
Abstract
From episodic crises and epidemiological studies of the past decades, air pollution is identified as the most important environmental determinant of human health, and this is supported by experimental studies in animals. Findings of these studies indicate that short- and long-term exposure to air pollution increases the risk for lung cancer, pulmonary and cardiovascular diseases, diabetes, and neurodegenerative disorders, all of which cause morbidity and mortality in humans. Polluted air is a complex mixture of gases (e.g., carbon monoxide and dioxide, ozone, nitric oxide, sulfur- and nitrogen dioxide), volatiles (e.g., hydrocarbons, aldehydes), and particulate matter, which affect multiple organ systems and cell types, leading to a variety of negative health consequences. The adverse health effects of air pollution appear to be, in part, mechanistically driven by the induction of both pulmonary and systemic oxidative stress. Many exposure studies using a variety of techniques have demonstrated increased oxidative stress in pulmonary and cardiovascular compartments that trigger lipid peroxidation and downstream inflammatory signaling. In this chapter, we review the evidence linking air pollutant-induced oxidative stress with specific pulmonary and cardiovascular outcomes of air pollution.
Access provided by Autonomous University of Puebla. Download reference work entry PDF
Similar content being viewed by others


Keywords
- NADPH Oxidase
- Total Antioxidant Capacity
- Ultrafine Particle
- Diesel Exhaust Particle
- Environmental Tobacco Smoke Exposure
These keywords were added by machine and not by the authors. This process is experimental and the keywords may be updated as the learning algorithm improves.
Introduction
It has been known for a long time that air pollution affects human health. Incidences such as the “Belgium Killer Fog” in the Meuse Valley in 1930 and in Donora in 1948 and the “London Smog” in 1952 have shown us clearly that exposure to air pollution could have adverse health effects. The “London Smog” caused an estimated increase of 4,000 direct fatalities and 12,000 deaths over the time period from December 1952 to February 1953 (Bell and Davis 2001). An increase in air pollution of about 9–15-fold during the London episode (between December 3 and 9) increased the mortality rates by 50–300 % in the following month (Bell and Davis 2001). Since then many epidemiological studies have identified an important role of air pollution in human health. These studies suggest that short-term and long-term exposure to air pollution increases morbidity and mortality, hospital admission, and the rates of lung cancer, pulmonary and cardiovascular disease, diabetes, and neurodegenerative disorders (Brook et al. 2004; Dockery et al. 1993; Pearson et al. 2010; Pope et al. 2004; Griffith and Levin 1989; Schneider et al. 2008; Zanobetti et al. 2003). Results from these epidemiological studies indicate a strong correlation between exposures to increased levels of air pollution and human health and are supported by several animal studies (Sun et al. 2009; Pinkerton et al. 2008; Nurkiewicz et al. 2011; Lei et al. 2005; Laskin et al. 2010; Kodavanti et al. 2003; Ghio and Devlin 2001; Happo et al. 2013; Bhatnagar 2004; Bhatnagar 2006). The adverse health effects of air pollution appear to be, in part, mechanistically driven by the induction of both pulmonary and systemic oxidative stress. In this chapter, we will discuss the evidence linking oxidative stress and specific pulmonary and cardiovascular effects of air pollution.
Air Pollution
Air Pollution and Oxidative Stress
Oxidative stress results from an increased production of reactive oxygen species causing an imbalance of the prooxidant-antioxidant equilibrium (Wellenius et al. 2012). The overproduction of reactive oxygen species (ROS) such as superoxide (O2 •−), hydroxyl radicals (•HO), and hydrogen peroxide (H2O2) or reactive nitrogen species (RNS) such as nitric oxide (NO•) and peroxynitrite (OONO−) can lead to the oxidation of biological molecules such as nucleic acids, proteins, and lipids and alter their function (Droge 2002; Sakamoto et al. 2007; Ghio et al. 2012). Under conditions, when ROS production overwhelms the biological antioxidant defense, cellular damage and impaired cell function as well as an increase in inflammation can result in tissue injury triggering the development of a variety of disorders such as cardiovascular and neurodegenerative diseases, atherosclerosis, cancer, and diabetes (Valavanidis et al. 2008; Franchini and Mannucci 2011; Griffith and Levin 1989; Brook et al. 2003).
Air pollution refers to a complex mixture of gases (e.g., carbon monoxide and dioxide, ozone, nitric oxide, sulfur and nitrogen dioxide), volatiles (e.g., hydrocarbons, aldehydes), and particulate matter. It is currently believed that particulate matter (PM) can induce oxidative stress directly, mainly via its organic and metal constituents, or indirectly by the activation of proinflammatory host defense mechanisms (Ghio et al. 2012). PM contains organic components, such as highly redox-active quinones that can generate ROS (Roberts and Martin 2007; Kumagai et al. 2002; Valavanidis et al. 2005; Banerjee et al. 2009) or polycyclic aromatic hydrocarbons, which can induce oxidative stress via cytochrome P450 (Bae et al. 2010; Pinkerton et al. 2008). Furthermore, PM contains redox-active metals such as iron (Fe) and nickel (Ni) that can induce the production of ROS and RNS by directly supporting electron transport (Colburn and Johnson 2003; Shinyashiki et al. 2009; Xu et al. 2012). The induction of oxidative stress by PM consequently contributes to the particle-induced inflammation by activating macrophages and neutrophils (Becker et al. 2005; Cao et al. 2007). The activation of phagocytotic cells triggers particle uptake what further accelerates ROS production (Goldsmith et al. 1997; Haberzettl et al. 2007). Moreover activation of macrophages and neutrophils as well as particle uptake triggers the release of proinflammatory mediators which in turn recruit more proinflammatory cells (Larson and Rosen 2002). This fuels a vicious cycle, in which increasing ROS/RNS generation and proinflammatory signaling lead to the acceleration of oxidative stress that is thought to be involved in the development of particle-induced pathology.
Particulate Matter (PM)
Particle Size, Composition, and Distribution
Particle Size and Particle Deposition
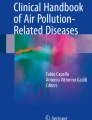
Particulate matter (PM) is a mixture of different-sized particles defined by their size into coarse (particles <10 μm in aerodynamic diameter, PM10), fine (particles ≤2.5 μm, PM2.5), and ultrafine (particles <0.1 μm, PM0.1) particles. Coarse particles are crustal materials derived from farming, mining, construction work, volcanic ash, wood burning, and vehicular and industrial processes (e.g., tire erosion). Fine and ultrafine particles are primarily products of combustion-derived processes (fossil fuels) used in mobile sources, e.g., vehicle traffic, and fixed industrial sources such as coal-fired power plants (see Fig. 69.1). The size of particles >0.5 μm is quantified by the aerodynamic diameter, determined by their transport in the gas phase (Willeke and Baron 1990; Stahlhofen et al. 1980). Particles <0.5 μm are enumerated by their thermodynamic diameter, because the transportation of these particles is predominantly influenced by diffusion and defined by their thermodynamic behavior in the gas phase (Heyder 1982). Because both aerodynamic and thermodynamic behaviors are affected by particle shape, shape is another important particle parameter, which ranges from perfect spheres to elongated fibers (Hofmann et al. 2009; Dai and Yu 1998).

Source, size, and body distribution of particulate matter (PM). PM originates from sources such as farming, wood fires, and traffic and industrial sources and depending upon its size can reach the lower regions of the respiratory tract into alveolar regions
Particle size and shape are important factors as they determine entry, penetration, body deposition, and clearance and consequently define the location in which they could contribute to the induction of oxidative stress (Fig. 69.1). Coarse particles (PM10) can only enter and deposit in the upper respiratory tract and are cleared by mucociliary clearance. In contrast, fine (PM2.5) and ultrafine particulate matter can reach the alveolar regions of the lungs. Moreover, ultrafine particles can pass through the alveolar epithelium and accumulate in the lung interstitium or reach the brain via the olfactory bulb (Oberdorster et al. 2005). Ultrafine PM might even pass from the lung into the circulation (Bates 1995; Bhopal et al. 1994). The distribution in the body is also dependent on the particle shape. For instance fibers such as asbestos can be up to 10 μm long and can reach the deeper respiratory tract as they can align perfectly in inhaled gas phase (Harris and Timbrell 1975). Moreover, particle size and shape are important factors that determine particle clearance, for example, particle uptake by macrophages is a function of size, shape, and surface characteristics and, thus, important factors for lung clearance (Semmler et al. 2004; Oberdorster et al. 1992; Albrecht et al. 2007). Particle size is a determining factor of biological deposition during exposure, and thus, it is a critical factor that contributes to the pathogenicity of respirable PM. Yet, because of the complex composition of PM, size alone is insufficient to completely explain PM-dependent toxicity.
Particle Concentration and Composition
Ambient particle concentrations are defined either as particle number concentration (typical environmental range: 102–105 particles/m3), which is mainly controlled by the ultrafine particle fraction, or as particle mass concentration (typical environmental range 1–100 μg/m3), primarily dominated by the fine particle fraction (Brauer et al. 2012). The 24 h USEPA National Ambient Air Quality Standards (NAAQS) are 35 μg/m3 or 150 μg/m3 for PM2.5 or PM10, respectively (National Ambient Air Quality Standards, http://www.epa.gov/air/criteria.html). Furthermore, the air quality index classifies PM2.5 and PM10 levels into categories reaching from good (PM2.5, 0–15 μg/m3; PM10, 0–50 μg/m3; no protection needed), moderate (PM2.5: 16–35 μg/m3, PM10: 51–154 μg/m3), unhealthy for sensitive groups (PM2.5, 36–150 μg/m3; PM10, 155–354 μg/m3), and very unhealthy (PM2.5, >150 μg/m3; PM10, >354 μg/m3; outdoor activities should be avoided, and susceptible groups should remain indoors) (Anderson et al. 2012). However, no threshold can be set for the risks that accompany PM exposure; therefore in 2005 the WHO set air quality guidelines of 25 or 50 μg/m3 for 24 h mean and 10 or 20 μg/m3 annual mean for PM2.5 or PM10, respectively (http://www.who.int/mediacenter/factsheet/fs313/en/index.html), to minimize effects on human health. Although regulations have reduced PM levels, PM levels in many places around the world still exceed the WHO guidelines. In the USA, the average range for PM2.5 is 5–50 μg/m3 and for PM10 is 10–100 μg/m3 with peak concentrations of 100 μg/m3 (PM2.5) or 300 μg/m3 (PM10) (Brook et al. 2010). In heavily polluted cities such as Delhi and Beijing, the annual average PM10 concentrations are 198 μg/m3 and 121 μg/m3, respectively (see WHO, OAP database). Similarly, annual PM2.5 reaches mean concentrations of 148.4 μg/m3 in Delhi (Dey et al. 2012) and 71.8–191.2 μg/m3 in Beijing, Tianjin, and Hebei (Zhao et al. 2013). In comparison, PM2.5 concentrations during occupational exposures known to be hazardous, e.g., of wildland firefighters or construction workers, range from 5.9 to 2,673 μg/m3 (Adetona et al. 2011) and 50 to 34,000 μg/m3 (Peters et al. 2009). Collectively, these data indicate that urban levels of PM2.5 in the rapidly developing countries are reaching levels deleterious to human health.
