
Abstract
Goal-directed fluid therapy is the administration of fluid, vasopressors, and inotropes to optimize hemodynamic parameters for better tissue perfusion. Current practice uses cardiac output, systolic, or pulse pressure variations as the targets to follow. However, none of these measures indicate cerebral physiology. Electroencephalogram, evoked potentials, and cerebral oximetry may be used to guide fluid therapy. Nevertheless, the evidence for these monitors to improve patient outcomes remains inconclusive. There are numerous barriers in implementing goal-directed fluid therapy during anesthesia and caring for critically ill patients. Further trials should define the goals to target, and feasibility in implementing protocol. More trials are required to define the benefit and risk ratio in adopting the goal-directed fluid therapy in specific patient populations.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
- Goal-directed fluid therapy
- Cardiac output monitoring
- Pulse pressure variation
- Cerebral oximetry
- Electroencephalogram
Goal-directed fluid therapy is a concept where administration of fluid, vasopressors, and inotropes is targeted to achieve an optimal hemodynamic parameter for better tissue perfusion [1]. In high-risk surgical patients, Shoemaker and colleagues reported a lower rate of postoperative complications, fewer deaths, earlier discharge from the hospital and the intensive care unit, and shorter duration of ventilation when perioperative cardiac index and oxygen delivery were increased to >4.5 L/min/m2 and >600 ml/min/m2, respectively [2]. The extraordinary results had drawn a lot of attention, and the approach has since extrapolated to various scenarios. In this respect, goal-directed fluid therapies have been studied extensively for the treatment of critically ill patients and during major surgery. In contrast, few studies have evaluated goal-directed fluid therapy in neurosurgical patients. In this chapter, we reviewed the clinical utility of goal-directed fluid therapy in patients having neurosurgery and receiving neurocritical care.
Which Goal to Direct Therapy?
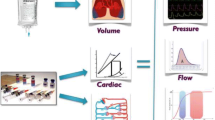
An integral part of goal-directed fluid therapy is to establish a “goal” to guide interventions. Ideally, the goal has to be clearly defined and prognostically important and can be measured accurately and noninvasively. Figure 1 shows the common parameters that have been used to gauge tissue perfusion during surgery.

Monitors for tissue perfusion
Traditional Goals
Arterial pressure is the primary determinant for driving tissue perfusion and is a standard monitor in contemporary anesthesia [3]. The major drawback of using arterial pressure is that there is no consensus on the minimum arterial pressure required to maintain organ function. In this respect, over 130 definitions on hypotension had been reported in the literature [4]. Nevertheless, multiple cohort studies, systematic reviews, and meta-analyses have shown an increased risk of postoperative adverse events with mean arterial pressure <65 mmHg or systolic arterial pressure <90 mmHg for >10 min [5,6,7,8]. In a randomized controlled trial (RCT), individualized blood pressure management with systolic arterial pressure maintained within 10% of baseline (n = 147) reduced the risk of postoperative organ dysfunction by 27% (95% confidence intervals, CI: 6–44%) compared with standard care (treating hypotension only when systolic arterial pressure was <80 mmHg, n = 145) [9]. Anesthesiologists may also monitor end-organ dysfunction using urine output, acid-base balance, and plasma lactate concentration. These measures however lack temporal resolution, require long turnover time, and tend to worsen only after significant hypoperfusion.
Cardiac Filling Pressures
Alternatively, anesthesiologists were accustomed in measuring cardiac filling pressures, such as central venous pressure and pulmonary artery occlusion pressure, to guide fluid therapy. As a measure of cardiac preload, it is assumed that an optimized filling pressure would be important to improve cardiac output and tissue perfusion. However, the absolute filling pressure is dependent on valvular pathology and ventricular compliance and is therefore a poor predictor for volume status or fluid responsiveness [10, 11].
Cardiac Output
Cardiac output is a surrogate marker of tissue oxygen delivery. Conventional measurement uses the indicator (e.g., cold saline, lithium, or indocyanine green) dilution technique, producing intermittent values, and requires insertion of invasive pulmonary artery catheter [12]. Recent technology development has allowed minimally invasive and beat-to-beat measurements of cardiac output [13, 14]. Currently, four methods are commercially available:
-
1.
Impedance cardiography
Transthoracic electrical bioimpedance (TEB) measures the resistance to a high frequency and low voltage current passing through the thorax. The rhythmic changes of impedance correspond to the variations in aortic blood volume during successive cardiac cycles. Therefore, variations in cardiac output will be reflected by the change in TEB [15]. Clearly, TEB signals are affected by electrical interference and may undermine the utility of the device.
-
2.
Doppler ultrasound
The Doppler technique measures blood flow velocity through the aortic valve and the descending thoracic aorta using suprasternal and esophageal probe, respectively [16]. Cardiac output is therefore the product of flow velocity, reference cross-sectional area, and heart rate.
-
3.
Arterial pressure waveform and pulse contour analysis
It has been long recognized that pulse pressure is directly proportional to stroke volume [17, 18]. Currently, three commercially available monitors have been developed to determine cardiac output based on arterial pulse contour. The LiDCO monitor (LiDCO, London, UK) applies the PulseCO™ algorithm to account for aortic impedance, arterial compliance, and peripheral vascular resistance in order to estimate beat-to-beat cardiac output [19, 20]. LiDCO requires regular calibration using subtherapeutic doses of lithium for dye dilution-derived cardiac output [20]. Similarly, PiCCO monitor (PULSION Medical Systems AG, Munich, Germany) uses a proprietary algorithm to analyze the systolic component of the arterial pulse [21]. Intermittent (transpulmonary) thermodilution-derived cardiac output is required for calibration. The Vigileo-FloTrac system (Edwards Lifesciences, Irvine, CA) measures cardiac output with standard arterial catheter attached special proprietary transducer. In contrast to the other monitors, FloTrac does not require additional calibration [22].
