
Abstract
Spermatozoa can be retrieved from either the epididymis or the testis, depending on the type of azoospermia, using different surgical methods such as PESA, TESA, TESE, and micro-TESE. After collecting the epididymal fluid or testicular tissue, laboratory techniques are used to remove contaminants, cellular debris, noxious microorganisms, and red blood cells. Processed spermatozoa may be used for intracytoplasmic sperm injection or eventually be cryopreserved. However, spermatozoa collected from either the epididymis or the testis are often compromised and more fragile than ejaculated ones. Therefore, sperm processing techniques should be used with great caution to avoid jeopardizing the sperm fertilizing potential in treatment cycles. In this chapter, we describe methods for the optimal processing of surgically retrieved specimens, either fresh or frozen–thawed. We also provide tools to aid in the identification of viable immotile spermatozoa for ICSI. The clinical outcomes of ICSI using testicular and epididymal sperm in azoospermic men are presented, and the tips and pitfalls of sperm processing techniques for surgically retrieved specimens are critically discussed.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others



Keywords
- PESA/TESA/TESE sperm processing
- Sperm processing with PESA/TESA/TESE
- ICSI spermatozoa identification
- Epididymal sperm aspiration
- Sperm processing techniques
- Intracytoplasmic sperm injection
- Azoospermia
- Epididymal spermatozoa
- Testicular spermatozoa
Two major breakthroughs occurred in the area of male infertility only 2–3 years apart [1–3]. The first was the development of intracytoplasmic sperm injection (ICSI) for the treatment of male factor infertility due to severely abnormal semen quality [1]. The second was the extension of ICSI to azoospermic males and the demonstration that spermatozoa derived from either the epididymis or the testis were capable of normal fertilization and pregnancy [2, 3]. In the case of azoospermia, two totally different clinical situations exist, i.e., obstructive and nonobstructive azoospermia (NOA). In obstructive azoospermia (OA), spermatogenesis is normal, but a mechanical blockage exists in the genital tract, somewhere between the epididymis and the ejaculatory duct, or the epididymis and vas deferens are totally or partially absent. Causes of OA are acquired or congenital. Acquired OA may be due to vasectomy; failure of vasectomy reversal; postinfectious diseases; surgical procedures in the scrotal, inguinal, pelvic, or abdominal regions; and trauma. Congenital causes of OA include cystic fibrosis, congenital absence of the vas deferens (CAVD), ejaculatory duct or prostatic cysts, and Young’s syndrome [4]. NOA comprises a spectrum of testicular histopathology resulting from various causes that include environmental toxins, medications, genetic and congenital abnormalities, varicocele, trauma, endocrinologic disorders, and idiopathic. Sperm can be easily obtained from men with OA whereas individuals exhibiting NOA have historically been the infertile men most difficult to treat [4, 5].
Several sperm retrieval methods have been developed to collect epididymal and testicular sperm in azoospermic men. It is out of our scope to discuss which technique is best to surgically retrieve sperm. As a general rule, either percutaneous (PESA) [6] or microsurgical epididymal sperm aspiration (MESA) [2] can be successfully used to retrieve sperm from the epididymis in men with OA. Testicular sperm aspiration (TESA) can be used to retrieve sperm from the testes either in men with OA who fail PESA or in those with NOA [6, 7]. Testicular sperm extraction (TESE) using single or multiple open biopsies [8–10] and, more recently, microsurgery (micro-TESE) are indicated for men with NOA [11–13] (Table 24.1).
Processing of surgically retrieved spermatozoa differs from the commonly used methods for processing ejaculates. Sperm processing should not only ease the selection of the best quality spermatozoa for ICSI but also optimize their fertilizing ability, whenever possible. The laboratory has a crucial role in the handling of these often compromised specimens, particularly in the cases of NOA and after the freeze–thawing process. In order to achieve their goals, laboratory personnel should (1) receive the best quality surgically retrieved specimen possible, with minimal or no contaminants such as red blood cells and noxious microorganisms, (2) minimize the iatrogenic cellular damage during sperm processing by mastering technical skills and controlling several factors, including centrifugation force and duration, exposure to ultraviolet light and temperature variation, laboratory air quality conditions, dilution and washing steps, quality of reagents, culture media, and disposable materials, and (3) improve the sperm fertilizing potential, if possible, by using stimulants or selecting viable sperm for ICSI when only immotile spermatozoa is available. In this chapter, our aims are to provide a step-by-step laboratory description of the commonly used methods for PESA/TESA/TESE sperm processing and identification of viable immotile sperm for ICSI, as well as to present our group’s clinical results of ICSI using testicular and epididymal sperm. Finally, we critically discuss the tips and pitfalls of sperm processing techniques for surgically retrieved specimens.
Step-by-Step Protocol of the Laboratory Procedures
Materials, Equipments, Reagents, and IVF Laboratory Setup
Operating Room
-
Sterile surgical gloves and syringes (1, 20 mL).
-
0.7 × 25 (22 G), 0.45 × 13 (26 G), and 1.2 × 40-mm (18 G; for TESA/TESE only) disposable needles.
-
2% Lidocaine hydrochloride solution.
-
Heating block for test tubes (e.g.: Fisher, USA).
-
Syringe holder (for TESA only, see Fig. 24.1).
Fig. 24.2 
TESA sperm processing. Flow chart illustrates TESA steps from the surgical procedure to the processing of testicular specimens for ICSI
-
Operating microscope (e.g.: DF Vasconcelos, Brazil; for micro-TESE only).
-
Microsurgery instruments (e.g.: ASSI, USA; for micro-TESE only).

IVF Laboratory
-
50 × 09-mm (e.g.: #351006, Falcon, USA) and 60 × 15-mm single well Petri dishes (e.g.: cat.#353037, Falcon, USA; for TESA/TESE only).
-
Disposable serological pipettes (5.0 mL; e.g.: cat.#4051 Costar or cat.#356543 Falcon, USA).
