
Abstract
The COVID-19 pandemic has affected the global healthcare system in many countries. India has faced complex multidimensional problems concerning the healthcare system during the COVID-19 outbreak. This article explores some of the implications of COVID-19 on the health system. Also, we attempt to study health economics and other related issues. We have developed the susceptible-exposed-infection-recovered model, logistic growth model, time interrupted regression model, and a stochastic approach for these problems. These models focus on the effect of prevention measures and other interventions for a pandemic on the healthcare system. Our study suggests that the above models are appropriate for COVID-19 at break and effective models for the implications of the pandemic on the healthcare system.
Access provided by Autonomous University of Puebla. Download conference paper PDF
Similar content being viewed by others


Keywords
- COVID-19
- Markov chain
- Logistic growth model
- SEIR model
- Time interrupted regression model
- Healthcare system
1 Introduction
The continuous spread of the COVID-19 outbreak is a new strain that has an impact at the global level and has become the greatest health challenge in the world. The COVID-19 pandemic has affected different people in various ways. The most important symptoms are fever, dry cough, tiredness, etc. The World Health Organization (2020) explained that some common symptoms are loss of taste, smell, and rashes on the skin. It’s high time to develop a medical solution for this. Lack of hospitals, physicians, health experts, and hospital beds are the severe scenarios facing India nowadays. Curfews, social distancing, self-isolation, and vaccinations all have a role in preventing pandemic transmission and high population density might make effective measures difficult. The Batch Markovian arrival process has been proposed by Neuts [1]. Assumptions are the Markov arrival process and its application to the stochastic model described by Chakravarthy [2]. Briggs has a long history of using Markov chains in public health decision-making and epidemiological research [3]. An application of the Markov model for economic (or) financial evaluation and medical decision-making was described by Sonnenberg and Beck [4]. Governments have taken effective steps such as partial lockdowns with social distancing, and isolations and vaccinations to reduce the transmissions of a pandemic, Zhang et al. [5]. Ozili and Arun have proposed mitigation measures for the intense effect on the global economic status [6]. Modeling for interventions taken to minimize the transmission rate of a pandemic in India by Mandal et al. [7]. In this study, the importance of increasing immunity, social distance, and lockdown measures concerning these measures can be useful in flattening the pandemic discussed by Bhola et al. [8]. Lopez et al. to reflect the environmental situation investigated the susceptible-exposed-infection-recovered model which presented dead, quantified, and protected population compartments [9]. Cano et al. defined the dynamics of the COVID-19 outbreak using a simple Markov model [7]. Several types of analysis have been made on the COVID-19 outbreak and describe the Ebola virus with demographic effects by Rachan [10]. The susceptible-exposed-infection-recovered model for demographic effects such as birth and mortality rate during COVID-19 outbreak was described by Hamzah et al. [11]. Analysis, forecast, simulation, and optimal controls for the Ebola virus used the susceptible-exposed-infection-recovered model by Porter [12]. The current pandemic is rising quickly and spreading to millions as evidenced by the many recorded cases in India by Sarkar et al. [6]. Many countries used vaccines, curfews, and self-isolation to control the COVID-19 pandemic. T. M Chen et al. are interested in studying the transmission patterns of the outbreak and the impact of further interventions [7]. A survey of social economic evaluation levels in many countries in the social mix through the R package by Chen and Zhou [13]. According to Adly et al. [14], the most definite answer for the public health system is to conduct tests as soon as possible to permit the rapid identification of active patients, effective treatment methods, and immediate self-isolation for susceptible cases. Describe the deterministic model for the impact of social distancing on the transmission dynamics of the COVID-19 outbreak in South Africa by Nyanadza et al. [15]. An analysis of the impact of lockdown measures taken to control the transmission dynamics of the COVID-19 outbreak in India was conducted by Youkta et al. [16]. Elinor Aviv-Sharon and Asaph Aharoni used generalized logistic modeling to characterize the transmission pattern and trace the trajectory of the COVID-19 outbreak, as well as the impact of specific interventions [17]. Details about the global preventive measures were described by Kumar et al. [18]. Verhulst developed the original logistic growth modeling for the biological population.
2 Overview of Indian Healthcare System and Changes in the COVID-19 Pandemic During this Period
Our country comprises 28 states and 8 union territories. Table 1 presents an overview of India's demographics.
