
Abstract
This chapter deals with the human oral microbiome which contains bacteria, bacteriophages/viruses, archaea, fungi, and protozoa. Modern molecular techniques used to analyze this microbiome are dealt with such as HOMINGS, oligotyping, high-throughput sequencing, whole-genome shotgun sequencing, single-cell genome sequencing, metatranscriptomics, and community-wide transcriptome analysis. The oral microbiota in health is described as well as that in periodontal disease and dental caries. Furthermore, the architecture of biofilms in periodontitis and caries is visualized. Our knowledge on the oral microbiota challenges the current practice of chairside diagnostics.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
These keywords were added by machine and not by the authors. This process is experimental and the keywords may be updated as the learning algorithm improves.
1 The Human Oral Microbiome
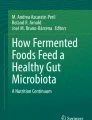
The human oral microbiome is composed of a variety of different microorganisms such as bacteria, bacteriophages/viruses, yeasts, archaea, and protozoa. It has been suggested that these organisms cause diseases by a synergistic or cooperative way and that the interspecies interactions have a crucial role whether the oral microbiota causes disease or not (He et al. 2014). What is remarkable for this microbiota is also that its commensals contribute to disease, e.g., to caries and periodontitis through ecological changes. Another noteworthy feature is that it is personalized, meaning that each person harbors a unique microbiota. This implies that the human microbiome is more different between individuals than within an individual (Fig. 10.1). It has also been shown that characteristics of an individual’s life history can be associated with the composition of the microbiome (Ding and Schloss 2014) and that the phylogenetic microbial structure varies with aging (Xu et al. 2014).

Humans are far more different from each other in their microbial composition than in their genomic composition. The colors on the left side of each individual represent bacterial phyla, while the colors on the right side indicate host genomic similarity. For the most part we contain similar phyla living in and on our bodies, including the oral cavity, but their relative abundance can be drastically different. On the other hand, our genomic composition is nearly identical, with only a small fraction (ca 0.1 %) differing across individuals (Adapted from Califf et al. 2014)
1.1 Bacteria
Bacteria have been considered the dominating part of the microbiome in man. However, while some six billion bacteria are present in the oral cavity, it contains potentially 35 times that many bacteriophages/viruses (Edlund et al. 2015). When Dewhirst et al. (2010) established the Human Oral Microbiome Database (HOMD) (http://www.homd.org/), it comprised over 600 prevalent bacterial taxa at the species level with distinct subsets predominating at different sites such as teeth, gingival sulcus, tongue, cheeks, hard/soft palate, and tonsils. The HOMD included 619 taxa from 13 phyla: Actinobacteria, Bacteroidetes, Chlamydiae, Chloroflexi, Euryarchaeota, Firmicutes, Fusobacteria, Proteobacteria, Spirochaetes, SR1, Synergistetes, Tenericutes, and TM7. The analysis comprised 1179 taxa. Among these 24 % were named, 8 % were cultivated but unnamed, and 68 % were uncultivated phylotypes. Later the number of oral phyla has been extended to 15, but 96 % of the sequences are accounted for by only 6 phyla: Actinobacteria, Bacteroidetes, Firmicutes, Fusobacteria, Proteobacteria, and Spirochaetes (Wade 2013). Recently, Camanocha and Dewhirst (2014) developed primer pairs for making phylum-selective 16S rRNA clone libraries and identified species from the lesser known oral phyla or candidate divisions including Synergistetes, TM7, Chlorobi, Chloroflexi, GN02, SR1, and WPS-2.
1.2 Bacteriophages/Viruses
Oral viruses in saliva are dominated by bacteriophages (Pride et al. 2012). Also dental plaque is inhabited by a community of bacteriophages (Naidu et al. 2014). Bacteriophages constitute the major part of the oral virome with relatively few eukaryotic viruses identified such as herpesviruses, papillomaviruses, enteroviruses, and circoviruses (Grinde and Olsen 2010; Naidu et al. 2014). The mouth has been found to have more genetic elements than the stool, i.e., viruses, plasmids, and transposons, although it has fewer bacteria (Zhang et al. 2013). Bacteriophages may serve as reservoirs for genes functioning in the oral cavity. Phage members of the oral virome can carry genes involved in resistance to complement degradation of immunoglobulins, adhesion to cells lining the oropharynx, and antibiotic resistance (Pride et al. 2012; Muniesa et al. 2013; Abeles et al. 2014; Quirós et al. 2014).
Oral viruses have gene functions that may be involved in the pathogenic roles of their host bacteria (Pride et al. 2012). The same salivary viruses could be identified at all time points over 60 days despite being present in low numbers (Abeles et al. 2014), reflecting that the oral viral ecosystem is stable. Most oral viruses are lysogenic and live in harmony with their hosts (Abeles and Pride 2014; Ly et al. 2014), and they may be important in shaping the microbial diversity of the oral cavity. Another peculiarity is that viral communities of the mouth are highly personalized (Willner et al. 2011; Pride et al. 2012), even more personalized than bacterial communities when analyzed with 16S rDNA sequencing (Abeles et al. 2014). A noteworthy feature is also that oral viruses vary according to host sex, rather than among individuals (Abeles et al. 2014). The human oral viral community is probably a result of the unique viral exposures of each individual (Abeles et al. 2014), but considerably more of the oral virobiota of people living together is shared than could be expected by chance (Robles-Sikisaka et al. 2013). Eukaryotic viruses such as Torque Teno viruses (TTVs) and SEN viruses have been found in the bloodstream of healthy people (Pride et al. 2012; Abeles and Pride 2014). Blood of healthy persons have previously been considered sterile. Both these groups of viruses are present in the human oral cavity (Pride et al. 2012). Also herpesviruses, shed in the mouth from healthy individuals, can be found in human blood (De Vlaminck et al. 2013). Therefore not only bacteria but also viruses can translocate through mucosal surfaces to the bloodstream and possibly be involved in systemic diseases.
It is well known that the human oral cavity contains a large and diverse variety of bacteria. What viruses it contains has to a great extent been overlooked. This particularly relates to the periodontal microbiota, although herpesviruses including Epstein-Barr virus and cytomegalovirus can be present in high copy counts in aggressive periodontitis and may interact with periodontopathogenic bacteria to cause the disease (Sunde et al. 2008; Slots 2011; Contreras et al. 2014). Ly et al. (2014) examined samples from saliva of periodontally healthy and diseased patients and found that the communities of viruses inhabiting saliva and subgingival and supragingival biofilms were composed mainly of bacteriophages. The virome composition was greatly reflected by the site it was collected from. The largest difference in composition was between supra-/subgingival plaque and saliva. Differences in virus composition were significantly related to the health status of viruses in plaque, but not to those in saliva. Noteworthy, there was a significant increase in myoviruses (generally lytic) in subgingival biofilm suggesting that these viruses may have a great importance to local bacterial diversity and that the virus may serve as useful indicators of the oral health status. Since viruses have the potential to form microbial communities as well as to elicit host immune response, they probably play an important role in human health (Edlund et al. 2015). Also, the fact that they are personal, persistent, and gender specific suggests that they can be important in the interplay between host genetics and the environment.