PM is a complex mixture that varies in concentration and composition due to the source as well as to season and meteorological conditions (e.g., temperature, wind, humidity). Ambient PM consists of organic (OC) and elemental (EC) carbon, sulfate, nitrate, and ammonium along with many elements such as sulfur, silica, and metals (e.g., iron, nickel, aluminum) (Xu et al. 2012; Bell 2012; O’Toole et al. 2010; Haberzettl et al. 2012; Chen et al. 2003). Different-sized particles have a different composition as PM10 particles are derived from crustal materials while fine and ultrafine particles are primarily products of combustion-derived processes (see Fig. 69.1). The composition of air pollution is mainly dependent on the source such as in urban areas, for example, the combustion of fossil fuels by industry, vehicles, or households, or in rural areas on processes like farming and mining. Other important factors that determine the composition and concentration of air pollution are geographical, seasonal, and meteorological factors as well as time (Becker et al. 2005; Junk et al. 2003; Wang and Lu 2006; Garcia-Suastegui et al. 2011; Forsberg et al. 1993). The air quality in the Utah Valley region depends on the topology and meteorological conditions; for example, during winter a low-pressure system can be trapped on the valley floor by a rapidly moving high-pressure system, a condition termed an inversion. During an inversion, emissions from vehicles, industry, and houses are trapped in the valley leading to a rapid, overall increase in air pollution including PM (Franchini and Mannucci 2009). At one time, a primary source of metal-rich PM in the valley was a steel mill. When the steel mill temporarily closed, it created conditions for a natural experiment because the PM levels increased by 2-fold in winter months when the mill was open compared with levels when the mill was closed (Franchini and Mannucci 2009). Subsequent reopening of the mill corresponded with a 2–3-fold increase in hospital admission of children (Roman et al. 2009) indicating that PM from the mill was responsible for inducing untoward health effects. This also suggested that PM toxicity depends in part upon both the concentration and the composition of the ambient air particles.
Particle Composition and Toxicity
Particle concentration and size are important aspects of PM toxicity, because they define number and surface area and determine deposition and elimination. Smaller particles have a greater surface area and have therefore a higher capacity to bind and transport toxic substances. For instance, a mass concentration of 10 μg/m3 consists of 1.2 million particles with a diameter of 2 μm comprising a surface area of 24 μm2/mL, whereas the same mass concentration of 10 μg/m3 consists of 2.4 million particles with a diameter of 20 nm with a surface area of 3,016 μm2/mL (Moghimi et al. 2005). Therefore, it has been suggested that particle surface area rather than the particle mass be used as the primary metric for particle dose (Oberdorster et al. 1994; Oberdorster et al. 2005; Brown et al. 2001). In addition to size and concentration, composition is another important aspect of PM toxicity. Different components are expected to trigger different biological responses, and one component is likely to be more potent than another. Specific particle components are associated with specific pathologies. One classic example is chronic exposure to silica, an element in coal mine dust leading to the development of silicosis (Kuempel et al. 2003; Castranova and Vallyathan 2000). Organic compounds such as poly-aromatic hydrocarbons (PAH) have been associated with allergic airway disease (Diaz-Sanchez 1997), while particle-associated metals such as vanadium induce airway fibrosis (Bonner et al. 2000). Carbon black, SO2, NO2, and chlorine concentration in PM appear to increase the risk of cardiovascular disease (Pereira Filho et al. 2008; Reis et al. 2009; Wheeler et al. 2011).
Epidemiological studies have demonstrated an association between an increase in mortality and the particle content of metals including iron, nickel, zinc, and lead (Laden et al. 2000; Burnett et al. 2000). PM samples in the Utah Valley collected at times when the steel mill was closed had a lower metal content and a decrease in PM-induced biological effects than PM collected at times when the steel mill was active (Dye et al. 2001; Frampton et al. 1999), indicating that a higher metal content increases the biological activity of this PM. Similarly, a study performed in Germany showed that exposure to metal-rich PM increases airway inflammation (Schaumann et al. 2004). Metals are also suggested to play a role in PM-induced cardiovascular effects. Redox-active metals such as copper, zinc, vanadium, and nickel have been associated with myocardial injury, arrhythmias, and decreases in vasoconstriction and vasodilatation (Kodavanti et al. 2003; Campen et al. 2001; Campen et al. 2002; Li et al. 2005; Bagate et al. 2006). Mechanistically, particle-associated metals such as iron, copper, vanadium, and nickel are thought to be directly involved in the particle-induced oxidative stress. Several studies demonstrate an association between the concentration of redox-active metals in PM with the formation of reactive oxygen species (ROS) and proinflammatory responses (Kadiiska et al. 1997; Lewis et al. 2003; Valavanidis et al. 2005), while other studies have been unsuccessful in demonstrating such dependency (Veranth et al. 2006; Brown et al. 2000). Organic compounds such as PAH have been demonstrated to have genotoxic and cytotoxic potential as well. Epidemiological and experimental studies indicate the carcinogenic and allergic potential of organic compounds in wood smoke and ambient and traffic-related PM (Hernandez-Garduno et al. 2004; Binkova et al. 2003; Suzuki et al. 1993). The potential of organic compounds to induce ROS-dependent cytotoxicity and proinflammatory responses has been demonstrated for organic extract of diesel exhaust particles (DEP) (Hiura et al. 1999; Ohtoshi et al. 1998; Boland et al. 2000). Similarly, endotoxins (e.g., lipopolysaccharide, LPS) are another organic component found in fine and coarse particles that can also induce oxidative stress and inflammation, e.g., via activation of macrophages (Monn et al. 2002; Welty et al. 2009).
Air Pollution and Epidemiology
Since the observation of the adverse health effects of air pollution in the “London Smog” episode, epidemiological studies over the past few decades have provided additional evidence of a strong association between air pollution and all cause morbidity and mortality (Zanobetti et al. 2002; Dominici et al. 2007; Bhatnagar 2006). A study performed across 20 US cities demonstrated that an increase of PM10 by 10 μg/m3 enhanced the daily mortality by 0.5 % (Samet et al. 2000). The Harvard Six Cities Study demonstrated decreased life expectancy in populations living in areas with higher levels of air pollution (Dockery et al. 1993). Furthermore, a positive correlation was found between the mortality due to lung cancer and cardiopulmonary disease (Dockery et al. 1993). Similarly, other extensive epidemiological studies indicate a strong, positive correlation between exposure to airborne particulate matter (PM) and pulmonary and cardiovascular morbidity and mortality (Zanobetti et al. 2000; Pope 2004; Braga et al. 2000; Pope et al. 2008). The strongest correlation between mortality and PM was found for fine particulate matter (PM2.5) derived from combustion (Dockery et al. 1993; Laden et al. 2000; Pope et al. 2002). Short-term exposure to PM is associated with an increase in the risk of myocardial infarction, arrhythmias, endothelial dysfunction, stroke, and thrombosis, whereas chronic exposures increase atherogenesis, the risk of mortality due to ischemic heart disease, arrhythmias, and heart failure (Bhatnagar 2006; Riles and Brook 2011; Brook and Brook 2011; Brook et al. 2010). Data from both human and animal studies indicate that changes in endothelial cell function are early and sensitive outcomes of PM exposure (Brook et al. 2009; Courtois et al. 2008). Recent epidemiological studies also suggest that exposure to air pollutants enhances the prevalence for type 2 diabetes (T2D) (Kramer et al. 2010; Puett et al. 2011; Coogan et al. 2012; Rajagopalan and Brook 2012).
Air Pollution and Mechanism(s) of Action
Although epidemiological studies have found strong evidence for the effects of PM on human health and many experimental studies suggest the involvement of pulmonary as well as systemic oxidative stress, no specific mechanism(s) has been identified. So far, it has been suggested that the adverse health outcomes after exposure to ambient particulate matter are attributable to three major pathways: (1) inhaled particulate matter induces oxidative stress and in turn inflammation in the lungs that then extends to systemic oxidative stress causing cardiovascular effects; (2) the ultrafine/nanosized particles (PM0.1) may enter the bloodstream and affect vascular health by direct interactions with the blood cells and the endothelium; and (3) particulate matter stimulates sensory receptors in the lung and induce cardiovascular effects via the central nervous system; however, these postulated mechanisms should not be considered to be mutually exclusive (Fig. 69.2). Furthermore, soluble compounds of particles are important for the biological action of PM and can have widespread peripheral (whole-body) distribution. For example, inhaled particles come in contact with the lung lining fluid (e.g., mucus, surfactant) dissolving the soluble particle fractions such as metals or organic components (e.g., poly-aromatic hydrocarbons, PAH). Thus, the leaching of soluble components can then induce effects in the lung or potentially distribute throughout the body causing toxic effects in many other organs besides the lung (Patton et al. 2004).

Hypothetical mechanism(s) of particle-induced cardiovascular injury. PM-induced oxidative stress and inflammation, PM-triggered stimulation of sensory nerves in the lung, and translocation of ultrafine PM are all viable hypotheses to explain the increased disease risk after exposure to environmental particulate air pollution
Air Pollution, Oxidative Stress, and Lung Disease
Particle-Induced Lung Disease
Exposure to particulate matter (PM) is associated with an increase in hospital admission for lung disease (Zanobetti et al. 2000), and exposure to air pollution stimulates oxidative stress and inflammation in the lung. The induction of pulmonary oxidative stress and inflammation is described for the exposure to ozone, NOx, and PM (Yang and Omaye 2009; Happo et al. 2013; Triantaphyllopoulos et al. 2011). PM induces the activation of alveolar macrophages and neutrophils that release reactive oxygen species (ROS) and cytokines inducing an inflammatory response in the lung (Danielsen et al. 2010; Seagrave et al. 2008; Becker et al. 2005). PM can also contain fungi spores and endotoxins that may further trigger lung inflammation and the generation of ROS (Schins et al. 2004). Inhalation of coal and silica mine dust induces oxidative stress that can lead to the development of fibrotic lung diseases (Castranova and Vallyathan 2000). Furthermore, exposure to air pollution increases the risk for chronic obstructive pulmonary disease (COPD), chronic bronchitis, asthma, and pneumonia infection (Grievink et al. 2000; Zanobetti et al. 2008; Lindgren et al. 2009; Peel et al. 2005). Allergic disease and asthma are increasing with rising traffic-related air pollution, and epidemiological studies have demonstrated that the rate of childhood asthma is significantly associated with PM10 exposure (Peters et al. 1997). A possible mechanism is that the exposure to air pollution causes oxidative damage of the bronchial epithelium and cilia (see Section Oxidative Stress in the Lung) resulting in a longer retention time of allergens on the epithelial surface. Although smoking is the strongest risk factor, exposure to PM also correlates with an increased risk for the development of lung cancer (Dockery et al. 1993; Pope et al. 1995; de Groot and Munden 2012). However, a clear mechanism for the carcinogenic effect of PM has remained elusive. One possible mechanism could be increased ROS formation. In vitro experiments have shown that the exposure to environmental particles induces the formation of hydroxyl radicals (•HO) and 8-hydroxydeoxyguanine (8-OHdG) in a lung epithelial cell line (Knaapen et al. 2002). The formation of the DNA modification 8-OHdG, an indicator of oxidative DNA damage, is found to be increased in mice exposed to diesel exhaust particles (DEP), and 8-OHdG levels correlate with the formation of lung tumors in exposed mice (Sato et al. 2000). Another hypothesis is that PM induces lung cancer by the induction of an inflammatory response independent of carcinogenic particle components (Borm et al. 2004; Harrison et al. 2004).
Oxidative Stress in the Lung
Combined in vitro and in vivo studies support the idea that respirable particles can induce pulmonary oxidative stress (Sagai et al. 1993; Li et al. 1996). The primary function of the lungs is gas exchange, which requires the inhalation of large amounts of ambient air. Consequently, the lung is exposed to large amounts of respirable airborne particulate matter entering the lung, which needs to be removed. For this, the lung is equipped with specialized host defense machinery, which depends on the interaction between particles and cells (e.g., alveolar macrophages) or fluids. Particle size and composition are determining factors for the interaction with the extracellular and intracellular lung defense mechanisms and, consequently, the induction of oxidative stress in the respiratory system.
