
Abstract
This chapter examines the internalizing, externalizing, and total behavior problems of 119 preschool-age children with HIV/AIDS in Uganda. Variables are examined according to an ecological model of stress and coping consistent with the co-constructivist approach proposed by Li (Psychol Bull 129:171–194, 2003). Specifically, the context in which the child is living (e.g., health variables, demographic variables, home environment, and caregiver variables represented by who is caring for the child, caregiver anxiety and depression, and child outcomes (internalizing, externalizing, and total behavior concerns) are examined. A dynamic relationship between the context and child was discovered. Nearly 45 % of the children within the sample exhibited internalizing behavior concerns. The caregiving environment, as well as caregiver adjustment (anxiety and depression), was predictive of child internalizing behaviors. Furthermore, child characteristics and demographic variables (gender, medication status, and socioeconomic status) contributed to the adjustment of the caregiver. These findings demonstrate the dynamic and reciprocal relationship between young children with HIV/AIDS in Uganda and the context in which they live.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others

Keywords
- Cerebral Malaria
- Psychological Adjustment
- Psychosocial Adjustment
- Internalize Behavior Problem
- Total Behavior Problem
These keywords were added by machine and not by the authors. This process is experimental and the keywords may be updated as the learning algorithm improves.
5.1 Impact of HIV/AIDS on the Children of Sub-Saharan Africa: Developmental Implications
In Uganda, about one million children are orphans with one or both parents dead due to HIV/AIDS. In fact, a new child is orphaned every 14 s in Uganda (Ronald and Sande 2005). The number of children who are themselves infected with HIV is 110,000, most likely through mother-to-child transmission (MTCT) (UNICEF 2008). HIV/AIDS infection has many different developmental implications. The impact of HIV/AIDS on cognitive development and psychosocial development will be addressed. Other dynamic contextual factors will also be considered in the development of preschool children with HIV/AIDS.
5.1.1 Cognitive Development
Children with HIV are at increased risk for developmental disabilities (Speigel and Bonwit 2002). This is especially true for children infected via mother-to-child transmission (MTCT), given that their central nervous systems are not fully developed when they contract the virus. Depending on the severity and progression of the central nervous system involvement, children with HIV may present with impairments that are diffuse and pervasive or impairments that are specific in nature (Armstrong et al. 1993; Knight et al. 2000). Therefore, when assessing the cognitive functioning of children with HIV, it is imperative to examine both global (e.g., intelligence quotient) and specific (e.g., processing speed, visual-spatial) domains of functioning.
In terms of language development, children with HIV tend to have difficulty with expressive language, although problems with both expressive and receptive language abilities may be present (Woodrich et al. 1999). Affected children may have decreased spontaneous and responsive vocalizations (Wachsler-Felder and Golden 2002). More generalized language impairments center on limited verbal, emotional, and motor expression. In general, pediatric HIV compromises the acquisition of language and development of language milestones. In school this may translate into the need for speech and language therapy in order to participate in and benefit from the educational setting (Papola et al. 1994). Further investigation is needed, however, to identify consistent language impairments that should be the target of early intervention.
Research on the cognitive functioning and academic achievement of young children with vertically transmitted HIV has produced inconsistent results. Some studies report that by school age, IQ scores of children with HIV are in the low-average range compared to uninfected peers who generally are within the average range (Speigel and Bonwit 2002). Papola et al. (1994) found that over half of the school-age children with HIV/AIDS that they tested were in the borderline cognitively impaired range of intelligence. Furthermore, children with HIV experiencing neurological impairment and associated cognitive delays are believed to experience continued neurological deterioration into adolescence. Ongoing cognitive deterioration has been shown in children with HIV/AIDS who have lost previously attained motor milestones (Landau and Pryor 1995).
To illustrate, Smith and colleagues (2006) collected data from 569 children between 3 and 7 years of age with HIV infections across several diverse demographic locations, including sites within Massachusetts, New York, Texas, Puerto Rico, and Illinois. These researchers reported that young children with HIV scored lower than controls on all domains of cognitive development. This was only true, however, if the children had also exhibited an AIDS-defining illness. These data suggest that children may only be at increased risk for poor cognitive outcomes if they have also had a severe illness associated with advanced stages of AIDS (Smith et al. 2006). By medically treating and preventing rapid disease progression for children with vertically transmitted HIV, the development of cognitive deficits may be significantly attenuated.
There is still much to be learned about children with HIV who survive into school age without severe cognitive complications. It is important to understand cognitive functioning because of its association with quality of life and ultimately survival. In fact, cognitive impairment can substantially affect survival, with about a threefold increased risk of death among children who are cognitively impaired (Zickler 2009).
5.1.2 Cross-Cultural Consistency
Some cross-cultural studies already have been conducted to understand the contextual impact of HIV on cognitive development. These studies provide important information on the cross-cultural consistency of neurocognitive development of individuals with HIV/AIDS. Similar impairments in abstraction/executive function, information processing speed, and learning have been reported in China and the United States (Cysique et al. 2007). In other studies including Nigerians with HIV infection, the patients exhibited a wide variety of neurological manifestations including cognitive impairment, peripheral neuropathy, and lower motor neuron facial palsy (Imam 2007).
Boivin and Giordani (2009) provide evidence for similar patterns of deficits in attention, working memory, and learning across cultures (African and American children) in children exposed to cerebral malaria and sickle-cell disease. Cross-cultural studies have also shown similar differences in brain development depending on caregiving characteristics such as age, relationship to the child, or mental health. Boivin and Giordani (2009) argue that these findings, suggesting some consistency in certain aspects of cognitive neurodevelopment in the face of chronic illness across different cultures, are consistent with Li’s (2003) co-constructivist framework and that such research is evidence for a universal brain/behavior omnibus that drives plasticity across the life span.
