
Abstract
Circulating nucleic acids have received an increasing scrutiny over the past decade with some applications, such as in prenatal diagnosis and oncology, being on the verge of use in clinical practice. It is crucial to implement optimal standardization of pre-analytical procedures. Currently, this domain has been poorly studied and there is no well-established procedure. This chapter examines the literature on the pre-analytical factors affecting nucleic acids from blood drawing to the storage of circulating cell-free DNA extracts ready for analysis and provides some elements as guidelines for a set procedure. In particular, this chapter reports on the choice between serum and plasma as the biological source but does not concern the actual nucleic acid extraction procedures (these will be dealt with in chapter “Circulating DNA and miRNA Isolation”). Currently, the lack of a standard operating procedure for the application of blood handling in a clinical setting is due to the lack of dispensing and sharing data among researchers as well as head-to-head comparative studies between techniques. This has led to in-house specific procedures that are, undoubtedly, prejudicial to the smooth translation of nucleic acid analysis into clinical practice. Hence, the proposed procedure should overcome this gap in technique.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
1 Introduction
Despite the great interest in circulating cfNA analysis, it is not as yet transferred into clinical practice. The lack of consistency between the various procedures at each pre-analytical and analytical step constitutes one of the major hurdles for the use of cfNA analysis in routine clinical practice. In recent years, cfNA reviews have regularly highlighted the lack of standardization between the various techniques used for cfNA analysis [1–9], constituting a bias when comparing data from different laboratories.
In this chapter, we review the main factors potentially affecting circulating cfDNA analysis from blood drawing to the storage of cfDNA extracts, and finally provide an optimal guideline for the pre-analytical treatment of samples that guarantees quality analysis.
This chapter is based on data reported in the literature and our own observations [10]. Particular attention has been devoted to the study of cfDNA fragmentation considering that it is an indicator of cfDNA stability during the handling and storage of samples. Our robust and precise cfDNA quantification method enabled a precise study of both the pre-analytical handling and portability of cfDNA analysis.
2 Optimal Blood Sampling
2.1 Serum or Plasma?
2.1.1 State of the Art
The choice of matrix, i.e. serum or plasma, is the first parameter to define for the standardization of cfDNA analysis. Reported data comparing cfDNA concentrations in paired plasma and serum samples reveal that the cfDNA concentration is significantly higher in serum than in plasma [11–18]. Some of these data are summarized in Table 1.
It is now commonly hypothesized and shown that the increased levels of cfDNA in serum are due to the clotting process of white blood cells in the collection tube leading to their lysis [11, 13–15, 19]. As a consequence, cfDNA in serum is at least slightly contaminated by genomic DNA released from white blood cells and specific cfDNA is diluted by high concentrations of non-specific genomic DNA. This point is crucial for the accurate detection of rare cfDNA sequences. While it has been established for a few years that plasma is better than serum, many studies in the field are still based on serum samples, certainly due to the propensity of clinical laboratories to prepare sera conventionally and to perform retrospective studies.
2.1.2 Our Observations
We have shown unequivocally that plasma is a better source of specific tumor-derived cfDNA [20]. Using xenografted mice (n = 4) with a human colorectal cancer cell line, we showed that total murine cfDNA concentration (i.e. targeting non tumor-derived cfDNA) was higher in serum samples than in plasma samples. Conversely, when studying human cfDNA concentration (i.e. targeting specific tumor-derived cfDNA), cfDNA concentrations were higher in plasma samples (Fig. 1). This observation confirms that the increase of cfDNA in serum samples is due to the release of DNA from blood cells.

Comparison of cfDNA amounts from serum (light bars) and plasma (dark bars) preparations. cfDNA concentration in plasma and serum from SW620 xenografts was determined using the mouse KRAS M3 (a), mouse PSATI M4 (b), human KRAS H2 (c) and human PSATI H5 (d) primer sets. ctDNA concentration for each mouse (Mo1, Mo2, Mo3 and Mo4) and the corresponding tumor weight (210, 610, 710 and 2,880 mg, respectively) are shown. Values were calculated from duplicate experiments each performed twice (from [20])
As plasma appears to be more adapted for specific cfDNA analysis, this chapter further focuses mainly on the pre-analytical factors potentially affecting cfDNA in the plasma fraction. Nevertheless, we will discuss the pre-analytical treatment of serum samples in Part 8 of this chapter.
2.2 Optimal Blood Collection Tube for Plasma Preparation
Plasma is obtained conventionally by blood drawing in either EDTA or citrate or heparin blood collection tubes. Heparin is prohibited for further PCR analysis since it is an inhibitor of the PCR [21]. K3EDTA collection tubes are commonly used for cfNA analysis, but another blood collection tube should be used, Cell-free DNATM blood collection tubes, which are specifically dedicated for cfDNA analysis. They are composed of K3EDTA with an additive agent allowing the preservation of cfDNA in blood samples for up to 14 days at room temperature (RT) [22]. The additive agent stabilizes white blood cells, preventing the release of genomic DNA and inhibiting nuclease-mediated DNA degradation. In this chapter, we will mainly focus on blood collected in K3EDTA collection tubes and present some data published with Cell-free DNATM blood collection tubes.