1.3 Archaea
Archaea were originally considered a primitive form of life that thrives in extreme environments. However, high numbers of methane-producing archaea (methanogens) have now been detected in the oral cavity (Belay et al. 1988), the gastrointestinal tract (Karlin et al. 1982), and vagina (Belay et al. 1990) of human beings. The reported oral archaea contain the genera Methanobrevibacter, Methanobacterium, Methanosarcina, and Methanosphaera and the order Thermoplasmatales (He et al. 2014). The main species is Methanobrevibacter oralis. Archaea have been detected in saliva, periodontitis, peri-implantitis, pericoronitis, and infected root canals (Brusa et al. 1987; Belay et al. 1988; Kulik et al. 2001; Lepp et al. 2004; Vianna et al. 2006, 2009; Vickerman et al. 2007; Conway de Macario and Macario 2009; Jiang et al. 2009; Matarazzo et al. 2011, 2012; Faveri et al. 2011; Mansfield et al. 2012; Bringuier et al. 2013). These studies detected a higher frequency of archaea in oral infections than in health. Thus the relative abundance of archaea in subgingival plaque increased with the severity of periodontitis and decreased with the reduction of periodontitis after treatment. Archaea may therefore be associated with periodontitis but the diversity of archaea is limited (Li et al. 2009). Almost all sequenced amplicons fell in the genus Methanobrevibacter of the Euryarchaeota phylum with M. oralis-like species as the most dominant. In root canal infections, presence of archaea was associated with clinical symptoms (Jiang et al. 2009). Although discussion of the clinical role of Euryarchaeota (including Methanobrevibacter smithii, M. oralis, and Methanosphaera stadtmanae) continues (Horz and Conrads 2010), and archaea are emerging organisms in complex human microbiomes (Dridi et al. 2011), methanogenic archaea do not seem to induce oral diseases directly. However, they may promote anaerobic infections through syntropic interactions with true pathogenic fermenting bacteria, e.g., through interspecies H2 transfer, thereby favoring growth of certain bacteria (Matarazzo et al. 2012). Thus, a positive correlation has been found between methanogens and Synergistes species in oral infections (Vianna et al. 2006; Vartoukian et al. 2007).
1.4 Fungi
Dupuy et al. (2014) performed massive parallel, high-throughput sequencing of internal transcribed spacer 1 (ITS1) amplicons from saliva after robust extraction methods. Their findings confirmed nearly every community member from a similar study by Ghannoum et al. (2010) who had detected 74 cultivable and 11 non-cultivable fungal genera in the oral cavity by using multitag pyrosequencing of panfungal ITS primers. A consensus on genus-level members of oral fungi (core mycobiome) was thereby reached. This study was the first to demonstrate not-yet-cultivated fungi in the oral cavity. It was suggested that such organisms could be the reason for failure in the treatment of oral fungal infections. Consensus members of the saliva microbiome were Candida/Pichia, Cladosporium/Davidiella, Alternaria/Lewia, Aspergillus/Emericella/Eurotium, Fusarium/Gibberella, Cryptococcus/Filobasidiella, and Aureobasidium. Weaker candidates for consensus inclusion were Saccharomyces, Epicoccum, and Phoma. Interestingly, Malassezia species, that are important commensals of human skin, were for the first time included in the oral core mycobiome. The oral fungal community showed a consistent intraindividual stability over time, but there was high interindividual variability (Monteira-da-Silva et al. 2014).
Interactions between fungi and bacteria, e.g., between Candida and streptococci, may influence oral health (Diaz et al. 2014). A symbiotic relationship between S. mutans and C. albicans has been found to synergize virulence of plaque biofilms in vivo (Falsetta et al. 2014). Thus S. gordonii glucosyltransferase promotes biofilm interactions with C. albicans (Ricker et al. 2014). Fungi probably have a role in maintaining a balance between microorganisms and the host (Krom et al. 2014).
1.5 Protozoa
Protozoa are parts of the normal microbiome. The best known are Entamoeba gingivalis and Trichomonas tenax (Vozza et al. 2005). They are present in subjects who neglect their oral hygiene and predominantly in subgingival plaque from patients with periodontal disease (Lange et al. 1983). Both have been linked to gingivitis and they were once considered pathogens. T. tenax has been correlated with xerostomia, burning mouth, and periodontal pockets (Kurnatowska 1993; Kurnatowska and Kurnatowski 1998). Later, it has become clear that these organisms increase when the oral hygiene deteriorates. Their increase may be due to nutrients accessible from debris and bacteria (Wade 2013). It is interesting though that metronidazole, frequently used as an effective supplement in the treatment of periodontitis, is active against both Entamoeba and Trichomonas.
2 Techniques to Analyze the Oral Microbiota
It should be realized that every technique that has been used to detect oral microorganisms has its strengths and limitations. Not all of these techniques will be dealt with here. Microscopy and culture were long standard methods for assessment of the oral microbiota. Later, culture helped us become more familiar with this microbiota when methods for recovery of anaerobic bacteria were developed. However, it soon became clear that only half of the oral microbiota could be cultured. Therefore culture-independent methods were exploited, particularly DNA-DNA hybridization and PCR-based assays. DNA-DNA hybridization (checkerboard) relied though on bacteria that could be cultivated for the making of whole genomic probes (Socransky et al. 1994), but reverse-capture checkerboard hybridization did not (Paster et al. 1998). Checkerboard DNA-DNA hybridization was helpful delineating bacteria clinically related to periodontitis such as the red and the orange complex (Socransky et al. 1998). Since there was reason to believe that also not-yet-cultivated bacteria could be involved in disease methods, targeting the small subunit (16S) ribosomal RNA molecule was used. These efforts have provided a vast amount of knowledge and description of the oral microbiota. They have also shown that the oral microbiota is not uniform but varies from site to site (Fig. 10.2). The information has been collected in the first curated collection of a human-associated microbiome, HOMD, which provides a description of the organisms and their genomics together with a 16S rRNA identification tool (Dewhirst et al. 2010), and later in the CORE database that is a phylogenetically curated 16S rDNA database of the core oral microbiome (Griffen et al. 2011). Although 16S rRNA gene amplification and Sanger sequencing significantly increased our knowledge of the major components of the oral microbiota, they did not provide information of the entire microbiota. Organisms that are present in low amounts were first revealed by pyrosequencing (next-generation sequencing methods).