5.1.3 Impact of Environment on Cognitive Development
The presence of the disease, alone, may not automatically lead to negative cognitive outcomes. Other environmental factors play a role in the expressed cognitive ability of children with HIV/AIDS. Hochhauser and colleagues (2008) tested the hypothesis that children in conditions of high environmental risk would be at greater risk for the cognitive complications related to immunosuppression. They found that children in highly stressful environments are at particular risk for HIV-associated cognitive decline. Highly stressful environments are thought to negatively impact adherence to medication, and conversely, environments with reduced stress may provide some degree of neuroprotection (Hochhauser et al. 2008). Thus, it is imperative to examine the cognitive abilities of young children with HIV with careful consideration of the context in which they live. Furthermore, identifying potentially modifiable environmental factors that play a role in cognitive development provides a logical avenue for intervention.
5.1.4 Psychosocial Development
Psychosocial adjustment is a multifaceted construct that refers to the mental health, or “a state of successful performance of mental function, resulting in productive activities, fulfilling relationships with other people, and the ability to adapt to change and to cope with adversity…” (U.S. Department of Health and Human Services 1999, p. 4). Children with HIV face many psychosocial consequences that are often exacerbated by frequent hospitalizations, poor social support, and lowered school performance. Some of the challenges faced by children with HIV include the loss of cognitive abilities, physical impairments, social stigma leading to rejection and isolation, and the fear of death (Landau and Pryor 1995). Psychosocial adjustment and cognitive impairment also may interact, themselves, in the adjustment of children with HIV. Carter et al. (2003) found that adults with HIV/AIDS who exhibited depression and medical symptoms also presented with increased cognitive complaints. Children with HIV/AIDS may exhibit this same relationship between depressive symptoms and cognitive deficits, although this has not yet specifically been studied.
HIV/AIDS infection carries a significant social stigma that evokes fear and discrimination towards children with the disease. In Uganda where there has been an open HIV/AIDS awareness policy for over 20 years, the stigma is still high (Bateganya et al. 2008). Children and families must also deal with issues centering on disclosure of the medical condition, which can further perpetuate discrimination secondary to the disease (Wiener et al. 2000).
The cognitive, physical, and social effects of HIV can contribute to infected children experiencing more subjective distress than uninfected children. This distress has been associated with resulting dysphoria, hopelessness, preoccupation with the illness, and poor body image (Brown et al. 2000). Affected children are prone to more anxiety and depression than uninfected children, and their parents also report increased conduct and hyperactivity problems. Children with HIV also have been found to suffer from disruption in attention and concentration, and severe social withdrawal (Armstrong et al. 1993).
In one study looking at the service needs of school-age children with HIV within the Bronx, 42 % of children were found to exhibit formal psychiatric diagnoses that included mood disorders (depression and anxiety), attention deficit hyperactivity disorder, and adjustment disorder (Papola et al. 1994). The authors of this study also found that as children grew older, they tended to exhibit more problematic emotions and behaviors (Papola et al. 1994). However, these findings are not consistent throughout the literature, with many of the discrepancies explained by differences in the population being studied. For example, one study conducted within the United States reported that among children with HIV, behavior problems decreased as the child aged (Franklin et al. 2007). Another study conducted within the United States concluded that there were no differences between the HIV and control groups with the exception of internalizing behavior problems that were actually exhibited by the control group (Bachanas et al. 2001). Within this study the variables that did make a difference when considering the psychosocial well-being of children with HIV/AIDS were stress, age, and coping strategies employed.
Similarly, Mellins and colleagues (2003) in their study of 307 children with vertically transmitted HIV did not find a link between HIV status and behavior problems, though biological and environmental factors were important in predicting behavioral problems (Mellins et al. 2003). This finding highlights the need to consider behavior of children with HIV within the geographical context.
As evidence of the emotional impact of HIV on the Ugandan child, a study of Ugandan AIDS orphans in a rural district had higher levels of anxiety, depression, and anger than their non-orphan counterparts. Symptoms exhibited by the AIDS orphans that were indicative of clinical depressive disorder included vegetative symptoms, feelings of hopelessness, and suicidal ideation (Atwine et al. 2005).
5.1.4.1 Psychosocial Adjustment and Caregiving Context
There is evidence to suggest that children infected with HIV who are living with a caregiver other than their biological mother demonstrate elevated internalizing behavior problems, presumably because of the mother’s illness/death (Bachanas et al. 2001). In fact, researchers who failed to show internalizing behavior concerns or somatic complaints when using the CBCL as a measure of psychosocial well-being of children with HIV/AIDS speculated that this could be due to the fact that the children in their study were all cared for by their biological parents (Franklin et al. 2007). In other words none of the sample had lost their primary caregiver to the disease as is common in other resource-poor regions such as Uganda.
In a study conducted by Pelton and Forehand (2005) of 105 African American children from New Orleans 6–11 years of age, the behavior of children whose parents were living with HIV was contrasted to the behavior of children whose parents had died of AIDS. Relative to children who were still living with their biological parents, those who were orphaned exhibited significantly more internalizing and externalizing problems (Pelton and Forehand 2005).
Many children with HIV within the African context live with caregivers other than their parents. Within Uganda it is not uncommon for households to be headed by grandparents who have traditionally been the recipients of financial support from their adult children (Nyesigomwe 2006). Though these alternative caregivers largely value their role in child rearing, they may not understand the importance of continued stringent medical care for the HIV-infected children they are looking after (Jones et al. 2005) or may be unable to meet their emotional, educational, nutritional, or medical needs because of advanced age and frail condition (Nyesigomwe 2006).
Caregiving takes place within a social context, and thus, it cannot be appropriately studied without attention paid to the conditions of poverty that may compromise child outcomes (Dawes et al. 2007). The death of parents with HIV/AIDS and the subsequent taking-in of their children, often by grandparents, have exacerbated household poverty (Hodge 2008). In South Africa, where the HIV/AIDS epidemic has been an ongoing struggle, caregiving has been recognized as a significant determining factor in psychosocial adjustment. If children receive quality care, they are more likely to exhibit social and behavioral adjustment, as well as intellectual achievement (Richter et al. 2004).
No matter who the primary caregiver of the child is, he/she has a role in the development and proper adjustment exhibited by the child. For example, psychological distress exhibited by the caregiver has a negative impact on the adjustment of the child, with the child exhibiting more internalizing behavior problems (Bachanas et al. 2001). Continued examination of the impact of the caregiver on the psychosocial resiliency of children living with HIV/AIDS is paramount.
