
Abstract
We discuss the use of quantitative data and methods to understand where and how COVID-19 spreads, to estimate and predict its impacts on population health and wellbeing, and to plan effective public health responses. Geographic approaches often involve developing multi-scalar and dynamic models that incorporate geographic processes and variability, harnessing big and real-time data on people’s mobilities and interactions, and paying attention to how gender, ethnicity, and other dimensions of people’s identities intersect with larger structures in impacting the uneven geographies of COVID-19 risk. Our chapter addresses each of these topics while highlighting the need for critical and place-based approaches that are sensitive to local and regional variability in COVID-19 processes and impacts.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


1 COVID-19 Data and Modeling
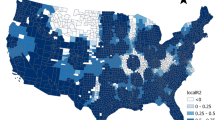
The COVID-19 pandemic demands innovative methods of quantitative analysis (QM) to understand where and how the disease spreads, to estimate and predict its impacts on population health and wellbeing, and to plan effective public health responses. We briefly review quantitative data and approaches to investigating geographical dimensions of COVID-19. These approaches will often involve: developing multi-scalar and dynamic models that incorporate geographic processes and variability; harnessing big and real-time data on people’s mobilities and interactions; and paying attention to how gender, ethnicity and other dimensions of people’s identities intersect with larger structures in impacting the uneven geographies of COVID-19 risk. Our chapter addresses each of these topics, after a brief discussion of quantitative geographic data on COVID-19.Quantitative data consist of counts or measurements of COVID-19-related disease incidence, behaviors, and contexts. From the start of the pandemic, maps and charts of COVID-19 incidence and spread have been central to our understandings of the disease and its widespread impacts (Fig. 54.1). Yet the quantitative data underlying these maps and charts are often poorly defined. Like all geographic health data, data on COVID-19 cases and deaths are outcomes of diverse reporting systems that affect what gets counted and why. Case definitions differ from place to place and change over time. Early in the pandemic, China only reported symptomatic cases; later, the country’s case definition changed to include asymptomatic cases. Reported data are also shaped by the extent and nature of COVID-19 testing. More extensive testing uncovers more positive cases, so places where testing is limited will show low COVID-19 incidence. Seizing this basic point, some federal officials in the United States (US) wanted to defund COVID-19 testing which would effectively hide the epidemic’s scope. Also, in most places, testing occurs when individuals decide to get tested or when healthcare providers request a test. As such, disease reports are structured by social, economic, and political processes that affect individual and provider decision-making. These diverse place-based processes can lead to gaps and biases in disease incidence data that strongly affect quantitative analysis results (McLafferty et al. 2020).

Maps of COVID-19 by state: (1a) total number of COVID-19 cases, (1b) COVID-19 cases per 100 K population, and (1c) COVID-19 test per 1000 population. COVID-19 case data are for July 21, 2020, from the US Centers for Disease Control and Prevention. COVID-19 test data were obtained from the Johns Hopkins Coronavirus Resources Center for July 24, 2020
In addition to maps and charts, QM can and are being used in modeling the uneven geographies of COVID-19 and planning public health interventions. Much modeling involves efforts to predict the shape of the COVID-19 curve—the timing and extent of disease spread—using spatial epidemiology approaches (Chap. 1). At a more granular level, we can also model COVID-19 spread using agent-based modeling, an approach that can incorporate differences in individual and group behavior and diverse geographic contexts. Agent-based modeling simulates the behaviors of individual “agents” in hypothetical geographic settings to predict spatial and temporal patterns of disease transmission (Mao 2014).
QM also have an important role in understanding contextual and compositional dimensions of COVID-19 prevalence. Demographic, social, environmental, and political factors at varying spatial scales affect COVID-19 incidence and outcomes (Table 54.1). These place-based factors can be analyzed using multilevel modeling, a method widely employed in health geography to investigate geographic variation in health and well-being (Duncan et al. 1996). Spatial and temporal variables such as proximity to high-prevalence areas and time along the epidemic curve also should be incorporated (Arcaya et al. 2012) because COVID-19 prevalence constantly changes as outbreaks unfold and public health interventions are adopted to contain them. Spatial modeling can also shed light on the many dimensions of COVID-19 testing including the intensity of testing and positivity rates, as illustrated in a recent case study of data for New York City (Cordes and Castro 2020).