Site specificity of predominant bacterial species in the mouth. Bacterial species or phylotypes were selected on the basis of their detection in multiple subjects for a given site. Distributions of bacterial species in oral sites among subjects are indicated by the columns of boxes to the right of the tree as follows: not detected in any subject (clear box), < 15 % of the total number of clones assayed (yellow box), and ≥ 15 % of the total number of clones assayed (green box). The 15 % cutoff for low and high abundance was chosen arbitrarily. Marker bar represents a 10 % difference in nucleotide sequences (From Aas et al. 2005)
2.1 HOMINGS
HOMINGS (http://homings.forsyth.org) apply the speed and efficiency of the next-generation sequencing using the Illumina platform. Almost 600 oral bacterial taxa can be identified with this technique which provides genus-level identification of the remaining sequences for 129 genera. It is thus more comprehensive than its predecessor HOMIM which gave simultaneous microarray detection of about 270 of the most prevalent, cultivated, and not-yet-cultivated oral bacterial species.
2.2 Oligotyping Analysis of the Human Oral Microbiome
A limited taxonomic resolution has often prevented understanding the census of bacterial populations in healthy individuals. By using 16S rRNA gene sequence data from nine sites in the oral cavity, Eren et al. (2014) identified 493 oligotypes from their V1-V3 data and 360 oligotypes from the V3-V5 data. The oligotypes were associated with species-level taxon names by comparing with HOMD. The authors discovered closely related oligotypes differing sometimes by only a single nucleotide that showed widely different distributions among oral sites and samples. Different habitat distributions of closely related oligotypes indicated a level of ecological and functional biodiversity not recognized previously. This technique combined with Shannon entropy has the capacity to analyze entire microbiomes and discriminate between closely related but distinct taxa in different habitats.
2.3 High-Throughput Sequencing (Pyrosequencing)
16S rRNA sequencing using next-generation sequencing has provided a wealth of new knowledge on the genetic composition of the oral microbiome in health and disease. The most useful of these approaches have relied on the 454 (Roche) pyrosequencing platform. In Table 10.1, the advantages and limitations of different high-throughput sequencing platforms are summarized.
2.4 Whole-Genome Shotgun Sequencing
Whole-genome shotgun sequencing (WGS) can provide highly accurate sequences in an economic way and has a fast turnaround (Hasan et al. 2014). WGS metagenomic sequencing has proved to be a powerful tool for studying the human microbiome. At present, WGS metagenomic data contain millions to billions of short reads and offer an unprecedented opportunity to identify species at or near strain level and their abundance.
2.5 Single-Cell Genome Sequencing
Remarkable in the identification of bacteria is single-cell genome sequencing which enables not only identification of microbes but links their functions to species, which is not feasible with metagenomic techniques. It also analyzes low-abundance species that can be lost in community-based analyses and can be useful in complementing metagenomic analyses (Yilmaz and Singh 2012). An ultimate goal of single-cell sequencing is recovery of genome sequences from each cell within an environment (Clingenpeel et al. 2015).
2.6 Metatranscriptomics of the Oral Microbiome during Health and Disease
Although new techniques have revealed what organisms are present in the oral microbiome, they do not tell anything about the viability of the organisms or their functions. Therefore efforts have been made recently to use microbiomics, metagenomics, and transcriptomics to better understand the role of the oral microbiome in health and disease. This may also help us to more efficiently prevent these diseases and provide a personalized treatment.
Our indigenous microbiota is closely linked to health. However, when disrupted the same microbiota can induce disease. Such diseases are characterized by changes in the relative amounts of different species. While such changes in the microbiota occur, it is also clear that the members of the microbial communities can differ markedly between individuals (Ge et al. 2013). This applies to the microbiota of both healthy and diseased individuals. In a study based on nine patient-matched healthy and diseased samples, 160,000 genes were compared in healthy and diseased periodontal communities (Jorth et al. 2014). Massive parallel RNA sequencing was used to demonstrate changes in the composition and gene expression of the microbiota in health and periodontitis. It was shown that both communities exhibited defined differences in metabolism that were conserved between patients. In contrast, the metabolic gene expression of individual species within the community varied greatly between patients. Disease-associated communities also showed conserved changes in metabolic and virulence gene expression. Thus, by using transcriptional profiling the authors could determine changes in the composition and gene expression of the human oral microbiota in health and periodontitis.
By using metatranscriptome analysis of periodontal biofilm in vitro, it was demonstrated that addition of periodontal pathogens to a healthy biofilm multispecies model had a drastic effect in changing the gene expression profiles of the organisms of the healthy community (Frias-Lopez and Duran-Pinedo 2012). Chaperones were highly upregulated, possibly due to stress, and there was a significant upregulation of ABC transporter systems and putative transposases. With pathogens present, proteins related to growth and division, as well as a large portion of transcription factors, were upregulated.
2.7 Community-Wide Transcriptome Analysis of the Oral Microbiome in Subjects With and Without Periodontitis
Our knowledge on the in situ activities of the organisms and their interaction with each other and with the environment is limited. Such knowledge may be obtained by characterizing gene expression profiles of the microbiome. In situ genome-wide transcriptome variation was studied in the subgingival microbiome of six periodontally healthy individuals and seven individuals with periodontitis (Duran-Pinedo et al. 2014). The overall metabolic activities defining disease were related to iron acquisition, lipopolysaccharide synthesis, and flagella synthesis. It was both noteworthy and unexpected that the majority of virulence factors upregulated in periodontitis came from organisms not considered as major pathogens. Also remarkable was that one of the organisms with characterized gene expression profile was from the uncultured candidate division TM7 exhibiting upregulation of putative virulence factors in disease. This demonstrated the importance of in situ metatranscriptomic studies for studying the possible etiological role of uncultured organisms. Unexpectedly, no viral sequence was detected in either the metagenome or the metatranscriptome.
3 Oral Microbiota in Health
The oral microbiota in health is highly diversified. It consists of approximately 600 predominant species (Dewhirst et al. 2010) that contribute to the health and physiology of the oral cavity. Two main types of tissues are colonized: soft and hard tissues. It is also clear that the oral cavity contains different niches for bacterial growth with different bacterial profiles that are site and subject specific (Fig. 10.2). Even close sites such as the dorsal and lateral sides of the tongue dorsum (Aas et al. 2005) and the vestibular and lingual surfaces of incisors and canines (Simon-Soro et al. 2013) have different microbiotas. The oral microbiota has, due to its continuum with the external environment, developed features to counteract challenges from foreign bacteria. There is probably a core microbiome for health which is common to all individuals (Zarco et al. 2012). In addition, there is a variable microbiome unique to individuals depending on lifestyle and physiological differences. Supporting the existence of a core microbiome was that identical bacterial sequences were detected in the oral cavities of unrelated healthy persons (Zaura et al. 2009). Transcription profiling defined a functional core microbiota of nearly 60 species in dental plaque (Peterson et al. 2014), and Wang et al. (2013) described a core disease-associated community in periodontitis by metagenomic sequencing. A study based on a large set of near full-length sequences in 10 healthy individuals identified 10 variables shared by 11 bacterial species (Bik et al. 2010). However, there were also significant interindividual differences. This supported the presence of both a core and a variable microbiome in the oral cavity. Based on several literature reports (Zarco et al. 2012) the major genera with the largest representation in the oral cavity were found to include Streptococcus, Veillonella, Granulicatella, Gemella, Actinomyces, Corynebacterium, Rothia, Fusobacterium, Porphyromonas, Prevotella, Capnocytophaga, Neisseria, Haemophilus, Treponema, Lactobacterium, Eikenella, Leptotrichia, Peptostreptococcus, Staphylococcus, Eubacteria, and Propionibacterium.