5.1.4.2 Socioeconomic Status
One of the contextual variables that can have a large impact on the psychosocial well-being of children is socioeconomic status (SES). The measure is used to understand how people within a community compare in terms of monetary income, the ability to meet the basic needs of the family members, and the level of education. Measures of SES have been shown to account for differences in performance, health, and overall well-being across illnesses.
Poverty has been established as a risk factor, associated with negative child outcomes especially for children under the age of 5 years and those in extreme and enduring poverty (Owens and Shaw 2003). Poverty also has been identified as one of the barriers preventing mothers from following through with care for their HIV-exposed infants in South Africa (Jones et al. 2005) and has been found to impact adherence to daily drug regimens among HIV-infected children in Uganda (Bikaako-Kajura et al. 2006). Nongovernmental organizations (NGOs) in Uganda have put substantial effort into helping families improve their economic situation in the hopes that it will lead to benefits in other aspects of life. For example, loans are given to families to start farms and other businesses that can then sustain an improved quality of life. Although the benefits seem to be apparent, it is not clear what impact family SES has on the psychosocial adjustment and subsequent quality of life of a child living with HIV/AIDS. Thus, it is important to understand the SES differences within the population and how it impacts the psychosocial adjustment of children with HIV/AIDS.
5.1.4.3 Psychosocial Adjustment and Child Variables
Bachanas et al. (2001) collected measures of psychological adjustment through caregiver report and child self-report of school-age children infected with HIV. The researchers found that age was a significant predictor of the children’s self-reported psychological adjustment. Younger children were shown to exhibit poorer psychological adjustment, but even when the data were analyzed without the youngest children (6 and 7 years of age), age was still significantly correlated with scores of psychological adjustment (Bachanas et al. 2001).
Another study focusing on caregiver reports of maladjustment found that aggressive behaviors of children with vertically transmitted HIV significantly decreased as the children grew older (Franklin et al. 2007). Age may be a reflection of adjustment to the diagnosis of HIV, caregiver adjustment over time, adjustment to the earlier death of a parent, or entry into school (Franklin et al. 2007).
Another hypothesis for differences in psychosocial adjustment based on increasing age is the concomitant increase in the sophistication of cognitive skills with age that may improve a child’s ability to cope with HIV-associated stressors. As the child ages and develops more sophisticated cognitive abilities, he/she is able to employ more sophisticated forms of coping (Engel and Melamed 2002). For example, older children are better able to manage their emotions using cognitive mediational control (Wertlieb et al. 1987), because they are felt to be more aware and able to label internal emotional states than can younger children. Younger children may not understand that they can regulate their emotions and are unable to see this process modeled by others because of the internal nature of emotional regulation (Compas et al. 1991). The role that increased age plays in terms of increased psychosocial adjustment, however, has yet to be clarified in resource-poor settings such as sub-Saharan Africa.
There is limited research investigating the potential impact of gender on quality of life for individuals living with HIV/AIDS in resource-poor African settings. Most of the research to date has been conducted in adults, with men reporting more positive feelings about their future than women (Chandra et al. 2009). To illustrate, men also are more likely to report feeling content and having positive experiences as compared to women (Chandra et al. 2009).
Women living with HIV also have been found to be more vulnerable to depressive symptomatology (Cook et al. 2002), show more patterns of sleep impairment, and have greater symptoms of anxiety (Junqueira et al. 2008) than men. In a large-scale study based in the United States, differences in health-related quality-of-life (QoL) scores were collected for men and women, throughout the course of HIV/AIDS treatment. Women reported lower health-related QoL scores than men in all domains, except social functioning at baseline. At 40 weeks of treatment, women still had lower scores in all QoL domains except overall health (Mrus et al. 2005). However, both men and women showed equivocal improvements in QoL over the entire course of treatment.
Although it appears that men are able to adapt to the disease more readily than women, some studies have identified strengths that women demonstrate over men when coping with HIV/AIDS. For example, women have been reported to show more strength in social functioning (Mrus et al. 2005) and score significantly higher than males on scales measuring domains of forgiveness, spirituality/religion, and personal beliefs (Chandra et al. 2009).
5.2 Theoretical Framework: Stress and Coping Model for Predicting Psychological Adjustment in HIV-Infected Children
In order to better understand the relationship between factors that may contribute to the psychological adjustment of children with HIV, Bachanas and colleagues (2001) developed a model of stress and coping. This model is used in this chapter to organize the ecological factors that are thought to contribute to the well-being of the child with HIV. The model also fits into the cross-level biocultural coconstructive framework described by Li (2003) to understand development.
In his framework Li argues that development is a dynamic process that is influenced by culture throughout the life span (life-span ontogeny) and through evolution (human phylogeny). Similarly, Bachanas et al. (2001) describe the psychosocial adjustment of children with HIV/AIDS by focusing on key health, and demographic parameters, as well as caregiver and child characteristics. This model by Bachanas and colleagues is also the organizing framework in the following chapter in this volume, which focuses on psychosocial adjustment of school-age rural Ugandan children with HIV.
Demographic parameters are important to consider throughout child development. Children are constantly interacting with the environment in which they are raised, and thus, development is impacted by the dynamic interactions experienced within that environment (Masten 2006). Some of the demographic information that may play a role in the child’s development include the child’s age, gender, weight for age, and family socioeconomic status. As noted earlier, research has shown that age and gender of the child can determine expectations for behaviors and day-to-day interactions. Living with HIV/AIDS may have very different effects on children of different ages and genders.
For example, studies conducted in resource-limited settings have found a significant association between weight for age and psychomotor functioning (Abubakar et al. 2008b). Weight for age also mediates the relationship between socioeconomic status and developmental outcome (Abubakar et al. 2008b). Furthermore, Abubakar and colleagues (2009) found that weight for age was an easily measurable benchmark in developmental monitoring for providing appropriate intervention. The family’s socioeconomic status and ability to meet the needs of the child as well as all of the family members also may impact psychosocial adjustment.
