and strategies for heart failure: recent advances in basic science. Lancet 378(9792):704–712. https://doi.org/10.1016/S0140-6736(11)60894-5
Sharma A, Sharma R, Chaudhary P, Vatsyayan R, Pearce V, Jeyabal PV, Zimniak P, Awasthi S, Awasthi YC (2008) 4-Hydroxynonenal induces p53-mediated apoptosis in retinal pigment epithelial cells. Arch Biochem Biophys 480(2):85–94. https://doi.org/10.1016/j.abb.2008.09.016
Shen C, Wang C, Fan F, Yang Z, Cao Q, Liu X, Sun X, Zhao X, Wang P, Ma X, Zhu H, Dong Z, Zou Y, Hu K, Sun A, Ge J (2015) Acetaldehyde dehydrogenase 2 (ALDH2) deficiency exacerbates pressure overload-induced cardiac dysfunction by inhibiting Beclin-1 dependent autophagy pathway. Biochim Biophys Acta 1852(2):310–318. https://doi.org/10.1016/j.bbadis.2014.07.014
Shen B, Pan Q, Yang Y, Gao Y, Liu X, Li W, Han Y, Yuan X, Qu Y, Zhao Z (2017a) miR-224 Affects Mammary Epithelial Cell Apoptosis and Triglyceride Production by Downregulating ACADM and ALDH2 Genes. DNA Cell Biol 36(1):26–33. https://doi.org/10.1089/dna.2016.3540
Shen C, Wang C, Han S, Wang Z, Dong Z, Zhao X, Wang P, Zhu H, Sun X, Ma X, Zhu H, Zou Y, Hu K, Ge J, Sun A (2017b) Aldehyde dehydrogenase 2 deficiency negates chronic low-to-moderate alcohol consumption-induced cardioprotecion possibly via ROS-dependent apoptosis and RIP1/RIP3/MLKL-mediated necroptosis. Biochim Biophys Acta 1863(8):1912–1918. https://doi.org/10.1016/j.bbadis.2016.11.016
Singh S, Arcaroli J, Thompson DC, Messersmith W, Vasiliou V (2015) Acetaldehyde and retinaldehyde-metabolizing enzymes in colon and pancreatic cancers. Adv Exp Med Biol 815:281–294. https://doi.org/10.1007/978-3-319-09614-8_16
Small EM, Frost RJ, Olson EN (2010) MicroRNAs add a new dimension to cardiovascular disease. Circulation 121(8):1022–1032. https://doi.org/10.1161/CIRCULATIONAHA.109.889048
Stachowicz A, Olszanecki R, Suski M, Wisniewska A, Toton-Zuranska J, Madej J, Jawien J, Bialas M, Okon K, Gajda M, Glombik K, Basta-Kaim A, Korbut R (2014) Mitochondrial aldehyde dehydrogenase activation by Alda-1 inhibits atherosclerosis and attenuates hepatic steatosis in apolipoprotein E-knockout mice. J Am Heart Assoc 3(6):e1329. https://doi.org/10.1161/JAHA.114.001329
Sui BD, Hu CH, Zheng CX, Jin Y (2016) Microenvironmental views on mesenchymal stem cell differentiation in aging. J Dent Res 95(12):1333–1340. https://doi.org/10.1177/0022034516653589
Sui BD, Hu CH, Liu AQ, Zheng CX, Xuan K, Jin Y (2017) Stem cell-based bone regeneration in diseased microenvironments: challenges and solutions. Biomaterials. https://doi.org/10.1016/j.biomaterials.2017.10.046
Sun A, Cheng Y, Zhang Y, Zhang Q, Wang S, Tian S, Zou Y, Hu K, Ren J, Ge J (2014a) Aldehyde dehydrogenase 2 ameliorates doxorubicin-induced myocardial dysfunction through detoxification of 4-HNE and suppression of autophagy. J Mol Cell Cardiol 71:92–104. https://doi.org/10.1016/j.yjmcc.2014.01.002
Sun A, Zou Y, Wang P, Xu D, Gong H, Wang S, Qin Y, Zhang P, Chen Y, Harada M, Isse T, Kawamoto T, Fan H, Yang P, Akazawa H, Nagai T, Takano H, Ping P, Komuro I, Ge J (2014b) Mitochondrial aldehyde dehydrogenase 2 plays protective roles in heart failure after myocardial infarction via suppression of the cytosolic JNK/p53 pathway in mice. J Am Heart Assoc 3(5):e779. https://doi.org/10.1161/JAHA.113.000779
Sun X, Zhu H, Dong Z, Liu X, Ma X, Han S, Lu F, Wang P, Qian S, Wang C, Shen C, Zhao X, Zou Y, Ge J, Sun A (2017) Mitochondrial aldehyde dehydrogenase-2 deficiency compromises therapeutic effect of ALDH bright cell on peripheral ischemia. Redox Biol 13:196–206. https://doi.org/10.1016/j.redox.2017.05.018
Tabas I (2010) The role of endoplasmic reticulum stress in the progression of atherosclerosis. Circ Res 107(7):839–850. https://doi.org/10.1161/CIRCRESAHA.110.224766