3.1 Microbiota in Periodontal Disease
Over the years, there have been several milestones and hypotheses on the microbial etiology of periodontitis (Hajishengallis and Lamont 2012). Etiologies related to specific organisms (amoeba, spirochetes, fusiforms, or streptococci), nonspecific plaque hypothesis/mixed anaerobic infections, microbial shift in periodontitis, specific plaque hypothesis, red complex bacteria (Porphyromonas gingivalis, Tannerella forsythia, Treponema denticola), ecological catastrophe hypothesis, disruption of periodontal tissue homeostasis, keystone pathogens, and polymicrobial synergy and dysbiosis (PSD) can be mentioned. This variability may partly be considered results of increased knowledge related to instrumental analytical improvements. However, rather than mentioning the microorganisms involved under each etiological heading, space will be devoted here to the most recent concept, PSD.
In the PSD model, it is recognized that the gingival crevice is colonized by a diverse microbiota where compatible microorganisms assemble into heterotypic communities. These are in equilibrium with the host. The organisms are controlled by the host, despite their production of toxic products such as proteases, overgrowth, and pathogenicity. Noteworthy, the microbial components of these communities vary over time from person to person and from site to site. The virulence of the entire community is increased by keystone pathogens such as P. gingivalis which can have interactive communication with accessory pathogens like the mitis group of streptococci, thereby orchestrating inflammatory disease by remodeling a normally benign microbiota into a dysbiotic one (Hajishengallis and Lamont 2012; Hajishengallis et al. 2012). The host immune response is not impaired and the abundance of the dysbiotic community increases, destroying tissue homeostasis and causing destruction of periodontal tissues. PSD is probably not the last model of periodontitis that will be launched, but it is attractive from the point that it reconciles the joint effects of a synergetic and a dysbiotic microbial community, rather than select organisms.
In terms of the microorganisms related to periodontitis, it should be mentioned that it is now moderate evidence in the literature to support the association of 17 species or phylotypes from the phyla Bacteroidetes, Candidatus Saccharibacteria, Firmicutes, Proteobacteria, Spirochaetes, and Synergistetes with periodontitis. Also the archaea domain seems to have an association with this disease (Pérez-Chaparro et al. 2014). As already mentioned, every human body carries a personalized microbiome that is important for maintaining health but also for eliciting disease (Zarco et al. 2012; Califf et al. 2014). According to Schwarzberg et al. (2014) who used next-generation sequencing, there is not a single microbial composition that represents a healthy periodontal state and that recovery from periodontal disease appears to shift from a personalized disease state to a personalized healthy state. Although there may be a consensus that particular communities will shift according to disease, there may not be a healthy part of these bacteria that is consistent across individuals. In contrast to this Griffen et al. (2012), using 16S multiple region pyrosequencing, found differences between health- and periodontitis-associated bacterial communities at all phylogenetic levels and distinct community profiles. Spirochaetes, Synergistetes, and Bacteroidetes were prominent phyla in disease, while Proteobacteria was detected at higher levels in healthy controls. Their data confirmed the association of species such as P. gingivalis, T. denticola, and T. forsythia with disease, but Filifactor alocis appeared to be at least as prevalent and disease associated. Abusleme et al. (2014), using 454 pyrosequencing of 16S rRNA gene libraries, found that periodontitis communities were high in Spirochaetes, Synergistetes, Firmicutes, and Chloroflexi among other taxa, while the proportion of Actinobacteria, especially Actinomyces, was more abundant in health.
A number of bacterial taxa and genes have been found to differ between health and disease. Until now data sets across studies have not been compared directly, and we do not know if the microbial variations observed across studies are consistent. Kirst et al. (2015) used 16S rRNA sequencing to survey the subgingival microbiota in 25 subjects with chronic periodontitis and 25 controls and compared their data with those of the Human Microbiome Project (HMP) (Turnbaugh et al. 2007; Griffen et al. 2012; Abusleme et al. 2013). They found a significantly altered microbiota with decreased heterogeneity in periodontal disease. Comparison with the other data sets showed that the subgingival microbiota clustered by study. However, differences between periodontal health and disease were greater than the technical variations between the studies. Two microbial clusters were detected. One was driven by Fusobacterium and Porphyromonas and was associated with periodontitis; the other consisted of Rothia and Streptococcus and was related to health.
In a study by Ly et al. (2014), the oral bacteriophage membership was significantly changed in persons with periodontitis compared to healthy subjects, mainly as a result of abundance of myoviruses in subgingival plaque. Myoviruses are mainly lytic. Their predominance in subjects with periodontitis suggested an active role for viruses in driving bacterial diversity in the periodontal pocket. They were more abundant than siphoviruses which generally have a lysogenic lifestyle. In supragingival plaque, however, there was no difference between myoviruses and siphoviruses. The altered ecology suggested for bacterial involvement in periodontitis could therefore also involve bacteriophages.
3.2 Biofilm Architecture in Periodontitis
Sampling of dental plaque will destroy its architecture making it difficult to conclude firmly on the relative pathogenic role of taxa. When different materials were kept for several days in periodontal pockets of patients with periodontitis and examined with electron microscopy and fluorescence in situ hybridization (FISH), those parts of carriers extending into the deepest zone of the pocket were mainly colonized by spirochetes and Gram-negative bacteria (Wecke et al. 2000). Those kept in shallower regions were colonized by streptococci. The methods allowed detailed analysis of the architecture of biofilms and identification of putative periodontal pathogens with single-cell resolution. Previous investigations had revealed presence of novel yet uncultivated organisms at a high frequency in periodontal pockets (Moter et al. 1998). All patients with rapidly progressive periodontitis (n = 53) harbored oral treponemes that were either new species such as T. maltophilum or uncultivable phylotypes. When enamel slices were used to examine the microbiota development of dental plaque, channels or pores filled with extracellular polymers were seen throughout the biofilm (Wood et al. 2000). Staining and confocal microscopy showed that the most viable and active areas of the biofilm were in the central parts and parts lining the channels. Plaque biofilms in the gingival crevice had a thin densely adherent layer on the surface of the root, while the bulk of the biofilm had a looser structure particularly where there was contact with the epithelial lining of the gingival crevice or periodontal pocket (Fig. 10.3). In outer layers structures such as corncob, test-tube brush, or rosette formations were detected together with not-yet-cultivated organisms such as spirochetes and members of the TM7 phylum (Fig. 10.4). In the plaque itself interacting bacteria exhibited a spatial organization, e.g., between streptococci and Fusobacterium nucleatum.

