
Abstract
Deficiency of pyridox(am)ine 5′-phosphate oxidase (PNPO, OMIM 610090) is a treatable autosomal recessive inborn error of metabolism. Neonatal epileptic encephalopathy and a low cerebrospinal fluid (CSF) pyridoxal 5′-phosphate level are the reported hallmarks of PNPO deficiency, but its clinical and biochemical spectra are not fully known. Case presentation: A girl born at 33 3/7 weeks of gestation developed seizures in the first hours of life. Her seizures initially responded to GABAergic agonists, but she subsequently developed a severe epileptic encephalopathy. Brain MRI and infectious and metabolic evaluations at birth, including urinary alpha-aminoadipic semialdehyde (AASA), were normal. Lumbar puncture at age 3 months showed: pyridoxal 5′-phosphate, 52 nmol/L (normal, 23–64); homovanillic acid, 392 nmol/L (normal, 450–1,132); 5-hydroxyindoleacetic acid, 341 nmol/L (normal, 179–711); and 3-ortho-methyldopa, 30 nmol/L (normal, below 300). The patient was not being treated with pyridoxine nor with pyridoxal 5′-phosphate at the time of the lumbar puncture. She died at age 14 months. A sequencing panel targeting 53 epilepsy-related genes revealed a homozygous missense mutation in PNPO (c.674G>A, p.R225H). Homozygosity was confirmed by parental testing. Expression studies of mutant p.R225H PNPO revealed greatly reduced activity. In conclusion, a normal CSF level of pyridoxal 5′-phosphate does not rule out PNPO deficiency.
Competing interests: None declared
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others
Keywords
- Status Epilepticus
- Infantile Spasm
- Epileptic Encephalopathy
- Homozygous Missense Mutation
- Good Seizure Control
These keywords were added by machine and not by the authors. This process is experimental and the keywords may be updated as the learning algorithm improves.
Introduction
Pyridox(am)ine 5′-phosphate oxidase deficiency (PNPO deficiency, OMIM 610090) is a treatable cause of neonatal epileptic encephalopathy (Mills et al. 2005), clinically resembling pyridoxine-dependent epilepsy due to antiquitin deficiency (OMIM 266100). Since PNPO is necessary for conversion of pyridoxine 5′-phosphate and pyridoxamine 5′-phosphate into pyridoxal 5′-phosphate (PLP; the only active form of vitamin B6), as well as for the recycling of PLP (Musayev et al. 2003), seizures in PNPO deficiency are usually resistant to pyridoxine but respond to pyridoxal 5′-phosphate (di Salvo et al. 2011), although several pyridoxine-responsive patients have been reported (Mills et al. 2014; Plecko et al. 2014).
Given the catastrophic natural history of PNPO deficiency (Mills et al. 2005) and the possibility of satisfactory outcomes in some cases with prompt diagnosis and treatment (Schmitt et al. 2010; Goyal et al. 2013), the development of reliable diagnostic tools for the disease is crucial.
PLP in cerebrospinal fluid has been proposed as an important diagnostic marker in PNPO deficiency, and reference ranges have been established for this purpose (Ormazabal et al. 2008). It is known that the finding of low CSF PLP is not in itself diagnostic of PNPO deficiency. Low CSF PLP has been reported in inborn errors of metabolism associated with the accumulation of metabolites that inactivate PLP such as antiquitin deficiency and molybdenum cofactor deficiency (Footitt et al. 2011), as well as in epileptic encephalopathy with no specific diagnosis (Goyal et al. 2013).
On the other hand, until the present report, all six patients with confirmed PNPO deficiency in whom pretreatment CSF PLP has been measured in the absence of PLP or pyridoxine supplementation have had low levels (cf. Table 1). Given the role of PNPO in the synthesis and recycling of PLP, the finding of low CSF PLP levels in deficient patients is also intuitively plausible. Nevertheless, as we show in the following report, the presence of a normal PLP level is insufficient to rule out PNPO deficiency.