Takeshita T, Morimoto K, Mao XQ, Hashimoto T, Furuyama J (1993) Phenotypic differences in low km aldehyde dehydrogenase in Japanese workers. Lancet 341(8848):837–838
Valentova M, von Haehling S, Bauditz J, Doehner W, Ebner N, Bekfani T, Elsner S, Sliziuk V, Scherbakov N, Murin J, Anker SD, Sandek A (2016) Intestinal congestion and right ventricular dysfunction: a link with appetite loss, inflammation, and cachexia in chronic heart failure. Eur Heart J 37(21):1684–1691. https://doi.org/10.1093/eurheartj/ehw008
van Riet EE, Hoes AW, Wagenaar KP, Limburg A, Landman MA, Rutten FH (2016) Epidemiology of heart failure: the prevalence of heart failure and ventricular dysfunction in older adults over time. A systematic review. Eur J Heart Fail 18(3):242–252. https://doi.org/10.1002/ejhf.483
Varga ZV, Ferdinandy P, Liaudet L, Pacher P (2015) Drug-induced mitochondrial dysfunction and cardiotoxicity. Am J Physiol Heart Circ Physiol 309(9):H1453–H1467. https://doi.org/10.1152/ajpheart.00554.2015
von Hardenberg A, Maack C (2017) Mitochondrial therapies in heart failure. Handb Exp Pharmacol 243:491–514. https://doi.org/10.1007/164_2016_123
Wall TL, Gallen CC, Ehlers CL (1993) Effects of alcohol on the EEG in Asian men with genetic variations of ALDH2. Biol Psychiatry 34(1–2):91–99
Wang F, Ye P (2014) Improving heart function by modulating myocardiocyte autophagy: a possible novel mechanism for cardiovascular protection of high-density lipoprotein. Lipids Health Dis 13:163. https://doi.org/10.1186/1476-511X-13-163
Wang P, Shen C, Diao L, Yang Z, Fan F, Wang C, Liu X, Sun X, Dong Z, Zhu H, Ma X, Cao Q, Zhao X, Ma D, Zou Y, Hu K, Sun A, Ge J (2015) Aberrant hypermethylation of aldehyde dehydrogenase 2 promoter upstream sequence in rats with experimental myocardial infarction. Biomed Res Int 2015:503692. https://doi.org/10.1155/2015/503692
Wang C, Fan F, Cao Q, Shen C, Zhu H, Wang P, Zhao X, Sun X, Dong Z, Ma X, Liu X, Han S, Wu C, Zou Y, Hu K, Ge J, Sun A (2016) Mitochondrial aldehyde dehydrogenase 2 deficiency aggravates energy metabolism disturbance and diastolic dysfunction in diabetic mice. J Mol Med (Berl) 94(11):1229–1240. https://doi.org/10.1007/s00109-016-1449-5
Wenzel P, Schuhmacher S, Kienhofer J, Muller J, Hortmann M, Oelze M, Schulz E, Treiber N, Kawamoto T, Scharffetter-Kochanek K, Munzel T, Burkle A, Bachschmid MM, Daiber A (2008) Manganese superoxide dismutase and aldehyde dehydrogenase deficiency increase mitochondrial oxidative stress and aggravate age-dependent vascular dysfunction. Cardiovasc Res 80(2):280–289. https://doi.org/10.1093/cvr/cvn182
Woods C, Shang C, Taghavi F, Downey P, Zalewski A, Rubio GR, Liu J, Homburger JR, Grunwald Z, Qi W, Bollensdorff C, Thanaporn P, Ali A, Riemer K, Kohl P, Mochly-Rosen D, Gerstenfeld E, Large S, Ali Z, Ashley E (2016) In vivo post-cardiac arrest myocardial dysfunction is supported by Ca2+/Calmodulin-dependent protein kinase II-mediated calcium long-term potentiation and mitigated by Alda-1, an agonist of aldehyde dehydrogenase type 2. Circulation 134(13):961–977. https://doi.org/10.1161/CIRCULATIONAHA.116.021618
Wu B, Yu L, Wang Y, Wang H, Li C, Yin Y, Yang J, Wang Z, Zheng Q, Ma H (2016) Aldehyde dehydrogenase 2 activation in aged heart improves the autophagy by reducing the carbonyl modification on SIRT1. Oncotarget 7(3):2175–2188. https://doi.org/10.18632/oncotarget.6814
Xia G, Fan F, Liu M, Wang S, Wu J, Shen C, Han S, Wang C, Jia J, Zou Y, Hu K, Ge J, Sun A (2016) Aldehyde dehydrogenase 2 deficiency blunts compensatory cardiac hypertrophy through modulating Akt phosphorylation early after transverse aorta constriction in mice. Biochim Biophys Acta 1862(9):1587–1593. https://doi.org/10.1016/j.bbadis.2016.05.019
Xiao Y, Yang Z, Wu QQ, Jiang XH, Yuan Y, Chang W, Bian ZY, Zhu JX, Tang QZ (2017) Cucurbitacin B protects against pressure overload induced cardiac hypertrophy. J Cell Biochem 118(11):3899–3910. https://doi.org/10.1002/jcb.26041