2.3 Blood Drawing Conditions
Holdenrieder et al. [23] showed that gentle hemolysis of blood samples triggered an increase in the plasma nucleosome level. They advised that blood should be drawn carefully in order to avoid hemolysis. A similar observation was also reported by Norton et al. [24] where agitation of K3EDTA blood samples led to a significant increase in cfDNA concentration compared to non-shaken samples. We confirmed that agitation of blood samples was responsible for a two-fold increase in the cfDNA concentration compared to non-shaken samples (Fig. 2).

Influence of agitation of K3EDTA blood samples on cfDNA concentration: samples from the same donor were incubated for 3 h at RT and one of them was submitted to constant agitation
2.4 Storage Conditions of Blood Samples
As the anticoagulant effect of K3EDTA is limited over time, the main challenge in the pre-analytical treatment of blood samples is to avoid any release of genomic DNA by blood cells during storage. Generally, good practice recommends performing analysis on blood collected in EDTA collection tubes within 6 h following venipuncture as a decrease in red and white cell counts and morphology changes occur when analysis is further delayed [25]. The observed decrease in white blood cells may be due to either apoptosis or necrosis in the collection tube and lead to the release of genomic DNA from white blood cells, which may contaminate specific cfDNA. Moreover, cfDNA has also been described as being bound to the cell surface [26], assuming that nucleic acids can unbind from the cell surface and lead to an increase in cfDNA concentration with prolonged storage (see chapter “The Biology of CNAPS”). We can also hypothesize that cfDNA is actively released from blood cells in the collection tube.
Blood drawing and blood sample storage time and temperature need to be carefully defined. For these reasons, the influence of the storage time and temperature between venipuncture and plasma preparation are two parameters widely studied and reported in the literature [11, 13, 23, 27–29, 31]. It is now well known that between blood drawing and processing, cfDNA concentrations increase slightly with time, certainly due to apoptosis and necrosis of white blood cells, as described above.
2.5 cfDNA Concentration
2.5.1 State of the Art
The reported data are quite conflicting: some authors have shown a significant increase of cfDNA concentration after 2 h of storage compared to a baseline value (i.e. blood processed at t = 0), while other authors have reported this increase after 24 h. Conversely, all data have demonstrated that storage temperature (RT or +4 °C) has no influence on cfDNA concentration. Non-exhaustive data from various clinical fields are summarized in Table 2.
2.5.2 Our Observations
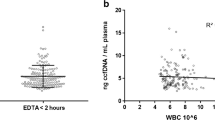
The influence of time delay and storage temperature on cfDNA concentrations between venipuncture and blood processing were tested in two different experiments. A slight increase in cfDNA concentration with time delay was observed and confirmed that storage temperature has no influence (Fig. 3a, b). Although a slight increase in the cfDNA concentration with time delay was observed, we confirmed that the cfDNA concentration did not vary significantly within 4 h following venipuncture at either RT or +4 °C. However, we demonstrated that 6 h of storage at RT triggered a two-fold increase in cfDNA concentration compared to samples processed soon after venipuncture.

(a). Influence of time delay between blood drawing and blood processing on total cfDNA concentration determined with a primer set amplifying a 105-bp sequence: samples from the same donor were incubated in different conditions. (b). Influence of time delay and temperature storage between blood drawing and blood processing on total cfDNA concentration determined with a primer set amplifying a 105-bp sequence: samples from the same donor were incubated in different conditions. Data in a and b were calculated from one either duplicate or triplicate experiment. Results were expressed as the mean (Adapted from [10])
2.6 cfDNA Fragmentation
Previous work on fetal cfDNA analysis reported the influence of time delay and temperature on cfDNA fragmentation [11] and demonstrated that fragmentation was not affected up to 6 h after blood sampling at both RT and +4 °C. Our group carefully examined the influence of these parameters on cfDNA fragmentation by determination of the DNA Integrity Index (DII: ratio of the mean cfDNA concentration determined using a primer set amplifying a 300-bp sequence to the mean cfDNA concentration determined using a primer set amplifying a 100-bp sequence), reflecting cfDNA fragmentation. We observed that the DII was not affected for up to 3 h of storage at either +4 °C or RT. However, a long delay of 6 h and sample agitation triggered a slight decrease in the DII, indicating that cfDNA may degrade with time and agitation (Fig. 4).

Influence of storage conditions on DII: DNA integrity index (ratio of the mean cfDNA concentration determined using a primer set amplifying a 300-bp sequence to the mean cfDNA concentration determined using a primer set amplifying a 100-bp sequence). Data were calculated from one either duplicate or triplicate experiment. Results were expressed as the mean
2.7 Influence of Storage Conditions on Cell-Free DNATM Blood Collection Tube-Drawn Blood Samples
The preservative agent of these tubes allows prolonged storage of blood samples at RT without any consequences on cfDNA level. Indeed, data published using these tubes report the conservation of cfDNA concentration values for up to 14 days at RT. Nevertheless, it seems that temperature variations can affect the cfDNA content and further studies need to confirm this observation. Some of the data are summarized in Table 3.