In addition, the arterial pressure waveform monitoring allows anesthesiologists to access fluid responsiveness. In this respect, variations in arterial pressure (5–10 mmHg) during respiration are normal phenomena due to the transmission of intrathoracic pressure. In spontaneously breathing patients, arterial pressure decreases with inspiration and increases with expiration. The reverse occurs in mechanical positive pressure ventilation, where pulmonary blood volume is shifted to the left ventricle during inspiration and therefore increases arterial pressure with an increase in preload. The increase in intrathoracic pressure also decreases right ventricular filling, and will decrease arterial pressure subsequently. In patients with hypovolemia, variation in arterial pressure is exaggerated, and therefore derived indices from the arterial waveform (e.g., stroke volume, systolic pressure, and pulse pressure variation) could be used to guide fluid administration (Fig. 2).
-
4.
Partial rebreathing method

Changes of arterial pressure with mechanical ventilation. Systolic pressure variation is the difference in systolic pressures at end-inspiration and end-expiration. Pulse pressure variation is the ratio between the difference and the mean of maximum and minimum pulse pressure. Red tracing, arterial pressure; blue tracing, central venous pressure; green tracing, airway pressure. Arterial, venous and airway pressure tracings courtesy of Dr. Robert Linton and Dr. Nick Linton (http://www.foxlinton.org/cardiac_output/PCOpages/spv2.html)
In this method, brief and step changes in carbon dioxide elimination is compared to the changes in end-tidal carbon dioxide tension [23]. The differential Fick method measures pulmonary blood flow and would only indicate cardiac output if the shunt fraction remains constant during the measurement period. Potentially, the technique could be integrated into anesthetic ventilator providing automated breath-to-breath cardiac output readings [24].
Measures of Cerebral Physiology
It should be noted that all the aforementioned technology measure systematic perfusion, and do not indicate cerebral physiology. Nevertheless, several modalities have been developed to measure cerebral hemodynamics, oxygenation, and electrophysiology (Table 1) [25], majority are designed for monitoring head-injured patients.
-
1.
Intracranial pressure
Intracranial pressure (ICP) can be measured by inserting a catheter into the ventricles, at the subdural or epidural spaces. In addition, a fiber-optic sensor could be inserted to measure the parenchymal ICP [26]. There are risks associated with ICP monitoring. The reported rate for bleeding and infection ranged from 0.5–2% to 1–5%, respectively [27]. Nevertheless, ICP monitoring has been commonly used in the management of severe head injury [28, 29]. It remains difficult to decide on the ICP threshold that will require treatment. In the Benchmark Evidence from South American Trials: Treatment of Intracranial Pressure (BEST:TRIP) trial, strategies aiming to maintain ICP <20 mmHg in severe traumatic brain-injured patients did not improve 6-month mortality, functional, and cognitive performance [30].
-
2.
Cerebral blood flow
Measurement of global cerebral blood flow (CBF) requires imaging technique (e.g., xenon CT). However, regional CBF could be determined by using bedside transcranial Doppler. This is a measure of flow velocity, and the measurement is operator dependent, requiring appropriate acoustic bone window and specific mounting devices for continuous monitoring. Nonetheless, cerebral blood flow velocity has been used to determine cerebrovascular reactivity of the major cerebral vessels, for adjusting lung ventilation and arterial pressure targets during the management of head-injured patients [31]. In addition, transcranial Doppler can be used to detect vasospasm and hyperemia (Table 1). In carotid endarterectomy, the Doppler signal can be used to detect microemboli during arterial clamp release [32, 33]. However, it is unclear what might be the optimal CBF flow velocity to target.
-
3.
Cerebral oxygenation
Global cerebral oxygenation could be determined by sampling of the venous blood drained to the dominant (90% right sided) jugular bulb [34]. A decrease in jugular venous oxygen saturation < 50% is thought to indicate brain ischemia. However, this measurement lacks spatial resolution. Several companies have since produced noninvasive cerebral oximeter that measures regional cerebral oxygenation using electromagnetic radiation (e.g., near-infrared) [35]. It should be noted that cerebral oxygenation is a relative measurement. Furthermore, the commercially available cerebral oximeters use different algorithms and the readings cannot be directly compared. Others have inserted a parenchymal probe with a Clark electrode to measure tissue oxygen tension. Tissue oxygen tension <20 mmHg is generally considered as critical [36].
-
4.
Cerebral biochemistry
Cerebral hypoxia and ischemia lead to anaerobic metabolism, cellular damage, and release of excitatory amino acids. This will lead to a depletion of glucose store and an increase in lactate, lactate-to-pyruvate ratio, glutamate, and glycerol concentrations. By inserting a microdialysis catheter into the brain, it is possible to measure the concentrations of these metabolites and to gauge the extent of cerebral insult within a small brain region [37]. There are, however, no consensus on the thresholds to intervene. Nevertheless, cerebral microdialysis helps clinicians to understand the pathophysiology associated with brain injury and has been used as a surrogate marker for evaluation of new drugs for neuroprotection [38, 39].
Goal-Directed Algorithms
After establishing the goal of interest, the next step is to design an algorithm so that appropriate treatments can be implemented to achieve these goals. Hemodynamic goals (e.g., arterial pressure, cardiac output, pulse pressure variation) are commonly managed with fluid challenges including a combination of colloid or crystalloid. In a systematic review and meta-analysis of 24 RCTs on goal-directed fluid therapy in patients having major surgery (n = 3861), intraoperative use of colloid was significantly higher in the goal-directed group compared with controls, mean difference (95% CI): 467 (331–603) ml [40]. In addition, the administration of vasopressors or inotropes is getting popular to achieve these goals (Fig. 3).