-
Pipettor 1–200 μL (e.g.: Gilson, France) and sterile tips (cat.#4804, Corning, USA).
-
Pipetting device (e.g.: Pipette-aid, Drummond Scientific, USA).
-
6-mL sterile centrifuge polystyrene tubes with caps (e.g.: cat.#352003, Falcon, USA).
-
0.7 × 25-mm needles and tuberculin syringes (e.g.: BD, USA; for TESA/TESE only).
-
Fine point permanent marker pen (e.g.: Sharpie, Sandford, USA).
-
Injection micropipettes (e.g.: cat.#MIC-50-35; Humagen, USA).
-
Laminar flow cabinet (e.g.: Veco, Brazil).
-
Warming plates (e.g.: Tokai-heat, Japan).
-
Stereomicroscope (e.g.: Leica GZ7, Switzerland).
-
Centrifuge (e.g.: model 225; Fisher Scientific, USA).
-
Inverted microscope (e.g.: Eclipse E400, Nikon, Japan) equipped with Hoffman modulation contrast and electrohydraulic micromanipulators (e.g.: Narishighe, Japan).
-
HEPES-buffered Human Tubal Fluid (e.g.: modified HTF culture medium, cat.#90126, Irvine Scientific, USA) and human serum albumin (e.g.: HSA, cat.#9988, Irvine Scientific, USA).
-
Mineral oil (e.g.: #9305, Irvine Scientific, USA).
-
PVP solution (e.g.: cat.#10111, Vitrolife, Sweden).
-
Colloidal density gradient (e.g.: Isolate®, cat.#99264, Irvine Scientific, USA).
Laboratory Setup
Note: Use sterile handling conditions under a laminar flow cabinet or clean room environment during all laboratory steps.
-
Prepare a 10 (for PESA) or 20 mL (TESA/TESE) HEPES-buffered protein-supplemented (5% HSA) sperm culture medium, and keep it at 37°C.
-
Transfer a 5 mL aliquot of the prepared sperm culture medium to a 6-mL polystyrene tube and send it to the operating room (sperm media is used to flush the aspirating system before aspiration and to incubate epididymal aspirates or testicular specimens upon collection).
-
Place two 50 × 09-mm Petri dishes on a warm surface (37°C) inside the laboratory workstation (for PESA only).
-
Prepare four 2-well dishes by transferring 0.5 and 1.0 mL sperm medium aliquots to the inner- and outer-dish wells, respectively (for TESA/TESE only). Place two of them onto a warm surface (37°C) inside the workstation, and send the others to the operating room (for TESE only).
-
Mount two tuberculin syringes connected with a 22-gauge needle (to be used as tools for mincing and squeezing seminiferous tubules in TESA/TESE processing).
PESA Sperm Processing
Surgical Technique
Note: PESA is performed under local anesthesia (at the spermatic cord level) in association with intravenous anaesthesia using propofol either at the day of oocyte retrieval or the day before.
-
A 10 mL solution of 2% lidocaine is injected around the spermatic cord near the external inguinal ring upon patient unconsciousness is achieved. The epididymis is stabilized between the index finger, thumb, and forefinger while the testis is held with the palm of the hand.
-
A 26-gauge needle attached to a 1-mL tuberculin syringe is inserted into the epididymis through the scrotal skin. Loupe-magnification is used to avoid injuring small vessels seen through the skin (Fig. 24.1).
Fig. 24.1 
PESA sperm processing. Flow chart illustrates PESA steps from the surgical procedure to the processing of epididymal aspirates for ICSI
-
Negative pressure is created, and the tip of the needle is gently moved in and out within the epididymis until fluid enters the syringe. The amount of epididymal fluid obtained during aspiration is often minimal (∼0.1 mL), except in cases of CAVD in which 0.3–1.0 mL may be aspirated.
-
The needle is withdrawn from the epididymis, and the aspirate is flushed into a 0.5–1.0 mL 37°C sperm medium.
-
The tube containing the epididymal aspirate is transferred to the IVF lab next door. PESA is repeated at a different site of the same epididymis (from cauda to caput) and/or at the contralateral one until adequate number of motile sperm is retrieved. If PESA fails to retrieve motile sperm for ICSI, TESA is performed at the same operative time (Fig. 24.1).

Sperm Processing
-
Homogenize epididymal aspirate and sperm medium to avoid sperm agglutination (epididymal spermatozoa tend to agglutinate fast). Keep aspirate-containing tubes capped at 37°C.
-
Place a 10–20 μL sperm suspension aliquot onto a Petri dish, and spread it as thin as possible using a micropipette tip. Examine the fluid under the inverted microscope (×400 magnification) to confirm the presence of motile sperm. Inform the surgeon promptly if an adequate number of motile sperm is available for ICSI. This step should take no more than 2–3 min to allow the surgeon to decide on continuing or finishing the surgical retrieval. If more PESA specimens are taken, pool samples of similar quality together for processing. If PESA fails and TESA specimens are obtained, process specimens according to the “TESA processing protocol” (see section “TESA Sperm Processing” and Fig. 24.2).
-
Upon finishing surgical retrieval, identify aspirate-containing tube(s) according to the epididymis side and site of aspiration, as well as to the presence of motile sperm. Make a decision upon the processing method to be used, i.e., simple washing or two-layer discontinuous mini-gradient centrifugation, based on a gross estimate of sperm density and motility. Use gradient centrifugation when the specimen contains high density of motile sperm, particularly if contaminated with red blood cells, cellular debris, and immotile sperm. Otherwise, use simple washing.
-
For density gradient centrifugation, layer an aliquot of the PESA aspirate up to 0.5 mL over 0.3 mL gradients of 45 and 90%, respectively, and centrifuge at 300 × g for 10 min. Resuspend the pellet in 1.5 mL fresh sperm medium and repeat centrifugation. Remove the supernatant carefully, leaving about 0.2 mL of medium above the pellet. Resuspend the pellet and keep at 37°C until use.