2.8 Comparison Between K3EDTA and Cell-Free DNATM Blood Collection Tubes
In the field of fetal cfDNA analysis, Hidestrand et al. [35] showed that there was no significant difference between cfDNA concentrations in samples shipped in EDTA collection tubes and samples shipped in cell-free DNATM blood collection tubes when the blood was processed immediately. However, Fernando et al. [34] demonstrated that cfDNA levels in blood samples drawn in cell-free DNATM blood collection tubes were stable for up to 14 days at RT, while they decreased when blood was drawn in K3EDTA collection tubes. Barrett et al. [28] showed that there was no significant difference for up to 3 days in the total cfDNA concentration when blood was drawn in cell-free DNATM blood collection tubes, while it increased after 24 h when blood was drawn in K3EDTA collection tubes. In the field of oncology, there are still no comparative results when blood is drawn in either EDTA tubes or cell-free DNATM blood collection tubes.
These data indicate that during this pre-analytical step, time delay and agitation should be treated with caution and in particular, the study protocol needs to define rigorously the time delay and the handling process. Agitation of blood samples should be prohibited.
2.9 Optimal Plasma Preparation
As the success of cfDNA analysis is largely dependent on the absence of contamination by genomic DNA, the main technical requirement for plasma preparation is to avoid any cell presence.
Indeed, Van Wijk et al. [36] studied the composition of plasma samples from pregnant women used to analyze cfDNA and reported the presence of fetal apoptotic cells in plasma. This was confirmed by Poon et al. [37] who found fetal cells in plasma samples from three pregnant women. This raised the following question: “Is plasma truly acellular after blood processing?”
2.9.1 State of the Art
Chiu et al. [38] studied different blood processing protocols on samples from pregnant women. They showed that a first blood centrifugation step at 1,600 g for 10 min. followed by a second plasma centrifugation step at 16,000 g for 10 min. was effective in producing cell-free plasma. cfDNA concentrations determined from these samples were similar to concentrations determined from plasma samples obtained by centrifugation followed by filtration with a 0.2 μm filter (reference protocol ensuring the production of a cell-free plasma fraction). Inversely, a unique centrifugation step at 800 g was not effective to eliminate all the cells in the plasma fraction.
Swinkels et al. [39] confirmed these results and added that the second high-speed plasma sample centrifugation step at 16,000 g can be performed either before or after storage of plasma samples at −20 °C.
Another question raised is “Does centrifugation cause the ex vivo release of DNA from blood cells?” [30]. Indeed, we can assume that a high centrifugation speed destroys blood cells and leads to release of genomic DNA. Lui et al. [30] evaluated the influence of centrifugation speeds (from 400 g to 16,000 g) on cfDNA and revealed that there was no significant difference with the speed value. However, in this study, only one blood centrifugation step was performed and each plasma sample was then filtered with a 0.2 μm filter in order to ensure truly cell-free plasma.
2.9.2 Our Observations
We proposed the following protocol for isolating cfDNA: a first blood sample centrifugation step at 1,200 g for 10 min followed by a second plasma centrifugation at 16,000 g for 10 min at +4 °C. We checked the validity of this protocol using a third centrifugation step for 10 min. at 16,000 g: (i) DNA concentrations determined from the supernatants of samples after the second and the third centrifugation step were similar; (ii) no DNA was detected in the bottom of the tube subjected to the third centrifugation step by qPCR; (iii) microscopic observation of plasma pellets after the second and the third centrifugation step revealed the absence of blood cells.
These data confirmed that the second centrifugation step is sufficient to provide quality cell-free plasma for cfDNA analysis.
3 Pre-analytical Treatment of Plasma Samples Before Nucleic Acid Extraction
Few data on this analytical step are available in the literature, even though it is a crucial phase: indeed, we can hypothesize that cfDNA structures present in the plasma are sensitive to storage conditions. In addition to chromatin or nucleosome cfDNA complexes, cfDNA may be integrated in vesicles i.e. exosomes or apoptotic bodies, or within nucleolipoprotein complex structures, such as virtosomes [40]. These forms may disintegrate with time and, as a consequence, lead to further release of detectable cfDNA in plasma samples. Time delay before extraction, temperature storage of plasma samples and freeze-thaw cycle numbers before nucleic acid extraction must be carefully specified.
3.1 Influence of Storage Conditions
3.1.1 cfDNA Concentration – State of the Art
One of the most extensive studies of this phase was by Holdenrieder et al. [41]. Even if it cannot be generalized to cfDNA analysis since the study was performed on serum and measures nucleosome levels only, this work indicates the sensitivity of nucleosomes to temperature variations: they seem to be more sensitive at +37 °C than at either +4 °C or RT. In serum samples stored at either +4 °C or RT for different lengths of time, the nucleosome level was stationary for up to 144 h of storage while at +37 °C, a significant decrease was observed after 6 h of storage. Considering that one part of cfDNA is complexed with nucleosomes, plasma samples should be stored at +4 °C or RT before nucleic acid extraction.
3.1.2 cfDNA Concentration – Our Observations
We showed that the cfDNA concentration slightly increased with time delay (from 0 to 4 h) before extraction at RT (Fig. 5a). We also tested different temperatures of storage and revealed that cfDNA concentrations were comparable when plasma samples were stored for 3 h at different temperatures (from −80 °C to RT) (Fig. 5b). However, we noted that the highest cfDNA concentrations were observed when samples were stored below +4 °C. The storage at RT triggered a slight decrease in cfDNA concentration.