Typical algorithm of goal-directed therapy using systolic pressure variation (SPV) and pulse pressure variation (PPV) in patients receiving general anesthesia with mechanical ventilation
In the management of neurocritical care patients, other measures, such as supplemental oxygen, hyperventilation, hypothermia, pentobarbital coma, osmotic therapy, and anticonvulsant, are used to achieve the goals (Fig. 4) [41].

Treatment algorithm (adopted from the Seattle International Severe Traumatic Brain Injury Consensus Conference) for patients with severe brain injury guided by intracranial pressure monitoring [41]. Patients who did not respond will require higher tier of treatments. MAP mean arterial pressure, CPP cerebral perfusion pressure, SpO2 arterial oxygen saturation, Hb hemoglobin, PaCO2 arterial partial pressure of carbon dioxide, ICP intracranial pressure, EVD external ventricular drain, EEG electroencephalogram, [Na] plasma sodium concentration, CT computed tomography
Outcomes of Goal-Directed Therapy
Targeting Hemodynamic Variables
Using the hemodynamic targets, >100 studies have evaluated the effectiveness of goal-directed fluid therapy to improve outcomes after surgery [42]. There were also >20 systematic reviews and meta-analyses summarizing these results. Using different combinations of studies on various outcomes, these analyses showed that goal-directed fluid therapy reduced rates of postoperative ileus [43,44,45,46], sepsis or infection [47,48,49], postoperative cardiovascular complications [50, 51], renal failure [48], or any complications [46, 52, 53]. Goal-directed fluid therapy also reduced hospital stay and duration of intensive care unit admission [45, 54,55,56,57], and there was a decrease in hospital or 30-day mortality, compared with controls in noncardiac surgery [58,59,60,61]. In cardiac surgery, overall complication rate and hospital stay were reduced with goal-directed fluid therapy [62]. Other meta-analyses, however, demonstrated no difference between groups [48, 53, 63,64,65,66,67,68,69,70]. Only few trials had studied goal-directed fluid therapy in neurosurgery [71,72,73,74]. Three trials had studied craniotomy [71,72,73] and one on spine surgery [74]. Only two trials reported postoperative outcomes [71, 72]. With limited sample size (total 208 patients), goal-directed fluid therapy reduced a composite of complications (sepsis, stroke, renal impairment, and all-cause mortality), 17% vs 35%, odds ratio (95% CI): 0.38 (0.20–0.73), p = 0.004, I2 = 0.0%.
Nevertheless, in an attempt to pool all 110 trials, Kaufmann and co-workers report large amount of heterogeneity, and it was not possible to perform meta-analysis. Furthermore, the results were sensitive to the studies included, sample size of individual trial [median (interquartile range) size = 40 [30,31,32,33,34,35,36,37,38,39,40,41,42,43,44,45,46,47,48,49,50,51,52,53,54,55,56,57,58,59,60,61,62,63,64] patients per group], monitors or targets chosen, and analytical methods used. Clearly, a large RCT is required to resolve the controversy whether target-guided therapy will improve postoperative outcomes [75, 76]. Two trials are currently ongoing. The FLuid Optimisation in Emergency LAparotomy (FLO-ELA) trial will randomize 7646 patients, ≥50 years to have anesthesia guided by stroke volume variation or control (ISRCTN14729158). Similarly, the OPtimisation of Peri-operaTive Cardiovascular Management to Improve Surgical outcomE II (OPTIMISE II) trial recruits 2502 patients having elective gastrointestinal surgery [77]. OPTIMISE II trial compares 30-day infection in patients receiving fluid and low-dose inotropes (dobutamine or dopexamine) to achieve the targeted stroke volume variation or usual care. The results will inform the role of hemodynamic-guided target therapy on postoperative outcomes.
Targeting Cerebral Variables
Electroencephalogram (EEG) is the commonest cerebral monitor during surgery. EEG-guided anesthesia is thought to be useful in avoiding excessive anesthetic administration and may improve postoperative outcomes. Several trials have evaluated the effect of EEG monitoring in reducing postoperative deaths. The Perioperative Quality Initiative (POQI)-6 conference gathered a number of international, multidisciplinary experts to review the literature on the clinical utility of EEG [78]. In nine trials (ten publications [79,80,81,82,83,84,85,86,87,88,89], n = 8512) that examined postoperative mortality, EEG-guided anesthesia did not reduce all-cause death rate, 14.1% vs 15.1%, relative risk (95%CI): 0.95 (0.80–1.12), P = 0.528, I2 = 38.4%. Since this systematic review, another large RCT was published. The Balanced Anesthesia trial randomized 6644 patients to receive deep or light anesthesia based on bispectral index (BIS) EEG monitoring. The death rate at 1 year after surgery in the deep anesthesia group (7.2%) was not different from the light anesthesia group (6.4%), p = 0.223. Figure 5 shows the updated meta-analysis. In 15,156 patients, the pooled relative risk (95%CI) was 0.94 (0.82–1.07), p = 0.339, I2 = 32.79%.

Forest plots of trials comparing the risk for long-term mortality after surgery in patients receiving EEG-guided or routine care anesthesia. *Patients in the control group received deeper anesthesia; CI, confidence interval; EEG, electroencephalogram; ENGAGES, Electroencephalography Guidance of Anesthesia to Alleviate Geriatric Syndromes; STRIDE, A Strategy to Reduce the Incidence of Postoperative Delirium in Elderly Patients
Alternatively, anesthesiologists have used cerebral oximetry to guide anesthetic administration. In a systematic review and meta-analysis of 15 trials (n = 1822), there was no convincing evidence that monitoring improved outcomes, primarily related to the lack of events [35, 90]. Nevertheless, cerebral oximetry monitoring might improve cognitive performance at 1 week after surgery and reduce intensive care unit stay by 5.5–6.9 h (n = 379) [90].