The capacity of hospital beds is mostly determined by a country's income level. Our country has an average of 0.55 beds per 100 people depending on income level. The pandemic has negatively affected global health and daily life. Contingency plans for an expected surge of cases were also added to the current scenario. Medical personnel, homoeopathic and ayurvedic practitioners, medical students, volunteers, sanitary workers, ex-servicemen, teachers, doctors, and others were identified across the municipal corporation to create an online information pool of 15.8 million human resources for a variety of activities needed to combat the outbreak. It was also critical to match the demand for medical equipment and pharmaceuticals with the rising supply of infrastructure and human resources. The demand for personal protective equipment increased as private hospitals became involved. The spread of COVID-19 disease affected human health, psychological problem, and economic status, and related restrictions were implemented to control the unexpected adverse effects on human health. There are also other challenges described by Singh et al. [19].
3 Propose Models and Materials
3.1 Data Sources
The data for India and other states were taken from the official websites of the ICMR (http://www.icmr.gov.in), the website of COVID-19 India (http://covid19india.org). These data were used in a study on the impact of COVID-19 on the Indian healthcare system.
3.2 Susceptible-Exposed-Infection-Recovered Model
This model is a compartmental model to study infectious disease and divides the population into four components such as Susceptible (S), Exposed (E), Infectious (I), and Recovered (R). Susceptible populations are those who are at risk of becoming infected. The people who have been infected with the sickness and are able to converse with others are said to be infected. Exposed people have been exposed to the disease but are not yet contagious, while recovered persons have recovered from their illness. The parameters (β, γ, and σ) are explained as follows: β is a transmission parameter, which is the number of effective contacts per unit of time per infected individual; γ is the rate of recovery in a specific time; and σ is the rate at which infected individuals become infectious. The differential equations that describe this model are as follows:
Subject to the conditions, S(0)>0, E(0)≥0, I(0)≥0, R(0)≥0.
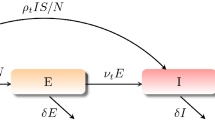
We consider this model, where the total population N = S + E + I + R (i.e., four components if added should be equal to the total population). We assume that the new individuals were a result of contacts within the susceptible group S(t). The transmission parameter β (contact rate) is giving a force of infectious λ = β(I(t)/N(t)) and the number of new infectious cases out of S(t) and into E(t) as βI(t)S(t)/N(t). The exposed persons progress to active cases in 2 weeks at a constant progression rate (k) n giving the number of individuals moving out of E(t) and into I(t) as kE(t). The infectious cases are denoted to recover at a constant rate σ. The cumulative number of recovered cases moving out of I(t) into R(t) is given by γ I(t). Given this model, we assumed the values of β, γ, and σ [20]. Jakhar et al. [20] describe for such parameters. We are assigning a basic reproduction ratio of 1.5, β to be 0.1, σ to be 0.1. Also, the γ is assumed to be 0.2 and the average infectious period is chosen to be 5 days (Fig. 1).

Relationship between each step of the SEIR model
3.3 Logistic Growth Model
This model is increased at the onset, but decreases at a later stage, as it approaches the maximum. In current COVID-19, the highest limit will be the cumulative population and the growth certainly comes down when a greater proposition of the population is infected. The reason for utilizing logistic growth modeling for the COVID-19 pandemic is that it has been proven that the epidemic grows exponentially in the early phases and then decreases in the later stages. This model is presented as \(y(t) = \frac{c}{{1 + a(e^{ - bt} )}}\) where y(t) denotes the number of individuals at any given time t, c denotes the limiting value, the maximum capacity for \(y.a = (c/y_0 ) - 1\), and “ b” is the rate of change. The number of cases at the beginning, also called the initial value, denotes \(\frac{c}{(1 + a)}\) and the maximum growth rate (t) is \(\log (a)/b\). . When y = c (the population size is maximum), y/c will be one. Hence, the (1-(y/c)) will be zero and the growth will be zero. The optimum parameter values can be obtained by nonlinear least square method.
3.4 Interrupted Time Series Multiple Regression Model
The model is the strongest, quasi-experimental tool for evaluating the longitudinal impact of interventions. The impact of immunization on the incidence of new cases and death cases was assessed using time interrupted regression analysis [21]. Figure 6 shows the diagrammatic representation and the results of the analyses are presented in Table 3.