(a). Influence of time delay before nucleic acids extraction on total cfDNA concentration determined with a primer set amplifying a 105-bp sequence: samples from the same donor were incubated in different conditions. (b). Influence of temperature storage between before nucleic acid extraction on total cfDNA concentration determined with a primer set amplifying a 105-bp sequence: samples from the same donor were incubated in different conditions (Adapted from [10])
3.2 cfDNA Fragmentation
We showed that the DII was not affected for up to 4 h of storage of plasma samples before extraction at RT. However, we observed also that the highest DII value was obtained when samples were stored below +4 °C as it seemed that storage at RT triggered a slight decrease of the DII value (Fig. 6a, b).

(a). Influence of time delay before nucleic acid extraction on DII: DNA integrity index (ratio of the mean cfDNA concentration determined using a primer set amplifying a 300-bp sequence to the mean cfDNA concentration determined using a primer set amplifying a 100-bp sequence). (b). Influence of temperature storage between before nucleic acid extraction on DII: DNA integrity index (ratio of the mean cfDNA concentration determined using a primer set amplifying a 300-bp sequence to the mean cfDNA concentration determined using a primer set amplifying a 100-bp sequence). Data in a and b were calculated from one either duplicate or triplicate experiment. Results were expressed as the mean (Adapted from [10])
3.3 Influence of Freeze-Thaw Cycles
3.3.1 cfDNA Concentration
Chan et al. [11] tested the influence up to three freeze-thaw cycles and showed that the cfDNA concentration was not significantly affected. We also investigated the effect of repeated freeze-thaw cycles and confirmed this observation (Fig. 7).

Influence of repeated freeze-thaw cycles on total cfDNA concentration determined with a primer set amplifying a 105-bp sequence: samples from the same donor were submitted to either 2 or 3 freeze-thaw cycles. Data were calculated from either one duplicate or triplicate experiment. Results were expressed as the mean (Adapted from [10])
3.3.2 cfDNA Fragmentation
However, it seems that repeated freeze-thaw cycles leads to cfDNA fragmentation. Chan et al. [11] showed a significant decrease in the cfDNA DII after three freeze-thaw cycles were applied to plasma samples. Such an observation confirms the sensitivity of circulating cfDNA structures to temperature variations.
We also report that after three freeze-thaw cycles applied to plasma samples, the DII significantly decreases (Fig. 8).

Influence of repeated freeze-thaw cycles on DII: DNA integrity index (ratio of the mean cfDNA concentration determined using a primer set amplifying a 300-bp sequence to the mean cfDNA concentration determined using a primer set amplifying a 100-bp sequence): samples from the same donor were submitted to either 1 or 2 or 3 freeze-thaw cycles (Adapted from [10])
These data highlight the need to carefully handle plasma samples before nucleic acid extraction.
4 Pre-analytical Treatment of cfDNA Extracts Between Nucleic Acid Extraction and cfDNA Analysis
Storage of cfDNA extracts and freeze-thaw cycle number must be carefully defined.
Chan et al. [11] showed that cfDNA concentration and fragmentation were stable in cfDNA extracts stored at −20 °C for up to three freeze-thaw cycles. We also tested the influence of freeze-thaw cycles applied to cfDNA extracts stored at −20 °C. Our results did not show any modification up to the third freeze-thaw cycle, thus confirming the observations by Chan et al. (Fig. 9a, b).

(a). Influence of cfDNA extracts freeze-thaw cycles on cfDNA concentration on total cfDNA concentration determined with a primer set amplifying a 105-bp sequence: samples from the same donor were submitted to either 1 or 2 or 3 freeze-thaw cycles. (b). Influence of cfDNA extracts freeze-thaw cycles on DII: DNA integrity index (ratio of the mean cfDNA concentration determined using a primer set amplifying a 300-bp sequence to the mean cfDNA concentration determined using a primer set amplifying a 100-bp sequence): samples from the same donor were submitted to either 1 or 2 or 3 freeze-thaw cycles (Adapted from [10])
5 Long-Term Storage of Plasma Samples and cfDNA Extracts
It is particularly important to define the duration of storage of plasma samples and cfDNA extracts for retrospective clinical studies.
5.1 State of the Art
Table 4 summarizes the main data reported in the literature [11, 42–45] on the storage of plasma samples and cfDNA extracts. Each study compares data from two consecutive tests performed at different time intervals. The results are quite conflicting and clear conclusions cannot be drawn
.
5.2 Our Observations
We performed a statistical study on the data obtained from samples used for a blinded, multicentre prospective clinical study comparing KRAS/BRAF mutational status determined from CRC plasma samples and paired CRC tumor sections (n = 106) [46]. The effects of storage at −80 °C on the cfDNA concentration were studied in 34 clinical plasma samples. Each sample was analyzed twice in the same way: extraction and immediate consecutive qPCR analysis. The time interval between the two analyses ranged from 1 to 270 days. Similarly, 25 cfDNA extracts stored at −20 °C were analyzed twice by qPCR. The time interval between the two analyses ranged from 1 to 150 days. To evaluate the effect of storage on cfDNA concentration, a variation factor, termed k, was determined (cfDNA concentration determined from the second analysis/cfDNA concentration determined from the first analysis).
The k-median values in cfDNA extracts (n = 25) and plasma samples (n = 34) were 0.88 and 1.03, respectively. No significant difference was shown between the k values in the two groups (p = 0.293). Alternatively, a significant difference was shown in the variance of the k values in the two groups (p < 0.05). The coefficient of variation of the k values in plasma samples was close to 50 %, while it was inferior to the technical coefficient of variation (24 %) for cfDNA extracts (Fig. 10a).