-
For simple washing, dilute epididymal aspirate with fresh sperm medium to a final volume of 1.5–2.0 mL. Centrifuge the mixture at 300 × g for 10 min, discharge the supernatant, and then resuspend the pellet in 0.2 mL of sperm medium. When a processed PESA sample is still contaminated with an excessive number of red blood cells, dilution and centrifugation with 2 mL erythrocyte lysis buffer may be required (see Table 24.2).
Table 24.2 Solutions for washing samples -
Prepare a Petri dish containing a series of microdrops under mineral oil for sperm pickup from a processed epididymal cell suspension (Fig. 24.3).
Fig. 24.3 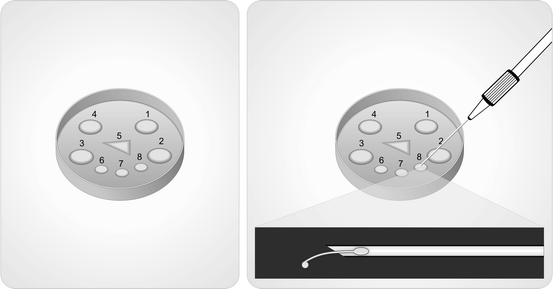
Preparation of microdroplets. A 50 × 09-mm Petri dish containing several microdroplets of culture medium under mineral oil is prepared for sperm pickup from a processed epididymal or testicular cell suspension. Microdroplets are prepared as follows: four 10 μL sperm medium at dish periphery to load specimens (numbered 1–4), one 4 μL polyvinylpyrrolidone (PVP) at dish center in a triangle shape to pick up selected sperm for ICSI (number 5), and two to three 10 μL sperm medium at dish center below the PVP triangle for washing (numbered 6–8). Alternatively, one of the sperm medium-containing microdroplets (e.g., number 8) or the peripheric ones (1–4) may be replaced with the hyposmotic or motility stimulant solutions, respectively (left). The hyposmotic swelling test is illustrated (right). The sperm tail is partially withdrawn from the injection micropipette into the HOS droplet. A swelling at the level of the tail tip may be seen under the inverted microscope with contrast at ×400 magnification
-
Load gently a 1 μL sperm suspension aliquot at the center of the polyvinylpyrrolidone (PVP) microdroplet if the suspension contains motile sperm with progressive motility. After 5–20 min incubation period, morphologically normal motile spermatozoa can be identified and picked up for ICSI with the injection micropipette under ×400 magnification at the edge of the PVP droplet. If progressive motility is low or absent and/or the sample is contaminated with cellular debris, load 1–4 μL sperm suspension aliquot at each 10 μL peripheral microdroplet of HEPES-buffered culture medium to facilitate search and selection of motile sperm. First, aspirate a small volume of PVP into the injection micropipette to improve control during sperm pickup and to avoid blowing air bubbles during ejection of selected sperm into the PVP droplet.
-
After finishing sperm pickup from the PESA-processed sample, wash the injection micropipette free of any debris in the PVP droplet.
-
Make a final morphologic sperm assessment under ×800 magnification in the group of preselected spermatozoa before ICSI. Immobilize, aspirate into the micropipette, and inject selected sperm into the cytoplasm of metaphase II oocytes.
-
Consider cryopreservation of leftover PESA-processed aspirates containing motile sperm that were not used for ICSI. Freezing can be carried out using the fast liquid nitrogen vapor method [14] (Fig. 24.1).

TESA Sperm Processing
Surgical Technique
Note: TESA is performed under local anesthesia, as described in the “PESA protocol,” in association with intravenous anaesthesia using propofol either at the day of oocyte retrieval or the day before.
-
After anesthetic blockade of the spermatic cord, the epididymis is stabilized between the index finger, thumb, and forefinger while the anterior scrotal skin is stretched.
-
A 18-gauge needle attached to a 20-mL syringe is connected to a syringe holder and is inserted through the stretched scrotal skin into the anteromedial or anterolateral portion of the superior testicular pole, in an oblique angle towards the medium and lower poles (Fig. 24.2). Loupe-magnification is used to avoid small vessels seen through the skin.
-
Negative pressure is created by pulling the syringe holder while the tip of the needle is moved in and out within the testis in an oblique plane to disrupt the seminiferous tubules and sample different areas. When a small piece of testicular tissue is aspirated, the needle is gently withdrawn from the testis while the negative pressure is maintained. A pair of microsurgery forceps is used to grab the seminiferous tubules that exteriorize from the scrotal skin, thus aiding in the removal of the specimen (see Fig. 24.2).
-
The specimen is flushed into a tube containing 0.5–1.0 mL warm sperm medium and is transferred to the IVF lab. TESA or TESE may be performed at the contralateral testis if insufficient number of sperm is retrieved for ICSI.
Sperm Processing
-
Discharge TESA aspirate to the outer-dish well. Under stereomicroscopy, identify seminiferous tubules and remove blood clots using the needled tuberculin syringes.
-
Transfer seminiferous tubules to the inner-dish well containing fresh sperm medium. Perform a mechanical dispersion of the tubules by mincing repeatedly using both needled tuberculin syringes (use one to hold tubules in place at the bottom of the dish and the other to squeeze and open them). Repeat this step until no intact tubules are seen (see Fig. 24.2).
-
Examine the homogenate to confirm the presence of sperm using the inverted microscope at ×400 magnification. Inform the surgeon promptly if an adequate number of sperm for ICSI is available. This step should take no more than 10 min because the patient is kept under anesthesia until a decision of continuing or finishing the surgical retrieval is made. If other TESA specimens are taken, carry out the initial processing steps described above. If TESE specimens are obtained, perform processing according to the “TESE sperm processing protocol” (see section “TESE Sperm Processing” and Fig. 24.4).