Children in advanced stages of HIV/AIDS are thought to be at the greatest risk for negative developmental outcomes. Health parameters are specified as the degree to which the disease has progressed within the child and reflect the potential for symptoms and medical complications. Researchers have found that the most informative measures of disease progression are CD4 cell counts and viral load, as they are the best predictors of mortality (Rouet et al. 2003).
Within the stress and coping model, caregiver characteristics are also considered important in understanding the psychosocial development of children with HIV. In their model of stress and coping, Bachanas and colleagues (2001) focus on the adaptation process of the caregiver. Specifically, they consider the stress level of the caregiver, the coping strategies that are used, and the overall family functioning. These factors are thought to be important because children are continually interacting with their caregivers and families, and thus, the caregiver can impact the child’s development (Masten 2006). There is a reciprocal relationship between the child and caregiver in which the child can influence the caregiver and is also influenced by the reactive behavior of the caregiver. Caregiver characteristics (e.g., anxiety, depression, and quality of interactions) all play a role in the psychosocial adjustment of the young child.
Child characteristics or personal qualities (e.g., cognitive ability, motor development) are also important within the stress and coping model. Conceptualized from the developmental psychopathology literature, the child is an active part of his or her own development. According to the core “agency” principal, there is a relationship between the brain development and the independence exhibited by the child (Masten 2006). One can use neuropsychological assessment to investigate this process, in that it gauges a child’s ability to think and learn while navigating and functioning within the physical and social environment.
Motor development also has been found to be an important part of this navigational and functional process and is often delayed in children with HIV in sub-Saharan Africa (Abubakar et al. 2008a). The impact of motor development delay can subsequently impair other neuropsychological domains of child functioning in African children with HIV (Abubakar et al. 2008a).
All of the factors discussed above can be considered integral parts of the coping and stress model and consistent with Li (2003) co-constructivist framework. This is because this paradigmatic framework emphasizes the dynamic roles of the child, the caregiver, and the overall environment in contributing to the psychosocial well-being of children with HIV/AIDS.
5.3 Analyzing the Stress and Coping Model of Psychosocial Well-Being in HIV Children
The model for stress and coping developed by Bachanas and colleagues (2001) was used to guide the collection of data and develop research questions for a model study of the psychosocial functioning of preschool-age children with HIV in a Ugandan rural setting. A model of this approach and the measures used is presented in Fig. 5.1. In order to understand the factors related to the psychosocial well-being of preschool children in Uganda with HIV/AIDS, following research questions were addressed:

Summary model of child adjustment. The strongest relationships exist on the left-hand side of the figure between caregiver emotional well-being (HSCL measures of depression/anxiety) and child psychosocial adjustment (CBCL global scales). HOME caregiving quality scores are related to caregiver depression/anxiety. The child’s psychosocial adjustment is related to the overall cognitive ability of the child as measured by the Mullen composite score. HIV illness parameters as indicated by HAART treatment status and weight-for-age physical growth are predictive both of HOME quality provided by the caregiver and of the child’s overall cognitive ability and development
-
1.
What health and demographic factors are important to the caregiving environment?
-
2.
What health and demographic factors are important to the cognitive development of young children with HIV/AIDS in Uganda?
-
3.
What health and demographic factors are related to caregiver adjustment (depression and anxiety)?
-
4.
Which variables (home environment, cognitive development, caregiver adjustment) are important to the psychosocial outcomes (internalizing, externalizing, and total behavior problems) of young Ugandan children with HIV/AIDS?
This study considers many mediating factors, including health variables, demographic variables, home environment variables, caregiver variables, and child factors within a single model. The relationship between these variables is organized using Bachanas and colleagues’ 2001 model of stress and coping, which fits with the cross-level dynamic biocultural co-constructivist paradigm discussed by Li (2003).
5.3.1 Methods
Baseline data from a longitudinal study of the effectiveness of a caregiver training of HIV-infected mothers in a rural Ugandan setting is used to provide a snapshot of the psychosocial well-being of preschool-age Ugandan children. In Uganda it is mandatory for pregnant women receiving care through a Ministry of Health facility to be tested for HIV/AIDS. Children were included in the study if they were between 1 and 5 years of age and not yet attending school. Their parent gave written consent to being in the study through all appropriated institutional and local approvals. If there was more than one child of the appropriate age in the household, they were all included. Children and families were excluded from the study if the child had a medical history of serious birth complications, severe malnutrition, bacterial meningitis, encephalitis, cerebral malaria, or other known brain injury or disorder requiring hospitalization or continued evidence of seizure or other neurological disability. Caregivers were also assessed for mental illness or disability to ensure that they could participate in the study.
All of the study measures were collected as baseline assessments as caregiver/child dyads were enrolled in the study. The one exception was a questionnaire evaluation of anxiety/depression of the caregiver, collected 6 months after the other baseline assessments occurred.
5.3.2 Participating Child/Caregiver Dyads
Participants included 119 children ages 1–5 years and their primary caregiver. The average age was 3½ years with a standard deviation of 1.3. Sixty-five of the participants were male (54.6 %) and 54 were female (45.4 %). Children in the study were mostly cared for by their biological mother (59.7 %). Grandmothers cared for 32 of the children (26.9 %), and 16 children (13.4 %) were being cared for by a stepmother, father, aunt, or uncle. Eighty of the children (68 %) are not on antiretroviral medication at the time of assessment, and 38 (32 %) were on Trimune highly active antiretroviral therapy (HAART).
5.3.3 Measures Used in the Present Model Analyses
The Caldwell Home Observation for the Measurement of the Environment (HOME) scale was developed to provide specific information about the home and caregiving environment as a stimulus to the learning and development of young children (Caldwell and Bradley 1979). It has been validated for use within the Ugandan context (Bangirana et al. 2009a). Through both caregiver report and direct observations, this measure characterizes the developmental milieu and caregiving style within the child’s home.
The Mullen scales of Early Learning were used to assess different developmental domains of children from birth to 68 months of age (Mullen 1995). The scales include Gross Motor (up to 36 months only), Visual Reception, Fine Motor, Receptive Language, and Expressive Language. The four Mullen scales with a cognitive performance component (Fine Motor, Visual Reception, Receptive Language, and Expressive Language) were used to derive the Early Learning Composite (g), which is a general measure of fluid intelligence in early childhood. The Early Learning Composite has been found be highly correlated with the Bayley Mental Development Index (r = 0.70), in validation studies (Mullen 1995).