The effect of goal-directed fluid therapy for the management of patients requiring neurocritical care remains less well defined [25]. Majority of the current guidelines recommend multimodality monitoring including ICP, cerebral autoregulation, oximetry, and intracerebral microdialysis [28, 29, 91, 92]. Nevertheless, the quality of evidence underlying these recommendations was low. Majority studies reported association and did not demonstrate causal relationship between goal-directed therapy and outcomes in neurocritical care patients. In particular, it is unclear what would be the minimum monitoring required and the targets that should be adopted (Table 1). Further outcome trials would be required before goal-directed fluid therapy could be widely adopted.
Conclusions
There are numerous barriers in implementing goal-directed fluid therapy during anesthesia and caring for critically ill patients. Further trials should define the goals to target, and feasibility in implementing protocol. Large RCTs are required to define the benefit and risk ratio in adopting the goal-directed fluid therapy in specific patient populations.
References
O'Neal JB, Shaw AD. Goal-directed therapy: what we know and what we need to know. Perioper Med (Lond). 2015;4:1.
Shoemaker WC, Appel PL, Kram HB, Waxman K, Lee TS. Prospective trial of supranormal values of survivors as therapeutic goals in high-risk surgical patients. Chest. 1988;94:1176–86.
Gelb AW, Morriss WW, Johnson W, Merry AF. International Standards for a Safe Practice of Anesthesia Workgroup: World Health Organization-World Federation of Societies of Anaesthesiologists (WHO-WFSA) International Standards for a Safe Practice of Anesthesia. Can J Anaesth. 2018;65:698–708.
Bijker JB, van Klei WA, Kappen TH, van Wolfswinkel L, Moons KG, Kalkman CJ. Incidence of intraoperative hypotension as a function of the chosen definition: literature definitions applied to a retrospective cohort using automated data collection. Anesthesiology. 2007;107:213–20.
Wijnberge M, Schenk J, Bulle E, Vlaar AP, Maheshwari K, Hollmann MW, Binnekade JM, Geerts BF, Veelo DP. Association of intraoperative hypotension with postoperative morbidity and mortality: systematic review and meta-analysis. BJS Open. 2021;5:zraa018.
Wesselink EM, Kappen TH, Torn HM, Slooter AJC, van Klei WA. Intraoperative hypotension and the risk of postoperative adverse outcomes: a systematic review. Br J Anaesth. 2018;121:706–21.
Hallqvist L, Granath F, Fored M, Bell M. Intraoperative hypotension and myocardial infarction development among high-risk patients undergoing noncardiac surgery: a nested case-control study. Anesth Analg. 2021;133:6–15. https://doi.org/10.1213/ANE.0000000000005391.
Roshanov PS, Sheth T, Duceppe E, Tandon V, Bessissow A, Chan MTV, Butler C, Chow BJW, Khan JS, Devereaux PJ. Relationship between perioperative hypotension and perioperative cardiovascular events in patients with coronary artery disease undergoing major noncardiac surgery. Anesthesiology. 2019;130:756–66.
Futier E, Lefrant JY, Guinot PG, Godet T, Lorne E, Cuvillon P, Bertran S, Leone M, Pastene B, Piriou V, Molliex S, Albanese J, Julia JM, Tavernier B, Imhoff E, Bazin JE, Constantin JM, Pereira B, Jaber S. INPRESS study group: effect of individualized vs standard blood pressure management strategies on postoperative organ dysfunction among high-risk patients undergoing major surgery: a randomized clinical trial. JAMA. 2017;318:1346–57.
Marik PE, Baram M, Vahid B. Does central venous pressure predict fluid responsiveness? A systematic review of the literature and the tale of seven mares. Chest. 2008;134:172–8.
Shippy CR, Appel PL, Shoemaker WC. Reliability of clinical monitoring to assess blood volume in critically ill patients. Crit Care Med. 1984;12:107–12.
Argueta EE, Paniagua D. Thermodilution cardiac output: a concept over 250 years in the making. Cardiol Rev. 2019;27:138–44.
Drummond KE, Murphy E. Minimally invasive cardiac output monitors. Continuing Education in Anaesthesia Critical Care & Pain. 2011;12:5–10.
Joosten A, Desebbe O, Suehiro K, Murphy LS, Essiet M, Alexander B, Fischer MO, Barvais L, Van Obbergh L, Maucort-Boulch D, Cannesson M. Accuracy and precision of non-invasive cardiac output monitoring devices in perioperative medicine: a systematic review and meta-analysis dagger. Br J Anaesth. 2017;118:298–310.
Sanders M, Servaas S, Slagt C. Accuracy and precision of non-invasive cardiac output monitoring by electrical cardiometry: a systematic review and meta-analysis. J Clin Monit Comput. 2020;34:433–60.
Pinto BB, Atlas G, Geerts BF, Bendjelid K. The use of the oesophageal Doppler in perioperative medicine: new opportunities in research and clinical practice. J Clin Monit Comput. 2017;31:895–902.
Westerhof N, Lankhaar J-W, Westerhof BE. The arterial Windkessel. Med Biol Eng Comput. 2009;47:131–41.
Frank O. The basic shape of the arterial pulse. First treatise: mathematical analysis. 1899. J Mol Cell Cardiol. 1990;22:255–77.
Linton NW, Linton RA. Estimation of changes in cardiac output from the arterial blood pressure waveform in the upper limb. Br J Anaesth. 2001;86:486–96.