Variation was evaluated using factor k: fold difference between two consecutive determinations of cfDNA concentration. (a). cfDNA concentration variation represented by k in 25 DNA extracts stored at −20 °C and 34 plasma samples stored at −80 °C. (b). cfDNA concentration variation represented by k in 20 DNA extracts stored at −20 °C for a period not exceeding 3 months and in 5 DNA extracts stored for more than 3 months. (c). cfDNA concentration variation represented by k in 28 plasma samples stored at −80 °C for a period not exceeding 3 months and in six plasma samples stored for more than 3 months. cfDNA concentrations were determined using the KRAS B1/B2 primer set (ng ml-1 plasma) (Adapted from [10])
Nevertheless, the k-median value in cfDNA extracts stored for less than 3 months was 0.89, while it decreased to 0.72 when cfDNA extracts were stored for more than 3 months (Fig. 10b).
In plasma samples, the k-median value was close to 1 whatever the length of the storage time, but there was a wide variation in the k values (Fig. 10c).
These data indicate that cfDNA concentration decreases with the length of the storage time; if the analysis aims to quantify and characterize cfDNA fragmentation then working on cfDNA extracts stored for up to 3 months is preferential. However, storage time has no influence on the detection of specific sequences or mutations in cfDNA as it has been shown that mutations can be detected several years after freezing plasma samples [47]; however, the sensitivity of the technique could be compromised since specific sequences may be present in smaller quantities after a long storage time.
6 Optimal Pre-analytical Treatment of Sera Samples
6.1 From Blood Drawing to Serum Preparation
Holdenrieder et al. [23] reported an optimal handling protocol for the measurement of nucleosomes in serum samples and recommended careful blood drawing in order to avoid any hemolysis. Centrifugation for serum preparation should be performed as soon as possible since it revealed an increase in nucleosome values with time delay before blood processing. This effect is more particularly marked at both RT and +37 °C. Such an observation is also reported by Jung et al. [13]: cfDNA concentrations significantly increase after 2 h of storage of blood samples and increases even more when samples are stored at RT rather than at +4 °C.
6.2 From Serum Preparation to the Analytical Process
Holdenrieder et al. [41] analyzed preanalytical parameters on serum samples such as vortexing-rolling-shaking, storage at different temperatures for different lengths of time and freeze-thaw cycles. The authors reported that vortexing-rolling-shaking serum samples had no influence on the nucleosome content. They observed that there was a slight modification of the nucleosome concentration after three freeze-thaw cycles.
The main preanalytical parameter studied was the duration and temperature of serum sample storage before analytical processing. They showed that nucleosome concentration was stable until 7 days of storage at both RT and +4 °C while it continually decreased at +37 °C and was significantly lower after 1 day of storage. This may be explained by the thermal activation of serum nucleases or nucleosome sensitivity to heating.
6.3 Long Term Storage of Sera Samples
Holdenrieder et al. [23] studied the influence of storage of serum samples at −20 °C for 0, 1, 2, 4, and 6 months and revealed no modification of the nucleosome value content. They reported an annual 7 % loss of nucleosome content value when serum samples were stored at −70 °C [43].
7 Preanalytical Treatment for cfRNA Analysis
As with cfDNA analysis, cfRNA analysis is concerned by the influence of many preanalytical parameters. Indeed, RNA is particularly known to be labile and degradable. Moreover, ribonucleases are present at high concentrations in blood and plasma. To explain the surprisingly relative stability of cfRNA in blood, it is assumed that cfRNA is protected by other structures: lipids, proteins, and nucleosomes [48].
Here the literature data on optimal treatment of samples for cfRNA analysis is summarized (see also sections “miRNA” and “Isolation Methods”).
7.1 From Blood Drawing to Plasma or Serum Preparation
Tsui et al. [49] studied different protocols for optimal cfRNA analysis. Interestingly, they showed that there were two types of cfRNA: particle associated and non-particle associated cfRNA. In their study, they discriminated total cfRNA (particle associated and non-particle associated) and non-particle associated cfRNA obtained by plasma/serum 0.22 μm filtration.
7.1.1 Plasma Preparation from K3EDTA Blood Shipped Samples
The authors revealed that there was a significant modification of the total cfRNA yield with an increase in the time delay between venipuncture and plasma preparation at RT, while there was no significant modification when blood was stored at +4 °C. Conversely, for exclusive non-particle associated cfRNA, there was no effect of either time delay or storage temperature.
In contrast, Holford et al. [48] showed that total cfRNA concentration significantly decreased after 2 h of storage of blood samples at +4 °C.
These authors recommended processing plasma as soon as possible after venipuncture. However, in some cases, prolonged storage of blood samples is inevitable. It is clear that stringent preanalytical standardization is required when analyzing cfRNA. This is a critical issue for implementing this promising approach.
7.1.2 Plasma Preparation from cfRNA BCTs Blood Shipped Samples
Nevertheless, Fernando et al. [50] compared the stability of cfRNA in blood samples shipped in K3EDTA blood collection tubes and cell-free RNA BCTs. These specific tubes contain a chemical cocktail preventing RNA degradation by inhibition of RNAse. After 3 days of storage of blood samples at RT, the authors showed that cfRNA concentrations were stable in blood samples drawn in cfRNA BCTs while they significantly increased in K3EDTA blood samples.