The Achenbach Child Behavior Checklist (CBCL) for preschool-age children is used to obtain caregiver’s reports of their 1½–5 year-old child’s competencies and behavior problems. Ratings by a parent are completed on 99 problem items, which combine to make the following scales: Emotionally Reactive, Anxious/Depressed, Somatic Complaints, Withdrawn, Attention Problems, Aggressive Behavior, and Sleep Problems. These scales are then used to derive composite scores for internalizing (emotional), externalizing (behavior towards others), and total behavior problems.
The CBCL has been widely used throughout child and adolescent psychiatry and pediatrics (Achenbach et al. 2008; Achenbach and Rescorla 2001) and has been adapted to the Ugandan context (Bangirana et al. 2009b). The scale is administered to the primary caregiver in an interview format. During the interview the items are read in the local language of Luganda by a study team member, and the caregiver indicates the extent to which the child displays the behavior.
Standardized-for-age Z scores (WAZ) was used as a measure of nutritional well-being and overall physical health as it relates to pediatric HIV African children (Abubakar et al. 2009). The Hopkins Symptom Checklist (HSCL) is a 25-item scale to assess the emotional well-being of adults (15 depression items and 10 anxiety items). This scale has previously been utilized to assess the emotional well-being of Ugandan adults in HIV-affected communities (Bass et al. 2006; Derogatis et al. 1974a, b) and in other studies of adult depression in sub-Saharan Africa (Bolton et al. 2003, 2004), yielding scores for the severity of caregiver depression and anxiety. The child’s relationship to the primary caregiver was classified into three categories that naturally arise in the population: mother, grandmother, and others (made up of stepmothers, aunts, fathers, or uncles).
For all children in the study, the stage of HIV infection was monitored through multiple means. The highly active antiretroviral treatment (HAART) status of the child was measured, and a 5 ml blood draw was used to obtain CD4+ T-cell counts and viral load.
5.4 Statistical Evaluation of the Ugandan HIV Early Childhood Assessments Within the Bachanas et al. Model
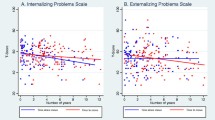
Using a Mann–Whitney statistical comparison of independent samples, there were no statistically significant differences between boys and girls for the CBCL domain scores (internalizing, externalizing, or total behavior problems). When looking at the number of children within the sample that were considered in the borderline and clinical range according to the CBCL cross-cultural norms (Achenbach 2010), about half of the sample was experiencing some internalizing behavior concerns. Specifically, 66 (55.5 %) of children were in the normal range for internalizing behaviors, while 22 (18.5 %) were in the borderline rage, and 31 (26.1 %) were in the clinical range.
For externalizing behaviors only 13 children were in the borderline (11) or clinical (2) range. For total behavior concerns, 80 (67.2 %) were in the normal range, with 19 (16 %) in the borderline range, and 20 (16.8 %) in the clinical range. There were no significant differences between boys and girls in the clinical or borderline range for internalizing, externalizing, or total behavior concerns.
Neither caregiver anxiety nor depression scores significantly differed among the principal caregiver groups (biological mother, grandmother, others). Likewise, there were no significant differences in HOME scores among the three caregiver groups.
5.4.1 Predicting Caregiving Environment
When only health predictors are considered, the child’s HIV viral load level is a significant predictor of HOME quality using a linear regression model. SES as measured by material possessions in the household was significantly predictive of HOME quality for our study children, with a linear regression model (P < 0.01).
5.4.2 Predicting Cognitive Development
HAART treatment status was significantly related to poorer performance on the composite Mullen score (overall cognitive ability) after adjusting for WAZ, gender, and HOME (analysis of covariance model—ANCOVA). This meant that clinically less stable children with HIV necessitating HAART were also at risk in terms of cognitive ability. Higher viral load level in children not on HAART was also significantly predictive of lower cognitive performance on the Mullen scales. Consistent with Abubakar et al. (2009), lower standardized weight for age was highly predictive of poorer performance on the Mullen composite cognitive performance and on gross motor development. Viral load and HAART treatment status were also significantly predictive of gross motor development and an ANCOVA model. Detailed statistical results from these analyses can be found in Table 5.1.
5.4.3 Predictors of Caregiver Adjustment Within the Present Model
The impact of health and demographic variables were considered separately for both caregiver anxiety and caregiver depression. In separate stand-alone linear regression analyses, less clinical stability for the child as indicated by HAART therapy and higher viral loads were predictive of higher depression and anxiety in the caregivers.
5.4.4 Predicting Psychosocial Outcomes Within the Present Model
To understand which of the ecological variables are important to psychosocial outcomes, internalizing, externalizing, and total behavior problems were considered separately. Caregiver depression, anxiety, and HOME quality of caregiving scores were significantly predictive of CBCL internalizing and total symptoms for the children (Table 5.2).
5.5 Summary of Bachanas Model Fit Within Present Study Sample
Figure 5.1 presents a schematic overview of the principal significant statistical relationships relevant to the Bachanas et al. model, as summarized in the previous sections and as detailed in Tables 5.1 and 5.2. The strongest relationships exist on the left-hand side of the figure between caregiver emotional well-being (HSCL measures of depression/anxiety) and child psychosocial adjustment (CBCL global scales). HOME caregiving quality scores are related to caregiver depression/anxiety. The child’s psychosocial adjustment is related to the overall cognitive ability of the child as measured by the Mullen composite score. HIV illness parameters as indicated by HAART treatment status and weight-for-age physical growth are predictive both of HOME quality provided by the caregiver and of the child’s overall cognitive ability and development.