We describe the first known patient with PNPO deficiency and a normal CSF PLP level, and we place her clinical presentation and diagnostic findings within the context of previously reported PNPO-deficient patients with a targeted literature review.
Methods
Cerebrospinal Fluid Analysis
Reversed phase HPLC and fluorescence detection were used for measurement of PLP, as described by Ormazabal et al. (2008), and reversed phase HPLC with electrochemical detection was used for measurement of neurotransmitter metabolites, as described by Hyland et al. (1993). Reference values for CSF pyridoxal 5′-phosphate were obtained using CSF from over 100 infants and children with neurological disease in whom seizures were not present. Values obtained were similar to published values (Ormazabal et al. 2008). CSF values decrease with age and the appropriate age-matched control group was used for comparison with the value obtained from our patient.
Mutant PNPO Expression Studies
The p.R225H mutant was created by site-directed mutagenesis and expressed in an in vitro translation system using a HeLa cell lysate (Thermo Scientific 1-Step Human Coupled IVT Kit) according to manufacturer’s instructions. The reaction was incubated for 6 h at 30°C. PNPO enzyme activity was measured with pyridoxamine 5′-phosphate (PMP) as substrate using an HPLC-mass spectrometry assay for B6 vitamers (Footitt et al. 2013). These methods are described in full elsewhere (Mills et al. 2014).
Literature Review
PubMed was searched for “PNPO”, “pyridoxal 5′-phosphate”, “pyridoxal 5′-phosphate-dependent epilepsy” and variants. Articles containing case descriptions of patients diagnosed with PNPO deficiency were retained for further analysis.
Duplicate descriptions of the same patient were combined, and patient descriptions that provided no clinical information and/or did not provide molecular proof of PNPO deficiency were excluded. In particular, two patients (Footitt et al. 2011) were excluded as no clinical information, apart from posttreatment plasma PLP levels, was provided. Likewise, one patient (Kuo and Wang 2002) was excluded, as the diagnosis was confirmed neither by molecular nor by biochemical methods. We also excluded patients G3 and G4 described by Mills et al. (2005), as it is unclear whether they had clinical symptoms of epileptic encephalopathy or died of complications of extreme prematurity. Finally, one patient (Veerapandiyan et al. 2011) was excluded as PNPO sequencing was normal.
The remaining 46 patient descriptions were compared with our patient using the following parameters: gestational age, age at seizure onset, presenting features, neuroimaging and EEG findings, history of treatment with and response to pyridoxine and PLP and outcome.
Patient descriptions were numbered 1–46, as shown in Table 2.
Results
Case Description
Our patient, a girl, was born at 333/7 weeks gestation to healthy non-consanguineous French-Canadian parents with no relevant family history. Before the premature onset of labour, the pregnancy had been uneventful apart from the sensation of abnormal “vibrating” fetal movements. Caesarean section was performed for breech presentation. Meconial fluid was observed, but Apgar scores were 9-9-9 (at 1, 5 and 10 min, respectively). Birth weight (2.080 kg) was normal for gestational age.
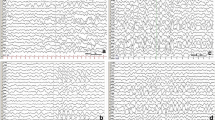
Myoclonic or multifocal seizures with abnormal movements of the head, eyes and mouth began at 2 h of life, and initially responded to benzodiazepines, with seizure-free periods of up to 9 days in the neonatal period. EEGs performed in the first 2 weeks of life displayed immature rhythms with inter-hemispheric asynchrony and prolonged intervals of attenuation of background rhythms lasting up to 60 s, compatible with tracé discontinu (discontinuous pattern), which failed to improve with maturation (Supplementary Figure 1a). Pyridoxine treatment was attempted on days 7–14 (100 mg intravenously, then 50 mg orally twice a day) and day 22 (50 mg twice a day); there was no clear effect on seizure activity, but somnolence and increased apnoeic episodes were observed. PLP was not administered. Initial lumbar puncture did not provide enough fluid for neurotransmitter analysis; subsequent attempts (five overall) were unsuccessful. Cerebral magnetic resonance imaging and infectious and metabolic evaluations, including urinary alpha-aminoadipic semialdehyde (AASA), were normal.