The respiratory lining fluid completely covers the respiratory tract epithelium from the nasal mucosa to the alveoli. This inhomogeneous fluid layer covers the sensitive respiratory epithelial cells and is the first line of protection against oxidative stress. Particles larger than 10 μm diameter (PM10) are removed mechanically by sneezing, coughing, or swallowing and are eliminated by the mucociliary escalator in the conducting airways. Respirable particles are trapped in the upper viscous mucus, a layer of highly glycosylated proteins – mucins – which are produced by airway epithelial, goblet, and mucus cells. The trapped particles are removed from the airways by movement of the ciliated epithelium supported by the resistance reducing watery sub-layer. The NO-dependent (Stout et al. 2007) cilia movement (or beating) can be upregulated by products of inflammatory cells such as cytokines (e.g., TNF-α). On the other hand, oxidants such as hydrogen peroxide (H2O2) and superoxide (O2 −•) can damage the cilia decreasing ciliary function. Hydrogen peroxide at relatively low concentration significantly impairs cilia beating and can result in cilia denudation (Feldman et al. 1994; Al-Shmgani et al. 2012), and likewise exposure to air pollution could damage the ciliated epithelium and alter cilia function (Pedersen 1990). Furthermore, oxidative stress causes mucus hypersecretion (Yoshida and Tuder 2007). Hypersecretion of mucus and impaired mucociliary clearance stimulated by oxidants can lead to airway mucus accumulation and reduced airflow (Nadel 2001; Rogers 2001).
The composition of the lining fluid changes in the deeper regions of the lungs. In the distal region and the alveoli, the mucus in the respiratory lining fluid is replaced by surfactant. Surfactant is a lipoprotein complex, which plays an important role in the stabilization of the alveoli as well as in the pulmonary host defense. In vitro experiments using synthetic lung epithelial lining fluid (sELF) demonstrated that residual oil fly ash (ROFA), a component of ambient PM, can initiate the oxidation of sELF (Sun et al. 2001). Surfactant proteins are important in the recognition and opsonization of pathogen, and their antioxidant capacity prevents lipid peroxidation and oxidative damage (McNeely and Coonrod 1994; Bridges et al. 2000), and binding of surfactant proteins to the particle surface not only alters the redox state of the lung milieu but also modifies the particle properties and their toxicity (Rehn et al. 2003; Kendall et al. 2004).
Furthermore, airway epithelial cells release other substances such as antioxidants and iron-binding proteins to protect against oxidative damage. Estimates based on the analysis of human bronchoalveolar lavage fluid (BALF) show that the respiratory lining fluid contains 40–370 μM urate, 45–170 μM GSH, approximately 50 μM ascorbate, and 1 μM α-tocopherol (van der Vliet et al. 1999). These molecules are excellent radical scavengers, i.e., these react with most radicals and oxidants. Moreover, the respiratory lining fluid contains antioxidant enzymes such as extracellular superoxide dismutase (ecSOD), catalase, and glutathione peroxidase (GPx) that protect against oxidative damage (Avissar et al. 1996; Oury et al. 1994; Hassing et al. 2009). Effects of ambient particles on these antioxidant proteins have been shown for instance by the instillation of respirable environmental PM which resulted in an increase in lipid peroxidation and a decrease in the antioxidant enzymes, SOD and catalase, in rats (Pradhan et al. 2005). Furthermore, overexpression of ecSOD protects against ROFA-induced injury (Ghio et al. 2002), further emphasizing the importance of the lung antioxidant system against PM toxicity.
Alveolar macrophages, which reside in the alveoli of the lung, are the first line of cellular host defense. Alveolar macrophages have two functions: (1) phagocytosis of invading pathogens and respirable particles and (2) synthesis and secretion of anti- and proinflammatory mediators. The uptake of particles by macrophages leads to the generation of ROS, cytokines, chemokines, and growth factors. Several studies demonstrate a connection between macrophage uptake of different environmental particles and the generation of ROS, ultimately leading to the production of TNF-α (Imrich et al. 1999; Nemmar et al. 2006; Albrecht et al. 2005; Haberzettl et al. 2007). The enzyme nicotinamide adenine dinucleotide phosphate (NADPH) oxidase is responsible for the “respiratory burst” (an increase of oxygen consumption of phagocytes exposed to pathogens) (Babior 1999; Park 2003). The activation of the enzyme is triggered by the activation of different surface receptors (e.g., CR3, FcγR) and depends on a functional actin cytoskeleton (Babior 1999; Park 2003). After stimulation, the cytosolic p40phox/p47phox/p67phox unit forms a membrane-bound complex with the membranous p22phox/gp91phox unit of the enzyme leading to the activation of the NADPH oxidase and the generation of ROS. Prevention of the uptake of silica particles by inhibition or depletion of the actin cytoskeleton, scavenger receptor, or FcγRII reduces ROS production and the induction of an inflammatory response and protects against lung injury (Kobzik 1995; Beamer and Holian 2005; Haberzettl et al. 2008). Recent studies indicate that pulmonary ROS initiates lipid peroxidation and accumulation of lipid aldehydes, e.g., POVPC, that can activate TLR4 receptor, and thus, lipid-derived aldehydes act as triggers of the inflammatory response (Kampfrath et al. 2011). Following TLR4 activation, NADPH oxidase assembles and promotes an increasing level of ROS, then more lipid peroxidation and more POVPC, and a positive feedback cycle ensues leading ultimately to cytokine/chemokine transcription, translation, and secretion (Conklin 2011) (Fig. 69.3).

Induction of oxidative stress and lipid peroxidation in the lungs triggers particle-induced vascular injury (Adapted with permission from Conklin 2011 from an illustration by Cosmocyte/Ikumi Kayama)
Air Pollution and Cardiovascular Effects
Evidence for Vascular Oxidative Stress in Environmental Exposures
Blood Space
Plasma/Serum
Antioxidants and lipoproteins represent major acellular components readily oxidized by lung-generated oxidants, and thus, several studies have focused on these as markers of oxidative stress. Moreover, many studies have demonstrated significant oxidative changes in these components after pollutant exposure in animal models and in human panel studies (Araujo et al. 2008; Liu et al. 2007; Liu et al. 2009; Lund et al. 2011; Possamai et al. 2010). Total antioxidant capacity (TAC) and thiobarbituric acid-reactive substances (TBARS) are convenient to measure and serve as indices of the collective acellular antioxidant and oxidized pool, which includes lipoproteins in the plasma or serum. The TAC assay can be performed using cuvette-based spectrophotometer, plate reader, or clinical chemistry autoanalyzer; however, the general nature of this assay has been criticized for its lack of specificity. Studies identifying alterations in plasma/serum TAC measured with this approach are met with skepticism, and often more specific assays are required to verify what specific antioxidant (e.g., ascorbate/Vitamin C; tocopherol/Vitamin E; uric acid) is altered by the exposure. In fact, a decrease in ascorbic acid (Vit. C) is thought to reflect oxidative stress yet no change in TBARS is found in active or passive smokers (Ayaori et al. 2000). Thus, general measures of oxidant stress, such as stable lipid peroxidation (LPO) products, malondialdehyde (MDA), and TBARS (MDA equivalents), are also viewed as nonspecific measures of oxidative stress, although these could be reflective of a change in the redox status. These markers, however, are unlikely to represent the reactive or causative agents in injury by virtue of their relative stability and accrual. Yet, studies relate plasma TBARS levels with air pollution or PM2.5 exposures indicating overall oxidative stress (Liu et al. 2007; Liu et al. 2009; Possamai et al. 2010). Recent studies using more selective and specific measures of antioxidant/oxidant changes in the plasma as effects of PM exposures, such as HDL antioxidant capacity (Araujo et al. 2008) or oxLDL (Lund et al. 2011), may be revealing more direct and perhaps causal changes that actually contribute to cardiovascular disease.
Circulating Blood Cells
Leukocytes: Circulating cells are also expected to encounter elevated levels of oxidants or at minimum an oxidative environment as these cells pass through the lung roughly once a minute (CO = HR * SV). Transit time and oxidative gradient provide a motive force for oxidation to directly and significantly impact cellular antioxidant capacity. One measure of the overall cellular oxidative stress is depletion of intracellular reduced glutathione (GSH), which can be conveniently measured by several methods, including the assay in which a change in fluorescence intensity of monochlorobimane (MCB) is measured. When MCB is bound to GSH, it emits fluorescence at 580 nm (excitation 515 nm). This can be measured using a fluorescent plate reader, fluorometer, or preferably a flow cytometer wherein a selective cell population or the cell status (e.g., CD45+, apoptotic) can be identified and the median fluorescence measured. For example, a 10 min inhalation exposure of mice to 50 ppm acrolein followed by a 4 h recovery significantly decreased MCB median fluorescence in circulating stem (e.g., Sca-1+) cells by nearly 50 % (Fig. 69.4a). Although high-level oxidant exposure could be expected to deplete cellular GSH, especially an αβ-unsaturated aldehyde such as acrolein, exposure to concentrated ambient particulate matter of PM2.5 (CAP) can also depress blood cellular GSH. For example, nine consecutive days (6 h/day) of CAP exposure led to a significantly lower median MCB fluorescence (decreased 30 %) in circulating endothelial progenitor cells (EPCs; Flk-1+/Sca-1+) (Fig. 69.4b and c). Although the mechanism(s) that leads to this drop in [GSH] in EPCs is not clear, it is evident that either CAP or acrolein exposure alone in healthy mice suppresses EPC mobilization from bone marrow via systemic VEGF resistance (Fig. 69.5) (Haberzettl et al. 2012; Wheat et al. 2011). The role of oxidative stress in these responses has not been delineated, and it is unclear whether CAP-induced VEGF resistance in mice is related to a similarly observed EPC suppression in healthy human adults acutely exposed to elevated ambient PM2.5 (O’Toole et al. 2010).

Glutathione depletion in blood cells of mice exposed to acrolein or CAP. (a) Acrolein inhalation (50 ppm, 30 min) depleted GSH levels (MCB mean fluorescence intensity measured by flow cytometry) in lymphocytes (left) and Flk-1+/Sca-1+ EPCs (right) at 4 h post-acrolein. Inhalation of acrolein (1 ppm, 4 days) or CAP (concentrated ambient particulate matter; 9 days) depleted GSH levels (MCB mean fluorescence intensity) in Flk-1+/Sca-1+ EPCs as shown in the representative histograms (b) and in the quantification (c) of the flow cytometric measurement. Data are mean ± SEM in % of control (n = 4−5, *p < 0.05)

Hypothetical mechanism by which fine particulate matter (PM2.5) or acrolein induce vascular VEGF resistance and impair EPC recruitment from the bone marrow
Red Blood Cells (RBC): The RBCs represent an abundant pool of circulating cells that could be monitored to gauge changes in the nature of the blood milieux. In diabetes, the hemoglobin A1c (HbA1c) level provides an integrated measure of hyperglycemia. Similarly, RBC can and are routinely used to index the level of oxidative stress induced by PM or CAP exposure by measuring their GSH or TBARS levels or their antioxidant capacity (e.g., Vit. C, catalase, GST, GPx). Numerous studies in humans and animals document changes in RBC antioxidant status as reflective of oxidative stress due to PM exposure although the causal relationship between changes in RBCs and cardiovascular disease, e.g., endothelial function or atherosclerosis, remains unclear (Araujo et al. 2008; Araujo and Nel 2009; Delfino et al. 2008; Possamai et al. 2010).