Fig. 24.4 
TESE sperm processing. Flow chart illustrates TESE steps from the surgical procedure using micro-TESE for the extraction of testicular parenchyma to the processing of testicular specimens for ICSI
-
Aspirate and transfer the cell suspension from the inner-well dish to a sterile centrifuge tube. Dilute the aspirate with 3 mL of fresh sperm medium and wash it at 300 × g for 7 min. Discharge the supernatant and resuspend the pellet in 0.2 mL of sperm medium. When a processed TESA specimen is still contaminated with an excessive number of red blood cells, dilution and centrifugation with erythrocyte lysis buffer may be required (see Table 24.2).
-
Prepare a Petri dish as described in the “PESA protocol” for sperm pickup from a processed testicular cell suspension (see Fig. 24.3).
-
Load 1–2 μL sperm suspension aliquot at each 10 μL peripheral microdroplet of HEPES-buffered culture medium to facilitate sperm search and pickup. Proceed to sperm selection and ICSI, as described in the “PESA protocol,” and consider cryopreservation of leftover testicular aspirates. Dishes with microdroplets containing TESA-processed sperm can be incubated up to 48 h before ICSI at room temperature in an attempt to improve testicular sperm motility.

TESE Sperm Processing
Micro-TESE Surgical Technique
Note: TESE is performed under local anesthesia, as described in the “PESA protocol,” in association with intravenous anaesthesia using propofol either at the day of oocyte retrieval or the day before. For micro-TESE, operating microscope and microsurgery technique are used throughout the procedure, as previously described [5, 11] (Fig. 24.4).
-
After anesthetic blockade of spermatic cord, the anterior scrotal skin is stretched and the skin and tunica vaginalis are infiltrated with 2 mL of 2% lidocaine. A transverse 2-cm incision is made through the anesthetized layers, and the testis is exteriorized.
-
A single, large, midportion incision is made in an avascular area of the tunica albuginea under 6–8× magnification, and the testicular parenchyma is widely exposed.
-
Dissection of the testicular parenchyma is carried out at ×16–25 magnification searching for enlarged seminiferous tubules (more likely to contain germ cells and eventually normal sperm production). The superficial and deep testicular regions may be examined, if necessary, and microsurgical-guided testicular biopsies are performed by removing enlarged tubules (Fig. 24.4). If enlarged tubules are not seen, then any tubule different than the remaining ones in size is excised [11]. If all tubules are identical in appearance, random microbiopsies (at least three at each testicular pole) are performed.
-
Each excised testicular tissue specimen is placed at the outer-well dish containing sperm media. Specimens are washed grossly to remove blood clots and are sent to the IVF laboratory for processing.
Sperm Processing
-
Transfer TESE fragments from the operating room dishes to the outer-well of a new dish in the IVF lab. Under stereomicroscopy, remove blood clots using the needled tuberculin syringes. Transfer fragments to the inner-well dish containing fresh medium and wash again until no blood clots are seen. Repeat these steps using new dishes if necessary, and make sure to start the mincing steps only when erythrocyte contamination is minimum (TESE fragments tend to be contaminated with excessive red blood cells).
-
Perform mechanical dispersion of the tubules, and follow the steps described in the “TESA protocol” (Fig. 24.4). Two laboratory technicians/embryologists should work together to speed up the sperm searching process (one mincing the tubules under the stereomicroscope and the other searching for spermatozoa under the inverted microscope). Inform the surgeon promptly if any sperm is found to allow him to decide upon continuing testicular microdissection or moving to the contralateral testis. If other TESE specimens are taken, carry out the initial processing steps described above.
Cryo-Thawed Epididymal/Testicular Sperm Processing
Epididymal and testicular spermatozoa may be cryopreserved using protocols routinely used for ejaculated sperm [15, 16]. After thawing, removal of cryoprotectant is carried out by simple washing, as described in the “TESA sperm processing protocol.” If only immotile spermatozoa are seen, a method for selecting viable sperm for ICSI may be used.
Methods for Selecting Viable Immotile Sperm for ICSI
It has been observed that conventional seminal parameters have little or no influence in ICSI outcomes, except when only immotile spermatozoa are available [17, 18]. In certain cases, only immotile spermatozoa are obtained after fresh or cryo-thawed PESA/TESA/TESE processing. Different strategies are described to differentiate live immotile spermatozoa from dead ones, thus aiding in the selection of viable gametes for ICSI.
Hyposmotic Swelling Test (HOST) [19–21]
-
Using the microinjection pipette, pick up morphologically normal immotile spermatozoa from the sperm medium droplet and transfer to PVP.
-
Aspirate a single spermatozoon head-first into the pipette.
-
Move the pipette to the hyposmotic solution (HOS) microdrop (see Fig. 24.3 and Table 24.2), and release only the sperm tail into the HOS solution. Keep it for 5–10 s and observe if a tail tip swelling occurs (sperm tail swelling is often minimal and is a marker of viability in fresh specimens, but may not be suitable for testing cryopreserved ones [21]).
-
If tail swelling is seen, aspirate the cell back to the pipette and release it in a drop of fresh medium to allow osmotic re-equilibration (tail swelling often disappears in 5–20 s). If tail swelling is not seen, discharge spermatozoon into the HOS solution.
-
Transfer the viable selected spermatozoon to the PVP drop. Repeat these steps until sufficient number of viable sperm is selected for ICSI.
Sperm Tail Flexibility Test (STFT) [22, 23]
-
Using the microinjection pipette, pick up morphologically normal immotile spermatozoa from sperm microdroplet (see Fig. 24.3) and transfer to PVP solution.
-
Align spermatozoa near the PVP droplet edge.
-
Touch sperm tail with the tip of the microinjection pipette, and force the tail to move up and down. Tail is considered flexible when it moves independently of the sperm head (sperm tail flexibility is considered a marker of sperm viability [22, 23]). If tail remains rigid upon touching and sperm head and tail move together as a unit, the spermatozoon is then considered nonviable for ICSI.