4 Implications of Preventive Measures
This section focuses to identify the spread of the COVID-19 pandemic associated with preventive measures taken in India, such as a discussion about the impact of curfew, social distancing, and corresponding other interventions using the incidence of daily cases. Assess the death rate about the epidemic control measures performed by India's healthcare system.
4.1 Impact of Lockdown Strategy
The purpose of this study is to discuss the effect of lockdown strategy to tackle the COVID-19 outbreak. Table 2 shows the growth rate of the epidemic during the COVID-19 outbreak in India.
In addition, we discovered that there are pre- and post-lockdown measures in India. Our government announced that the curfew would begin in May 2021 during the second wave. The peak of the second wave would have arrived in mid-May 2021. Figures 3 and 4 show the complete lockdown measures based on the SEIR model.
4.2 Effects of Social Distancing Based on a Stochastic Approach
Social distancing is a key part of preventing the spread of the pandemics and it is the best form of response in managing the affected rate of COVID-19. But a large population density can make this action challenging. The study of this section is clear and discusses the effect of social distancing through a simple stochastic approach. We propose the simple Markov chain to represent the impact of social distancing on the transmission dynamics of a pandemic. Figure 2 describes how individuals can transmit between states. After becoming symptomatic, they migrate from the susceptible population to becoming infected, then to being contagious virus (shedding). They may become ill and die as a result.

Explain the Markov chain and how individuals can transmit between states after infection
We use the transition probabilities, \(s_0\)–\(s_7\) follow an Erlang distribution. This distribution is a special case of the gamma distribution, denoted as ε but scaled when various outcomes from a state are possible from Fig. 2. We observed the dynamics when individuals move from one state to another. The transition probability, \(s_0\), can be denoted through a desired basic reproduction number, \(R_0\), as it can be simply shown that
During the pandemic, Halloran defined the basic reproduction number as the average number of secondary infected individuals caused by primary cases [22]. The basic reproduction number on the day the values are implemented is used to reduce the number of people infected by each shedding or sick individual. Our study discussed the effect of social distancing rate on virus infection based an epidemiological model. We consider the constant rate ρ (0 < ρ <1), where ρ0 means perfect social distancing. But also investigate the impacts of ρ = 0.1, ρ= 0.2, and ρ = 0.3.
The capacity of the COVID-19 infection is modified as follows:
The dynamic system of differential equations, including the assumption in pandemic in India, is defined by
We used next-generation matrix method and the basic reproduction number of the model system (Eq. (1)), where,
.
The product of AB-1 is given by \(AB^{ - 1} = \left[ {\begin{array}{*{20}c} {\frac{\beta }{\gamma }} & {\frac{\beta }{\gamma }} \\ 0 & 0 \\ \end{array} } \right]\) with the spectral radius defined by
4.3 Mortality Trends
The COVID-19 pandemic becomes a serious health problem in all states in India. Maharashtra is the center of the COVID-19 virus by records. Gujarat and Telangana reported the same percentage of infected cases. Gujarat has a greater rate of deaths, and meanwhile Delhi has a lower percentage of infection cases than Karnataka, but it has a higher percentage of deaths. Mostly, the COVID-19 pandemic is infecting the male community in India, with a high affected rate of individuals between 30 and 40 years. In these, ages above 60 years are mainly reported as deaths by Joe et al. [23]. Now, we discussed the growth model of mortality trends. Also, we identify the relationship between COVID-19 death counts and population density in India through some statistical methods (see Table 4 and Fig. 7).
5 Analysis and Results
We have identified that before the implementation of the lockdown on March 2020 and the second lockdown announcement on May 2021. However, this peak has shifted to mid-August 2020 and July 2021 following the enforcement of severe countrywide lockdown. The following is an analysis of the scenario in India before and after the lockdown.
We observed from Figs. 3 and 4 the contribution of different immigration parameters during pre- and the post-lockdown pandemic situations in India. Also, we identified the effect of the lockdown strategy to tackle the COVID-19 outbreak. Here, the pre-lockdown situation is considered an as initial condition, after that the post-lockdown situation will be considered. From this study, we observed that the data is significant during the 2020 lockdown and non-significant during the 2021 lockdown. According to Table 2, the growth rate decreases after the 2020 lockdown and increases after the 2021 lockdown. According to this study, India's quarantine looks to be beneficial or effective in delaying the epidemic's peak. As a result, these findings are extremely beneficial to get time for preparedness in the healthcare system.