Vasculature
Endothelium
Because endothelial cells line the vessel lumen, it is likely that these cells are a prime target of ROS generated in the blood by inhaled pollutants. However, because of the limited, single squamous cell layer morphology of the endothelium and the susceptibility of histological analysis on the endothelium to artifactual problems (e.g., “edge effect,” denudation), few studies have unambiguously demonstrated endothelium-derived ROS levels following environmental PM2.5 exposures in vivo. The literature contains numerous publications demonstrating the effects of particulate matter or emissions exposures on endothelial function (Brook et al. 2002; Knuckles et al. 2008; Mills et al. 2005; Nurkiewicz et al. 2006, 2009), but very few reports provide evidence of increased endothelial cell ROS production as a causative event that induces functional deficits. This could be due in part to a limitation of specific probes and technical concerns as mentioned above or it could be due to greater ROS generation in other parts of the vascular wall or in the blood that impacts the endothelium. Yet oxidation of endothelial-specific targets such as tetrahydrobiopterin (BH4), required for NO synthesis by eNOS, is thought to be one mechanism leading to endothelial dysfunction through diminished NO production (Campen 2009). Plasma levels of the cleaved form of the LOX-1 receptor, soluble LOX-1, is elevated after exposure to DEP in mice and humans (Lund et al. 2011) indicating that the LOX-1 receptor could be an additional target. For example, oxLDL is a potent agonist of endothelial cell LOX-1 receptor activation and subsequent endothelin-1 (ET-1) transcription. This mechanism has been well described in vehicular emission exposures in mice and appears to be dependent on the particulate matter fraction being present and inducing LDL oxidation (Lund et al. 2011). Because LOX-1 is localized to the endothelium, it follows that LOX activation may be an important feature of the overall constellation of changes that comprise endothelium dysfunction. Moreover, expression and secretion of ET-1 is implicated in vascular dysfunction and atherosclerosis associated with particulate matter exposures via the LOX-1 pathway (Cherng et al. 2009; Lund et al. 2009, 2011).
Numerous studies implicate a role of ROS as causative in pollutant exposure-induced endothelium dysfunction. In animal models, absence/ablation of an important antioxidant enzyme (e.g., gene deletion/deficiency) is a typical approach used to demonstrate the contribution of the antioxidant pathway to endothelium protection and, by proxy, a causative role of oxidative stress. For example, exposure to environmental tobacco smoke (ETS) is a robust inducer of endothelium dysfunction in humans (Puranik and Celermajer 2003) and in several animal models, yet the underlying mechanism(s) remains unclear. Our previous work has shown that whole-body deletion of the antioxidant enzyme, glutathione S-transferase P (GSTP), leads to aortic endothelium dysfunction after a 3-day ETS exposure (Conklin et al. 2009). Interestingly, this effect was recapitulated by inhalation exposure of GSTP-null mice to acrolein (1 ppm; 5 h/d *3 days) or by exposure of isolated aorta to acrolein (10 μM), an effect that was blocked by co-incubation with N-acetylcysteine (NAC; 10 μM), implicating endothelial cell GSH depletion in the mechanism of acrolein-induced dysfunction (Conklin et al. 2009). Similarly, treatment with NAC (200 mg/kg, i.p.), each day prior to ETS exposure for 3 days resulted in a similar level of protection against endothelium dysfunction. These data lend further support to the idea that GSH preservation protects against oxidant exposure in vivo (Fig. 69.6).

Endothelial function in mice pretreated with vehicle or N-acetylcysteine (NAC) before exposure to air (control) or environmental tobacco smoke (ETS). (a) PE-induced contraction; (b) ACh mediated relaxation
Smooth Muscle/Vascular Media
Although endothelium dysfunction (as described above) is considered to be mechanistically linked to the hypertensive effects of PM2.5 exposure (Brook and Rajagopalan 2009), the endothelium may not be the only PM2.5 target in the blood vessel. The smooth muscle cell layer, aka tunica media, can also be affected independent of the endothelium, and thus, changes in blood pressure with PM2.5 exposure could be due to activated vascular smooth muscle as well as endothelium dysfunction (decreased NO bioavailability). As mentioned above, PM exposure could lead to activation of the central nervous system (CNS) and alterations in vascular smooth muscle cell tone via innervation of the blood vessel wall. Several studies have demonstrated in animals and humans an increase in blood pressure following PM exposure (Serinelli et al. 2010; Bartoli et al. 2009). In animals, the increase in blood pressure in dogs is prevented by α-adrenergic antagonist treatment (Bartoli et al. 2009). As described above, Mills and colleagues found altered endothelium-dependent responses to acetylcholine in humans exposed to PM, but this change was not accompanied by any change in vascular dilatation in response to the calcium channel blocker, verapamil, which acts primarily as a smooth muscle relaxant (Mills et al. 2008). It is unclear, however, whether oxidative stress in vascular smooth muscle cells (VSMC) is generated during PM exposure and/or is necessary for subsequent changes in blood pressure, but this is of high interest and deserves additional investigation. This effect could be especially important in studies that examine the vascular effects associated with nanoparticle exposures wherein <100 nm particles may gain access to the bloodstream and the blood vessel wall. However, the results of studies investigating the translocation of nanosized particles after instillation or inhalation are controversial. Although several studies show the entry of small fractions of nanosized TiO2, DEP, and carbonous particles in animals and humans (Geiser et al. 2005; Muhlfeld et al. 2007; Nemmar et al. 2002, 2004), other studies using iridium or carbon have been unsuccessful (Kreyling et al. 2002; Wiebert et al. 2006; Mills et al. 2006). This has important implications because nanoparticles are an essential part of an emerging field of nanomedicine and imaging (Janib et al. 2010). For example, Nurkiewicz and colleagues observe microvascular dysfunction in spinotrapezius arteries of rats acutely exposed to nanoparticles (Knuckles et al. 2012; Nurkiewicz et al. 2006, 2011). These investigations are important because these studies focused on the microvasculature, i.e., arteries/arterioles, that regulates vascular resistance and, thus, regulate blood pressure. Recent studies have shown that nanoparticle-induced microvascular endothelial dysfunction is accompanied by changes in vascular contractility that are also dependent on ROS, MPO, COX, and sympathetic nerve stimulation in an increasingly complex manner (Knuckles et al. 2012). Enhanced arteriolar tone (and increased blood pressure) would also be an expected outcome from observed increases in ET-1 blood levels resulting from oxLDL/LOX-1 changes with PM exposure as described above (Lund et al. 2011).
Chronic CAP exposure has been found to be associated with decreased aortic contractility, an effect that is independent of changes in ACh-induced endothelium-dependent relaxation and is reversed by guanylyl cyclase inhibitor (ODQ) (Ying et al. 2009). Supportive data show an increase in the levels of medial nitration, ROS, iNOS, and NADPH oxidase subunit expression, suggesting long-term upregulation of inflammatory signaling and non-phagocytic iNOS and NADPH oxidase in the vessel wall. These changes could likely alter smooth muscle function and likely promote smooth muscle phenotype change, migration, and proliferation (Ginnan et al. 2008), which in turn may enhance neointimal formation and atherosclerosis. In agreement with this view, several studies have shown that chronic CAP (PM2.5, UFP) exposure enhances atherosclerotic lesion formation in atherosclerosis-prone mice models (e.g., apoE-null mice) (Ying et al. 2009; Campen et al. 2010; Sun et al. 2005; Araujo and Nel 2009).
Adventitia/Perivascular Adipose Tissue (PVAT)
Several studies have implicated the outside of the vascular wall as an important entry point for inflammatory cells that can influence vascular structure and function. It has been recently suggested that PM exposure leads to the mobilization and the recruitment of proinflammatory monocytes identified as Ly6Chigh+ cells to PVAT measured by flow cytometry (Kampfrath et al. 2011). This suggestion is based on the observation that 6 months of CAP exposure increased the levels of Ly6Chigh+ cells in the lungs (perhaps, expected) of mice and to a greater extent accumulation in the PVAT of the aorta. This accumulation of Ly6Chigh+ cells is associated with increased NADPH oxidase and endothelial dysfunction, an effect ameliorated in NADPH oxidase-deficient mice (p47phox−/−), indicating dependence on NADPH oxidase and its specific localization to PVAT. These findings suggest a complicated mechanistic scenario in which oxidative stress in the lungs initiates peripheral signals that ultimately increase vascular oxidative stress to a level that becomes deleterious to the endothelium resulting in endothelium dysfunction (Conklin 2011) (Fig. 69.3).
Air Pollution and Metabolic Disorders: Is Oxidative Stress a Common Mechanism?
Epidemiological studies provide ample evidence that exposure to ambient air pollution is associated with the incidence, prevalence, and severity of diabetes. For instance, diabetics are more vulnerable to cardiovascular and allergic diseases after exposure to elevated ambient PM2.5 levels (Pereira Filho et al. 2008; Schneider et al. 2010; Hampel et al. 2012; Brook et al. 2010). Moreover, the vascular effects associated with coarse, fine, and ultrafine particles were more pronounced in subjects with diabetes (Chen and Schwartz 2008; Stewart et al. 2010). Epidemiological studies in diabetic patients (O’Neill et al. 2007) and studies in streptozotocin-diabetic rats (Lei et al. 2005) suggest that an inflammatory mechanism is responsible for the increased susceptibility. Moreover, recent studies also suggest that PM2.5 exposure enhances the prevalence of type 2 diabetes (T2D) (Kramer et al. 2010; Pearson et al. 2010; Coogan et al. 2012). In children, PM2.5 levels are significantly associated with markers of inflammation, oxidative stress, and insulin resistance (Kelishadi et al. 2009). In mice, chronic exposure to PM2.5 increases adiposity as well as inflammation and insulin resistance (Sun et al. 2009), and early life exposure to PM2.5 for 10 weeks led to a significant elevation of insulin resistance, adiposity, and vascular dysfunction in mice (Xu et al. 2010). These effects were mitigated by the genetic ablation of NADPH oxidase p47phox (Xu et al. 2010) indicating dependency on oxidative stress. The role of specific sites of ROS generation in causing the overall effects of PM2.5 is unclear. In summary, investigations in human and animals suggest that the induction of oxidative stress might also play a role in the development of PM2.5-induced insulin resistance and the progression to T2D.
Summary and Conclusions
Air pollution affects multiple organ systems and has an effect on an array of different cell types thereby leading to a variety of negative health consequences. Although the specific mechanism(s) has not been identified in all cases, several studies indicate that the induction of oxidative stress plays a major role in the development of PM-induced lung, cardiovascular, and metabolic disease. In the lungs, the overproduction of ROS/RNS seems to be due to a direct interaction between PM and surface lining fluids such as mucus and with cells such as alveolar macrophages. Moreover, cardiovascular effects are most likely also driven by oxidative stress regardless whether the underlying mechanism is the induction of oxidative stress and inflammation in the lungs due to central nervous system-mediated oxidative stress or due to the translocation of ultrafine/nanosized particles (PM0.1) into the bloodstream that directly affect vascular health via interactions with the endothelium and cause cardiovascular injury. Additional studies are required to distinguish between these (and other) possibilities and to clearly define the role of reactive oxygen species in mediating the toxicity of ambient air particles.