Fluorescence in situ hybridization (FISH) of a subgingival biofilm showing the close spatial relationship between facultatively anaerobic Streptococcus spp. (orange) and obligately anaerobic Fusobacterium spp. (magenta). Subgingival biofilms of periodontitis patients were obtained using a carrier system. Bacteria were visualized in 3 μm cross sections of the biofilms using the following probes simultaneously: probe EUB338, which detects most bacteria (green); probe Strep1⁄2, which shows streptococci; probe FUS664, which detects most Fusobacterium spp.; and nonspecific nucleic acid stain DAPI (blue). Details of oligonucleotide probes are available at probeBase (http://www.microbial-ecology.net/probebase/) (From Marsh et al. (2011) with permission)

High numbers of group I treponemes (orange) in a subgingival biofilm, most of which are yet uncultured. The carrier section was hybridized with probe TRE I together with FUNU for detection of Fusobacterium nucleatum⁄canifelinum (light blue), which forms a cluster in the lower left corner, and DAPI (dark blue) (From Marsh et al. (2011) with permission)
3.3 Bacteria Associated with Caries
Recent theories divide the dental caries process into three reversible stages: the dynamic stability stage, the acidogenic stage, and the aciduric stage (Takahashi and Nyvad 2008, 2011; Nyvad et al. 2013). The microbiota on clinically sound enamel consists mainly of non-mutans streptococci and Actinomyces. Here acidification is mild and infrequent which is reflected in a balanced demineralization/remineralization or a shift in the mineral balance toward a net mineral gain (dynamic stability stage). Acidification becomes moderate and frequent when sugar is added. This may increase the acidogenicity and acidurance of non-mutans bacteria. There can also be a selective increase in more aciduric strains such as low pH non-mutans streptococci. In the end, this will shift the demineralization/remineralization balance, so that a net mineral loss occurs, leading to initiation/progression of dental caries (acidogenic stage). If the acidogenic conditions become severe and prolonged, aciduric bacteria will predominate by acid-induced selection (aciduric stage). At this stage, mutans streptococci, lactobacilli, aciduric strains of non-mutans streptococci, Actinomyces, bifidobacteria, and yeasts may become dominant.
Different components of the microbiota may play different roles in initial enamel lesions compared to caries extension into dentin. The hydroxyapatite-rich enamel likely requires a more acidic microbiota for demineralization than dentin. The highly acidogenic species include S. mutans, acidogenic non-mutans streptococci, Actinomyces species, and Bifidobacterium/Scardovia species (Chalmers et al. 2015), whereas caries progression into dentin may involve proteolysis by Prevotella species of proteins denatured by acidic species (Hashimoto et al. 2011). It seems likely that the proteolytic component also will lead to pulp tissue necrosis considering the frequent detection of Gram-negative taxa in root canal infections.
As for the microorganisms involved in caries, direct pyrosequencing of samples from dental cavities showed that cavities are not dominated by S. mutans but contain a complex community of bacterial species (Belda-Ferre et al. 2012). This supported previous 16S rRNA sequencing studies (Corby et al. 2005; Aas et al. 2008) and the idea that dental caries is a polymicrobial disease. Pyrosequencing also supported that oral bacteria are specific at different stages of caries progression (Jiang et al. 2014). In children with severe dental caries, the genera Streptococcus, Granulicatella, and Actinomyces had increased significantly (Jiang et al. 2013).
By performing comprehensive 16S DNA profiling of the dental plaque microbiome of both caries-free and caries-active microbiomes, the signatures associated with dental health outnumbered those associated with dental caries by nearly twofold (Peterson et al. 2013). It was suggested that a shift in the abundance of groups of species, rather than the appearance of new cariogenic species or the pathogenicity of a single species, best describes the distinction between caries-free and caries-active microbiota.
Detection of major bacteria present in dental caries needs to be followed by information on the metabolic activity of the biofilm. Therefore, approaches such as metagenomic, metatranscriptomic, metaproteomic, and metabolomic analysis should be used to provide better information on the dynamic caries process. The precise determination of function requires the analysis of individual cells and cultures. In this context, it is important that previously uncultured microorganisms are being brought to culture. Emphasis should also be made to obtain site-specific sampling of microbial communities for studying the molecular ecology in situ of caries (Dige et al. 2014).
The next-generation sequencing technique was combined with a metagenomic technique and showed that individuals who had never suffered from caries had an overrepresentation of functional genetic categories such as genes for antimicrobial peptides and quorum sensing. They did not carry mutans streptococci (Belda-Ferre et al. 2012). Interestingly, several isolates belonging to healthy conditions inhibited the growth of cariogenic bacteria when they were co-cultured. Thus, the metagenomic approach enabled quantitation of the most abundant bacteria and confirmed presence of bacteria with a protective effect against cariogenic species.
3.4 Architecture of Biofilms in Caries
In occlusal caries, FISH showed a distinct difference in the bacterial composition between different ecological niches in the caries process (Dige et al. 2014). Biofilms located at the entrance of fissures had an inner compact layer of microorganisms structured in palisades often with a columnar pattern (Fig. 10.5). They were often identified as Actinomyces and were covered by a loosely structured bacterial layer consisting of various genera that were similar to supragingival biofilm. Within the proper fissure the biofilm appeared less metabolically active as estimated from low fluorescence signal intensity and presence of material of nonbacterial origin. Invasion of bacteria, often Lactobacillus and Bifidobacterium spp., into dentinal tubules was seen only at advanced stages of caries with cavity formation.