The baby was discharged on clobazam 9 mg/kg/day with satisfactory seizure control at 6 weeks of chronological age. Myoclonic seizures and episodes of tonic flexion spasms unresponsive to topiramate and ACTH occurred 3 weeks later. EEGs revealed slow background activity with episodes of rhythm desynchronisation and attenuation (electrodecremental patterns) without hypsarrhythmia. At 4 and 5 months, she was hospitalised for benzodiazepine-responsive status epilepticus.
CSF was obtained by lumbar puncture under fluoroscopic guidance at 4 months of age. Cell count, protein content, glucose, lactate, amino acids, 5-methyltetrahydrofolate and pterin metabolites were normal. The CSF pyridoxal 5′-phosphate was 52 nmol/L (normal, 23–64); homovanillic acid, 392 nmol/L (normal, 450–1,132); 5-hydroxyindoleacetic acid, 341 nmol/L (normal, 179–711); and 3-ortho-methyldopa, 30 nmol/L (normal, below 300). An additional early eluting unknown compound was seen in the chromatogram obtained from the analysis of CSF pyridoxal 5′-phosphate (not shown). A likely candidate is pyridoxine phosphate (Pearl et al. 2013), but unfortunately we have been unable to obtain a reference compound for verification studies. Pyridoxamine has been reported to be elevated in plasma and CSF in PNPO deficiency in patients receiving pyridoxal 5′-phosphate or pyridoxine (Ware et al. 2014). Our patient was not receiving B6 therapy at the time of lumbar puncture so the unknown compound is unlikely to be pyridoxamine although this remains to be verified.
After the second episode of status epilepticus at age 5 months, she suffered from refractory epilepsy (multifocal and tonic seizures, spasms) and repeated status epilepticus (responsive to IV lorazepam or phenobarbital).
She had better seizure control from 7½ to 12 months of age (one seizure a week or fewer), which a trial of ketogenic diet did not improve further. In retrospect, this period coincided with the administration of pyridoxine (100 mg twice a day) and ended after pyridoxine was discontinued; she was, however, also being treated with phenobarbital, clobazam and clonazepam, and the relationship between pyridoxine and seizure control was not clinically apparent at the time. She had severe psychomotor delay, and her head circumference declined from the 50th percentile at birth to between the second and fifth percentiles.
At the chronological age of 12 months, she presented with a refractory status epilepticus. She had tonic seizures (Supplementary Figure 1b), followed by refractory subclinical continuous multifocal epileptic activity on EEG accompanied by hypoventilation and apnoea; multifocal seizure activity on EEG responded to midazolam perfusion but recurred when the perfusion was stopped. Cerebral MRI was still normal apart from atrophic changes and delays in myelination, both mild. She died at 14 months of age, having been taken off life support.
A sequencing panel targeting 53 epilepsy-related genes (Medical Neurogenetics) revealed an apparently homozygous missense mutation in PNPO (c.674G>A, p.R225H). Homozygosity was confirmed by parental testing. Samples from this patient were also included in an exome-sequencing study of unexplained infantile spasms, which simultaneously revealed the same PNPO mutation as our investigation (Michaud et al. 2014).
The p.R225H mutation was characterised in several fashions. Arginine 225 is conserved from yeast to humans (Supplementary Figure 2), is located at the active site of PNPO and interacts directly with the phosphate moiety of pyridoxal 5′-phosphate (Musayev et al. 2003). In silico analysis using PolyPhen-2, Proveen and Mutation Taster predicted p.R225H to be pathogenic. During the preparation of this article, the p.R225H mutation was reported in other patients with PNPO deficiency (Mills et al. 2014; Plecko et al. 2014; Ware et al. 2014). Finally, in vitro expression of a mutant PNPO cDNA containing p.R225H produced 8% of the PNPO activity of wild-type controls.