References
Adetona O, Dunn K, Hall DB, Achtemeier G, Stock A, Naeher LP (2011) Personal PM(2.5) exposure among wildland firefighters working at prescribed forest burns in southeastern United States. J Occup Environ Hyg 8:503–511
Albrecht C, Knaapen AM, Becker A, Hohr D, Haberzettl P, van Schooten FJ, Borm PJ, Schins RP (2005) The crucial role of particle surface reactivity in respirable quartz-induced reactive oxygen/nitrogen species formation and APE/Ref-1 induction in rat lung. Respir Res 6:129
Albrecht C, Hohr D, Haberzettl P, Becker A, Borm PJ, Schins RP (2007) Surface-dependent quartz uptake by macrophages: potential role in pulmonary inflammation and lung clearance. Inhal Toxicol 19(Suppl 1):39–48
Al-Shmgani HS, Moate RM, Sneyd JR, Macnaughton PD, Moody AJ (2012) Hyperoxia-induced ciliary loss and oxidative damage in an in vitro bovine model: the protective role of antioxidant vitamins E and C. Biochem Biophys Res Commun 429:191–196
Anderson JO, Thundiyil JG, Stolbach A (2012) Clearing the air: a review of the effects of particulate matter air pollution on human health. J Med Toxicol 8:166–175
Araujo JA, Nel AE (2009) Particulate matter and atherosclerosis: role of particle size, composition and oxidative stress. Part Fibre Toxicol 6:24
Araujo JA, Barajas B, Kleinman M, Wang X, Bennett BJ, Gong KW, Navab M, Harkema J, Sioutas C, Lusis AJ, Nel AE (2008) Ambient particulate pollutants in the ultrafine range promote early atherosclerosis and systemic oxidative stress. Circ Res 102:589–596
Avissar N, Finkelstein JN, Horowitz S, Willey JC, Coy E, Frampton MW, Watkins RH, Khullar P, Xu YL, Cohen HJ (1996) Extracellular glutathione peroxidase in human lung epithelial lining fluid and in lung cells. Am J Physiol 270:L173–L182
Ayaori M, Hisada T, Suzukawa M, Yoshida H, Nishiwaki M, Ito T, Nakajima K, Higashi K, Yonemura A, Ohsuzu F, Ishikawa T, Nakamura H (2000) Plasma levels and redox status of ascorbic acid and levels of lipid peroxidation products in active and passive smokers. Environ Health Perspect 108:105–108
Babior BM (1999) NADPH oxidase: an update. Blood 93:1464–1476
Bae S, Pan XC, Kim SY, Park K, Kim YH, Kim H, Hong YC (2010) Exposures to particulate matter and polycyclic aromatic hydrocarbons and oxidative stress in schoolchildren. Environ Health Perspect 118:579–583
Bagate K, Meiring JJ, Gerlofs-Nijland ME, Cassee FR, Borm PJ (2006) Signal transduction pathways involved in particulate matter induced relaxation in rat aorta–spontaneous hypertensive versus Wistar Kyoto rats. Toxicol In Vitro 20:52–62
Banerjee A, Trueblood MB, Zhang X, Manda KR, Lobo P, Whitefield PD, Hagen DE, Ercal N (2009) N-acetylcysteineamide (NACA) prevents inflammation and oxidative stress in animals exposed to diesel engine exhaust. Toxicol Lett 187:187–193
Bartoli CR, Wellenius GA, Diaz EA, Lawrence J, Coull BA, Akiyama I, Lee LM, Okabe K, Verrier RL, Godleski JJ (2009) Mechanisms of inhaled fine particulate air pollution-induced arterial blood pressure changes. Environ Health Perspect 117:361–366
Bates DV (1995) The effects of air pollution on children. Environ Health Perspect 103(Suppl 6): 49–53
Beamer CA, Holian A (2005) Scavenger receptor class A type I/II (CD204) null mice fail to develop fibrosis following silica exposure. Am J Physiol Lung Cell Mol Physiol 289:L186–L195
Becker S, Dailey LA, Soukup JM, Grambow SC, Devlin RB, Huang YC (2005) Seasonal variations in air pollution particle-induced inflammatory mediator release and oxidative stress. Environ Health Perspect 113:1032–1038
Bell ML (2012) Assessment of the health impacts of particulate matter characteristics. Res Rep Health Eff Inst 161:5–38
Bell ML, Davis DL (2001) Reassessment of the lethal London fog of 1952: novel indicators of acute and chronic consequences of acute exposure to air pollution. Environ Health Perspect 109(Suppl 3):389–394
Bhatnagar A (2004) Cardiovascular pathophysiology of environmental pollutants. Am J Physiol Heart Circ Physiol 286:H479–H485
Bhatnagar A (2006) Environmental cardiology: studying mechanistic links between pollution and heart disease. Circ Res 99:692–705
Bhopal RS, Phillimore P, Moffatt S, Foy C (1994) Is living near a coking works harmful to health? A study of industrial air pollution. J Epidemiol Community Health 48:237–247
Binkova B, Cerna M, Pastorkova A, Jelinek R, Benes I, Novak J, Sram RJ (2003) Biological activities of organic compounds adsorbed onto ambient air particles: comparison between the cities of Teplice and Prague during the summer and winter seasons 2000–2001. Mutat Res 525:43–59
Boland S, Bonvallot V, Fournier T, Baeza-Squiban A, Aubier M, Marano F (2000) Mechanisms of GM-CSF increase by diesel exhaust particles in human airway epithelial cells. Am J Physiol Lung Cell Mol Physiol 278:L25–L32
Bonner JC, Rice AB, Moomaw CR, Morgan DL (2000) Airway fibrosis in rats induced by vanadium pentoxide. Am J Physiol Lung Cell Mol Physiol 278:L209–L216
Borm PJ, Schins RP, Albrecht C (2004) Inhaled particles and lung cancer, part B: paradigms and risk assessment. Int J Cancer 110:3–14
Braga AL, Zanobetti A, Schwartz J (2000) Do respiratory epidemics confound the association between air pollution and daily deaths? Eur Respir J 16:723–728
Brauer M, Amann M, Burnett RT, Cohen A, Dentener F, Ezzati M, Henderson SB, Krzyzanowski M, Martin RV, van Dingenen R, van Donkelaar A, Thurston GD (2012) Exposure assessment for estimation of the global burden of disease attributable to outdoor air pollution. Environ Sci Technol 46:652–660
Bridges JP, Davis HW, Damodarasamy M, Kuroki Y, Howles G, Hui DY, McCormack FX (2000) Pulmonary surfactant proteins A and D are potent endogenous inhibitors of lipid peroxidation and oxidative cellular injury. J Biol Chem 275:38848–38855
Brook RD, Brook JR (2011) A road forward to improve public health. Circulation 123:1705–1708
Brook RD, Rajagopalan S (2009) Particulate matter, air pollution, and blood pressure. J Am Soc Hypertens 3:332–350
Brook RD, Brook JR, Urch B, Vincent R, Rajagopalan S, Silverman F (2002) Inhalation of fine particulate air pollution and ozone causes acute arterial vasoconstriction in healthy adults. Circulation 105:1534–1536
Brook RD, Brook JR, Rajagopalan S (2003) Air pollution: the “Heart” of the problem. Curr Hypertens Rep 5:32–39
Brook RD, Franklin B, Cascio W, Hong Y, Howard G, Lipsett M, Luepker R, Mittleman M, Samet J, Smith SC JR, Tager I (2004) Air pollution and cardiovascular disease: a statement for healthcare professionals from the Expert Panel on Population and Prevention Science of the American Heart Association. Circulation 109:2655–2671
Brook RD, Urch B, Dvonch JT, Bard RL, Speck M, Keeler G, Morishita M, Marsik FJ, Kamal AS, Kaciroti N, Harkema J, Corey P, Silverman F, Gold DR, Wellenius G, Mittleman MA, Rajagopalan S, Brook JR (2009) Insights into the mechanisms and mediators of the effects of air pollution exposure on blood pressure and vascular function in healthy humans. Hypertension 54:659–667
Brook RD, Rajagopalan S, Pope CA 3rd, Brook JR, Bhatnagar A, Diez-Roux AV, Holguin F, Hong Y, Luepker RV, Mittleman MA, Peters A, Siscovick D, Smith SC Jr, Whitsel L, Kaufman JD (2010) Particulate matter air pollution and cardiovascular disease: an update to the scientific statement from the American Heart Association. Circulation 121:2331–2378
Brown DM, Stone V, Findlay P, Macnee W, Donaldson K (2000) Increased inflammation and intracellular calcium caused by ultrafine carbon black is independent of transition metals or other soluble components. Occup Environ Med 57:685–691
Brown DM, Wilson MR, Macnee W, Stone V, Donaldson K (2001) Size-dependent proinflammatory effects of ultrafine polystyrene particles: a role for surface area and oxidative stress in the enhanced activity of ultrafines. Toxicol Appl Pharmacol 175:191–199
Burnett RT, Brook J, Dann T, Delocla C, Philips O, Cakmak S, Vincent R, Goldberg MS, Krewski D (2000) Association between particulate- and gas-phase components of urban air pollution and daily mortality in eight Canadian cities. Inhal Toxicol 12(Suppl 4):15–39
Campen MJ (2009) Nitric oxide synthase: “enzyme zero” in air pollution-induced vascular toxicity. Toxicol Sci 110:1–3
Campen MJ, Nolan JP, Schladweiler MC, Kodavanti UP, Evansky PA, Costa DL, Watkinson WP (2001) Cardiovascular and thermoregulatory effects of inhaled PM-associated transition metals: a potential interaction between nickel and vanadium sulfate. Toxicol Sci 64:243–252
Campen MJ, Nolan JP, Schladweiler MC, Kodavanti UP, Costa DL, Watkinson WP (2002) Cardiac and thermoregulatory effects of instilled particulate matter-associated transition metals in healthy and cardiopulmonary-compromised rats. J Toxicol Environ Health A 65:1615–1631
Campen MJ, Lund AK, Knuckles TL, Conklin DJ, Bishop B, Young D, Seilkop S, Seagrave J, Reed MD, McDonald JD (2010) Inhaled diesel emissions alter atherosclerotic plaque composition in ApoE(−/−) mice. Toxicol Appl Pharmacol 242:310–317
Cao Q, Zhang S, Dong C, Song W (2007) Pulmonary responses to fine particles: differences between the spontaneously hypertensive rats and wistar kyoto rats. Toxicol Lett 171:126–137
Castranova V, Vallyathan V (2000) Silicosis and coal workers’ pneumoconiosis. Environ Health Perspect 108(Suppl 4):675–684
Chen JC, Schwartz J (2008) Metabolic syndrome and inflammatory responses to long-term particulate air pollutants. Environ Health Perspect 116:612–617
Chen LW, Chow JC, Doddridge BG, Dickerson RR, Ryan WF, Mueller PK (2003) Analysis of a summertime PM2.5 and haze episode in the mid-Atlantic region. J Air Waste Manag Assoc 53:946–956
Cherng TW, Campen MJ, Knuckles TL, Gonzalez Bosc L, Kanagy NL (2009) Impairment of coronary endothelial cell ET(B) receptor function after short-term inhalation exposure to whole diesel emissions. Am J Physiol Regul Integr Comp Physiol 297:R640–R647
Colburn KA, Johnson PR (2003) Public health. Air pollution concerns not changed by S-PLUS flaw. Science 299:665–666
Conklin DJ (2011) Beware the air! Why particulate matter matters. Circ Res 108:644–647
Conklin DJ, Haberzettl P, Prough RA, Bhatnagar A (2009) Glutathione-S-transferase P protects against endothelial dysfunction induced by exposure to tobacco smoke. Am J Physiol Heart Circ Physiol 296:H1586–H1597
Coogan PF, White LF, Jerrett M, Brook RD, Su JG, Seto E, Burnett R, Palmer JR, Rosenberg L (2012) Air pollution and incidence of hypertension and diabetes mellitus in black women living in Los Angeles. Circulation 125:767–772