5.6 Health and Demographic Predictors of Cognitive Development
Children with HIV are at increased risk for developmental disabilities (Speigel and Bonwit 2002), consistent with the data presented in this chapter that demonstrated that specific health and demographic variables (i.e., poorer clinical stability as indicated by lower weight for age and need for HAART) impacted children’s overall cognitive development and ability. A linkage between medication status, as a surrogate for progression of HIV/AIDS, and lowered developmental cognitive scores also would be expected, as children are not put on medication until their illness reaches a significant level (i.e., elevated viral load and CD4 count, as well as an AIDS-defining illness). Thus, it makes sense that with increased symptoms from more aggressive disease course, represented by the need for HAART, would come decreased cognitive scores, as was found in this sample of Ugandan children with HIV/AIDS. This is consistent with the findings of Smith and colleagues (2006) who reported significantly lower cognitive development scores for children ages 3–7 years with HIV/AIDS and exhibiting an AIDS-defining illness.
Similarly, weight for age as a measure of physical health and development was significantly predictive of Mullen gross motor and cognitive developmental outcomes for our study children. WAZ has also been linked to psychomotor outcomes for HIV-infected children in Kenya, with healthier children exhibiting higher psychomotor skills (Abubakar et al. 2009).
5.6.1 Psychosocial Outcomes for Young Ugandan Children with HIV/AIDS
The psychosocial child outcome variables chosen for the study presented in this chapter were internalizing, externalizing, and total behavior concerns from the CBCL. Not surprisingly, the caregiving environment played a role in both internalizing behaviors and externalizing behaviors exhibited by the young Ugandan children with HIV/AIDS. Specifically, children’s internalizing behavior concerns were influenced by the caregiver’s anxiety, depression, and the quality of the interactions within the home environment. The total behavior concerns exhibited by the study population were related to the caregiver’s depressive symptoms and the caregiving environment, but were also influenced by the socioeconomic status of the family. These findings are consistent with other research carried out in South Africa, a country strongly affected by the HIV/AIDS epidemic. In this setting, caregiving quality, perhaps as mediated by strength of caregiver/child attachment, has been identified as a key factor in the psychosocial adjustment of children. If children have quality care, they are more likely to exhibit social and behavioral adjustment, as well as intellectual achievement (Richter et al. 2004).
There were no significant predictors for externalizing behavior concerns in this study. On the other hand, there were few children reported by their caregivers to exhibit externalizing behavior concerns, restricting the range of responses and reducing the power to obtain significant findings. Children are reported to exhibit significantly more internalizing behaviors than externalizing ones. However, it also may be the case that caregivers are more concerned about the internalizing behaviors and do not feel that externalizing behaviors present as significant a problem to the family. This suggests that researchers may be better served to focus interventions for children with HIV/AIDS and their caregivers on anxious and depressive symptoms and not be as concerned with aggressive or externalizing behaviors.
5.7 Conclusion: Bachanas et al. Model Within a Co-constructivist Paradigm
Given the psychosocial, motor, and cognitive development delays faced by a significant proportion of our present sample of rural Ugandan HIV study children, it is imperative to understand the ecological factors contributing to the psychosocial adjustment of these children. The Bachanas et al. model provides a useful framework for doing so, and our study findings were consistent with this overall model. Such a framework also provides a vantage point for identifying strategic points of intervention for these at-risk children.
The results from this study show a dynamic relationship between demographic variables, health variables, caregiving variables, and child psychosocial development (see Fig. 5.2). This can be used for identifying interventions. For example, both internalizing behavior concerns and total behavior concerns are influenced by the caregiving environment or the quality of the home environment as measured by the quality of interactions between the caregiver and the child. Children’s internalizing behaviors also were influenced by the caregiver’s anxiety and depression. Boivin and colleagues are presently in the first year of an NIH-sponsored randomized controlled clinical trial (RCT) of the effects of a year-long caregiver training intervention for caregivers of rural Ugandan children with HIV and caregivers of children uninfected but born to infected mothers. This study will evaluate the impact training to improve caregiving in the home, on quality of caregiving, emotional well-being of the caregiver and child dyad, and subsequent developmental outcomes for the child. The present model indicates that caregiver training may be the single most strategic point of intervention for these outcomes (Fig. 5.1).

Outcomes: ecological model of factors contributing to psychosocial development of young children with HIV/AIDS
This model approach is also consistent with the biocultural co-constructivist framework described by Li (2003). Like this framework these results emphasize the dynamic interplay between the child and his/her environment in psychosocial development.
References
Abubakar, A., Holding, P., Newton, C. R. J. C., Van Baar, A., & Van De Vijver, F. J. R. (2009). The role of weight for age and disease stage in poor psychomotor outcome of HIV-infected children in Kilifi, Kenya. Developmental Medicine and Child Neurology, 51, 968–973.
Abubakar, A., Van Baar, A., Van de Vijver, F. J. R., Holding, P., & Newton, C. R. J. C. (2008a). Paediatric HIV and neurodevelopment in sub-Saharan Africa: A systematic review. Tropical Medicine & International Health, 13, 880–887.
Abubakar, A., Van de Vijver, F., Van Bar, A., Mbonani, L., Kalu, R., Newton, C., et al. (2008b). Socioeconomic status, anthropometric status, and psychomotor development of Kenyan children from resource-limited settings: A path-analytic study. Early Human Development, 84, 613–621.
Achenbach, T. M. (2010). The multicultural supplement to the manual for the ASEBA preschool forms and profiles. Burlington, VT: ASEBA Corporation.
Achenbach, T. M., Becher, A., Dopfner, M., Heiervang, E., Roessner, V., Steinhausen, H. C., et al. (2008). Multicultural assessment of child and adolescent psychopathology with ASEBA and SDQ instruments: Research findings, applications, and future directions. Journal of Child Psychology and Psychiatry, 49, 251–275.
Achenbach, T. M., & Rescorla, L. A. (2001). Manual for the ASEBA school-age forms and profiles. Burlington, VT: University of Vermont, Research Center for Children, Youth, and Families.
Armstrong, F. D., Seidel, J. F., & Swales, T. P. (1993). Pediatric HIV infection: A neuropsychological and educational challenge. Journal of Learning Disabilities, 26, 92–103.
Atwine, B., Cantor-Graae, E., & Bajunirwe, F. (2005). Psychological distress among AIDS orphans in rural Uganda. Social Science & Medicine, 61, 555–564.