(a–c) Images of in vivo biofilms on dental occlusal surfaces. (a–c) Toluidine blue-stained sections showing an overview of occlusal surfaces with shallow fissure-like morphology (a), groove-like morphology, (b) and cavitated caries lesion (c). Arrows refer to the areas illustrated in b, d, i, j, and l, respectively. (d–i) Confocal laser scanning microscopy images of microbial colonization patterns from above the entrance of shallow fissures and groove-like occlusal surfaces. In all confocal laser scanning microscopy images, red represents all bacteria that are neither Streptococcus spp. (yellow/green in d–i) nor Actinomyces spp. (purple/magenta in e, g–i) nor Fusobacterium spp. (purple/magenta in f). Note that the biofilm could be divided into an inner compact layer of palisade-like bacteria (d–h) often with a columnar pattern (g, h) on top of which a looser structured layer (d, e, f, h, i) with non-stained voids (d, i) was seen. The outermost part of the decalcified enamel showed a thin auto-fluorescent layer without bacteria (blue or green in d, g), and invaginations of developmental origin were often filled with bacteria (d, g, arrows). All images are oriented with the biofilm surface upward. Scale bars: 500 μm a–c) and 25 μm (d–i) (Adopted from Dige et al. (2014) with permission)
3.5 Future Chairside Diagnostics of Dental Plaque
Molecular studies have informed us about the great complexity of the oral microbiota both in health and disease, and we have been able to study microbial communities on a large scale due to advancements in sequencing and bioinformatics. They have also pointed out that specific organisms are not responsible for disease but rather rely on the supplementary action of other organisms. Recent studies have further taught us that a species can comprise strains of different virulence. This throws doubt on the species as a reasonable diagnostic unity (Wade 2013). The development of molecular diagnostics has been so fast that it seems reasonable now to turn to functions of the microbiota, rather than to what organisms are present. This makes a great challenge to chairside diagnostics of dental plaque which should try to implement the new knowledge into their procedures, rather than focus on a handful of select organisms.
References
Aas JA, Paster BJ, Stokes LN, et al. Defining the normal bacterial flora of the oral cavity. J Clin Microbiol. 2005;43:5721–32.
Aas JA, Griffen AL, Dardis SR, et al. Bacteria of dental caries in primary and permanent teeth in children and young adults. J Clin Microbiol. 2008;46:1407–17.
Abeles SR, Pride DT. Molecular bases and role of viruses in the human microbiome. J Mol Biol. 2014. http://dx.doi.org/10.1016/j.jmb.2014.07.002.
Abeles SR, Robles-Sikisaka R, Ly M, et al. Human oral viruses are personal, persistent and gender-consistent. ISME J. 2014;8:1753–67.
Abusleme L, Dupuy AK, Dutzan N, et al. The subgingival microbiome in health and periodontitis and its relationship with community biomass and inflammation. ISME J. 2013;7:1016–25. http://dx.doi.org/10.1038/ismej.2012.174.
Abusleme L, Hong BY, Dupuy AK, et al. Influence of DNA extraction on oral microbial profiles obtained via 16S rRNA gene sequencing. J Oral Microbiol. 2014;6. doi:10.3402/jom.v6.23990.
Belay N, Johnson R, Rajagopal BS, et al. Methanogenic bacteria from human dental plaque. Appl Environ Microbiol. 1988;54:600–3.
Belay N, Mukhopadhyay B, Conway de Macario E, et al. Methanogenic bacteria in human vaginal samples. J Clin Microbiol. 1990;28:1666–8.
Belda-Ferre P, Alcaraz LD, Cabrera-Rubio R, et al. The oral metagenome in health and disease. ISME J. 2012;6:46–56.
Bik EM, Long CD, Armitage GC, et al. Bacterial diversity in the oral cavity of ten healthy individuals. ISME J. 2010;4:962–74.
Bringuier A, Khelaifia S, Richet H, et al. Real-time PCR quantification of Methanobrevibacter oralis in periodontitis. J Clin Microbiol. 2013;51:993–4.
Brusa T, Conca R, Ferrara A, et al. The presence of methanobacteria in human subgingival plaque. J Clin Periodontol. 1987;14:470–1.
Califf K, Gonzalez A, Knight R, et al. The human microbiome: getting personal. Microbe. 2014;9:410–5.
Camanocha A, Dewhirst FE. Host-associated bacterial taxa from Chlorobi, Chloroflexi, GN02, Synergistetes, SR1, TM7, and WPS-2 phyla/candidate divisions. J Oral Microbiol. 2014;6:25468. http://dx.doi.org/10.3402/jom.v6.25468.
Chalmers NI, Oh KO, Hughes CV, et al. Pulp and plaque microbiotas of children with severe early childhood caries. J Oral Microbiol. 2015;7:25951. doi:10.3402/jom.v7.25951.
Clingenpeel S, Clum A, Schwientek P, et al. Reconstructing each cell’s genome within complex microbial communities – dream or reality? Front Microbiol. 2015;5:771. doi:10.3389/fmicb.2014.00771.
Contreras A, Botero JE, Slots J. Biology and pathogenesis of cytomegalovirus in periodontal disease. Periodontol 2000. 2014;64:40–56.
Conway de Macario E, Macario AJL. Methanogenic archaea in health and disease: a novel paradigm of microbial pathogenesis. Int J Med Microbiol. 2009;299:99–108.
Corby PM, Lyons-Weiler J, Bretz WA, et al. Microbial risk indicators of early childhood caries. J Clin Microbiol. 2005;43:5753–9.
De Vlaminck I, Khush KK, Strehl C, et al. Temporal response of the human virome to immunosuppression and antiviral therapy. Cell. 2013;155:1178–87.
Dewhirst FE, Chen T, Izard J, et al. The human oral microbiome. J Bacteriol. 2010;192:5002–17.
Diaz PI, Strausbaugh LD, Dongari-Bagtzoglou A. Fungal-bacterial interactions and their relevance to oral health: linking the clinic and the bench. Front Cell Infect Microbiol. 2014;4:101. doi:10.3389/fcimb.2014.00101.
Dige I, Grønkjær L, Nyvad B. Molecular studies of the structural ecology of natural occlusal caries. Caries Res. 2014;48:451–60.
Ding T, Schloss PD. Dynamics and associations of microbial community types across the human body. Nature. 2014;509:357–60.
Dridi B, Raoult D, Drancourt M. Archaea as merging organisms in complex human microbiomes. Anaerobe. 2011;17:56–63.
Dupuy AK, David MS, Lu L, et al. Redefining the human oral mycobiome with improved practices in amplicon-based taxonomy: discovery of Malassezia as a prominent commensal. PLoS One. 2014;9:e90899.
Duran-Pinedo AE, Chen T, Teles R, et al. Community-wide transcriptome of the oral microbiome in subjects with and without periodontitis. ISME J. 2014;8:1659–72.
Edlund A, Santiago-Rodriguez TM, Boehm TK, et al. Bacteriophage and their potential roles in the human oral cavity. J Oral Microbiol. 2015;7:27423. http://dx.doi.org/10.3402/jom.v7.27423.
Eren AM, Borisy GG, Huse SM, et al. Oligotyping analysis of the human oral microbiome. Proc Natl Acad Sci U S A. 2014;15(111):E2875–84. doi:10.1073/pnas.140964412.
Falsetta ML, Klein MI, Colonne PM, et al. Symbiotic relationship between Streptococcus mutans and Candida albicans synergizes virulence of plaque biofilms in vivo. Infect Immun. 2014;82:1968–81.