Courtois A, Andujar P, Ladeiro Y, Baudrimont I, Delannoy E, Leblais V, Begueret H, Galland MA, Brochard P, Marano F, Marthan R, Muller B (2008) Impairment of NO-dependent relaxation in intralobar pulmonary arteries: comparison of urban particulate matter and manufactured nanoparticles. Environ Health Perspect 116:1294–1299
Dai YT, Yu CP (1998) Alveolar deposition of fibers in rodents and humans. J Aerosol Med 11:247–258
Danielsen PH, Loft S, Jacobsen NR, Jensen KA, Autrup H, Ravanat JL, Wallin H, Moller P (2010) Oxidative stress, inflammation, and DNA damage in rats after intratracheal instillation or oral exposure to ambient air and wood smoke particulate matter. Toxicol Sci 118:574–585
de Groot P, Munden RF (2012) Lung cancer epidemiology, risk factors, and prevention. Radiol Clin North Am 50:863–876
Delfino RJ, Staimer N, Tjoa T, Polidori A, Arhami M, Gillen DL, Kleinman MT, Vaziri ND, Longhurst J, Zaldivar F, Sioutas C (2008) Circulating biomarkers of inflammation, antioxidant activity, and platelet activation are associated with primary combustion aerosols in subjects with coronary artery disease. Environ Health Perspect 116:898–906
Dey S, Di Girolamo L, Van Donkelaar A, Trpathi SN, Gupta T, Mohan M (2012) Variability of outdoor fine particulate (PM2.5) concentration in the Indian Subcontinent: A remote sensing approach. Remote Sens Environ 127:153–161
Diaz-Sanchez D (1997) The role of diesel exhaust particles and their associated polyaromatic hydrocarbons in the induction of allergic airway disease. Allergy 52:52–56, discussion 57–58
Dockery DW, Pope CA III, Xu X, Spengler JD, Ware JH, Fay ME, Ferris BG Jr, Speizer FE (1993) An association between air pollution and mortality in six U.S. cities. N Engl J Med 329:1753–1759
Dominici F, Peng RD, Zeger SL, White RH, Samet JM (2007) Particulate air pollution and mortality in the United States: did the risks change from 1987 to 2000? Am J Epidemiol 166:880–888
Droge W (2002) Free radicals in the physiological control of cell function. Physiol Rev 82:47–95
Dye JA, Lehmann JR, McGee JK, Winsett DW, Ledbetter AD, Everitt JI, Ghio AJ, Costa DL (2001) Acute pulmonary toxicity of particulate matter filter extracts in rats: coherence with epidemiologic studies in Utah Valley residents. Environ Health Perspect 109(Suppl 3):395–403
Feldman C, Anderson R, Kanthakumar K, Vargas A, Cole PJ, Wilson R (1994) Oxidant-mediated ciliary dysfunction in human respiratory epithelium. Free Radic Biol Med 17:1–10
Forsberg B, Stjernberg N, Falk M, Lundback B, Wall S (1993) Air pollution levels, meteorological conditions and asthma symptoms. Eur Respir J 6:1109–1115
Frampton MW, Ghio AJ, Samet JM, Carson JL, Carter JD, Devlin RB (1999) Effects of aqueous extracts of PM(10) filters from the Utah valley on human airway epithelial cells. Am J Physiol 277:L960–L967
Franchini M, Mannucci PM (2009) Particulate air pollution and cardiovascular risk: short-term and long-term effects. Semin Thromb Hemost 35:665–670
Franchini M, Mannucci PM (2011) Thrombogenicity and cardiovascular effects of ambient air pollution. Blood 118:2405–2412
Garcia-Suastegui WA, Huerta-Chagoya A, Carrasco-Colin KL, Pratt MM, John K, Petrosyan P, Rubio J, Poirier MC, Gonsebatt ME (2011) Seasonal variations in the levels of PAH-DNA adducts in young adults living in Mexico City. Mutagenesis 26:385–391
Geiser M, Rothen-Rutishauser B, Kapp N, Schurch S, Kreyling W, Schulz H, Semmler M, Im Hof V, Heyder J, Gehr P (2005) Ultrafine particles cross cellular membranes by nonphagocytic mechanisms in lungs and in cultured cells. Environ Health Perspect 113:1555–1560
Ghio AJ, Devlin RB (2001) Inflammatory lung injury after bronchial instillation of air pollution particles. Am J Respir Crit Care Med 164:704–708
Ghio AJ, Suliman HB, Carter JD, Abushamaa AM, Folz RJ (2002) Overexpression of extracellular superoxide dismutase decreases lung injury after exposure to oil fly ash. Am J Physiol Lung Cell Mol Physiol 283:L211–L218
Ghio AJ, Carraway MS, Madden MC (2012) Composition of air pollution particles and oxidative stress in cells, tissues, and living systems. J Toxicol Environ Health B Crit Rev 15:1–21
Ginnan R, Guikema BJ, Halligan KE, Singer HA, Jourd’Heuil D (2008) Regulation of smooth muscle by inducible nitric oxide synthase and NADPH oxidase in vascular proliferative diseases. Free Radic Biol Med 44:1232–1245
Goldsmith CA, Frevert C, Imrich A, Sioutas C, Kobzik L (1997) Alveolar macrophage interaction with air pollution particulates. Environ Health Perspect 105(Suppl 5):1191–1195
Grievink L, Smit HA, Brunekreef B (2000) Anti-oxidants and air pollution in relation to indicators of asthma and COPD: a review of the current evidence. Clin Exp Allergy 30:1344–1354
Griffith DE, Levin JL (1989) Respiratory effects of outdoor air pollution. Postgrad Med 86(111):116, 118
Haberzettl P, Duffin R, Kramer U, Hohr D, Schins RP, Borm PJ, Albrecht C (2007) Actin plays a crucial role in the phagocytosis and biological response to respirable quartz particles in macrophages. Arch Toxicol 81:459–470
Haberzettl P, Schins RP, Hohr D, Wilhelmi V, Borm PJ, Albrecht C (2008) Impact of the FcgammaII-receptor on quartz uptake and inflammatory response by alveolar macrophages. Am J Physiol Lung Cell Mol Physiol 294:L1137–L1148
Haberzettl P, Lee J, Duggineni D, McCracken J, Bolanowski D, O’Toole TE, Bhatnagar A, Conklin DJ (2012) Exposure to ambient air fine particulate matter prevents VEGF-induced mobilization of endothelial progenitor cells from the bone marrow. Environ Health Perspect 120:848–856
Hampel R, Breitner S, Schneider A, Zareba W, Kraus U, Cyrys J, Geruschkat U, Belcredi P, Muller M, Wichmann HE, Peters A (2012) Acute air pollution effects on heart rate variability are modified by SNPs involved in cardiac rhythm in individuals with diabetes or impaired glucose tolerance. Environ Res 112:177–185
Happo MS, Uski O, Jalava PI, Kelz J, Brunner T, Hakulinen P, Maki-Paakkanen J, Kosma VM, Jokiniemi J, Obernberger I, Hirvonen MR (2013) Pulmonary inflammation and tissue damage in the mouse lung after exposure to PM samples from biomass heating appliances of old and modern technologies. Sci Total Environ 443:256–266
Harris RL Jr, Timbrell V (1975) The influence of fibre shape in lung deposition-mathematical estimates. Inhaled Part 4(Pt 1):75–89
Harrison RM, Smith DJ, Kibble AJ (2004) What is responsible for the carcinogenicity of PM2.5? Occup Environ Med 61:799–805
Hassing C, Twickler M, Brunekreef B, Cassee F, Doevendans P, Kastelein J, Cramer MJ (2009) Particulate air pollution, coronary heart disease and individual risk assessment: a general overview. Eur J Cardiovasc Prev Rehabil 16:10–15
Hernandez-Garduno E, Brauer M, Perez-Neria J, Vedal S (2004) Wood smoke exposure and lung adenocarcinoma in non-smoking Mexican women. Int J Tuberc Lung Dis 8:377–383
Heyder J (1982) Particle transport onto human airway surfaces. Eur J Respir Dis Suppl 119:29–50
Hiura TS, Kaszubowski MP, Li N, Nel AE (1999) Chemicals in diesel exhaust particles generate reactive oxygen radicals and induce apoptosis in macrophages. J Immunol 163:5582–5591
Hofmann W, Morawska L, Winkler-Heil R, Moustafa M (2009) Deposition of combustion aerosols in the human respiratory tract: comparison of theoretical predictions with experimental data considering nonspherical shape. Inhal Toxicol 21:1154–1164
Imrich A, Ning YY, Kobzik L (1999) Intracellular oxidant production and cytokine responses in lung macrophages: evaluation of fluorescent probes. J Leukoc Biol 65:499–507
Janib SM, Moses AS, Mackay JA (2010) Imaging and drug delivery using theranostic nanoparticles. Adv Drug Deliv Rev 62:1052–1063
Junk J, Helbig A, Luers J (2003) Urban climate and air quality in Trier Germany. Int J Biometeorol 47:230–238
Kadiiska MB, Mason RP, Dreher KL, Costa DL, Ghio AJ (1997) In vivo evidence of free radical formation in the rat lung after exposure to an emission source air pollution particle. Chem Res Toxicol 10:1104–1108
Kampfrath T, Maiseyeu A, Ying Z, Shah Z, Deiuliis JA, Xu X, Kherada N, Brook RD, Reddy KM, Padture NP, Parthasarathy S, Chen LC, Moffatt-Bruce S, Sun Q, Morawietz H, Rajagopalan S (2011) Chronic fine particulate matter exposure induces systemic vascular dysfunction via NADPH oxidase and TLR4 pathways. Circ Res 108:716–726
Kelishadi R, Mirghaffari N, Poursafa P, Gidding SS (2009) Lifestyle and environmental factors associated with inflammation, oxidative stress and insulin resistance in children. Atherosclerosis 203:311–319
Kendall M, Brown L, Trought K (2004) Molecular adsorption at particle surfaces: a PM toxicity mediation mechanism. Inhal Toxicol 16(Suppl 1):99–105
Knaapen AM, Shi T, Borm PJ, Schins RP (2002) Soluble metals as well as the insoluble particle fraction are involved in cellular DNA damage induced by particulate matter. Mol Cell Biochem 234–235:317–326
Knuckles TL, Lund AK, Lucas SN, Campen MJ (2008) Diesel exhaust exposure enhances venoconstriction via uncoupling of eNOS. Toxicol Appl Pharmacol 230:346–351
Knuckles TL, Yi J, Frazer DG, Leonard HD, Chen BT, Castranova V, Nurkiewicz TR (2012) Nanoparticle inhalation alters systemic arteriolar vasoreactivity through sympathetic and cyclooxygenase-mediated pathways. Nanotoxicology 6:724–735
Kobzik L (1995) Lung macrophage uptake of unopsonized environmental particulates. Role of scavenger-type receptors. J Immunol 155:367–376
Kodavanti UP, Moyer CF, Ledbetter AD, Schladweiler MC, Costa DL, Hauser R, Christiani DC, Nyska A (2003) Inhaled environmental combustion particles cause myocardial injury in the Wistar Kyoto rat. Toxicol Sci 71:237–245
Kramer U, Herder C, Sugiri D, Strassburger K, Schikowski T, Ranft U, Rathmann W (2010) Traffic-related air pollution and incident type 2 diabetes: results from the SALIA cohort study. Environ Health Perspect 118:1273–1279
Kreyling WG, Semmler M, Erbe F, Mayer P, Takenaka S, Schulz H, Oberdorster G, Ziesenis A (2002) Translocation of ultrafine insoluble iridium particles from lung epithelium to extrapulmonary organs is size dependent but very low. J Toxicol Environ Health A 65:1513–1530
Kuempel ED, Attfield MD, Vallyathan V, Lapp NL, Hale JM, Smith RJ, Castranova V (2003) Pulmonary inflammation and crystalline silica in respirable coal mine dust: dose–response. J Biosci 28:61–69
Kumagai Y, Koide S, Taguchi K, Endo A, Nakai Y, Yoshikawa T, Shimojo N (2002) Oxidation of proximal protein sulfhydryls by phenanthraquinone, a component of diesel exhaust particles. Chem Res Toxicol 15:483–489
Laden F, Neas LM, Dockery DW, Schwartz J (2000) Association of fine particulate matter from different sources with daily mortality in six U.S. cities. Environ Health Perspect 108:941–947