Jonas MM, Tanser SJ. Lithium dilution measurement of cardiac output and arterial pulse waveform analysis: an indicator dilution calibrated beat-by-beat system for continuous estimation of cardiac output. Curr Opin Crit Care. 2002;8:257–61.
Laight NS, Levin AI. Transcardiopulmonary thermodilution-calibrated arterial waveform analysis: a primer for anesthesiologists and intensivists. J Cardiothorac Vasc Anesth. 2015;29:1051–64.
Suehiro K, Tanaka K, Matsuura T, Funao T, Yamada T, Mori T, Nishikawa K. The Vigileo-FloTrac system: arterial waveform analysis for measuring cardiac output and predicting fluid responsiveness: a clinical review. J Cardiothorac Vasc Anesth. 2014;28:1361–74.
Peyton PJ, Kozub M. Performance of a second generation pulmonary capnotracking system for continuous monitoring of cardiac output. J Clin Monit Comput. 2018;32:1057–64.
Peyton PJ, Wallin M, Hallbäck M. New generation continuous cardiac output monitoring from carbon dioxide elimination. BMC Anesthesiol. 2019;19:28.
Smith M. Multimodality neuromonitoring in adult traumatic brain injury: a narrative review. Anesthesiology. 2018;128:401–15.
Le Roux P. In: Laskowitz D, Grant G, editors. Intracranial pressure monitoring and management, translational research in traumatic brain injury. Boca Raton (FL): CRC Press/Taylor and Francis Group; 2016.
Tavakoli S, Peitz G, Ares W, Hafeez S, Grandhi R. Complications of invasive intracranial pressure monitoring devices in neurocritical care. Neurosurgical Focus FOC. 2017;43:E6.
Picetti E, Rossi S, Abu-Zidan FM, Ansaloni L, Armonda R, Baiocchi GL, Bala M, Balogh ZJ, Berardino M, Biffl WL, Bouzat P, Buki A, Ceresoli M, Chesnut RM, Chiara O, Citerio G, Coccolini F, Coimbra R, Di Saverio S, Fraga GP, Gupta D, Helbok R, Hutchinson PJ, Kirkpatrick AW, Kinoshita T, Kluger Y, Leppaniemi A, AIR M, Maier RV, Minardi F, Moore EE, Myburgh JA, Okonkwo DO, Otomo Y, Rizoli S, Rubiano AM, Sahuquillo J, Sartelli M, Scalea TM, Servadei F, Stahel PF, Stocchetti N, Taccone FS, Tonetti T, Velmahos G, Weber D, Catena F. WSES consensus conference guidelines: monitoring and management of severe adult traumatic brain injury patients with polytrauma in the first 24 hours. World J Emerg Surg. 2019;14:53.
Carney N, Totten AM, O'Reilly C, Ullman JS, Hawryluk GW, Bell MJ, Bratton SL, Chesnut R, Harris OA, Kissoon N, Rubiano AM, Shutter L, Tasker RC, Vavilala MS, Wilberger J, Wright DW, Ghajar J. Guidelines for the management of severe traumatic brain injury, fourth edition. Neurosurgery. 2017;80:6–15.
Chesnut RM, Temkin N, Carney N, Dikmen S, Rondina C, Videtta W, Petroni G, Lujan S, Pridgeon J, Barber J, Machamer J, Chaddock K, Celix JM, Cherner M, Hendrix T. Global Neurotrauma Research Group: a trial of intracranial-pressure monitoring in traumatic brain injury. N Engl J Med. 2012;367:2471–81.
Zeiler FA, Ercole A, Czosnyka M, Smielewski P, Hawryluk G, Hutchinson PJA, Menon DK, Aries M. Continuous cerebrovascular reactivity monitoring in moderate/severe traumatic brain injury: a narrative review of advances in neurocritical care. Br J Anaesth. 2020;S0007-0912:30966–3.
Robba C, Taccone FS. How i use transcranial doppler. Crit Care. 2019;23:420.
Chan MT, Lam JM. New monitors for neurological functions: part 1. Curr Anaesth Crit Care. 1999;10:87–97.
Chan MT, Lam JM. New monitors for neurological functions: part 2. Curr Anaesth Crit Care. 1999;10:147–57.
Thiele RH, Shaw AD, Bartels K, Brown CH IV, Grocott H, Heringlake M, Gan TJ, Miller TE, McEvoy MD. American Society for Enhanced Recovery and Perioperative Quality Initiative Joint Consensus Statement on the role of neuromonitoring in perioperative outcomes: cerebral near-infrared spectroscopy. Anesth Analg. 2020;131:1444–55.
Le Roux PD, Oddo M. Parenchymal brain oxygen monitoring in the neurocritical care unit. Neurosurg Clin N Am. 2013;24:427–39.
Tasneem N, Samaniego EA, Pieper C, Leira EC, Adams HP, Hasan D, Ortega-Gutierrez S. Brain multimodality monitoring: a new tool in neurocritical care of comatose patients. Crit Care Res Pract. 2017;2017:6097265.
Carteron L, Bouzat P, Oddo M. Cerebral microdialysis monitoring to improve individualized neurointensive care therapy: an update of recent clinical data. Front Neurol. 2017;8:601.
Zeiler FA, Thelin EP, Helmy A, Czosnyka M, Hutchinson PJA, Menon DK. A systematic review of cerebral microdialysis and outcomes in TBI: relationships to patient functional outcome, neurophysiologic measures, and tissue outcome. Acta Neurochir. 2017;159:2245–73.
Corcoran T, Rhodes JE, Clarke S, Myles PS, Ho KM. Perioperative fluid management strategies in major surgery: a stratified meta-analysis. Anesth Analg. 2012;114:640–51.