-
Repeat these steps until sufficient number of viable sperm is selected for ICSI.
Motility Stimulant Sperm Challenge (MSC) [24–26]
Note: Example given using a 5-mM pentoxifylline (PF) solution (see Table 24.2).
-
Load a 4 μL aliquot of fresh or cryopreserved PESA/TESA/TESE sperm suspension into the motility stimulant solution microdroplet, and incubate for 20 min (see Fig. 24.3).
-
Examine the specimen microscopically searching for moving sperm. In cases of positive MSC, slight noticeable tail twitching is often seen (in rare occasions, vigorous twisting may be observed).
-
Pick up motile sperm using the microinjection pipette, and transfer to a fresh microdroplet of sperm medium. Repeat this step 3–4× to wash out any residual PF solution (PF was shown to be embryotoxic in animal studies [27], but is apparently safe if used only on sperm [26]).
-
Keep selected spermatozoa in culture or place them into a PVP droplet for sperm selection and immobilization before ICSI.
-
Repeat these steps until sufficient number of viable sperm is selected for ICSI to be carried out.
Expert Commentary
PESA and TESA are effective surgical sperm retrieval methods for men with OA regardless of the cause (Table 24.3). However, the adoption of strict criteria to determine that the azoospermia is indeed obstructive is crucial for obtaining a high successful retrieval rate in the range of 90–100%. Using PESA, our approach is to perform the first aspiration at the epididymis corpus, and proceed to the caput if necessary as aspirates from the cauda are usually rich in poor-quality senescent spermatozoa, debris, and macrophages. Based on our findings, motile spermatozoa is obtained in 73% of the cases after the first or second aspiration. TESA is required as a rescue procedure after a failed PESA in approximately 14% of the individuals (Table 24.3). Most cases of PESA failures are not necessarily technical failures because immotile spermatozoa are found. However, in certain cases of epididymis fibrosis due to multiple PESA attempts or postinfection, PESA may be ineffective. In these cases, PESA can be attempted at the contralateral epididymis or TESA can be applied (Table 24.3). Routinely, procedures are performed under local anesthesia, with or without intravenous sedation, and at the same day of oocyte retrieval. Patients are discharged 1 h later and can return to normal activities in the same day. Oral analgesics are prescribed but pain complaint is minimal. The most common complication is fibrosis at the aspiration site. Other potential complications include hematoma, bleeding, and infection, but are rare [8]. Some authors advocate that MESA allows the collection of larger and cleaner quantities of sperm than PESA, but this debate is trivial. In our series of 142 men with OA, cumulative successful retrieval rate after PESA and/or TESA was 97.9% (Table 24.3), and an adequate number of motile sperm for cryopreservation was obtained in approximately 31% (35/112) of the cases. Clinical outcomes of ICSI using PESA- or TESA-derived spermatozoa are similar in OA (Table 24.4), and results are comparable to those obtained with ejaculated sperm [28] (Table 24.5). Although the cryopreservation rate after PESA is not high, repeated aspirations can be carried out in men with OA at lower cost and morbidity than MESA. In rare circumstances, we perform MESA in men presenting coagulopathies.
When gradient centrifugation is chosen for PESA sperm processing, we recommend that part of the sample is spared and processed by simple washing. The reason is the unpredictability of gradient centrifugation to recover motile sperm in such cases. If recovery is less than desired, we can rely on the washed sample to select motile sperm for ICSI. Due to the relatively low sperm yields in PESA and TESA, it is important to use low volumes of media during sperm processing and wash the sample only once. Centrifugation force and time should be carefully controlled to avoid jeopardizing the often compromised sperm motility.
For NOA, TESE, with or without magnification, is clearly the preferred approach. Efficiency of TESA for retrieving spermatozoa in NOA is only 10–30% [29], except in the favorable cases of men with testicular histopathology showing hypospermatogenesis, to whom retrieval rates are approximately 80–100% [13] (Table 24.6). Nonetheless, if a previous TESA attempt had been successful in a man with NOA, its positive predictive value for a successful second attempt is 70% [30]. Based on these results, it is our opinion that TESA should be reserved for NOA individuals having a diagnostic testicular biopsy histopathology showing hypospermatogenesis or with a previous successful TESA attempt. However, if TESA fails, we neither perform a second aspiration in the same testis, at the same operative time, nor convert it to an open procedure, to avoid the risk of hematoma and testicular injury. From our clinical experience, it is very difficult to identify enlarged seminiferous tubules in such cases, even using the operating microscope, because extensive bleeding is often seen. In these occasions, we opt to perform TESA or TESE at the contralateral testis. For NOA patients without previous diagnostic testicular biopsy or TESA attempt, our choice is to perform sperm extraction using micro-TESE.