7.1.3 Serum Preparation from K3EDTA Blood Shipped Samples
Tsui et al. [49] realized the same studies for serum preparation from clotted blood samples. They showed that total cfRNA concentration significantly increases with time delay before centrifugation at RT and +4 °C. Conversely, for the non-particle associated cfRNA, the time delay had no influence on its concentration.
8 Conclusions
The numerous discrepancies reported in the literature on cfDNA studies are mainly due to poor reproducibility and differences in handling procedures, thus highlighting their crucial importance. Analysis of data in the literature and our own results reveal the crucial influence of preanalytical factors on cfDNA analysis. Evaluation of all the factors potentially affecting cfDNA concentration and fragmentation leads us to describe here, for the first time, the optimal pre-analytical handling conditions for cfDNA analysis:
-
(i)
plasma is a better matrix than serum since it avoids contamination of specific cfDNA by blood-cell genomic DNA;
-
(ii)
EDTA or cell-free DNATM collection tubes prevent the release of genomic DNA by blood cells;
-
(iii)
blood must be processed within 4 h following blood drawing;
-
(iv)
high-speed centrifugation ensures the absence of any cells in the plasma and a second high-speed centrifugation step is highly recommended;
-
(v)
plasma samples are sensitive to temperature variations and freeze-thaw cycles.
-
(vi)
plasma must be aliquoted and may be stored at −80 °C for up to 9 months;
-
(vii)
cfDNA extracts may sustain a maximum of three freeze-thaw cycles and storage at −20 °C for up to 3 months for cfDNA concentration and fragmentation analysis or 9 months for specific sequence detection.
The specific guidelines for plasma cfDNA analysis at each preanalytical step are represented Fig. 11.

Specific guidelines for plasma cfDNA analysis from peripheral blood drawing to storage
Standardization of pre-analytical operating procedures would certainly consolidate the promising potential of cfDNA analysis as a powerful liquid biopsy [51–55] in the field of oncology and a diagnostic tool in prenatal diagnosis [56, 57].
Concerning cfRNA analysis, few data are available in the literature and further observations are needed for the standardization of handling procedures for cfRNAs.
References
Chan KCA, Lo YMD (2007) Circulating tumour-derived nucleic acids in cancer patients: potential applications as tumour markers. Br J Cancer 96:681–685
Fleischhacker M, Schmidt B (2007) Circulating nucleic acids (CNAs) and cancer – a survey. Biochim Biophys Acta 1775:181–232
Gormally E, Caboux E, Vineis P, Hainaut P (2007) Circulating free DNA in plasma or serum as biomarker of carcinogenesis: practical aspects and biological significance. Mutat Res 635:105–117
Johnson PJ, Lo YM (2002) Plasma nucleic acids in the diagnosis and management of malignant disease. Clin Chem 48:1186–1193
Jung K, Fleischhacker M, Rabien A (2010) Cell-free DNA in the blood as a solid tumor biomarker – a critical appraisal of the literature. Clin Chim Acta 411:1611–1624
Schwarzenbach H, Hoon DSB, Pantel K (2011) Cell-free nucleic acids as biomarkers in cancer patients. Nat Rev Cancer 11:426–447
Swarup V, Rajeswari MR (2007) Circulating (cell-free) nucleic acids – a promising, non-invasive tool for early detection of several human diseases. FEBS Lett 581:795–799
Tsang JC, Lo YM (2007) Circulating nucleic acids in plasma/serum. Pathology 39:197–207
Wagner J (2012) Free DNA – new potential analyte in clinical laboratory diagnostics? Biochem Med (Zagreb) 22:24–38
El Messaoudi S, Rolet F, Mouliere F, Thierry AR (2013) Circulating cell-free DNA analysis: preanalytical considerations. Clin Chim Acta 424:222–230
Chan KC, Yeung SW, Lui WB, Rainer TH, Lo YM (2005) Effects of preanalytical factors on the molecular size of cell-free DNA in blood. Clin Chem 51:781–784
Jen J, Wu L, Sidransky D (2000) An overview on the isolation and analysis of circulating tumor DNA in plasma and serum. Ann N Y Acad Sci 906:8–12
Jung M, Klotzek S, Lewandowski M, Fleischhacker M, Jung K (2003) Changes in concentration of DNA in serum and plasma during storage of blood samples. Clin Chem 49:1028–1029
Lee TH, Montalvo L, Chrebtow V, Busch MP (2001) Quantitation of genomic DNA in plasma and serum samples: higher concentrations of genomic DNA found in serum than in plasma. Transfusion 41:276–282
Lui YY, Chik KW, Chiu RW, Ho CY, Lam CW, Lo YM (2002) Predominant hematopoietic origin of cell-free DNA in plasma and serum after sex-mismatched bone marrow transplantation. Clin Chem 48:421–427