Targeted Literature Review
Clinical Findings
We reviewed the clinical presentation, response to treatment and outcome of the 48 previously described cases of PNPO deficiency (summarised in Table 3 and detailed in Supplementary Table 1) and their pretreatment biochemical findings (summarised in Table 1 and detailed in Supplementary Table 2).
Our patient’s clinical presentation was consistent with previous reports. Prematurity was a finding in 27/44 (61%) of patients for whom gestational age was known, and in at least 5/46 (11%), abnormal movements were noted in utero. 27/44 (61%) of patients presented with seizures on the first day of life and all but two (96%) before 1 month of age; the exceptions were a child treated from birth and therefore asymptomatic (patient 23) and a child first presenting with infantile spasms at age 5 months (patient 26). Clinical descriptions of the seizures were available in 33/46 cases (72%); of these, myoclonus was reported in 20/33 (61%) and abnormal oral, ocular or head movements in 9/33 (27%). Metabolic acidosis was present in 13/46 (28%) of cases. Burst suppression was reported in 20 of the 35 patients for whom EEG data were available (57%), but various other EEG patterns were also described, including at least 7/35 (20%) with a discontinuous pattern.
Our patient had an ambiguous response to pyridoxine in the neonatal period – no change in seizure frequency but increased apnoeic episodes and lethargy, which have been associated with pyridoxine responsiveness in antiquitin deficiency (Stockler et al. 2011) – and later had a period of relatively good seizure control that coincided with pyridoxine administration; in retrospect, she may well have been partially pyridoxine responsive. 37/46 (80%) of previously described patients underwent a pyridoxine trial; of these, 17/37 (46%) showed a clear clinical response. Our patient’s p.R225H genotype is one of several reported to be associated with pyridoxine responsiveness (Mills et al. 2014; Plecko et al. 2014). Five patients homozygous for p.R225H and seven homozygous for a mutant allele containing p.R225H and p.R116Q have been identified. Of these 12 patients, 10 had a clear response to pyridoxine. Furthermore, each of the two non-responsive patients (patients 36 and 38) had younger affected siblings who were pyridoxine responsive but who were noted to respond gradually. It is therefore conceivable that patients 36 and 38 might also have responded to longer pyridoxine trials. The correlation between genotype and pyridoxine responsiveness is imperfect for other mutations as well. For instance, only 4/7 patients with one or two p.D33V mutant alleles were classified as pyridoxine responsive, suggesting that genotype alone cannot accurately predict pyridoxine responsiveness.
PLP was administered to 24/46 patients (52%) and was associated with a clear positive response in 18/24 (75%). Surprisingly, in 4/24 (17%) of cases, pyridoxine-responsive patients reacted poorly to a transition to PLP (with status epilepticus in two cases and an increase or recurrence of seizures in two others).
Clinical outcome was influenced by treatment and response to treatment. All 17 pyridoxine-responsive patients survived, as did all but one (93%) of the 15 patients who either did not receive pyridoxine or did not respond but did receive PLP. On the other hand, all 13 patients who either did not receive pyridoxine or did not respond, and also did not receive PLP, died: 9 in the first weeks of life (69%) and the rest between 5 and 7 months (31%). One patient survived for approximately 3 years before PLP treatment was begun (Patient 9); therefore, survival beyond 1 year is possible, though rare, in non-pyridoxine-responsive patients without PLP treatment. Overall, 14/46 patients (30%) died, at a median age of 33 days (range 7 days to 7 months). Information (often limited) about psychomotor development was available for all 32 survivors: 12/32 (38%) had significant developmental and/or neurological sequelae, while 20/32 (63%) had a normal or mildly delayed development.
Findings in Cerebrospinal Fluid
Our patient had normal CSF levels of PLP, 3-ortho-methyldopa and 5-HIAA, with mildly decreased levels of HVA.