The use of optical magnification during TESE limits the risk of vascular injury and optimizes the chances of finding sperm [10–12]. Although no absolute predictors for sperm retrieval are available in NOA, the probability of retrieving sperm varies according to the testicular histopathology results [12, 13] (Table 24.6). Proper identification of testicular vessels under the tunica albuginea is made prior to the placement of an incision into the testis. Microsurgery also allows the preservation of intratesticular blood supply, as well as the identification of tubules more likely to harbor sperm production. Therefore, efficacy of sperm retrieval is improved while the risks of large tissue removal are minimized. Excision of large biopsy samples in conventional TESE has been shown to impair testosterone production [31]. Tissue removal in micro-TESE is often 50- to 70-fold less than standard TESE [11], and the small amount of tissue extracted facilitates sperm processing. Selection of spermatozoa from a smaller population of contaminating testicular cells allows more ease and greater speed for sperm pickup and injection process, as well as alleviates contamination and blockage of the injection needle with cells and debris. It is far less technically demanding and labor intensive to extract spermatozoa from small volume specimens than large pieces of testicular tissue that must be dissected, red blood cells lysed, and the rare spermatozoa searched for in a tedious fashion under an inverted microscope. TESE sperm processing may be incredibly labor intensive, and the searching process may miss the rare spermatozoa within a sea of seminiferous tubules and other cells. TESE/micro-TESE may be scheduled either for the day of oocyte collection and ICSI or the day before. In the latter, processed specimens are incubated in a closed HEPES-buffered culture system (microdrops under mineral oil) at room temperature, inside a laminar flow cabinet or in a clean room for a maximum of 48 h, to avoid bacterial contamination. Culture of specimens at 37°C inside the incubator should be avoided since contamination with scrotum skin-derived bacteria is often seen. From our data, optimal fertilization by ICSI using surgically retrieved sperm is obtained when the time frame from hCG administration to microinjection does not exceed 44 h [32]. Testicular tissue sperm processing, searching, and selection of viable spermatozoa for ICSI may take several hours in NOA cases. Our laboratory takes approximately 12 min to handle a single testicular spermatozoon from searching to microinjection in NOA, but only 5.5 min in OA. In other words, the average time required to perform ICSI in a standard NOA treatment cycle involving 8–12 metaphase II oocytes is approximately 2 h. Therefore, we elect to perform micro-TESE the day before oocyte collection when a busy next day IVF laboratory workload is anticipated. Additionally, we recommend that two laboratory technicians work together during the initial processing steps (one mincing the tubules and the other searching for spermatozoa) to speed up the searching process and to allow a faster feedback to the surgeon who may decide to end the procedure if sperm is found or to continue dissecting the seminiferous tubules. Our laboratory performs the processing of testicular specimens by mincing and shredding the whole tissue instead of using enzymatic digestion. The mechanical preparation has the advantage of being fast, requiring about 15–30 min, while enzymatic digestion is more time consuming, requiring at least 4 h [33]. Studies comparing both techniques show conflicting results, but large series were unable to confirm the superiority of one technique over the other for processing fresh or frozen testicular sperm [33–36].
The clinical outcomes of ICSI using testicular sperm extracted by TESA or micro-TESE from NOA individuals are significantly lower than those obtained with either ejaculated or epididymal/testicular sperm taken from men with OA [28] (Table 24.5). Our data indicate that testicular spermatozoa of men with severely impaired spermatogenesis have decreased fertility potential and may have a higher tendency to carry deficiencies such as the ones related to the centrioles and genetic material, which ultimately affect the capability of the male gamete to activate the egg and trigger the formation and development of a normal zygote and a viable embryo [28].
The concept of cryopreservation may be used in association with sperm retrieval procedures. Some centers prefer to retrieve and intentionally cryopreserve sperm for future use. This strategy offers the advantage of avoiding ovarian stimulation when no sperm is obtained from testicular specimens. If sperm is found and frozen, thawing can be done at any time, thus obviating the need to organize two operations (oocyte and sperm retrieval) at the same day. Also, cryopreservation may be an interesting tool to spare leftover specimens that would be discharged after ICSI, especially if the treatment cycle does not result in a pregnancy. Future ICSI attempts may be carried out without repeated surgical retrievals. We routinely freeze excess motile epididymal spermatozoa which are not needed for the current ICSI cycle. Most often, motile sperm will be available after thawing in such cases, and ICSI outcomes using motile fresh or frozen epididymal sperm seems not to differ [37]. Cryopreservation of testicular sperm is also advisable, especially for men with NOA who often require multiple ICSI attempts to conceive but may not have an adequate number of sperm available for repeated retrieval attempts. However, postthawed testicular sperm are often immotile or exhibit only a twitching motility, and ICSI results using immotile testicular sperm are lower than fresh ones [17, 38]. Methods for selecting immotile viable sperm for ICSI are available, but results are limited for cryopreserved specimens. HOST may not discriminate viable and nonviable frozen–thawed spermatozoa [21]. Response to motility stimulants is unpredictable, and STFT has not been validated in large series [22–27]. The application of a single laser shot to the far end of the sperm tail has been shown to cause a curling of the tail only in viable sperm, similar to the reaction observed with the HOST, but this method has not been validated in cryo-thawed specimens [39]. We currently use the STFT for discriminating viable and nonviable immotile sperm for ICSI. Using this method, normal fertilization rates obtained by our group has been fair (39.9%). In vitro incubation of fresh or frozen retrieved sperm in culture medium may aid to obtain a more viable and functionally normal sperm population that obviates the risks of using immotile unselected sperm for ICSI. Sperm culture media have the components to support normal metabolism of immotile, mature, retrieved spermatozoa that may become motile by incubation [40]. However, in vitro incubation should be limited to a maximum of 48 h since contamination by bacteria that normally come from the scrotal skin is almost a rule after a period of 36–48 h, even when strict sterile operating and laboratory conditions are used. According to each group’s results, different strategies can be developed. If freezing of surgically retrieved specimens provides similar results than those obtained by using fresh sperm, then the use of freezing specimens would be preferable. If not, fresh specimens are preferable. In our hands, ICSI is performed with fresh testicular sperm whenever possible, even with the risk of submitting the female partner to unnecessary ovarian stimulation or the male to repeated retrievals. The reasons are related to the lower pregnancy rates obtained with cryo-thawed immotile testicular sperm by our group and others [18, 38, 40, 41]. To date, our technique for cryopreserve surgically-retrieved sperm is the standard liquid nitrogen vapor method using TEST-yolk buffer and glycerol as cryoprotectants [14–16]. Epididymal specimens are concentrated by washing before freezing, and testicular sperm are freed from the testicular parenchyma, i.e., testicular homogenates are frozen. Cryopreservation of few sperm into an empty zona pellucida and the use of stimulants before freezing may optimize results [15, 24, 42, 43]. Recently, it has been shown that human spermatozoa can be successfully vitrified, and this strategy may be of interest for preserving small quantities of surgically retrieved gametes [44].