GWJ H, Aguilera S, Buki A, Bulger E, Citerio G, Cooper DJ, Arrastia RD, Diringer M, Figaji A, Gao G, Geocadin R, Ghajar J, Harris O, Hoffer A, Hutchinson P, Joseph M, Kitagawa R, Manley G, Mayer S, Menon DK, Meyfroidt G, Michael DB, Oddo M, Okonkwo D, Patel M, Robertson C, Rosenfeld JV, Rubiano AM, Sahuquillo J, Servadei F, Shutter L, Stein D, Stocchetti N, Taccone FS, Timmons S, Tsai E, Ullman JS, Vespa P, Videtta W, Wright DW, Zammit C, Chesnut RM. A management algorithm for patients with intracranial pressure monitoring: the Seattle International Severe Traumatic Brain Injury Consensus Conference (SIBICC). Intensive Care Med. 2019;45:1783–94.
Kaufmann T, Clement RP, Scheeren TWL, Saugel B, Keus F, van der Horst ICC. Perioperative goal-directed therapy: a systematic review without meta-analysis. Acta Anaesthesiol Scand. 2018;62:1340–55.
Giglio MT, Marucci M, Testini M, Brienza N. Goal-directed haemodynamic therapy and gastrointestinal complications in major surgery: a meta-analysis of randomized controlled trials. Br J Anaesth. 2009;103:637–46.
Gómez-Izquierdo JC, Feldman LS, Carli F, Baldini G. Meta-analysis of the effect of goal-directed therapy on bowel function after abdominal surgery. Br J Surg. 2015;102:577–89.
Sun Y, Chai F, Pan C, Romeiser JL, Gan TJ. Effect of perioperative goal-directed hemodynamic therapy on postoperative recovery following major abdominal surgery-a systematic review and meta-analysis of randomized controlled trials. Crit Care. 2017;21:141.
Xu C, Peng J, Liu S, Huang Y, Guo X, Xiao H, Qi D. Goal-directed fluid therapy versus conventional fluid therapy in colorectal surgery: A meta analysis of randomized controlled trials. Int J Surg. 2018;56:264–73.
Dalfino L, Giglio MT, Puntillo F, Marucci M, Brienza N. Haemodynamic goal-directed therapy and postoperative infections: earlier is better. A systematic review and meta-analysis Crit Care. 2011;15:R154.
Grocott MP, Dushianthan A, Hamilton MA, Mythen MG, Harrison D, Rowan K. Optimisation Systematic Review Steering Group: perioperative increase in global blood flow to explicit defined goals and outcomes following surgery. Cochrane Database Syst Rev. 2012;11:CD004082.
Yuan J, Sun Y, Pan C, Li T. Goal-directed fluid therapy for reducing risk of surgical site infections following abdominal surgery - a systematic review and meta-analysis of randomized controlled trials. Int J Surg. 2017;39:74–87.
Giglio M, Dalfino L, Puntillo F, Rubino G, Marucci M, Brienza N. Haemodynamic goal-directed therapy in cardiac and vascular surgery. A systematic review and meta-analysis. Interact Cardiovasc Thorac Surg. 2012;15:878–87.
Arulkumaran N, Corredor C, Hamilton MA, Ball J, Grounds RM, Rhodes A, Cecconi M. Cardiac complications associated with goal-directed therapy in high-risk surgical patients: a meta-analysis. Br J Anaesth. 2014;112:648–59.
Ripolles-Melchor J, Casans-Frances R, Espinosa A, Abad-Gurumeta A, Feldheiser A, Lopez-Timoneda F, Calvo-Vecino JM, Ear Group EARG. Goal directed hemodynamic therapy based in esophageal Doppler flow parameters: a systematic review, meta-analysis and trial sequential analysis. Rev Esp Anestesiol Reanim. 2016;63:384–405.
Ripolles J, Espinosa A, Martinez-Hurtado E, Abad-Gurumeta A, Casans-Frances R, Fernandez-Perez C, Lopez-Timoneda F, Calvo-Vecino JM, Group EAR. Intraoperative goal directed hemodynamic therapy in noncardiac surgery: a systematic review and meta-analysis. Braz J Anesthesiol. 2016;66:513–28.
Berger MM, Gradwohl-Matis I, Brunauer A, Ulmer H, Dunser MW. Targets of perioperative fluid therapy and their effects on postoperative outcome: a systematic review and meta-analysis. Minerva Anestesiol. 2015;81:794–808.
Benes J, Giglio M, Brienza N, Michard F. The effects of goal-directed fluid therapy based on dynamic parameters on post-surgical outcome: a meta-analysis of randomized controlled trials. Crit Care. 2014;18:584.
Li P, Qu LP, Qi D, Shen B, Wang YM, Xu JR, Jiang WH, Zhang H, Ding XQ, Teng J. Significance of perioperative goal-directed hemodynamic approach in preventing postoperative complications in patients after cardiac surgery: a meta-analysis and systematic review. Ann Med. 2017;49:343–51.
Feng S, Yang S, Xiao W, Wang X, Yang K, Wang T. Effects of perioperative goal-directed fluid therapy combined with the application of alpha-1 adrenergic agonists on postoperative outcomes: a systematic review and meta-analysis. BMC Anesthesiol. 2018;18:113.
Ripolles-Melchor J, Espinosa A, Martinez-Hurtado E, Abad-Gurumeta A, Casans-Frances R, Fernandez-Perez C, Lopez-Timoneda F, Calvo-Vecino JM. Perioperative goal-directed hemodynamic therapy in noncardiac surgery: a systematic review and meta-analysis. J Clin Anesth. 2016;28:105–15.