Pre-lockdown pandemic situation

Post-lockdown pandemic situation
5.1 Results for Effect of Social Distancing
The following figures describe the several social distancing constant rates involving, and then changes to susceptible, exposed, recovery and death trajectory.
In this study, the effect of social distancing is discussed. We represent through a constant rate ρ (0 < ρ < 1), R0 (basic reproduction number) will be determined using a stochastic approach and the value of ρ will be determined using the SEIR model. Here ρ = 0 is the perfect social distance and the value of ρ will be considered in three categories 0.1 (10%), 0.2 (20%), and 0.3 (30%) and investigated for exposed infection and recovery path (see Fig. 5).

a Shows fit the SEIR model and consider the social distancing = 10% (i.e., ρ = 0.1). b Shows fit the SEIR model and consider the social distancing = 20% (i.e., ρ = 0.2). c Shows fit the SEIR model and consider the social distancing = 30% (i.e., ρ = 0.3)
5.2 Result for Vaccination Intervention Using Time Series Multiple Regression Models
This section displays the results of the impact of the vaccine on the incidence of new cases and death cases. Then a detailed regression analysis of new incidence cases, mortality, and vaccination growth due to COVID-19 in India (Table 3).
From this section, vaccination intervention is discussed on the basis of time series multiple regression model. Here vaccine (y) is considered as dependent variable and incident cases (x1) and death cases (x2) are independent variables. The incident case coefficient values will be discussed if the vaccination increases. So, we conclude that the vaccination in 2021 is significant (see Fig. 6).

Fit the time series multiple regression model for vaccine intervention on incidents of new cases and death cases
5.3 Results for COVID-19 Mortality Trend
This result fits the growth model on death counts. We classified three phases and observed the coefficient values. Then, we observed that phases two and three were less than the first phase (see Table 4). We discovered from this study peck of death counts by the end of 2020. In addition, we investigated the impact of India's population density on the pandemic spread and mortality. After that, we observe a moderate association between the COVID-19 pandemic and population density (see Fig. 7).

Averaged death counts due to COVID-19 with population density in India
5.4 Reviews and Descriptions of Other Implications
1. The effect of public health interventions
These treatments have the impact of controlling public health problems; the main goal is to stop an outbreak from spreading and reduce the size of the epidemic. In the absence of a safe antiviral, public health initiatives, including social isolation, contact tracing, mask fabrication, effective quarantine, and travel restrictions, are used to stop and reduce outbreak pressure. Whereas public awareness of the virus and personal protection (e.g., self-isolation) has been developed. These measures guide the changes in medical seeking development and epidemiological characteristics. The differences in prediction based on different health strategies and the travel restriction effects were most significant. Also, different studies on the implications of contact tracking and self-isolation, but it was denoted that improving reporting and quarantine rates. Yue Xiang's various discussions on the implications of public health interventions are discussed above [24].
2. The economic impacts
India is a developing country and it has the second highest population with the fifth-largest economy. Kavita Singh studied the economic effects of a pandemic on people with chronic illnesses in India, focusing on underserved metropolitan areas and rural populations [19]. While the restoration of economic activity among persons infected with COVID-19 appears to be resulting in economic recovery, economic modeling indicates that the average economic value per individual life lost in the pandemic in India is 7.09–8.22 times the country's GDP per capita. Instead of a nationwide lockdown, Arora P demonstrates how a lockdown policy implemented within Indian states in the event of a pandemic can result in substantial unemployment [25].
3. The effect of policy and technology
We identified the high recovery rate from the outbreak in India as an output of significant technological impacts. The COVID-19 disease has tested the country’s epidemic preparedness in terms of its health infrastructure, interventions of policy, and communication technology. Initially, the impact of a time and one of the most strict lockdown policies was observed to reduce the spread of disease. Similarly, it used the country to prepare critical medical infrastructure, public resources, and technological advances. Isha Goel provided an overview of India's epidemiological state and highlighted the potential consequences of policy and technology changes [26].