Xu T, Liu S, Ma T, Jia Z, Zhang Z, Wang A (2017) Aldehyde dehydrogenase 2 protects against oxidative stress associated with pulmonary arterial hypertension. Redox Biol 11:286–296. https://doi.org/10.1016/j.redox.2016.12.019
Xue R, Zeng J, Chen Y, Chen C, Tan W, Zhao J, Dong B, Sun Y, Dong Y, Liu C (2017) Sestrin 1 ameliorates cardiac hypertrophy via autophagy activation. J Cell Mol Med 21(6):1193–1205. https://doi.org/10.1111/jcmm.13052
Yang X, Sreejayan N, Ren J (2005) Views from within and beyond: narratives of cardiac contractile dysfunction under senescence. Endocrine 26(2):127–137. https://doi.org/10.1385/ENDO:26:2:127
Yu YH, Liao PR, Guo CJ, Chen CH, Mochly-Rosen D, Chuang LM (2016) PKC-ALDH2 pathway plays a novel role in adipocyte differentiation. PLoS One 11(8):e161993. https://doi.org/10.1371/journal.pone.0161993
Zhang Y, Ren J (2011) ALDH2 in alcoholic heart diseases: molecular mechanism and clinical implications. Pharmacol Ther 132(1):86–95. https://doi.org/10.1016/j.pharmthera.2011.05.008
Zhang P, Xu D, Wang S, Fu H, Wang K, Zou Y, Sun A, Ge J (2011) Inhibition of aldehyde dehydrogenase 2 activity enhances antimycin-induced rat cardiomyocytes apoptosis through activation of MAPK signaling pathway. Biomed Pharmacother 65(8):590–593. https://doi.org/10.1016/j.biopha.2009.12.001
Zhang H, Gong DX, Zhang YJ, Li SJ, Hu S (2012a) Effect of mitochondrial aldehyde dehydrogenase-2 genotype on cardioprotection in patients with congenital heart disease. Eur Heart J 33(13):1606–1614. https://doi.org/10.1093/eurheartj/ehs061
Zhang Y, Babcock SA, Hu N, Maris JR, Wang H, Ren J (2012b) Mitochondrial aldehyde dehydrogenase (ALDH2) protects against streptozotocin-induced diabetic cardiomyopathy: role of GSK3beta and mitochondrial function. BMC Med 10:40. https://doi.org/10.1186/1741-7015-10-40
Zhang Y, Mi SL, Hu N, Doser TA, Sun A, Ge J, Ren J (2014) Mitochondrial aldehyde dehydrogenase 2 accentuates aging-induced cardiac remodeling and contractile dysfunction: role of AMPK, Sirt1, and mitochondrial function. Free Radic Biol Med 71:208–220. https://doi.org/10.1016/j.freeradbiomed.2014.03.018
Zhang Y, Wang C, Zhou J, Sun A, Hueckstaedt LK, Ge J, Ren J (2017) Complex inhibition of autophagy by mitochondrial aldehyde dehydrogenase shortens lifespan and exacerbates cardiac aging. Biochim Biophys Acta 1863(8):1919–1932. https://doi.org/10.1016/j.bbadis.2017.03.016
Zhu H, Sun A, Zhu H, Li Z, Huang Z, Zhang S, Ma X, Zou Y, Hu K, Ge J (2014) Aldehyde dehydrogenase-2 is a host factor required for effective bone marrow mesenchymal stem cell therapy. Arterioscler Thromb Vasc Biol 34(4):894–901. https://doi.org/10.1161/ATVBAHA.114.303241
Zhu Y, Zhang D, Zhou D, Li Z, Li Z, Fang L, Yang M, Shan Z, Li H, Chen J, Zhou X, Ye W, Yu S, Li H, Cai L, Liu C, Zhang J, Wang L, Lai Y, Ruan L, Sun Z, Zhang S, Wang H, Liu Y, Xu Y, Ling J, Xu C, Zhang Y, Lv D, Yuan Z, Zhang J, Zhang Y, Shi Y, Lai M (2017) Susceptibility loci for metabolic syndrome and metabolic components identified in Han Chinese: a multi-stage genome-wide association study. J Cell Mol Med 21(6):1106–1116. https://doi.org/10.1111/jcmm.13042
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2019 Springer Nature Singapore Pte Ltd.
About this chapter

Cite this chapter
Li, W., Shen, C., Yin, L., Ge, J., Sun, A. (2019). Aldehyde Dehydrogenase 2 and Heart Failure. In: Ren, J., Zhang, Y., Ge, J. (eds) Aldehyde Dehydrogenases. Advances in Experimental Medicine and Biology, vol 1193. Springer, Singapore. https://doi.org/10.1007/978-981-13-6260-6_5
Download citation
DOI: https://doi.org/10.1007/978-981-13-6260-6_5
Published:
Publisher Name: Springer, Singapore
Print ISBN: 978-981-13-6259-0
Online ISBN: 978-981-13-6260-6
eBook Packages: Biomedical and Life SciencesBiomedical and Life Sciences (R0)