Rollins KE, Lobo DN. Intraoperative goal-directed fluid therapy in elective major abdominal surgery: a meta-analysis of randomized controlled trials. Ann Surg. 2016;263:465–76.
Giglio M, Manca F, Dalfino L, Brienza N. Perioperative hemodynamic goal-directed therapy and mortality: a systematic review and meta-analysis with meta-regression. Minerva Anestesiol. 2016;82:1199–213.
Michard F, Giglio MT, Brienza N. Perioperative goal-directed therapy with uncalibrated pulse contour methods: impact on fluid management and postoperative outcome. Br J Anaesth. 2017;119:22–30.
Aya HD, Cecconi M, Hamilton M, Rhodes A. Goal-directed therapy in cardiac surgery: a systematic review and meta-analysis. Br J Anaesth. 2013;110:510–7.
Ripolles J, Espinosa A, Casans R, Tirado A, Abad A, Fernandez C, Calvo J. Colloids versus crystalloids in objective-guided fluid therapy, systematic review and meta-analysis. Too early or too late to draw conclusions. Braz J Anesthesiol. 2015;65:281–91.
Watt DG, McSorley ST, Horgan PG, McMillan DC. Enhanced recovery after surgery: which components, if any, impact on the systemic inflammatory response following colorectal surgery?: a systematic review. Medicine (Baltimore). 2015;94:e1286.
van der Zee EN, Egal M, Gommers D, Groeneveld AB. Targeting urine output and 30-day mortality in goal-directed therapy: a systematic review with meta-analysis and meta-regression. BMC Anesthesiol. 2017;17:22.
Chong MA, Wang Y, Berbenetz NM, McConachie I. Does goal-directed haemodynamic and fluid therapy improve peri-operative outcomes?: a systematic review and meta-analysis. Eur J Anaesthesiol. 2018;35:469–83.
Zhang X, Zheng W, Chen C, Kang X, Zheng Y, Bao F, Gan S, Zhu S. Goal-directed fluid therapy does not reduce postoperative ileus in gastrointestinal surgery: a meta-analysis of randomized controlled trials. Medicine (Baltimore). 2018;97:e13097.
Rollins KE, Mathias NC, Lobo DN. Meta-analysis of goal-directed fluid therapy using transoesophageal Doppler monitoring in patients undergoing elective colorectal surgery. BJS Open. 2019;3:606–16.
Tyagi A, Maitra S, Bhattacharjee S. Comparison of colloid and crystalloid using goal-directed fluid therapy protocol in non-cardiac surgery: a meta-analysis of randomized controlled trials. J Anesth. 2020;34:865–75.
Pearse RM, Harrison DA, MacDonald N, Gillies MA, Blunt M, Ackland G, Grocott MP, Ahern A, Griggs K, Scott R, Hinds C, Rowan K, Group OS. Effect of a perioperative, cardiac output-guided hemodynamic therapy algorithm on outcomes following major gastrointestinal surgery: a randomized clinical trial and systematic review. JAMA. 2014;311:2181–90.
Luo J, Xue J, Liu J, Liu B, Liu L, Chen G. Goal-directed fluid restriction during brain surgery: a prospective randomized controlled trial. Ann Intensive Care. 2017;7:16.
Wu J, Ma YH, Wang TL, Xu G, Fan L, Zhang Y. Goal-directed fluid management based on the auto-calibrated arterial pressure-derived stroke volume variation in patients undergoing supratentorial neoplasms surgery. Int J Clin Exp Med. 2017;10:3106–14.
Hasanin A, Zanata T, Osman S, Abdelwahab Y, Samer R, Mahmoud M, Elsherbiny M, Elshafaei K, Morsy F, Omran A. Pulse pressure variation-guided fluid therapy during supratentorial brain tumour excision: a randomized controlled trial. Open Access Maced J Med Sci. 2019;7:2474–9.
Picard J, Bedague D, Bouzat P, Ollinet C, Albaladejo P, Bosson JL, Payen JF. Oesophageal Doppler to optimize intraoperative haemodynamics during prone position. A randomized controlled trial. Anaesth Crit Care Pain Med. 2016;35:255–60.
Biais M, Pearse R. Perioperative haemodynamic therapy: why are recommendations not being adopted? Anaesth Crit Care Pain Med. 2019;38:5–7.
MacDonald N, Pearse RM. Peri-operative hemodynamic therapy: only large clinical trials can resolve our uncertainty. Crit Care. 2011;15:122.
Edwards MR, Forbes G, MacDonald N, Berdunov V, Mihaylova B, Dias P, Thomson A, Grocott MP, Mythen MG, Gillies MA, Sander M, Phan TD, Evered L, Wijeysundera DN, SA MC, Aldecoa C, Ripolles-Melchor J, Hofer CK, Abukhudair H, Szczeklik W, Grigoras I, Hajjar LA, Kahan BC, Pearse RM. OPTIMISE II Investigators: optimisation of Perioperative Cardiovascular Management to Improve Surgical Outcome II (OPTIMISE II) trial: study protocol for a multicentre international trial of cardiac output-guided fluid therapy with low-dose inotrope infusion compared with usual care in patients undergoing major elective gastrointestinal surgery. BMJ Open. 2019;9:e023455.
Chan MTV, Hedrick TL, Egan TD, Garcia PS, Koch S, Purdon PL, Ramsay MA, Miller TE, McEvoy MD, Gan TJ. Perioperative Quality Initiative W: American Society for Enhanced Recovery and Perioperative Quality Initiative Joint Consensus Statement on the role of neuromonitoring in perioperative outcomes: electroencephalography. Anesth Analg. 2020;130:1278–91.
Leslie K, Myles PS, Forbes A, Chan MTV. The effect of bispectral index monitoring on long-term survival in the B-aware trial. Anesth Analg. 2010;110:816–22.