Conclusions/Key Points
-
PESA and TESA are simple and efficient surgical methods for epididymal and testicular sperm retrieval, respectively, in men with OA. For NOA, TESE, with or without magnification (micro-TESE), should be the preferred approach. The use of microsurgery during TESE may improve the efficacy of sperm extraction with significantly less tissue removed, which ultimately facilitates sperm processing. Sperm retrieval should be carried out either at the day of oocyte retrieval or the day before, depending on the laboratory workload.
-
The primary goal of PESA/TESA/TESE sperm processing is the recovery of a clean sample containing motile sperm. Such specimens are more fragile, and often compromised in motility, as compared to the ones obtained from ejaculates. Laboratory techniques should be carried out with great caution to avoid jeopardizing the sperm fertilizing potential. The whole process starts with the surgical collection of the best quality specimen possible. During laboratory steps, minimal iatrogenic cellular damage may be achieved by strict control of centrifugation force and duration, exposure to ultraviolet light and temperature variation, laboratory air quality conditions, as well as the use of high-quality reagents, materials, and equipments.
-
PESA sperm processing may be performed either by mini-gradient centrifugation or simple washing using low volumes of culture media. Testicular specimens may be processed either by mechanical mincing of seminiferous tubules or enzymatic digestion, with similar results, and homogenates are simply washed. The mechanical preparation is significantly faster than enzymatic digestion.
-
The use of unselected immotile epididymal/testicular sperm for ICSI negatively impact clinical outcomes. Methods for selecting viable immotile sperm for ICSI include the HOST, STFT, and motility stimulants.
-
The concept of cryopreservation may be useful for intentionally cryopreserve retrieved sperm for future use or spare leftover specimens that would be discharged after ICSI. Different strategies can be developed according to each group’s results. If freezing of surgically retrieved specimens provides similar results than those obtained with the use of fresh sperm, then the use of freezing specimens would be preferable. If not, fresh specimens are preferable.
References
Palermo G, Joris H, Devroey P, et al. Pregnancies after intracytoplasmic sperm injection of single spermatozoan into an oocyte. Lancet. 1992;340:17–8.
Silber S, Nagy ZP, Liu J, et al. Conventional in-vitro fertilization versus intracytoplasmic sperm injection for patients requiring microsurgical sperm aspiration. Hum Reprod. 1994;9:1705–9.
Devroey P, Liu J, Nagy ZP, et al. Pregnancies after testicular extraction (TESE) and intracytoplasmic sperm injection (ICSI) in non-obstructive azoospermia. Hum Reprod. 1995;10:1457–60.
Esteves SC, Miyaoka R, Agarwal A. An update on the clinical assessment of the infertile male. Clinics (Sao Paulo). 2011;66:691–700.
Esteves SC, Glina S. Recovery of spermatogenesis after microsurgical subinguinal varicocele repair in azoospermic men based on testicular histology. Int Braz J Urol. 2005;31:541–8.
Craft I, Tsirigotis M, Bennett V, et al. Percutaneous epididymal sperm aspiration and intracytoplasmic sperm injection in the management of infertility due to obstructive azoospermia. Fertil Steril. 1995;63:1038–42.
Craft I, Tsirigotis M. Simplified recovery, preparation and cryopreservation of testicular spermatozoa. Hum Reprod. 1995;10:1623–7.
Raviv G, Levron J, Menashe Y, et al. Sonographic evidence of minimal and short-term testicular damage after testicular sperm aspiration procedures. Fertil Steril. 2004;82:442–4.
Okada H, Dobashi M, Yamazaki T, et al. Conventional versus microdissection testicular sperm extraction for nonobstructive azoospermia. J Urol. 2002;168:1063–7.
Tsujimura A, Matsumiya K, Miyagawa Y, et al. Conventional multiple or microdissection testicular sperm extraction: a comparative study. Hum Reprod. 2002;17:2924–9.
Schlegel PN. Testicular sperm extraction: microdissection improves sperm yield with minimal tissue excision. Hum Reprod. 1999;14:131–5.
Ramasamy R, Lin K, Gosden LV, et al. High serum FSH levels in men with nonobstructive azoospermia does not affect success of microdissection testicular sperm extraction. Fertil Steril. 2009;92:590–3.
Esteves SC, Verza Jr S, Prudencio C, Seol B. Sperm retrieval rates (SRR) in nonobstructive azoospermia (NOA) are related to testicular histopathology results but not to the etiology of azoospermia. Fertil Steril 2010;94:S132.
Esteves SC, Sharma RK, Thomas AJ, et al. Improvement in motion characteristics and acrosome status in cryopreserved spermatozoa by swim-up processing before freezing. Hum Reprod. 2000;15:2173–9.
Esteves SC, Spaine DM, Cedenho AP. Effects of pentoxifylline treatment before freezing on motility, viability and acrosome status of poor quality human spermatozoa cryopreserved by the liquid nitrogen vapor method. Braz J Med Biol Res. 2007;40:985–92.
Verza Jr S, Feijo CM, Esteves SC. Resistance of human spermatozoa to cryoinjury in repeated cycles of thaw-refreezing. Int Braz J Urol. 2009;35:581–91.
Nagy ZP, Liu J, Joris H, et al. The result of intracytoplasmic sperm injection is not related to any of the three basic sperm parameters. Hum Reprod. 1995;10:1123–9.
Dafopoulos K, Griesinger G, Schultze-Mosgau A, et al. Factors affecting outcome after ICSI with spermatozoa retrieved from cryopreserved testicular tissue in non-obstructive azoospermia. Reprod Biomed Online. 2005;10:455–60.
Liu J, Tsai YL, Katz E, et al. High fertilization rate obtained after intracytoplasmic sperm injection with 100% no motile spermatozoa selected by using a simple modified hypo-osmotic swelling test. Fertil Steril. 1997;68:373–5.
Sallam HN, Farrag A, Agameya A-F, et al. The use of the modified hypo-osmotic swelling test for the selection of immotile testicular spermatozoa in patients treated with ICSI: a randomized controlled study. Hum Reprod. 2005;20:3435–40.