Faveri M, Gonҫalves LFH, Feres M, et al. Prevalence and microbiological diversity of Archaea in peri-implantitis subjects by 16S ribosomal RNA clonal analysis. J Periodontal Res. 2011;46:338–44.
Frias-Lopez J, Duran-Pinedo A. Effect of periodontal pathogens on the metatranscriptome of a healthy multispecies biofilm model. J Bacteriol. 2012;194:2082–95.
Ge X, Rodriguez R, Trinh M, et al. Oral microbiome of deep and shallow dental pockets in chronic periodontitis. PLoS One. 2013;8:e65520. http://dx.doi.org/10.1371/journal.pone.0065520.
Ghannoum MA, Jurevic RJ, Mukherjee PK, et al. Characterization of the oral fungal microbiome (mycobiome) in healthy individuals. PLoS Pathog. 2010;6:e1000713. doi:10.1371/journal.ppat.1000713.
Griffen AL, Beall CJ, Firestone ND, et al. CORE: a phylogenetically curated 16S rDNA database of the core oral microbiome. PLoS One. 2011;6:e19051.
Griffen AL, Beall CJ, Campbell JH, et al. Distinct and complex bacterial profiles in human periodontitis and health revealed by 16S pyrosequencing. ISME J. 2012;6:1176–85. doi:10.1038/ismej.2011.191.
Grinde B, Olsen I. The role of viruses in oral disease. J Oral Microbiol. 2010;2. doi:10.3402/jom.v2i0.2127.
Hajishengallis G, Lamont RJ. Beyond the red complex and into more complexity: the polymicrobial synergy and dysbiosis (PSD) model of periodontal disease etiology. Mol Oral Microbiol. 2012;27:409–19.
Hajishengalllis G, Darveau RP, Curtis MA. The keystone-pathogen hypothesis. Nat Rev Microbiol. 2012;10:717–25.
Hasan NA, Young BA, Minard-Smith AT, et al. Microbial community profiling of human saliva using shotgun metagenomic sequencing. PLoS One. 2014;9:e97699. doi:10.1371/journal.pone.0097699.
Hashimoto K, Sato T, Shimauchi H, et al. Profiling of dental plaque microflora on root caries lesions and the protein-denaturing activity of these bacteria. Am J Dent. 2011;24:295–9.
He J, Li Y, Cao Y, et al. The oral microbiome diversity and its relation to human diseases. Folia Microbiol (Praha). 2014. doi:10.1007/s12223-014-0342-2.
Horz H-P, Conrads G. The discussion goes on: what is the role of Euryarcheota in humans? Archaea. 2010. doi:10.1155/2010/967271.
Jiang YT, Xia WW, Li CL, et al. Preliminary study of the presence and association of bacteria and archaea in teeth with apical periodontitis. Int Endod J. 2009;42:1096–103.
Jiang W, Zhang J, Chen H. Pyrosequencing analysis of oral microbiota in children with severe early childhood dental caries. Curr Microbiol. 2013;67:537–42.
Jiang W, Ling Z, Lin X, et al. Pyrosequencing analysis of oral microbiota shifting in various caries states in childhood. Microb Ecol. 2014;67:962–9.
Jorth P, Turner KH, Gumus P, et al. Metatranscriptomics of the human oral microbiome during health and disease. mBio. 2014;5:e01012–4.
Karlin DA, Jones RD, Stroehlein JR, et al. Breath methane excretion in patients with unresected colorectal cancer. J Natl Cancer Inst. 1982;69:573–6.
Kirst ME, Li EC, Alfant B, et al. Dysbiosis and alterations in predicted functions of the subgingival microbiome in chronic periodontitis. Appl Environ Microbiol. 2015;81:783–93.
Krom BP, Kidwai S, ten Cate JM. Candida and other fungal species: forgotten players of healthy oral microbiota. J Dent Res. 2014;93:445–51.
Kulik EM, Sandmeier H, Hinni K, et al. Identification of archaeal rDNA from subgingival dental plaque by PCR amplification and sequence analysis. FEMS Microbiol Lett. 2001;196:129–33.
Kurnatowska AJ. Search for convergence between values of indicators for evaluating oral cavity status as recommended by WHO and presence of fungi or Trichomonas tenax. (Article in Polish). Med Dosw Mikrobiol. 1993;45:393–6.
Kurnatowska AJ, Kurnatowski P. Trichomonosis of the oral cavity complicated by mycosis. Parassitologia. 1998;40:339–42.
Lange DE, Stockmann H, Höcker K. Vorkommen und Identifizierung von Protozoen in der menschlichen Mundhöhle. Dtsch Zahnarztl Z. 1983;38:906–10.
Lepp PW, Brinig MM, Ouverney CC, et al. Methanogenic Archaea and human periodontal disease. Proc Natl Acad Sci U S A. 2004;101:6176–81.
Li CL, Liu DL, Jiang YT, et al. Prevalence and molecular diversity of Archaea in subgingival pockets of periodontitis patients. Oral Microbiol Immunol. 2009;24:343–6.
Loman NJ, Constantinidou C, Chan JZM, et al. High-throuhput bacterial genome sequencing: an embarrassment of choice, a world of opportunity. Nat Rev Microbiol. 2012;10:599–606. doi:10.1038/nrmicro2850.
Ly M, Abeles SR, Boehm TK, et al. Altered oral viral ecology in association with periodontal disease. mBio. 2014;5:e01133–14.
Mansfield JM, Campbell JH, Bhandari AR, et al. Molecular analysis of 16S rRNA genes identifies potentially periodontal pathogenic bacteria and archaea in the plaque of partially erupted third molars. J Oral Maxillofac Surg. 2012;70:1507–14.
Marsh PD, Moter A, Devine DA. Dental plaque biofilms: communities, conflict and control. Periodontol 2000. 2011;55:16–35.
Matarazzo F, Ribeiro AC, Feres M, et al. Diversity and quantitative analysis of Archaea in aggressive periodontitis and periodontally healthy subjects. J Clin Periodontol. 2011;38:621–7.
Matarazzo F, Ribeiro AC, Faveri M, et al. The domain Archaea in human mucosal surfaces. Clin Microbiol Infect Dis. 2012;18:834–40.
Monteira-da-Silva F, Araujo R, Sampaio-Maia B. Interindividual variability and intraindividual stability of oral fungal microbiota over time. Med Mycol. 2014;52:498–505.
Moter A, Hoenig C, Choi BK, et al. Molecular epidemiology of oral treponemes associated with periodontal disease. J Clin Microbiol. 1998;36:1399–403.
Muniesa M, Colomer-Lluch M, Jofre J. Could bacteriophages transfer antibiotic resistance genes from environmental bacteria to human body-associated bacterial populations? Mob Genet Elements. 2013;3:e25847.