Larson BA, Rosen S (2002) Understanding household demand for indoor air pollution control in developing countries. Soc Sci Med 55:571–584
Laskin DL, Mainelis G, Turpin BJ, Patel KJ, Sunil VR (2010) Pulmonary effects of inhaled diesel exhaust in young and old mice: a pilot project. Res Rep Health Eff Inst 151:3–31
Lei YC, Hwang JS, Chan CC, Lee CT, Cheng TJ (2005) Enhanced oxidative stress and endothelial dysfunction in streptozotocin-diabetic rats exposed to fine particles. Environ Res 99:335–343
Lewis AB, Taylor MD, Roberts JR, Leonard SS, Shi X, Antonini JM (2003) Role of metal-induced reactive oxygen species generation in lung responses caused by residual oil fly ash. J Biosci 28:13–18
Li XY, Gilmour PS, Donaldson K, Macnee W (1996) Free radical activity and pro-inflammatory effects of particulate air pollution (PM10) in vivo and in vitro. Thorax 51:1216–1222
Li Z, Carter JD, Dailey LA, Huang YC (2005) Pollutant particles produce vasoconstriction and enhance MAPK signaling via angiotensin type I receptor. Environ Health Perspect 113:1009–1014
Lindgren A, Stroh E, Montnemery P, Nihlen U, Jakobsson K, Axmon A (2009) Traffic-related air pollution associated with prevalence of asthma and COPD/chronic bronchitis. A cross-sectional study in Southern Sweden. Int J Health Geogr 8:2
Liu L, Ruddy TD, Dalipaj M, Szyszkowicz M, You H, Poon R, Wheeler A, Dales R (2007) Influence of personal exposure to particulate air pollution on cardiovascular physiology and biomarkers of inflammation and oxidative stress in subjects with diabetes. J Occup Environ Med 49:258–265
Liu L, Poon R, Chen L, Frescura AM, Montuschi P, Ciabattoni G, Wheeler A, Dales R (2009) Acute effects of air pollution on pulmonary function, airway inflammation, and oxidative stress in asthmatic children. Environ Health Perspect 117:668–674
Lund AK, Lucero J, Lucas S, Madden MC, McDonald JD, Seagrave JC, Knuckles TL, Campen MJ (2009) Vehicular emissions induce vascular MMP-9 expression and activity associated with endothelin-1-mediated pathways. Arterioscler Thromb Vasc Biol 29:511–517
Lund AK, Lucero J, Harman M, Madden MC, McDonald JD, Seagrave JC, Campen MJ (2011) The oxidized low-density lipoprotein receptor mediates vascular effects of inhaled vehicle emissions. Am J Respir Crit Care Med 184:82–91
McNeely TB, Coonrod JD (1994) Aggregation and opsonization of type A but not type B Hemophilus influenzae by surfactant protein A. Am J Respir Cell Mol Biol 11:114–122
Mills NL, Tornqvist H, Robinson SD, Gonzalez M, Darnley K, Macnee W, Boon NA, Donaldson K, Blomberg A, Sandstrom T, Newby DE (2005) Diesel exhaust inhalation causes vascular dysfunction and impaired endogenous fibrinolysis. Circulation 112:3930–3936
Mills NL, Amin N, Robinson SD, Anand A, Davies J, Patel D, de la Fuente JM, Cassee FR, Boon NA, Macnee W, Millar AM, Donaldson K, Newby DE (2006) Do inhaled carbon nanoparticles translocate directly into the circulation in humans? Am J Respir Crit Care Med 173:426–431
Mills NL, Robinson SD, Fokkens PH, Leseman DL, Miller MR, Anderson D, Freney EJ, Heal MR, Donovan RJ, Blomberg A, Sandstrom T, Macnee W, Boon NA, Donaldson K, Newby DE, Cassee FR (2008) Exposure to concentrated ambient particles does not affect vascular function in patients with coronary heart disease. Environ Health Perspect 116:709–715
Moghimi SM, Hunter AC, Murray JC (2005) Nanomedicine: current status and future prospects. FASEB J 19:311–330
Monn C, Fendt R, Koller T (2002) Ambient PM(10) extracts inhibit phagocytosis of defined inert model particles by alveolar macrophages. Inhal Toxicol 14:369–385
Muhlfeld C, Geiser M, Kapp N, Gehr P, Rothen-Rutishauser B (2007) Re-evaluation of pulmonary titanium dioxide nanoparticle distribution using the “relative deposition index”: evidence for clearance through microvasculature. Part Fibre Toxicol 4:7
Nadel JA (2001) Role of epidermal growth factor receptor activation in regulating mucin synthesis. Respir Res 2:85–89
Nemmar A, Hoet PH, Vanquickenborne B, Dinsdale D, Thomeer M, Hoylaerts MF, Vanbilloen H, Mortelmans L, Nemery B (2002) Passage of inhaled particles into the blood circulation in humans. Circulation 105:411–414
Nemmar A, Hoylaerts MF, Hoet PH, Nemery B (2004) Possible mechanisms of the cardiovascular effects of inhaled particles: systemic translocation and prothrombotic effects. Toxicol Lett 149:243–253
Nemmar A, Hoylaerts MF, Nemery B (2006) Effects of particulate air pollution on hemostasis. Clin Occup Environ Med 5:865–881
Nurkiewicz TR, Porter DW, Barger M, Millecchia L, Rao KM, Marvar PJ, Hubbs AF, Castranova V, Boegehold MA (2006) Systemic microvascular dysfunction and inflammation after pulmonary particulate matter exposure. Environ Health Perspect 114:412–419
Nurkiewicz TR, Porter DW, Hubbs AF, Stone S, Chen BT, Frazer DG, Boegehold MA, Castranova V (2009) Pulmonary nanoparticle exposure disrupts systemic microvascular nitric oxide signaling. Toxicol Sci 110:191–203
Nurkiewicz TR, Porter DW, Hubbs AF, Stone S, Moseley AM, Cumpston JL, Goodwill AG, Frisbee SJ, Perrotta PL, Brock RW, Frisbee JC, Boegehold MA, Frazer DG, Chen BT, Castranova V (2011) Pulmonary particulate matter and systemic microvascular dysfunction. Res Rep Health Eff Inst 164:3–48
Oberdorster G, Ferin J, Morrow PE (1992) Volumetric loading of alveolar macrophages (AM): a possible basis for diminished AM-mediated particle clearance. Exp Lung Res 18:87–104
Oberdorster G, Ferin J, Lehnert BE (1994) Correlation between particle size, in vivo particle persistence, and lung injury. Environ Health Perspect 102(Suppl 5):173–179
Oberdorster G, Oberdorster E, Oberdorster J (2005) Nanotoxicology: an emerging discipline evolving from studies of ultrafine particles. Environ Health Perspect 113:823–839
Ohtoshi T, Takizawa H, Okazaki H, Kawasaki S, Takeuchi N, Ohta K, Ito K (1998) Diesel exhaust particles stimulate human airway epithelial cells to produce cytokines relevant to airway inflammation in vitro. J Allergy Clin Immunol 101:778–785
O’Neill MS, Veves A, Sarnat JA, Zanobetti A, Gold DR, Economides PA, Horton ES, Schwartz J (2007) Air pollution and inflammation in type 2 diabetes: a mechanism for susceptibility. Occup Environ Med 64:373–379
O’Toole TE, Hellmann J, Wheat L, Haberzettl P, Lee J, Conklin DJ, Bhatnagar A, Pope CA 3RD (2010) Episodic exposure to fine particulate air pollution decreases circulating levels of endothelial progenitor cells. Circ Res 107:200–203
Oury TD, Chang LY, Marklund SL, Day BJ, Crapo JD (1994) Immunocytochemical localization of extracellular superoxide dismutase in human lung. Lab Invest 70:889–898
Park JB (2003) Phagocytosis induces superoxide formation and apoptosis in macrophages. Exp Mol Med 35:325–335
Patton JS, Fishburn CS, Weers JG (2004) The lungs as a portal of entry for systemic drug delivery. Proc Am Thorac Soc 1:338–344
Pearson JF, Bachireddy C, Shyamprasad S, Goldfine AB, Brownstein JS (2010) Association between fine particulate matter and diabetes prevalence in the U.S. Diabetes Care 33:2196–2201
Pedersen M (1990) Ciliary activity and pollution. Lung 168(Suppl):368–376
Peel JL, Tolbert PE, Klein M, Metzger KB, Flanders WD, Todd K, Mulholland JA, Ryan PB, Frumkin H (2005) Ambient air pollution and respiratory emergency department visits. Epidemiology 16:164–174
Pereira Filho MA, Pereira LA, Arbex FF, Arbex M, Conceicao GM, Santos UP, Lopes AC, Saldiva PH, Braga AL, Cendon S (2008) Effect of air pollution on diabetes and cardiovascular diseases in Sao Paulo, Brazil. Braz J Med Biol Res 41:526–532
Peters A, Dockery DW, Heinrich J, Wichmann HE (1997) Short-term effects of particulate air pollution on respiratory morbidity in asthmatic children. Eur Respir J 10:872–879
Peters S, Thomassen Y, Fechter-Rink E, Kromhout H (2009) Personal exposure to inhalable cement dust among construction workers. J Environ Monit 11:174–180
Pinkerton KE, Zhou Y, Zhong C, Smith KR, Teague SV, Kennedy IM, Menache MG (2008) Mechanisms of particulate matter toxicity in neonatal and young adult rat lungs. Res Rep Health Eff Inst 3–41, discussion 43–52
Pope CA 3RD (2004) Air pollution and health - good news and bad. N Engl J Med 351:1132–1134
Pope CA III, Thun MJ, Namboodiri MM, Dockery DW, Evans JS, Speizer FE, Heath CW Jr (1995) Particulate air pollution as a predictor of mortality in a prospective study of U.S. adults. Am J Respir Crit Care Med 151:669–674
Pope CA III, Burnett RT, Thun MJ, Calle EE, Krewski D, Ito K, Thurston GD (2002) Lung cancer, cardiopulmonary mortality, and long-term exposure to fine particulate air pollution. JAMA 287:1132–1141
Pope CA III, Burnett RT, Thurston GD, Thun MJ, Calle EE, Krewski D, Godleski JJ (2004) Cardiovascular mortality and long-term exposure to particulate air pollution: epidemiological evidence of general pathophysiological pathways of disease. Circulation 109:71–77
Pope CA III, Renlund DG, Kfoury AG, May HT, Horne BD (2008) Relation of heart failure hospitalization to exposure to fine particulate air pollution. Am J Cardiol 102:1230–1234
Possamai FP, Junior SA, Parisotto EB, Moratelli AM, Inacio DB, Garlet TR, Dal-Pizzol F, Filho DW (2010) Antioxidant intervention compensates oxidative stress in blood of subjects exposed to emissions from a coal electric-power plant in South Brazil. Environ Toxicol Pharmacol 30:175–180
Pradhan A, Waseem M, Dogra S, Khanna AK, Kaw JL (2005) Alterations in bronchoalveolar lavage constituents, oxidant/antioxidant status, and lung histology following intratracheal instillation of respirable suspended particulate matter. J Environ Pathol Toxicol Oncol 24:19–32
Puett RC, Hart JE, Schwartz J, Hu FB, Liese AD, Laden F (2011) Are particulate matter exposures associated with risk of type 2 diabetes? Environ Health Perspect 119:384–389
Puranik R, Celermajer DS (2003) Smoking and endothelial function. Prog Cardiovasc Dis 45:443–458
Rajagopalan S, Brook RD (2012) Air pollution and type 2 diabetes: mechanistic insights. Diabetes 61:3037–3045
Rehn B, Seiler F, Rehn S, Bruch J, Maier M (2003) Investigations on the inflammatory and genotoxic lung effects of two types of titanium dioxide: untreated and surface treated. Toxicol Appl Pharmacol 189:84–95
Reis MA, Carvalho A, Taborda A, Quaresma A, Dias G, Alves LC, Mota M, Chaves PC, Teixeira R, Rodrigues PO (2009) High airborne PM2.5 chlorine concentrations link to diabetes surge in Portugal. Sci Total Environ 407:5726–5734
Riles E, Brook R (2011) The air quality index: a tool for managing patients with cardiopulmonary disease. Am J Med 124:705–707