Steinman CR (1975) Free DNA in serum and plasma from normal adults. J Clin Invest 56:512–515
Thijssen MA, Swinkels DW, Ruers TJ, de Kok JB (2002) Difference between free circulating plasma and serum DNA in patients with colorectal liver metastases. Anticancer Res 22:421–425
Umetani N, Hiramatsu S, Hoon DS (2006) Higher amount of free circulating DNA in serum than in plasma is not mainly caused by contaminating extraneous DNA during separation. Ann N Y Acad Sci 1075:299–307
Lam NY, Rainer TH, Chiu RW, Lo YM (2004) EDTA is a better anticoagulant than heparin or citrate for delayed blood processing for plasma DNA analysis. Clin Chem 50:256–257
Thierry AR, Mouliere F, Gongora C, Ollier J, Robert B, Ychou M, Del Rio M, Molina F (2010) Origin and quantification of circulating DNA in mice with human colorectal cancer xenografts. Nucleic Acids Res 38:6159–6175
Beutler E, Gelbart T, Kuhl W (1990) Interference of heparin with the polymerase chain reaction. Biotechniques 9:166
Streck: A standardized method for sample collection, stabilization and transport of cell-free plasma DNA. http://www.streck.com/product.aspx?p=Cell-Free%20DNA%20BCT
Holdenrieder S, Stieber P, Bodenmüller H, Fertig G, Fürst H, Schmeller N, Untch M, Seidel D (2001) Nucleosomes in serum as a marker for cell death. Clin Chem Lab Med 39:596–605
Norton SE, Luna KK, Lechner JM, Qin J, Fernando MR (2013) A new blood collection device minimizes cellular DNA release during sample storage and shipping when compared to a standard device. J Clin Lab Anal 27(4):305–311
Tatsumi N, Miwa S, Lewis SM (2002) Specimen collection, storage, and transmission to the laboratory for hematological tests. Int J Hematol 75:261–268
Laktionov PP, Tamkovich SN, Rykova EY, Bryzgunova OE, Starikov AV, Kuznetsova NP, Vlassov VV (2004) Cell-surface-bound nucleic acids: free and cell-surface-bound nucleic acids in blood of healthy donors and breast cancer patients. Ann N Y Acad Sci 1022:221–227
Angert RM, LeShane ES, Lo YM, Chan LY, Delli-Bovi LC, Bianchi DW (2003) Fetal cell-free plasma DNA concentrations in maternal blood are stable 24 hours after collection: analysis of first- and third-trimester samples. Clin Chem 49:195–198
Barrett AN, Zimmermann BG, Wang D, Holloway A, Chitty LS (2011) Implementing prenatal diagnosis based on cell-free fetal DNA: accurate identification of factors affecting fetal DNA yield. PLos One 6(10):e25202
Board RE, Williams VS, Knight L, Shaw J, Greystoke A, Ranson M, Dive C, Blackhall FH, Hughes A (2008) Isolation and extraction of circulating tumor DNA from patients with small cell lung cancer. Ann N Y Acad Sci 1137:98–107
Lui YY, Chik KW, Lo YM (2002) Does centrifugation cause the ex vivo release of DNA from blood cells? Clin Chem 48:2074–2076
Xue X, Teare MD, Holen I, Zhu YM, Woll PJ (2009) Optimizing the yield and utility of circulating cell-free DNA from plasma and serum. Clin Chim Acta 404:100–104
Wong D, Moturi S, Angkachatchai V, Mueller R, DeSantis G, van den Boom D, Ehrich M (2013) Optimizing blood collection, transport and storage conditions for cell free DNA increases access to prenatal testing. Clin Biochem 46(12):1099–1104
Das K, Fernando MR, Basiaga S, Wigginton SM, Williams T (2014) Effects of a novel cell stabilizing reagent on DNA amplification by PCR as compared to traditional stabilizing reagents. Acta Histochem 116:55–60. doi:10.1016/j.acthis.2013.05.002
Fernando MR, Chen K, Norton S, Krzyzanowski G, Bourne D, Hunsley B, Ryan WL, Bassett C (2010) A new methodology to preserve the original proportion and integrity of cell-free fetal DNA in maternal plasma during sample processing and storage. Prenat Diagn 30(5):418–424
Hidestrand M, Stokowski R, Song K, Oliphant A, Deavers J, Goetsch M, Simpson P, Kuhlman R, Ames M, Mitchell M, Tomita-Mitchell A (2012) Influence of temperature during transportation on cell-free DNA analysis. Fetal Diagn Ther 31:122–128
van Wijk IJ, de Hoon AC, Jurhawan R, Tjoa ML, Griffioen S, Mulders MA, van Vugt JM, Oudejans CB (2000) Detection of apoptotic fetal cells in plasma of pregnant women. Clin Chem 46:729–731
Poon LL, Leung TN, Lau TK, Lo YM (2000) Prenatal detection of fetal Down’s syndrome from maternal plasma. Lancet 356:1819–1820
Chiu RW, Poon LL, Lau TK, Leung TN, Wong EM, Lo YM (2001) Effects of blood-processing protocols on fetal and total DNA quantification in maternal plasma. Clin Chem 47:1607–1613
Swinkels DW, Wiegerinck E, Steegers EA, de Kok JB (2003) Effects of blood-processing protocols on cell-free DNA quantification in plasma. Clin Chem 49:525–526