Naidu M, Robles-Sikisaka R, Abeles SR, et al. Characterization of bacteriophage communities and CRISPR profiles from dental plaque. BMC Microbiol. 2014;14:175.
Nyvad B, Crielaard W, Mira A, et al. Dental caries from a molecular microbiological perspective. Caries Res. 2013;47:89–102.
Paster BJ, Bartoszyk IM, Dewhirst FE. Identification of oral streptococci using PCR-based, reverse-capture, checkerboard hybridization. Methods Cell Sci. 1998;20:223–31.
Pérez-Chaparro PJ, Gonҫalves C, Figueiredo LC, et al. Newly identified pathogens associated with periodontitis: a systematic review. J Dent Res. 2014;93:846–58.
Peterson SN, Snedsrud E, Liu J, et al. The dental plaque microbiome in health and disease. PLoS One. 2013;8:e58487.
Peterson SN, Meissner T, Su AI, et al. Functional expression of dental plaque microbiota. Front Cell Infect Microbiol. 2014;4:108. doi:10.3389/fcimb.2014.00108.
Pride DT, Salzman J, Haynes M, et al. Evidence of a robust resident bacteriophage population revealed through analysis of the human salivary virome. ISME J. 2012;6:915–26.
Quirós P, Colomer-Lluch M, Martínez-Castillo A, et al. Antibiotic resistance genes in the bacteriophage DNA fraction of human fecal samples. Antimicrob Agents Chemother. 2014;58:606–9.
Ricker A, Vickerman M, Dongari-Bagtzoglou A. Streptococcus gordonii glucosyltransferase promotes biofilm interactions with Candida albicans. J Oral Microbiol. 2014;6. doi:10.3402/jom.v6.23419.
Robles-Sikisaka R, Ly M, Boehm T, et al. Association between living environment and human oral viral ecology. ISME J. 2013;7:1710–24.
Schwarzberg K, Le R, Bharti B, et al. The personal oral microbiome obscures the effects of treatment on periodontal disease. PLoS One. 2014;9:86708.
Simon-Soro Á, Tomás I, Cabrera-Rubio R, et al. Microbial geography of the oral cavity. J Dent Res. 2013;92:616–21. doi:10.1177/0022034513488119.
Slots J. Herpesvirus periodontitis: infection beyond biofilm. J Calif Dent Assoc. 2011;39:393–9.
Socransky SS, Smith C, Martin L, et al. “Checkerboard” DNA-DNA hybridization. Biotechniques. 1994;17:788–92.
Socransky SS, Haffajee AD, Cugini MA, et al. Microbial complexes in subgingival plaque. J Clin Periodontol. 1998;25:134–44.
Sunde PT, Olsen I, Enersen M, et al. Human cytomegalovirus and Epstein-Barr virus in apical and marginal periodontitis: a role in pathology? J Med Virol. 2008;80:1007–11.
Takahashi N, Nyvad B. Caries ecology revisited: microbial dynamics and the caries process. Caries Res. 2008;42:409–18.
Takahashi N, Nyvad B. The role of bacteria in the caries process: ecological perspectives. J Dent Res. 2011;90:294–303.
Turnbaugh PJ, Ley RE, Hamady M, et al. The human microbiome project. Nature. 2007;449:804–10. http://dx.doi.org/10.1038/nature06244.
Vartoukian SR, Palmer RM, Wade WG. The division “Synergistes”. Anaerobe. 2007;13:99–106.
Vianna ME, Conrads G, Gomes BPFA, et al. Identification and quantification of archaea involved in primary endodontic infections. J Clin Microbiol. 2006;44:1274–82.
Vianna ME, Conrads G, Gomes BPFA, et al. T-RFLP-based mcrA gene analysis of methanogenic archaea in association with oral infections and evidence of a novel Methanobrevibacter phylotype. Oral Microbiol Immunol. 2009;24:417–22.
Vickerman MM, Brossard KA, Funk DB, et al. Phylogenetic analysis of bacterial and archaeal species in symptomatic and asymptomatic endodontic infections. J Med Microbiol. 2007;56:110–8.
Vozza I, Zino G, Puddu P, et al. Study on the frequency of protozoa and mycetes in the oral cavity. Minerva Stomatol. 2005;54:575–81.
Wade WG. Characterisation of the human oral microbiome. J Oral Biosci. 2013;55:143–8.
Wang J, Qi J, Zhao H, et al. Metagenomic sequencing reveals microbiota and its functional potential associated with periodontal disease. Sci Rep. 2013;3:1843. doi:10.1038/srep01843.
Wecke J, Kersten T, Madela K, et al. A novel technique for monitoring the development of bacterial biofilms in human periodontal pockets. FEMS Microbiol Lett. 2000;191:95–101.
Willner D, Furlan M, Schmieder R, et al. Metagenomic detection of phage-encoded platelet-binding factors in the human oral cavity. Proc Natl Acad Sci U S A. 2011;108 Suppl 1:4547–53.
Wood SR, Kirkham J, Marsh PD, et al. Architecture of intact natural human plaque biofilms studied by confocal laser scanning microscopy. J Dent Res. 2000;79:21–7.
Xu X, He J, Xue J, et al. Oral cavity contains distinct niches with dynamic microbial communities. Environ Microbiol. 2014. doi:10.1111/1462-2920.12502.
Yilmaz S, Singh AK. Single cell genome sequencing. Curr Opin Biotechnol. 2012;23:437–43. doi:10.1016/j.copbio.2011.11.018.
Zarco MF, Vess TJ, Ginsburg GS. The oral microbiome in health and disease and the potential impact of personalized dental medicine. Oral Dis. 2012;18:109–20. doi:10.1111/j.1601-0825.2011.01851.x.
Zaura E, Keijser BJ, Huse SM, et al. Defining the healthy “core microbiome” of oral communities. BMC Microbiol. 2009;9:259. doi:10.1186/1471-2180-9-259.
Zhang Q, Rho M, Tang H, et al. CRISPR-Cas systems target a diverse collection of invasive mobile genetic elements in human microbiomes. Genome Biol. 2013;14:R40. doi:10.1186/gb-2013-14-4-r40.
Acknowledgment
The author wants to acknowledge funding through a grant from the European Commission (FP7-HEALTH-306029 “TRIGGER”).
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2016 Springer International Publishing Switzerland
About this chapter
Cite this chapter
Olsen, I. (2016). The Oral Microbiome in Health and Disease. In: Lynge Pedersen, A. (eds) Oral Infections and General Health. Springer, Cham. https://doi.org/10.1007/978-3-319-25091-5_10
Download citation
DOI: https://doi.org/10.1007/978-3-319-25091-5_10
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-25089-2
Online ISBN: 978-3-319-25091-5
eBook Packages: MedicineMedicine (R0)