In the literature, PLP was measured before PLP administration in only 7/46 patients (15%). In 6/7 (86%), PLP levels were below the reference range. The exception, a patient with a low-normal CSF PLP level, was receiving high-dose pyridoxine, with a partial clinical and biochemical response (Patient 1).
3-Ortho-methyldopa levels were elevated, as expected, in 9/12 (75%) patients; 3/12 (25%) of patients, like ours, had normal levels (one of these, however, was receiving pyridoxine at the time of sampling). HVA and 5-HIAA levels were reported in 19/46 patients (41%). Of these, 5-HIAA was low in seven (37%), normal in eight (42%) and high in 4 (21%); Likewise, HVA was low in seven cases (37%), normal in nine (47%) and high in three (16%). Of the patients with normal 5-HIAA and HVA, however, two were receiving pyridoxine at the time of sampling.
Discussion
To our knowledge, this is the first PNPO-deficient patient to present with normal CSF PLP levels in the absence of PLP or pyridoxine supplementation.
There is no evidence that this counterintuitive finding is explicable by error or artefact. The diagnosis of PNPO deficiency in our patient has been confirmed by both molecular and enzymatic methods. Likewise, there was no evidence of sample mix-up or laboratory error. Lumbar ultrasound showed no pockets of abnormal fluid accumulation nor anatomical abnormalities that might affect CSF dynamics. Repeat testing of the CSF specimen confirmed the initial observations, yielding an inter-assay difference of less than 1%. Our patient died before the results of PNPO sequencing became available, and repeat lumbar puncture or a therapeutic trial with PLP was not performed.
In retrospect our patient was probably partially pyridoxine responsive, like other reported p.R225H homozygotes. She had received no pyridoxine for 3 months before the lumbar puncture, however, making it unlikely that the previous treatment with pyridoxine could have altered PLP concentrations at the time of CSF sampling.
Pretreatment PLP levels have not been reported for other patients with p.R225H PNPO mutations; indeed, pretreatment PLP levels have been reported for only seven patients in the literature. The fraction of PNPO-deficient patients with normal CSF PLP levels is therefore unknown. A channelling mechanism has been suggested for the transfer of newly formed PLP from pyridoxal kinase and PNPO to the various enzymes that require it as a cofactor (di Salvo et al. 2011). If this is the case, certain PNPO mutations might adversely affect this transfer step as well as the known enzymatic activity of PNPO. We speculate that, under such circumstances, a normal CSF PLP level would be insufficient to ensure adequate delivery of cofactor to PLP-dependent enzymes, leading a patient to become symptomatic despite a normal CSF PLP level.
By showing that a normal CSF PLP level does not suffice to rule out PNPO deficiency, this report highlights the difficulties involved in diagnosing this condition. The clinical spectrum of PNPO deficiency has now been broadened, ranging from in utero presentations to a hitherto asymptomatic child presenting at 5 months with infantile spasms (Mills et al. 2014). As seen above, neurotransmitter metabolite levels may be variable in PNPO deficiency. A low level of CSF PLP is not a specific marker for PNPO deficiency (Footitt et al. 2011; Goyal et al. 2013); the present report shows that neither is it a sensitive diagnostic marker. A trial of treatment with PLP has the advantage of being potentially both therapeutic and diagnostic. PLP responsiveness, however, may also indicate other causes of PLP deficiency (Goyal et al. 2013). PLP may also exert a nonspecific anticonvulsant effect (Wang et al. 2005), although the responsive patients were not tested for PNPO deficiency in this study. Surprisingly, treatment with PLP may even exacerbate symptoms, at least in some pyridoxine-responsive patients (Mills et al. 2014; Plecko et al. 2014). Finally, while PNPO sequencing and deletion/duplication analysis is specific to PNPO deficiency and is likely to identify most affected patients, its utility is at present limited by the difficulty of interpreting sequence variants of uncertain significance and the possibility of unidentified pathogenic mutations in noncoding sequence.