6 Discussion
The COVID-19 pandemic has various implications for the world economy as well as for many aspects of human health, education, the physical of individuals, etc. In this study, we investigated the impact of a few factors on the healthcare system during COVID-19 as well as the illness spread related to preventive measures performed in India. In this section, the data was separated into pre-lockdown and post-lockdown: in the lockdown period implemented on the years 2020 and 2021, the infection and recovery rate paths are determined using the SEIR model. From this, the lockdown period on 2021 is significant which means that infection rate is decreased and simultaneously recovery has increased; in the lockdown period in 2021, the data is not significant which means the infection rate doesn’t change, which has been shown in Figs. 2 and 3. Next the Markov chain is used to determine the effect of social distancing. The transition probability state is applied to the death state in the population; from this the basic reproduction number (R0) value is determined with this SEIR model. The social distancing contact rate (\(\rho\)) is separated into three (0.1, 0.2, and 0.3) and using this exposed, infection, and recovery rates are analyzed. From this, we can conclude that if the social distancing percentage increases, then the infections will decrease. The infection and death rates are analyzed based on the time series multiple regression model in vaccine intervention. Using this public health intervention is discussed. The regression and coefficient values are calculated for the vaccination coverage increase and death decrease. As the death count increases after May 2021, the path is determined using the growth model; COVID-19’s mortality, population density, and impacts are also discussed. Finally, other implications and their reviews and descriptions are also discussed.
7 Conclusion
Our research found that the most effective public health intervention is to conduct screening tests as soon as possible to aid in the rapid identification of infected cases, quick treatment, and immediate isolation of susceptible cases. We also discovered that pandemic-related preventive strategies, such as social distancing, wearing masks in public places, self-hygiene, and remote working and learning, can all have a significant impact on pandemic transmission. In addition, the above-mentioned model might be used to design and prepare health systems in this study. This research provided a systematic approach to avoid recording, and controlling the spread of COVID-19.
References
Neuts, MF.: Matrix-geometric solutions in stochastic models: an algorithmic approach. Courier Corporation (1994)
Chakravarthy, S.R.: The batch Markovian arrival process: a review and future work. Adv. Probab. Theory Stoch. Process. 1, 21–49 (2001)
Briggs, A., Sculpher, M.: An introduction to Markov modeling for economic evaluation. Pharmacoeconomics 13(4), 397–409 (1998). (Apr)
Sonnenberg, FA., Beck JR.: Markov models in medical decision making: a practical guide. Medical decision making. 13(4), 322–38 (1993). (Dec)
Zhang, Y., Jiang, B., Yuan, J., Tao, Y.: The impact of social distancing and epicenter lockdown on the COVID-19 epidemic in mainland China: A data-driven SEIQR model study. MedRxiv. (1 Jan 2020)
Ozili, P.K., Arun, T.: Spillover of COVID-19: impact on the global economy. SRN 3562570. (27 Mar 2020)
Mandal, S., Bhatnagar, T., Arinaminpathy, N., Agarwal, A., Chowdhury, A, Murhekar, M., Gangakhedkar, RR., Sarkar, S.: Prudent public health intervention strategies to control the corona virus disease 2019 transmission in India: a mathematical model-based approach. Indian J. Med. Res. 151(2–3), 190 (2020). (Feb)
Bhola, J., Venkateswaran, V.R., Koul, M.: Corona epidemic in Indian context: predictive mathematical modelling. MedRxiv. https://www.medrxiv.org/content/medrxiv/early/2020/04/07/2020.04.03.20047175.full.pdf
López, L., Rodo, X.: A modified SEIR model to predict the COVID-19 outbreak in Spain and Italy: simulating control scenarios and multi-scale epidemics. Results Phys. 21, 103746 (2021). (Feb 1)