Another key area for adoption of QM is in planning and managing the public health response. Methods like location-allocation analysis can assist in identifying locations for COVID-19 testing centers and vaccination and treatment sites to minimize people’s travel times and distances to reach them. Other applications include analyzing constraints on hospital capacity to estimate where additional capacity may be needed (Woodul et al. 2019). The enormous scope of the COVID-19 pandemic means that preventative and treatment measures such as immunizations will need to be rolled out on a massive scale to diverse populations in diverse and dispersed settings, and geographic methods will be crucial for accomplishing this equitably and efficiently.
2 GPS-Based Data and Methods
Human mobilities and interactions escalated the spread of COVID-19, and real-time quantitative geospatial data and methods are increasingly important for understanding and modeling the disease. Such data are generated from GPS-based devices including mobile phones and fixed and portable sensors recording time, date, and locational coordinates. The data can be used to assess people’s daily mobilities, social interactions, and behaviors while helping to provide appropriate recommendations to control and respond to COVID-19 spread, whether through lockdown, sheltering in place, or a stay-at-home order. This section outlines the important roles of mobile phone data as a tool for contact tracing and detecting the spread of disease during the COVID-19 pandemic.
Mobile phone data—commonly in the form of mobile applications (apps) that people can easily download—are increasingly used for contact tracing. These data can show who, when, and where a person may have encountered COVID-19 carriers (Oliver et al. 2020). This role is crucial to tracing potential carriers and those exposed to the virus. COVID-19 contact tracing may allow individuals to receive COVID-19 updates, alerts, and questions through their mobile phones, reducing the need for in-person contact.
Mobile phone contact tracing apps have been used in many countries during the pandemic. South Korea created a daily mobile phone app to alert individuals about places that have been visited by those infected by COVID-19. Singapore deployed the TraceTogether app, NZ COVID Tracer was used in New Zealand, and Australia uses the COVIDsafe app. In China, Taiwan, and Hong Kong, the contact tracing worked effectively to reduce the spread of the disease. Although the use of tracing apps has been debated within many European countries, Germany, Spain, and Latvia use similar technologies. In the United States, the country with the highest number of COVID-19 cases in the world, there are no plans to implement contact tracing apps on a national scale. However, companies like Apple and Google now provide “COVID-19 Exposure Notifications” on iPhone or Android settings, and users can decide whether to turn on the notification alerts.
Aside from contact tracing, real-time quantitative geospatial data can help researchers better understand how, to/from whom, and where COVID-19 spreads. Health geographers and epidemiologists have harnessed real-time mobility data in analyzing health-related environmental exposures and behaviors (Prior et al. 2019), and efforts are underway to apply them in modeling COVID-19. Yong et al. (2020) used data from contact tracing apps to create activity maps to determine possible exposures and examine potential epidemiological links between cases and clusters. Similar data formed the basis for Ferretti et al.’s (2020) mathematical model of the exponential phase of COVID-19 spread and the impact of public health interventions. These “big data” analyses typically require large-scale computing resources and innovative spatiotemporal and statistical approaches to identify meaningful trends and associations.
3 Critical Perspectives on Quantitative Approaches
Although quantitative geospatial data and methods have a key role in understanding and responding to COVID-19, their use needs to be framed within a critical lens. Unevenness in data collection and reporting relates not only to lack of resources and testing but also to racial, ethnic, and linguistic biases that vary geographically. In the United States, for example, the rapid spread of COVID-19 in American Indian reservations has been linked to inadequate public health infrastructure and the failure to tailor public health messages to local languages and cultural norms (Rodriguez-Lonebear et al. 2020). These processes led to underreporting and inadequate interventions that in turn fueled COVID-19 spread. Thus, axes of difference, such as race, gender, and class, become embedded in quantitative geospatial data during the data creation process (Leszczynski and Elwood 2015) and, in turn, constrain the public health response. If these biases are ignored, then crucial policy recommendations may not be identified and put forth. To avoid recreating structural harm through quantitative geospatial data and analysis, researchers may consider the three P’s: perspective, purpose, and privacy.