In the absence of a diagnostic gold standard, a combination of approaches is likely to yield the best results. As we have shown, a normal CSF PLP level does not rule out PNPO deficiency. The present report highlights the critical importance of a timely therapeutic trial of pyridoxal 5′-phosphate in the context of a neonatal epileptic encephalopathy; in the presence of a positive response, molecular testing can in most cases clarify the diagnosis.
References
Bagci S, Zschocke J, Hoffmann GF et al (2008) Pyridoxal phosphate-dependent neonatal epileptic encephalopathy. Arch Dis Child Fetal Neonatal Ed 93(2):F151–F152
di Salvo ML, Contestabile R, Safo MK (2011) Vitamin B(6) salvage enzymes: mechanism, structure and regulation. Biochim Biophys Acta 1814(11):1597–1608
Footitt EJ, Heales SJ, Mills PB, Allen GF, Oppenheim M, Clayton PT (2011) Pyridoxal 5′-phosphate in cerebrospinal fluid; factors affecting concentration. J Inherit Metab Dis 34(2):529–538
Footitt EJ, Clayton PT, Mills K et al (2013) Measurement of plasma B6 vitamer profiles in children with inborn errors of vitamin B6 metabolism using an LC-MS/MS method. J Inherit Metab Dis 36(1):139–145
Goyal M, Fequiere PR, McGrath TM, Hyland K (2013) Seizures with decreased levels of pyridoxal phosphate in cerebrospinal fluid. Pediatr Neurol 48(3):227–231
Hoffmann GF, Schmitt B, Windfuhr M et al (2007) Pyridoxal 5′-phosphate may be curative in early-onset epileptic encephalopathy. J Inherit Metab Dis 30(1):96–99
Hyland K, Surtees RA, Heales SJ, Bowron A, Howells DW, Smith I (1993) Cerebrospinal fluid concentrations of pterins and metabolites of serotonin and dopamine in a pediatric reference population. Pediatr Res 34(1):10–14
Khayat M, Korman SH, Frankel P et al (2008) PNPO deficiency: an under diagnosed inborn error of pyridoxine metabolism. Mol Genet Metab 94(4):431–434
Kuo MF, Wang HS (2002) Pyridoxal phosphate-responsive epilepsy with resistance to pyridoxine. Pediatr Neurol 26(2):146–147
Michaud JL, Lachance M, Hamdan FF et al (2014) The genetic landscape of infantile spasms. Hum Mol Genet 23(18):4846–4858
Mills PB, Surtees RA, Champion MP et al (2005) Neonatal epileptic encephalopathy caused by mutations in the PNPO gene encoding pyridox(am)ine 5′-phosphate oxidase. Hum Mol Genet 14(8):1077–1086
Mills PB, Camuzeaux SS, Footitt EJ et al (2014) Epilepsy due to PNPO mutations: genotype, environment and treatment affect presentation and outcome. Brain 137(Pt 5):1350–1360
Musayev FN, Di Salvo ML, Ko TP, Schirch V, Safo MK (2003) Structure and properties of recombinant human pyridoxine 5′-phosphate oxidase. Protein Sci 12(7):1455–1463
Ormazabal A, Oppenheim M, Serrano M et al (2008) Pyridoxal 5′-phosphate values in cerebrospinal fluid: reference values and diagnosis of PNPO deficiency in paediatric patients. Mol Genet Metab 94(2):173–177
Pearl PL, Hyland K, Chiles J, McGavin CL, Yu Y, Taylor D (2013) Partial pyridoxine responsiveness in PNPO Deficiency. JIMD Rep 9:139–142
Plecko B, Paul K, Mills P et al (2014) Pyridoxine responsiveness in novel mutations of the PNPO gene. Neurology 82(16):1425–1433
Porri S, Fluss J, Plecko B et al (2014) Positive outcome following early diagnosis and treatment of pyridoxal 5-phosphate oxidase deficiency: a case report. Neuropediatrics 45(1):64–68
Ruiz A, García-Villoria J, Ormazabal A et al (2008) A new fatal case of pyridox(am)ine 5′-phosphate oxidase (PNPO) deficiency. Mol Genet Metab 93(2):216–218