Rachah, A.: Analysis, simulation and optimal control of a SEIR model for Ebola virus with demographic effects. Commun. Fac. Sci. Univ. Ankara Ser. A1 Math. Stati. 67(1), 179–97 (2018). (Jan 1)
Hamzah, F.B., Lau, C., Nazri, H., Ligot, D.V., Lee, G., Tan, C.L., Shaib, M.K., Zaidon, U.H., Abdullah, A.B., Chung, M.H.: CoronaTracker: worldwide COVID-19 outbreak data analysis and prediction. Bull. World Health Organ. 1(32) (2020). (Mar 19)
Porter, AT.: A path-specific approach to SEIR modeling. Doctoral dissertation, The University of Iowa (2012)
Chen, TM., Rui, J., Wang, QP., Zhao, ZY., Cui, JA., Yin, L.: A mathematical model for simulating the phase-based transmissibility of a novel corona virus. Infect. Dis. Poverty 9(1), 1–8 (2020). (Dec)
Adly, H.M., AlJahdali, I.A., Garout, M.A., Khafagy, A.A., Saati, A.A., Saleh, S.A.: Correlation of COVID-19 pandemic with healthcare system response and prevention measures in Saudi Arabia. Int. J. Environ. Res. Public Health 17(18), 6666 (2020). (Jan)
Nyabadza, F., Chirove, F., Chukwu, C.W., Visaya, M.V.: Modelling the potential impact of social distancing on the COVID-19 epidemic in South Africa. Comput. Math. Methods Med. (1 Jan 2020)
Youkta, K., Paramanik, R.N.: Epidemiological model for India's COVID‐19 pandemic. J. Public Aff. e2639 (2021). (Feb 18)
Aviv-Sharon, E., Aharoni, A.: Generalized logistic growth modeling of the COVID-19 pandemic in Asia. Infect. Dis. Modell. 5, 502–9 (2020). (Jan 1)
Kumar, S.U., Kumar, D.T., Christopher, B.P., Doss, C.: The rise and impact of COVID-19 in India. Front. Med. 7, 250 (2020) (May 22)
Singh, K., Kondal, D., Mohan, S., Jaganathan, S., Deepa, M., Venkateshmurthy, N.S., Jarhyan, P., Anjana, R.M., Narayan, K.V., Mohan, V., Tandon, N.: Health, psychosocial, and economic impacts of the COVID-19 pandemic on people with chronic conditions in India: a mixed methods study. BMC Public Health 21(1), 1–5 (2021). (Dec)
Jakhar, M., Ahluwalia, P.K., Kumar, A.: COVID-19 epidemic forecast in different states of India using Sir Model. Medrxiv (1 Jan 2020)
Wagner, A.K., Soumerai, S.B., Zhang, F., Ross- Degnan, D.: Segmented regression analysis of interrupted time series studies in medication use research. J. Clin. Pharm. Herapeal. 27(4), 299–309 (2002). (14 Aug 2002)
Halloran, M.E.: Concepts of transmission and dynamics. Epidemiologic methods for the study of infectious diseases. 56, 85–96 (2001). (Mar 22)
Joe, W., Kumar, A., Rajpal, S., Mishra, U.S., Subramanian, S.V.: Equal risk, unequal burden? Gender differentials in COVID-19 mortality in India. J. Global Health Sci. 2(1) (2020). (May 14)
Xiang, Y., Jia, Y., Chen, L., Guo, L., Shu, B., Long, E.: COVID-19 epidemic prediction and the impact of public health interventions: a review of COVID-19 epidemic models. Infect. Dis. Modell. (7 Jan 2021)
Arora, P., Kumar, H., Panigrahi, B.K.: Prediction and analysis of COVID-19 positive cases using deep learning models: a descriptive case study of India. Chaos, Solitons Fractals 139, 110017 (2020)
Goel, I., Sharma, S., Kashiramka, S.: Effects of the COVID-19 pandemic in India: an analysis of policy and technological interventions. Health Policy Technol. 10(1), 151–64 (2021). (Mar 1)
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2023 The Author(s), under exclusive license to Springer Nature Singapore Pte Ltd.
About this paper

Cite this paper
Sasikumar, R., Arriyamuthu, P. (2023). Modeling for Implications of COVID-19 Pandemic on Healthcare System in India. In: Sharma, R.K., Pareschi, L., Atangana, A., Sahoo, B., Kukreja, V.K. (eds) Frontiers in Industrial and Applied Mathematics. FIAM 2021. Springer Proceedings in Mathematics & Statistics, vol 410. Springer, Singapore. https://doi.org/10.1007/978-981-19-7272-0_46
Download citation
DOI: https://doi.org/10.1007/978-981-19-7272-0_46
Published:
Publisher Name: Springer, Singapore
Print ISBN: 978-981-19-7271-3
Online ISBN: 978-981-19-7272-0
eBook Packages: Mathematics and StatisticsMathematics and Statistics (R0)