Roberts S, Martin MA (2007) Methods for bias reduction in time-series studies of particulate matter air pollution and mortality. J Toxicol Environ Health A 70:665–675
Rogers DF (2001) Mucus hypersecretion in chronic obstructive pulmonary disease. Novartis Found Symp 234:65–77, discussion 77–83
Roman AO, Prieto CM, Mancilla FP, Astudillo OP, Dussaubat AA, Miguel WC, Lara MJ (2009) Association between air pollution and cardiovascular risk. Rev Med Chil 137:1217–1224
Sagai M, Saito H, Ichinose T, Kodama M, Mori Y (1993) Biological effects of diesel exhaust particles. I. In vitro production of superoxide and in vivo toxicity in mouse. Free Radic Biol Med 14:37–47
Sakamoto N, Hayashi S, Gosselink J, Ishii H, Ishimatsu Y, Mukae H, Hogg JC, van Eeden SF (2007) Calcium dependent and independent cytokine synthesis by air pollution particle-exposed human bronchial epithelial cells. Toxicol Appl Pharmacol 225:134–141
Samet JM, Dominici F, Curriero FC, Coursac I, Zeger SL (2000) Fine particulate air pollution and mortality in 20 U.S. cities, 1987–1994. N Engl J Med 343:1742–1749
Sato H, Sone H, Sagai M, Suzuki KT, Aoki Y (2000) Increase in mutation frequency in lung of Big Blue rat by exposure to diesel exhaust. Carcinogenesis 21:653–661
Schaumann F, Borm PJ, Herbrich A, Knoch J, Pitz M, Schins RP, Luettig B, Hohlfeld JM, Heinrich J, Krug N (2004) Metal-rich ambient particles (particulate matter 2.5) cause airway inflammation in healthy subjects. Am J Respir Crit Care Med 170:898–903
Schins RP, Lightbody JH, Borm PJ, Shi T, Donaldson K, Stone V (2004) Inflammatory effects of coarse and fine particulate matter in relation to chemical and biological constituents. Toxicol Appl Pharmacol 195:1–11
Schneider A, Neas L, Herbst MC, Case M, Williams RW, Cascio W, Hinderliter A, Holguin F, Buse JB, Dungan K, Styner M, Peters A, Devlin RB (2008) Endothelial dysfunction: associations with exposure to ambient fine particles in diabetic individuals. Environ Health Perspect 116:1666–1674
Schneider A, Hampel R, Ibald-Mulli A, Zareba W, Schmidt G, Schneider R, Ruckerl R, Couderc JP, Mykins B, Oberdorster G, Wolke G, Pitz M, Wichmann HE, Peters A (2010) Changes in deceleration capacity of heart rate and heart rate variability induced by ambient air pollution in individuals with coronary artery disease. Part Fibre Toxicol 7:29
Seagrave J, Campen MJ, McDonald JD, Mauderly JL, Rohr AC (2008) Oxidative stress, inflammation, and pulmonary function assessment in rats exposed to laboratory-generated pollutant mixtures. J Toxicol Environ Health A 71:1352–1362
Semmler M, Seitz J, Erbe F, Mayer P, Heyder J, Oberdorster G, Kreyling WG (2004) Long-term clearance kinetics of inhaled ultrafine insoluble iridium particles from the rat lung, including transient translocation into secondary organs. Inhal Toxicol 16:453–459
Serinelli M, Gianicolo EA, Cervino M, Mangia C, Portaluri M, Vigotti MA (2010) Acute effects of air pollution in Brindisi (Italy): a case-crossover analysis. Epidemiol Prev 34:100–107
Shinyashiki M, Eiguren-Fernandez A, Schmitz DA, di Stefano E, Li N, Linak WP, Cho SH, Froines JR, Cho AK (2009) Electrophilic and redox properties of diesel exhaust particles. Environ Res 109:239–244
Stahlhofen W, Gebhart J, Heyder J (1980) Experimental determination of the regional deposition of aerosol particles in the human respiratory tract. Am Ind Hyg Assoc J 41:385–398a
Stewart JC, Chalupa DC, Devlin RB, Frasier LM, Huang LS, Little EL, Lee SM, Phipps RP, Pietropaoli AP, Taubman MB, Utell MJ, Frampton MW (2010) Vascular effects of ultrafine particles in persons with type 2 diabetes. Environ Health Perspect 118:1692–1698
Stout SL, Wyatt TA, Adams JJ, Sisson JH (2007) Nitric oxide-dependent cilia regulatory enzyme localization in bovine bronchial epithelial cells. J Histochem Cytochem 55:433–442
Sun G, Crissman K, Norwood J, Richards J, Slade R, Hatch GE (2001) Oxidative interactions of synthetic lung epithelial lining fluid with metal-containing particulate matter. Am J Physiol Lung Cell Mol Physiol 281:L807–L815
Sun Q, Wang A, Jin X, Natanzon A, Duquaine D, Brook RD, Aguinaldo JG, Fayad ZA, Fuster V, Lippmann M, Chen LC, Rajagopalan S (2005) Long-term air pollution exposure and acceleration of atherosclerosis and vascular inflammation in an animal model. JAMA 294:3003–3010
Sun Q, Yue P, Deiuliis JA, Lumeng CN, Kampfrath T, Mikolaj MB, Cai Y, Ostrowski MC, Lu B, Parthasarathy S, Brook RD, Moffatt-Bruce SD, Chen LC, Rajagopalan S (2009) Ambient air pollution exaggerates adipose inflammation and insulin resistance in a mouse model of diet-induced obesity. Circulation 119:538–546
Suzuki T, Kanoh T, Kanbayashi M, Todome Y, Ohkuni H (1993) The adjuvant activity of pyrene in diesel exhaust on IgE antibody production in mice. Arerugi 42:963–968
Triantaphyllopoulos K, Hussain F, Pinart M, Zhang M, Li F, Adcock I, Kirkham P, Zhu J, Chung KF (2011) A model of chronic inflammation and pulmonary emphysema after multiple ozone exposures in mice. Am J Physiol Lung Cell Mol Physiol 300:L691–L700
Valavanidis A, Fiotakis K, Bakeas E, Vlahogianni T (2005) Electron paramagnetic resonance study of the generation of reactive oxygen species catalysed by transition metals and quinoid redox cycling by inhalable ambient particulate matter. Redox Rep 10:37–51
Valavanidis A, Fiotakis K, Vlachogianni T (2008) Airborne particulate matter and human health: toxicological assessment and importance of size and composition of particles for oxidative damage and carcinogenic mechanisms. J Environ Sci Health C Environ Carcinog Ecotoxicol Rev 26:339–362
van der Vliet A, O’Neill CA, Cross CE, Koostra JM, Volz WG, Halliwell B, Louie S (1999) Determination of low-molecular-mass antioxidant concentrations in human respiratory tract lining fluids. Am J Physiol 276:L289–L296
Veranth JM, Moss TA, Chow JC, Labban R, Nichols WK, Walton JC, Watson JG, Yost GS (2006) Correlation of in vitro cytokine responses with the chemical composition of soil-derived particulate matter. Environ Health Perspect 114:341–349
Wang XK, Lu WZ (2006) Seasonal variation of air pollution index: Hong Kong case study. Chemosphere 63:1261–1272
Wellenius GA, Burger MR, Coull BA, Schwartz J, Suh HH, Koutrakis P, Schlaug G, Gold DR, Mittleman MA (2012) Ambient air pollution and the risk of acute ischemic stroke. Arch Intern Med 172:229–234
Welty LJ, Peng RD, Zeger SL, Dominici F (2009) Bayesian distributed lag models: estimating effects of particulate matter air pollution on daily mortality. Biometrics 65:282–291
Wheat LA, Haberzettl P, Hellmann J, Baba SP, Bertke M, Lee J, McCracken J, O’Toole TE, Bhatnagar A, Conklin DJ (2011) Acrolein inhalation prevents vascular endothelial growth factor-induced mobilization of Flk-1+/Sca-1+ cells in mice. Arterioscler Thromb Vasc Biol 31:1598–1606
Wheeler AJ, Xu X, Kulka R, You H, Wallace L, Mallach G, van Ryswyk K, Macneill M, Kearney J, Dabek-Zlotorzynska E, Wang D, Poon R, Williams R, Stocco C, Anastassopoulos A, Miller JD, Dales R, Brook JR (2011) Windsor, Ontario exposure assessment study: design and methods validation of personal, indoor, and outdoor air pollution monitoring. J Air Waste Manag Assoc 61:142–156
Wiebert P, Sanchez-Crespo A, Seitz J, Falk R, Philipson K, Kreyling WG, Moller W, Sommerer K, Larsson S, Svartengren M (2006) Negligible clearance of ultrafine particles retained in healthy and affected human lungs. Eur Respir J 28:286–290
Willeke K, Baron PA (1990) Sampling and interpretation errors in aerosol monitoring. Am Ind Hyg Assoc J 51:160–168
Xu X, Yavar Z, Verdin M, Ying Z, Mihai G, Kampfrath T, Wang A, Zhong M, Lippmann M, Chen LC, Rajagopalan S, Sun Q (2010) Effect of early particulate air pollution exposure on obesity in mice: role of p47phox. Arterioscler Thromb Vasc Biol 30:2518–2527
Xu X, Deng F, Guo X, Lv P, Zhong M, Liu C, Wang A, Tzan K, Jiang SY, Lippmann M, Rajagopalan S, Qu Q, Chen LC, Sun Q (2012) Association of systemic inflammation with marked changes in particulate air pollution in Beijing in 2008. Toxicol Lett 212:147–156
Yang W, Omaye ST (2009) Air pollutants, oxidative stress and human health. Mutat Res 674:45–54
Ying Z, Kampfrath T, Thurston G, Farrar B, Lippmann M, Wang A, Sun Q, Chen LC, Rajagopalan S (2009) Ambient particulates alter vascular function through induction of reactive oxygen and nitrogen species. Toxicol Sci 111:80–88
Yoshida T, Tuder RM (2007) Pathobiology of cigarette smoke-induced chronic obstructive pulmonary disease. Physiol Rev 87:1047–1082
Zanobetti A, Schwartz J, Dockery DW (2000) Airborne particles are a risk factor for hospital admissions for heart and lung disease. Environ Health Perspect 108:1071–1077
Zanobetti A, Schwartz J, Samoli E, Gryparis A, Touloumi G, Atkinson R, Le Tertre A, Bobros J, Celko M, Goren A, Forsberg B, Michelozzi P, Rabczenko D, Aranguez Ruiz E, Katsouyanni K (2002) The temporal pattern of mortality responses to air pollution: a multicity assessment of mortality displacement. Epidemiology 13:87–93
Zanobetti A, Schwartz J, Samoli E, Gryparis A, Touloumi G, Peacock J, Anderson RH, le Tertre A, Bobros J, Celko M, Goren A, Forsberg B, Michelozzi P, Rabczenko D, Hoyos SP, Wichmann HE, Katsouyanni K (2003) The temporal pattern of respiratory and heart disease mortality in response to air pollution. Environ Health Perspect 111:1188–1193
Zanobetti A, Bind MA, Schwartz J (2008) Particulate air pollution and survival in a COPD cohort. Environ Health 7:48
Zhao PS, Dong F, He D, Zhao XJ, Zhang WZ, Yao Q, Liu HY (2013) Characteristics of concentrations and chemical compositions for PM2.5 in the region of Beijing, Tianjin, and Hebei, China. Atmos Chem Phys Discuss 13:863–901
Acknowledgments
We thank James McCracken, Ph.D., Timothy E. O’Toole, Ph.D., David Young, Jongmin Lee, Ph.D., and Duane Bolanowski for technical assistance. Work in the authors’ laboratories is supported by grants from AHA, EPA, DOD and NIH.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2014 Springer-Verlag Berlin Heidelberg
About this entry
Cite this entry
Haberzettl, P., Bhatnagar, A., Conklin, D.J. (2014). Particulate Matter and Oxidative Stress – Pulmonary and Cardiovascular Targets and Consequences. In: Laher, I. (eds) Systems Biology of Free Radicals and Antioxidants. Springer, Berlin, Heidelberg. https://doi.org/10.1007/978-3-642-30018-9_120
Download citation
DOI: https://doi.org/10.1007/978-3-642-30018-9_120
Published:
Publisher Name: Springer, Berlin, Heidelberg
Print ISBN: 978-3-642-30017-2
Online ISBN: 978-3-642-30018-9
eBook Packages: Biomedical and Life SciencesReference Module Biomedical and Life Sciences