Kertai MD, Pal N, Palanca BJ, Lin N, Searleman SA, Zhang L, Burnside BA, Finkel KJ, Avidan MS. Association of perioperative risk factors and cumulative duration of low bispectral index with intermediate-term mortality after cardiac surgery in the B-Unaware Trial. Anesthesiology. 2010;112:1116–27.
Kertai MD, Palanca BJ, Pal N, Burnside BA, Zhang L, Sadiq F, Finkel KJ, Avidan MS. Bispectral index monitoring, duration of bispectral index below 45, patient risk factors, and intermediate-term mortality after noncardiac surgery in the B-Unaware trial. Anesthesiology. 2011;114:545–56.
Abdelmalak BB, Bonilla A, Mascha EJ, Maheshwari A, Tang WH, You J, Ramachandran M, Kirkova Y, Clair D, Walsh RM, Kurz A, Sessler DI. Dexamethasone, light anaesthesia, and tight glucose control (DeLiT) randomized controlled trial. Br J Anaesth. 2013;111:209–21.
Chan MT, Cheng BC, Lee TM, Gin T. CODA Trial Group: BIS-guided anesthesia decreases postoperative delirium and cognitive decline. J Neurosurg Anesthesiol. 2013;25:33–42.
Radtke FM, Franck M, Lendner J, Kruger S, Wernecke KD, Spies CD. Monitoring depth of anaesthesia in a randomized trial decreases the rate of postoperative delirium but not postoperative cognitive dysfunction. Br J Anaesth. 2013;110(Suppl 1):i98–105.
Brown CH IV, Azman AS, Gottschalk A, Mears SC, Sieber FE. Sedation depth during spinal anesthesia and survival in elderly patients undergoing hip fracture repair. Anesth Analg. 2014;118:977–80.
Short TG, Leslie K, Campbell D, Chan MT, Corcoran T, O'Loughlin E, Frampton C, Myles P. A pilot study for a prospective, randomized, double-blind trial of the influence of anesthetic depth on long-term outcome. Anesth Analg. 2014;118:981–6.
Sieber FE, Neufeld KJ, Gottschalk A, Bigelow GE, Oh ES, Rosenberg PB, Mears SC, Stewart KJ, Ouanes JP, Jaberi M, Hasenboehler EA, Li T, Wang NY. Effect of depth of sedation in older patients undergoing hip fracture repair on postoperative delirium: the STRIDE randomized clinical trial. JAMA Surg. 2018;153:987–95.
Wildes TS, Mickle AM, Ben Abdallah A, Maybrier HR, Oberhaus J, Budelier TP, Kronzer A, SL MK, Park D, Torres BA, Graetz TJ, Emmert DA, Palanca BJ, Goswami S, Jordan K, Lin N, Fritz BA, Stevens TW, Jacobsohn E, Schmitt EM, Inouye SK, Stark S, Lenze EJ, Avidan MS, ENGAGES Research Group. Effect of electroencephalography-guided anesthetic administration on postoperative delirium among older adults undergoing major surgery: the ENGAGES randomized clinical trial. J Am Med Assoc. 2019;321:473–83.
Short TG, Campbell D, Frampton C, Chan MTV, Myles PS, Corcoran TB, Sessler DI, Mills GH, Cata JP, Painter T, Byrne K, Han R, Chu MHM, McAllister DJ, Leslie K, Australian and New Zealand College of Anaesthetists Clinical Trials Network, Balanced Anaesthesia Study Group. Anaesthetic depth and complications after major surgery: an international, randomised controlled trial. Lancet. 2019;394:1907–14.
Yu Y, Zhang K, Zhang L, Zong H, Meng L, Han R. Cerebral near-infrared spectroscopy (NIRS) for perioperative monitoring of brain oxygenation in children and adults. Cochrane Database Syst Rev. 2018;1:CD010947.
Ruhatiya RS, Adukia SA, Manjunath RB, Maheshwarappa HM. Current Status and Recommendations in Multimodal Neuromonitoring. Indian J Crit Care Med. 2020;24:353–60.
Le Roux P, Menon DK, Citerio G, Vespa P, Bader MK, Brophy GM, Diringer MN, Stocchetti N, Videtta W, Armonda R, Badjatia N, Boesel J, Chesnut R, Chou S, Claassen J, Czosnyka M, De Georgia M, Figaji A, Fugate J, Helbok R, Horowitz D, Hutchinson P, Kumar M, McNett M, Miller C, Naidech A, Oddo M, Olson D, O'Phelan K, Provencio JJ, Puppo C, Riker R, Robertson C, Schmidt M, Taccone F, Neurocritical Care S, European Society of Intensive Care M. Consensus summary statement of the International Multidisciplinary Consensus Conference on Multimodality Monitoring in Neurocritical Care : a statement for healthcare professionals from the Neurocritical Care Society and the European Society of Intensive Care Medicine. Intensive Care Med. 2014;40:1189–209.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2022 The Author(s), under exclusive license to Springer Nature Singapore Pte Ltd.
About this chapter

Cite this chapter
Chan, M.T.V., Chan, C.S. (2022). Goal-Directed Fluid Therapy. In: Prabhakar, H., S Tandon, M., Kapoor, I., Mahajan, C. (eds) Transfusion Practice in Clinical Neurosciences. Springer, Singapore. https://doi.org/10.1007/978-981-19-0954-2_8
Download citation
DOI: https://doi.org/10.1007/978-981-19-0954-2_8
Published:
Publisher Name: Springer, Singapore
Print ISBN: 978-981-19-0953-5
Online ISBN: 978-981-19-0954-2
eBook Packages: MedicineMedicine (R0)