Perspective questions the view that data are ownerless and without bias (“the view from nowhere”). It emphasizes that data are created via socially and politically designed platforms and systems that result in gaps and biases (Elwood and Leszczynski 2018). For COVID-19, these biases can stem from differences in reporting and testing among population groups and places. Testing and reporting vary widely across localities, states/provinces, and countries reflecting resource constraints and sociopolitical influences. At the same time, factors like access to healthcare, cost of testing, and knowledge of and mistrust in healthcare systems strongly affect people’s willingness and ability to get tested. This can result in lack of testing among low-income and vulnerable populations that becomes embedded in quantitative testing data which in turn diminishes the extent of disease in these communities. To address these concerns, researchers need to think critically about data collection and reporting methods and the resulting biases and silences.
Purpose asks about what interests the data, analyses, and results serve. Geospatial applications and services can target certain groups over others (Leszczynski and Elwood 2015). In the United States, the high costs of COVID-19 testing (in some cases $150 per test), which serve the interests of biomedical companies, constrain people’s ability to get tested and in turn affect quantitative data about the pandemic. Maps can also serve varying purposes. Hotspot maps of COVID-19 can stigmatize particular places and populations despite the maps’ utility for planning and intervention. Because the pandemic has disproportionately impacted racial and ethnic minorities and other vulnerable populations, hotspot maps can promote ‘othering’ responses that involve blaming those groups for COVID-19 spread. Understanding the purposes underpinning quantitative data and results and their uneven implications for population groups and places is crucial for more accurate analyses and policy recommendations.
Privacy, the last P, speaks to purpose and perspective as well. How data is created, analyzed, and displayed can impact the level of privacy of the groups being studied. With respect to COVID-19, the contact tracing apps discussed in the previous section raise critical concerns about the privacy and confidentiality of individuals’ locational information. Where people were, when, and with whom are all revealed via these apps. Although these data are crucial for intervening to limit COVID-19 spread, the individuals tracked may have little control over how their own data are collected and stored and who has access to it. Geographers have developed methods and approaches for protecting privacy of geospatial data that can inform collection and dissemination of GPS data in the context of COVID-19.
4 Conclusion
Quantitative geospatial data and methods are useful and important in understanding and responding to COVID-19. Their applicability extends from mapping indicators of COVID-19 incidence, outcomes, spread, and impacts to more complex modeling efforts that assess underlying place- and population-based disease influences and that guide predictive modeling efforts and public health interventions. There are also significant opportunities to harness novel GPS-based big data to chart the pandemic’s many influences on mobility and social interactions and to facilitate activities such as contact tracing that are crucial in slowing the pandemic’s rapid spread. We argue that these efforts not only require larger datasets and more complex spatiotemporal models but also methods that are sensitive to people and place. The uneven impacts of COVID-19 among population groups and the varying trajectories of spread among places call for context-dependent approaches and approaches tailored to the distinct/unequal experiences and exposures of specific population groups.
We also emphasize the need for quantitative researchers to think critically about data and methods in investigating COVID-19. Quantitative data are not neutral. They reflect the platforms and processes through which they are generated, all of which differ from place to place. For COVID-19, platforms are rooted in the place-based economic and political relations that govern case definitions and funding, procedures, and regulations for reporting and testing systems. Moreover, COVID-19 data are impacted by individual and provider decisions about diagnosis and treatment and thus are filtered through healthcare systems. Along with these data issues, quantitative researchers need to think carefully about how the results of their research will be interpreted, shared, and understood and whose lives and livelihoods will be affected via privacy and purpose concerns. Critical and place-based quantitative approaches will be central to ongoing efforts to curb COVID-19 and mitigate its widespread and unequal impacts.