Esteves SC, Sharma RK, Thomas Jr AJ, et al. Suitability of the hypo-osmotic swelling test for assessing the viability of cryopreserved sperm. Fertil Steril. 1996;66:798–804.
Soares JB, Glina S, Antunes Jr N, et al. Sperm tail flexibility test: a simple test for selecting viable spermatozoa for intracytoplasmic sperm injection from semen samples without motile spermatozoa. Rev Hosp Clin Fac Med Sao Paulo. 2003;58:250–3.
Oliveira NM, Sanchez RV, Fiesta SR, et al. Pregnancy with frozen-thawed and fresh testicular biopsy after motile and immotile sperm microinjection, using the mechanical touch technique to assess viability. Hum Reprod. 2004;19:262–5.
Esteves SC, Sharma RK, Thomas Jr AJ, et al. Cryopreservation of human spermatozoa with pentoxifylline improves the post-thaw agonist-induced acrosome reaction rate. Hum Reprod. 1998;13:3384–9.
Terriou P, Hans E, Giorgetti C, et al. Pentoxifylline initiates motility in spontaneously immotile epididymal and testicular spermatozoa and allows normal fertilization, pregnancy, and birth after intracytoplasmic sperm injection. J Assist Reprod Genet. 2000;17:194–9.
Kovacic B, Vlaisavljevic V, Reljic M. Clinical use of pentoxifylline for activation of immotile testicular sperm before ICSI in patients with azoospermia. J Androl. 2006;27:45–52.
Yovich JL. Pentoxifylline: actions and applications in assisted reproduction. Hum Reprod. 1993;8:1786–91.
Verza Jr S, Esteves SC. Sperm defect severity rather than sperm source is associated with lower fertilization rates after intracytoplasmic sperm injection. Int Braz J Urol. 2008;34:49–56.
Friedler S, Raziel A, Strassburger D, et al. Testicular sperm retrieval by percutaneous fine needle aspiration compared to testicular sperm extraction by open biopsy in men with non-obstructive azoospermia. Hum Reprod. 1997;12:1488–93.
Fasouliotis SJ, Safran A, Porat-Katz A, et al. A high predictive value of the first testicular fine needle aspiration in patients with non-obstructive azoospermia for sperm recovery at the subsequent attempt. Hum Reprod. 2002;17:139–42.
Schlegel PN, Su LM. Physiologic consequences of testicular sperm extraction. Hum Reprod. 1997;12:1688–92.
Schneider DT, Gomes AP, Verza Jr S, et al. Optimal time interval for intracytoplasmic sperm injection after administration of human chorionic gonadotrophin in severe male factor infertility. Fertil Steril. 2006;86:S155.
Verheyan G, De Croo I, Tournaye H, et al. Comparison of four mechanical methods to retrieve spermatozoa from testicular tissue. Hum Reprod. 1995;10:2956–9.
Salzbrunn A, Benson DM, Holstein AF, et al. A new concept for the extraction of testicular spermatozoa as a tool for assisted fertilization (ICSI). Hum Reprod. 1996;11:752–5.
Nagy ZP, Verheyen G, Tournaye H, et al. An improved treatment procedure for testicular biopsy specimens offers more efficient sperm recovery: case series. Fertil Steril. 1997;68:376–9.
Baukloh V. Retrospective multicentre study on mechanic and enzymatic preparation of fresh and cryopreserved testicular biopsies. Hum Reprod. 2002;17:1788–94.
Devroey P, Silber S, Nagy ZP, et al. Ongoing pregnancies and birth after intracytoplasmic sperm injection with frozen-thawed epididymal spermatozoa. Hum Reprod. 1995;10:903–6.
Fisher R, Baukloh V, Naether OGJ, et al. Pregnancy after intracytoplasmic sperm injection of spermatozoa from frozen-thawed testicular biopsy. Hum Reprod. 1996;11:2197–9.
Aktan TM, Montag M, Duman S, et al. Use of laser to detect viable but immotile spermatozoa. Andrologia. 2004;36:366–9.
Zhu J, et al. In vitro maturation of testicular spermatozoa. Hum Reprod. 1996;11:231–2.
Konc J, Kanya K, Cseh S. The effect of condition/state of testicular spermatozoa injected to the outcome of TESE-ICSI-ET cycles. Eur J Obstet Gynecol Reprod Biol. 2008;141:39–43.
Liu J, Zheng XZ, Baramki TA, et al. Cryopreservation of a small number of fresh human testicular spermatozoa and testicular spermatozoa cultured in vitro for 3 days in an empty zona pellucida. J Androl. 2000;21:409–13.
Levi-Setti PE, Albani E, Negri L, et al. Cryopreservation of a small number of spermatozoa in yolk-filled human zonae pellucidae. Arch Ital Urol Androl. 2003;75:195–8.
Isachenko E, Isachenko V, Weiss JM, et al. Acrosomal status and mitochondrial activity of human spermatozoa vitrified with sucrose. Reproduction. 2008;136:167–73.
Acknowledgment
The authors would like to acknowledge Christina Prudencio and Bill Seol, for their assistance in data collection and processing, and Mrs. Fabiola Bento for editorial and text revision.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2012 Springer Science+Business Media, LLC
About this chapter
Cite this chapter
Esteves, S.C., Verza, S. (2012). PESA/TESA/TESE Sperm Processing. In: Nagy, Z., Varghese, A., Agarwal, A. (eds) Practical Manual of In Vitro Fertilization. Springer, New York, NY. https://doi.org/10.1007/978-1-4419-1780-5_24
Download citation
DOI: https://doi.org/10.1007/978-1-4419-1780-5_24
Published:
Publisher Name: Springer, New York, NY
Print ISBN: 978-1-4419-1779-9
Online ISBN: 978-1-4419-1780-5
eBook Packages: MedicineMedicine (R0)