Bachanas, P. J., Kullgren, K. A., Suzman Schwarz, K., Lanier, B., McDaniel, S., Smith, J., et al. (2001). Predictors of psychological adjustment in school-age children infected with HIV. Journal of Pediatric Psychology, 26, 343–352.
Bangirana, P., Musisi, S., Allebeck, P., Giordani, B., John, C. C., Opoka, R. O., et al. (2009a). A preliminary examination of the construct validity of the KABC-II in Ugandan children with a history of cerebral malaria. African Health Sciences, 19, 186–192.
Bangirana, P., Nakasujja, N., Giordani, B., Opoda, R. O., John, C. C., & Boivin, M. J. (2009b). Reliability of the Luganda version of the child behaviour checklist in measuring behavioural problems after cerebral malaria. Child and Adolescent Psychiatry and Mental Health, 3, 38.
Bass, J., Neugebauer, R., Clougherty, K. F., Verdeli, H., Wickramaratne, P., Ndogoni, L., et al. (2006). Group interpersonal psychotherapy for depression in rural Uganda: 6-month outcome: Randomized controlled trial. The British Journal of Psychiatry, 188, 567–573.
Bateganya, F. H., Kyomuhendo, S., Jagwe-Wadda, G., & Opesen, C. C. (2008). Male involvement in Uganda: Challenges and opportunities. In M. L. Foller & H. Thorn (Eds.), The politics of AIDS: Globalization, the state and civil society (pp. 123–138). New York: Palgrave Macmillan.
Bikaako-Kajura, W., Luyirika, E., Purcell, D. W., Downing, J., Kaharuza, F., Mermin, J., et al. (2006). Disclosure of HIV status and adherence to daily drug regimens among HIV infected children in Uganda. AIDS and Behavior, 10, s85–s93.
Boivin, M. J., & Giordani, B. (2009). Neuropsychological assessment of African children: Evidence for a universal brain/behavior omnibus within a coconstructivist paradigm. Progress in Brain Research, 178, 113–135.
Bolton, P., Bass, J., Neugebauer, R., Verdeli, H., Clougherty, K. F., Wickramaratne, P., et al. (2003). Group interpersonal psychotherapy for depression in rural Uganda: A randomized controlled trial. Journal of the American Medical Association, 289, 3117–3124.
Bolton, P., Wilk, C. M., & Ndogoni, L. (2004). Assessment of depression prevalence in rural Uganda using symptom and function criteria. Social Psychiatry and Psychiatric Epidemiology, 39, 442–447.
Brown, L. K., Lourie, K. J., & Pao, M. (2000). Children and adolescents living with HIV and AIDS: A review. Journal of Child Psychology and Psychiatry, 41, 81–96.
Caldwell, B. M., & Bradley, R. H. (1979). Home observation for measurement of the environment. Little Rock, AR: University of Arkansas Press.
Carter, S. L., Rourke, S. B., Murji, S., Shore, D., & Rourke, B. P. (2003). Cognitive complaints, depression, medical symptoms, and their association with neuropsychological functioning in HIV infection: A structural equation model analysis. Neuropsychology, 17, 410–419.
Chandra, P. S., Satyanarayana, V. A., Satishchandra, P., Satish, K. S., & Kumar, M. (2009). Do men and women with HIV differ in their quality of life? A study from South India. AIDS and Behavior, 13, 110–117.
Compas, B. E., Banez, G. A., Malcarne, V., & Worsham, N. (1991). Perceived control and coping with stress: A developmental perspective. Journal of Social Issues, 47, 23–34.
Cook, J., Cohen, M., Burke, J., Grey, D., Anastos, K., Kirstein, L., et al. (2002). Effects of depressive symptoms and mental health quality of life on use of highly active antiviral therapy among HIV-seropositive women. Journal of Acquired Immune Deficiency Syndromes, 30, 401–409.
Cook, P., & Toit, L. D. (2005). Overcoming adversity with children affected by HIV/AIDS in the indigenous south African cultural context. In M. Ungar (Ed.), Handbook for working with children and youth: Pathways to resilience across cultures and contexts (pp. 247–262). Thousand Oaks, CA: Sage.
Cysique, L. A., Jin, H., Franklin, J., Morgan, E. E., Shi, C., Yu, X., et al. (2007). Neurobehavioral effects of HIV-1 infection in China and the United States: A pilot study. Journal of the International Neuropsychological Society, 13, 781–790.
Dawes, A., Bray, R., VanDerMerwe, R. B., & VanDerMerwe, A. (Eds.). (2007). Monitoring child well-being: A South African rights-based approach. Cape Town: HSRC Press.
Derogatis, L. R., Lipman, R. S., Rickels, K., Uhlenhuth, E. H., & Covi, L. (1974a). The Hopkins Symptom Checklist (HSCL): A measure of primary symptom dimensions. Modern Problems of Pharmacopsychiatry, 7, 79–110.
Derogatis, L. R., Lipman, R. S., Rickels, K., Uhlenhuth, E. H., & Covi, L. (1974b). The Hopkins Symptom Checklist (HSCL): A self-report symptom inventory. Behavioral Science, 19, 1–15.
Engel, R. G., & Melamed, B. G. (2002). Stress and coping in children at risk for medical problems. In L. L. Hayman, M. M. Mahon, & J. R. Turner (Eds.), Chronic illness in children: An evidence-based approach (pp. 171–198). New York: Springer.
Franklin, S., Lim, H. J., & Havens, P. L. (2007). Longitudinal behavioral and academic adjustment in children with HIV infection. Journal of Clinical Psychology in Medical Settings, 14, 335–343.
Hochhauser, C. J., Gaur, S., Marone, R., & Lewis, M. (2008). The impact of environmental risk factors on HIV-associated cognitive decline in children. AIDS Care, 20, 692–699.
Hodge, M. (2008). HIV/AIDS, demographics and economic development. In E. M. Omwami, S. Commins, & E. J. Keller (Eds.), HIV/AIDS in Africa: Challenges and impact (pp. 7–26). Trenton, NJ: Africa World Press.
Imam, I. (2007). Neurological manifestation of HIV infection in Nigerians. African Journal of AIDS Research, 6, 187–192.