References
Arcaya, M., Brewster, M., Zigler, C., & Subramanian, S. V. (2012). Area variations in health: A spatial multilevel modeling approach. Health & Place, 18, 824–831.
Cordes, J., & Castro, M. (2020). Spatial analysis of COVID clusters and contextual factors in New York City. Spatial and Spatiotemporal Epidemiology, 34, 100355. https://doi.org/10.1016/j.sste.2020.100355.
Duncan, C., Jones, K., & Moon, G. (1996). Do places matter? A multi-level analysis of regional variations in health-related behaviour in Britain. Social Science and Medicine, 37(6), 725–733.
Elwood, S., & Leszczynski, A. (2018). Feminist digital geographies. Gender, Place and Culture, 25(5), 629–644. https://doi.org/10.1080/0966369X.2018.1465396.
Ferretti, L., Wymant, C., Kendall, M., Zhao, L., Nurtay, A., Abeler-Dorner, L., Parker, M., et al. (2020). Quantifying SARS-CoV-2 transmission suggests epidemic control with digital contact tracing. Science, 368, eabb6936. https://doi.org/10.1126/science.abb6936.
Leszczynski, A., & Elwood, S. (2015). Feminist geographies of new spatial media. Canadian Geographer, 59(1), 12–28. https://doi.org/10.1111/cag.12093.
Mao, L. (2014). Modeling triple-diffusions of infectious diseases, information, and preventive behaviors through a metropolitan social network—An agent-based simulation. Applied Geography, 50, 31–39. https://doi.org/10.1016/j.apgeog.2014.02.005.
McLafferty, S., Schneider, D., & Abelt, K. (2020). Placing volunteered geographic health information: Socio-spatial bias in 311 bed bug report data for New York City. Health & Place, 62, 102282. https://doi.org/10.1016/j.healthplace.2019.102282.
Oliver, N., Lepri, B., Sterly, H., Lambiotte, R., Delataille, S., De Nadai, M., et al. (2020). Mobile phone data for informing public health action across the COVID-19 pandemic lifecycle. Science Advances, 6(23), eabc0764. https://doi.org/10.1126/sciadv.abc0764.
Prior, L., Manley, D., & Sabel, C. (2019). Biosocial health geography: New exposomic geographies of health and place. Progress in Human Geography, 43(3), 531–552. https://doi.org/10.1177/0309132518772644.
Rodriguez-Lonebear, D., Barceló, N. E., Akee, R., & Carroll, S. R. (2020). American Indian reservations and COVID-19: Correlates of early infection rates in the pandemic. Journal of Public Health Management and Practice: JPHMP, 26(4), 371–377. https://doi.org/10.1097/PHH.0000000000001206.
Woodul, R. L., Delamater, P. L., & Emch, M. (2019). Hospital surge capacity for an influenza pandemic in the triangle region of North Carolina. Spatial and Spatiotemporal Epidemiology, 30, 100285. https://doi.org/10.1016/j.sste.2019.100285.
Yong, S. E. F., Anderson, D. E., Wei, W. E., Pang, J., Chia, W. N., & Tan, C. W. (2020). Connecting clusters of COVID-19: An epidemiological and serological investigation. Lancet Infectious Disease, 20(7), 809–815.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2021 The Author(s), under exclusive license to Springer Nature Switzerland AG
About this chapter

Cite this chapter
McLafferty, S.L., Guhlincozzi, A., Winata, F. (2021). Counting COVID: Quantitative Geographical Approaches to COVID-19. In: Andrews, G.J., Crooks, V.A., Pearce, J.R., Messina, J.P. (eds) COVID-19 and Similar Futures. Global Perspectives on Health Geography. Springer, Cham. https://doi.org/10.1007/978-3-030-70179-6_54
Download citation
DOI: https://doi.org/10.1007/978-3-030-70179-6_54
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-030-70178-9
Online ISBN: 978-3-030-70179-6
eBook Packages: Earth and Environmental ScienceEarth and Environmental Science (R0)