Schmitt B, Baumgartner M, Mills PB et al (2010) Seizures and paroxysmal events: symptoms pointing to the diagnosis of pyridoxine-dependent epilepsy and pyridoxine phosphate oxidase deficiency. Dev Med Child Neurol 52(7):e133–e142
Stockler S, Plecko B, Gospe SM Jr et al (2011) Pyridoxine dependent epilepsy and antiquitin deficiency: clinical and molecular characteristics and recommendations for diagnosis, treatment and follow-up. Mol Genet Metab 104(1–2):48–60
Veerapandiyan A, Winchester SA, Gallentine WB et al (2011) Electroencephalographic and seizure manifestations of pyridoxal 5′-phosphate-dependent epilepsy. Epilepsy Behav 20(3):494–501
Wang HS, Kuo MF, Chou ML et al (2005) Pyridoxal phosphate is better than pyridoxine for controlling idiopathic intractable epilepsy. Arch Dis Child 90(5):512–515
Ware TL, Earl J, Salomons GS et al (2014) Typical and atypical phenotypes of PNPO deficiency with elevated CSF and plasma pyridoxamine on treatment. Dev Med Child Neurol 56(5):498–502
Acknowledgments
GAM and AML are supported by the Canadian Institutes for Health Research (CIHR).
PTC and PBM are supported by funding from Great Ormond Street Children’s Charity.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Additional information
Communicated by: Cornelis Jakobs, PhD
Electronic Supplementary Material
Below is the link to the electronic supplementary material.
Appendices
Synopsis
Pyridoxal 5′-phosphate levels in cerebrospinal fluid may be normal in neonatal epileptic encephalopathy caused by pyridox(am)ine 5′-phosphate oxidase (PNPO) deficiency.
Compliance with Ethics Guidelines
Conflicts of Interest
Alina Levtova, Stephane Camuzeaux, Anne-Marie Laberge, Pierre Allard, Catherine Brunel-Guitton, Paola Diadori, Elsa Rossignol, Peter T. Clayton, Philippa B. Mills and Grant A. Mitchell declare no conflict of interest.
Keith Hyland is Vice President of Medical Neurogenetics, a company that measures pyridoxal 5′-phosphate in cerebrospinal fluid and performs sequencing of the PNPO gene.
Informed Consent
The investigations performed were done on a clinical basis. Consent was obtained from the family for the publication of this patient’s history.
Details of the Contributions of Individual Authors
-
Writing and preparation of the manuscript: AL and GM
-
Clinical management and investigation of the patient: AL, AML, PD, ER, GM
-
Detailed review of the patient’s neurological and electrophysiological presentation: PD, ER
-
cDNA cloning and expression studies of the mutant PNPO enzyme: SC, PC, PM
-
Measurement of neurotransmitter metabolites and pyridoxal 5′-phosphate in cerebrospinal fluid and analysis of fluorescence chromatograms: KH
-
Critical review of the manuscript: All authors.
Rights and permissions
Copyright information
© 2015 SSIEM and Springer-Verlag Berlin Heidelberg
About this chapter
Cite this chapter
Levtova, A. et al. (2015). Normal Cerebrospinal Fluid Pyridoxal 5′-Phosphate Level in a PNPO-Deficient Patient with Neonatal-Onset Epileptic Encephalopathy. In: Zschocke, J., Baumgartner, M., Morava, E., Patterson, M., Rahman, S., Peters, V. (eds) JIMD Reports, Volume 22. JIMD Reports, vol 22. Springer, Berlin, Heidelberg. https://doi.org/10.1007/8904_2015_413
Download citation
DOI: https://doi.org/10.1007/8904_2015_413
Received:
Revised:
Accepted:
Published:
Publisher Name: Springer, Berlin, Heidelberg
Print ISBN: 978-3-662-47452-5
Online ISBN: 978-3-662-47453-2
eBook Packages: MedicineMedicine (R0)