Gahan PB, Stroun M (2010) The virtosome-a novel cytosolic informative entity and intercellular messenger. Cell Biochem Funct 28:529–538
Holdenrieder S, Mueller S, Stieber P (2005) Stability of nucleosomal DNA fragments in serum. Clin Chem 51:1026–1029
Frattini M, Balestra D, Verderio P, Gallino G, Leo E, Sozzi G, Pierotti MA, Daidone MG (2005) Reproducibility of a semiquantitative measurement of circulating DNA in plasma from neoplastic patients. J Clin Oncol 23:3163–3164
Holdenrieder S, Von Pawel J, Nagel D, Stieber P (2010) Long-term stability of circulating nucleosomes in serum. Anticancer Res 30:1613–1615
Lee T, LeShane ES, Messerlian GM, Canick JA, Farina A, Heber WW, Bianchi DW (2002) Down syndrome and cell-free fetal DNA in archived maternal serum. Am J Obstet Gynecol 187:1217–1221
Sozzi G, Roz L, Conte D, Mariani L, Andriani F, Verderio P, Pastorino U (2005) Effects of prolonged storage of whole plasma or isolated plasma DNA on the results of circulating DNA quantification assays. J Natl Cancer Inst 97:1848–1850
Thierry AR, Mouliere F, El Messaoudi S, Mollevi C, Lopez-Crapez E, Rolet F, Gillet B, Gongora C, Dechelotte P, Robert B, Del Rio M, Lamy PJ, Bibeau F, Nouaille M, Loriot V, Jarrousse AS, Molina F, Mathonnet M, Pezet D, Ychou M (2014) Clinical validation of the detection of KRAS and BRAF mutations from circulating tumor DNA. Nat Med 20(4):430–435
Kopreski MS, Benko FA, Kwee C, Leitzel KE, Eskander E, Lipton A, Gocke CD (1997) Detection of mutant K-ras DNA in plasma or serum of patients with colorectal cancer. Br J Cancer 76:1293–1299
Holford NC, Sandhu HS, Thakkar H, Butt AN, Swaminathan R (2008) Stability of beta-actin mRNA in plasma. Ann N Y Acad Sci 1137:108–111
Tsui NB, Ng EK, Lo YM (2002) Stability of endogenous and added RNA in blood specimens, serum, and plasma. Clin Chem 48(10):1647–1653
Fernando MR, Norton SE, Luna KK, Lechner JM, Qin J (2012) Stabilization of cell-free RNA in blood samples using a new collection device. Clin Biochem 45(16–17):1497–1502
Diaz LA Jr, Williams RT, Wu J, Kinde I, Hecht JR, Berlin J, Allen B, Bozic I, Reiter JG, Nowak MA, Kinzler KW, Oliner KS, Vogelstein B (2012) The molecular evolution of acquired resistance to targeted EGFR blockade in colorectal cancers. Nature 486:537–540
Misale S, Yaeger R, Hobor S, Scala E, Janakiraman M, Liska D, Valtorta E, Schiavo R, Buscarino M, Siravegna G, Bencardino K, Cercek A, Chen CT, Veronese S, Zanon C, Sartore-Bianchi A, Gambacorta M, Gallicchio M, Vakiani E, Boscaro V, Medico E, Weiser M, Siena S, Di Nicolantonio F, Solit D, Bardelli A (2012) Emergence of KRAS mutations and acquired resistance to anti-EGFR therapy in colorectal cancer. Nature 486:532–536
Mouliere F, El Messaoudi S, Gongora C, Guedj AS, Robert B, Del Rio M, Molina F, Lamy PJ, Lopez-Crapez E, Mathonnet M, Ychou M, Pezet D, Thierry AR (2013) Circulating cell-free DNA from colorectal cancer patients may reveal high KRAS or BRAF mutation load. Transl Oncol 6(3):319–328
Mouliere F, El Messaoudi S, Pang D, Dritschilo A, Thierry AR (2014) Multi-marker analysis of circulating cell-free DNA toward personalized medicine for colorectal cancer. Mol Oncol 8(5):927–941
Murtaza M, Dawson SJ, Tsui DW, Gale D, Forshew T, Piskorz AM, Parkinson C, Chin SF, Kingsbury Z, Wong AS, Marass F, Humphray S, Hadfield J, Bentley D, Chin TM, Brenton JD, Caldas C, Rosenfeld N (2013) Non-invasive analysis of acquired resistance to cancer therapy by sequencing of plasma DNA. Nature 497:108–112
Shea JL, Diamandis EP, Hoffman B, Lo YM, Canick J, van den Boom D (2013) A new era in prenatal diagnosis: the use of cell-free fetal DNA in maternal circulation for detection of chromosomal aneuploidies. Clin Chem 59(8):1151–1159
Srinivasan A, Bianchi DW, Huang H, Sehnert AJ, Rava RP (2013) Noninvasive detection of fetal subchromosome abnormalities via deep sequencing of maternal plasma. Am J Hum Genet 92:167–176
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2015 Springer Science+Business Media Dordrecht
About this chapter
Cite this chapter
El Messaoudi, S., Thierry, A.R. (2015). Pre-analytical Requirements for Analyzing Nucleic Acids from Blood. In: Gahan, P. (eds) Circulating Nucleic Acids in Early Diagnosis, Prognosis and Treatment Monitoring. Advances in Predictive, Preventive and Personalised Medicine, vol 5. Springer, Dordrecht. https://doi.org/10.1007/978-94-017-9168-7_3
Download citation
DOI: https://doi.org/10.1007/978-94-017-9168-7_3
Published:
Publisher Name: Springer, Dordrecht
Print ISBN: 978-94-017-9167-0
Online ISBN: 978-94-017-9168-7
eBook Packages: MedicineMedicine (R0)