Jones, S. A., Sherman, G. G., & Varga, C. A. (2005). Exploring socio-economic conditions and poor follow-up rates of HIV-exposed infants in Johannesburg, South Africa. AIDS Care, 17, 466–470.
Junqueira, P., Bellucci, S., Rossini, S., & Reimao, R. (2008). Women living with HIV/AIDS: Sleep impairment, anxiety and depression symptoms. Arquivos de Neuro-Psiquiatria, 66, 817–820.
Knight, W. G., Mellins, C. A., Levenson, R. L., Jr., Arpadi, S. M., & Kairam, R. (2000). Brief report: Effects of pediatric HIV infection on mental and psychomotor development. Journal of Pediatric Psychology, 25, 583–587.
Landau, S., & Pryor, J. B. (1995). Pediatric HIV: School-based sequelae and curricular interventions for infection prevention and social acceptance. School Psychology Review, 24, 213–230.
Li, S. (2003). Biocultural orchestration of developmental plasticity across levels: The interplay of biology and culture in shaping the mind and behavior across the life span. Psychological Bulletin, 129, 171–194.
Liebenberg, L., & Ungar, M. (Eds.). (2008). Resilience in action: Working with youth across cultures and contexts. Toronto, ON: University of Toronto Press.
Masten, A. (2006). Developmental psychopathology: Pathways to the future. International Journal of Behavioral Development, 30, 47–54.
Mellins, C. A., Smith, R., O’Driscoll, P., Lawrence, M. S., Brouwers, P., Chase, C., et al. (2003). High rates of behavioral problems in perinatally HIV-infected children are not linked to HIV disease. Pediatrics, 111, 384–393.
Mrus, J. M., Williams, P. L., Tsevat, J., Cohen, S. E., & Wu, A. W. (2005). Gender differences in health-related quality of life in patients with HIV/AIDS. Quality of Life Research, 14, 479–491.
Mullen, E. M. (1995). Mullen scales of early learning (AGSth ed.). Circle Pines, MN: American Guidance Services.
Nyesigomwe, L. (2006). Strengthening the capacity of grandparents in providing care to young children affected by HIV/AIDS. Journal of Intergenerational Relationships, 4, 55–63.
Owens, E. B., & Shaw, D. S. (2003). Poverty and early childhood adjustment. In S. S. Luthar (Ed.), Resilience and vulnerability: Adaptation in the context of childhood adversities (pp. 267–292). New York: Cambridge University Press.
Papola, P., Alvarez, M., & Cohen, H. J. (1994). Developmental and service needs of school-age children with human immunodeficiency virus infection: A descriptive study. Pediatrics, 94, 914–918.
Pelton, J., & Forehand, R. (2005). Orphans of the AIDS epidemic: An examination of clinical level problems in children. Journal of the American Academy of Child and Adolescent Psychiatry, 44, 585–591.
Richter, L. M., Manegold, J., & Pather, R. (2004). Family and community interventions for children affected by AIDS. Cape Town: HSRC Press.
Ronald, A. R., & Sande, M. A. (2005). HIV/AIDS care in Africa today. Clinical Infectious Disease, 40, 1045–1048.
Rouet, G., Sakarovitch, C., Msellati, P., Elenga, N., Montcho, C., Viho, I., et al. (2003). Pediatric viral human immunodeficiency virus type 1 RNA levels, timing of infection, and disease progression in children. Pediatrics, 112, e289–e297.
Smith, R., Malee, K., Leighty, R., Brouwers, P., Mellins, C., Hittelman, J., et al. (2006). Effects of perinatal HIV infection and associated risk factors on cognitive development among young children. Pediatrics, 117, 851–862.
Smith, R. A., & Rimal, R. (2009). The impact of social capital on HIV-related actions as mediated by personal and proxy efficacies in Namibia. AIDS and Behavior, 13, 133–144.
Speigel, H. M. L., & Bonwit, A. M. (2002). HIV infection in children. In M. Batshaw (Ed.), Children with disabilities (5th ed., pp. 123–139). Baltimore: Brookes.
U.S. Department of Health and Human Services. (1999). Mental health: A report of the surgeon general. Rockville, MD: Author.
UNICEF. (2008). Children and HIV/AIDS. Retrieved April 26, 2008, from http://www.unicef.org/aids/
Wachsler-Felder, J. L., & Golden, C. J. (2002). Neuropsychological consequences of HIV in children. A review of current literature. Clinical Psychology Review, 22, 441–462.
Wertlieb, D., Weigel, C., & Feldstein, M. (1987). Measuring children’s coping. The American Journal of Orthopsychiatry, 57, 548–560.
Wiener, L. S., Battles, H. B., & Heilman, N. (2000). Public disclosure of a child’s HIV infection: Impact on children and families. AIDS Patient Care and STDs, 14, 485–497.
Woodrich, D. L., Swerdlik, M. E., Chenneville, T., & Landau, S. (1999). HIV/AIDS among children and adolescents: Implications for the changing roles of school psychologists. School Psychology Review, 28, 228–241.
Zickler, P. (2009). When the body suffers, the mind suffers. Monitor on Psychology, 40, 31–34.
Acknowledgements
The work and examples in this chapter were supported in part by grant R34MH082663 (PI: Boivin) from NIMH.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2013 Springer Science+Business Media New York
About this chapter
Cite this chapter
Busman, R.A., Page, C., Oka, E., Giordani, B., Boivin, M.J. (2013). Factors Contributing to the Psychosocial Adjustment of Ugandan Preschool Children with HIV/AIDS. In: Boivin, M., Giordani, B. (eds) Neuropsychology of Children in Africa. Specialty Topics in Pediatric Neuropsychology. Springer, New York, NY. https://doi.org/10.1007/978-1-4614-6834-9_5
Download citation
DOI: https://doi.org/10.1007/978-1-4614-6834-9_5
Published:
Publisher Name: Springer, New York, NY
Print ISBN: 978-1-4614-6833-2
Online ISBN: 978-1-4614-6834-9
eBook Packages: Behavioral ScienceBehavioral Science and Psychology (R0)