
Abstract
The National Radiation Protection Institute (NRPI) performed the study evaluating linear accelerator (linac) unscheduled downtime and other parameters related to linac failure (e.g. treatment cancellations, patients transferred to other linac, patients treated with modified dose fractionation) at radiotherapy departments in the Czech Republic. Thirteen radiotherapy departments with at least one linac (out of 21 departments in the Czech Republic) voluntarily participated in the study covering 29 out of 47 linacs. Downtime was evaluated for a one year period from July of 2016 to June of 2017. The methodology was as follows: NRPI designed the data entry form which was sent electronically to medical physicists at participating radiotherapy departments. Data related to linac failures were filled in. The completed forms were evaluated by NRPI. Unscheduled downtime was defined as time when linac cannot be operated during operating hours. Unscheduled downtime per linac per year ranged from 4 to 222 h (mean = 73 h, median = 61 h). Downtime percentage calculated as a ratio of downtime and total sum of operating hours per year ranged from 0.2 to 7.6% (mean = 2.8%, median = 2.2%). The number of treatment cancellations per linac per year ranged from 0 to 661. Unified methodology enabled objective comparison of linac downtime at particular radiotherapy departments in the Czech Republic. The study confirmed usefulness of having minimally two matched linacs at a department. The results of this study could help radiotherapy departments negotiate better service contract (e.g. agreement on maximum guaranteed downtime).
Access provided by Autonomous University of Puebla. Download conference paper PDF
Similar content being viewed by others


Keywords
1 Introduction
Linear accelerator (linac) failures complicate clinical operation at the radiotherapy departments. Moreover, these failures (particularly the prolonged ones) lead to the unscheduled interruptions in radiotherapy treatment and as a result complicate correct realization of the treatment from a radiobiology perspective.
Potential unreliability of the linacs increases the risk of unintended irradiation of patients, thus there is a link to radiation protection of patients. For the needs of the State Office for Nuclear Safety, which is national regulatory authority responsible for radiation protection and safety, the National Radiation Protection Institute (NRPI) performed the study evaluating linac downtime and its clinical impacts (e.g. treatment cancellations and patients transferred to other linac) at radiotherapy departments in the Czech Republic.
Thirteen radiotherapy departments out of 21 departments in the Czech Republic equipped with at least one linac voluntarily participated in the study covering 29 out of 47 linacs. Downtime and its clinical impacts were evaluated for a one year period from July of 2016 to June of 2017. Data were evaluated anonymously. Out of 29 linacs, 18 linacs of vendor No. 1 and 11 linacs of vendor No. 2 were analyzed within the study. Years of linac installation ranged from 2003 to 2016 (mean = 2010, median = 2009).
2 Materials and Methods
The parameters evaluated within the study were as follows: number of failures (number of interruptions) that led to linac downtime, downtime, downtime percentage, number of treatment cancellations, number of treatments when patients were transferred to other linac at the department, number of patients treated with modified dose fractionation and number of treatments when verification of patient positioning could not be performed.
The methodology used in the study was as follows: NRPI designed the data entry form in Excel which was sent electronically to medical physicists at participating radiotherapy departments. In this form, data related to linac failures were filled in (e.g. time of occurrence of linac failure, time of report linac failure to service organization, time of service engineer arrival, time of linac being repaired, time of interruption of clinical operation). Also clinical impacts, e.g. number of treatment cancellations and number of treatments when patients were transferred to other linac, were filled in. Completed forms were sent back to the NRPI, where forms from all departments were gathered, reviewed, corrected (if needed) and evaluated.
Unscheduled downtime was defined as time when linac cannot be operated during operating hours. Only interruptions of half an hour and longer were recorded. Preventive service maintenance work did not count as downtime.
Downtime percentage was calculated as a ratio of downtime and total sum of operating hours per year. The total sum of operating hours per year was calculated as a product of typical daily operating hours (e.g. 12 h) as reported by departments and the number of operating days per year. Operating hours relate to the hours when patients are treated. The hours for performing linac quality assurance are not counted.
Treatment cancellations are defined as instances when patients due to the linac failure could not be treated on the scheduled treatment day.
Apart from the downtime also the work time limitation was recorded. It is the time when linac is in clinical operation but there is a failure of one of its part, e.g. kilovoltage (kV) imaging system. Clinical impacts related to the work time limitation were evaluated.
3 Results
3.1 Downtime
The number of failures per year that led to linac downtime at 13 radiotherapy departments ranged from 2 to 44 (mean = 12, median = 9).
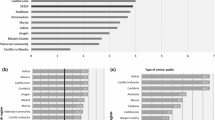
Unscheduled downtime per linac per year ranged from 4 to 222 h (mean = 73 h, median = 61 h). Downtime percentage per linac per year found out at 13 radiotherapy departments is shown in Fig. 1 and ranges from 0.2 to 7.6% (mean = 2.8%, median = 2.2%).

Downtime percentage per linac per year found out at 13 radiotherapy departments. The columns represent individual linacs at radiotherapy departments. Blue columns represent linac vendor No. 1, green columns represent linac vendor No. 2 (Color figure online)
3.2 Clinical Impacts
The number of treatment cancellations per linac per year found out at 13 radiotherapy departments is shown in Fig. 2. Two departments (No. 7 and 13) did not provide such data. The number of treatment cancellations per linac per year ranged from 0 to 661 (mean = 107, median = 56).

Treatment cancellations per linac per year found out at 13 radiotherapy departments. The columns represent individual linacs at radiotherapy departments. Departments No. 7 and 13 did not provide such data. Department No. 1 and 10 had 0 treatment cancellations for all linacs. Department No. 4 had 0 treatment cancellations for second linac. Department No. 11 had 0 treatment cancellations for first linac. Blue columns represent linac vendor No. 1 and green columns represent linac vendor No. 2 (Color figure online)
During linac downtime 9 out of 13 departments transferred patients to other matched linac at the department. The number of treatments when patients were transferred to other matched linac at the department ranged from 32 to 906 (mean = 216, median = 108).
Due to the linac downtime two departments modified dose fractionation for patients. At one department the dose fractionation was modified for five patients, the second department did not provide such data.
Due to the linac failures verification of patient positioning using kV imaging system could not be performed on seven linacs at five radiotherapy departments. At one department this verification could not be performed in approximately 210 treatments on one linac and in 266 treatments on the other linac. At the second department verification of patient positioning could not be performed in 16 treatments on one linac and in 5 treatments on the other linac. Three remaining departments did not provide such data.
4 Discussion
4.1 Downtime
As can be seen in Fig. 1, there is a variation in linac downtime percentage across the departments. The reason is that downtime percentage is influenced by many factors. Downtime percentage depends not only on reliability of the individual linac operation but also on other factors such as complexity of treatments (3D conformal radiotherapy (3DCRT), intensity modulated radiotherapy (IMRT), volumetric modulated arc therapy (VMAT) or stereotactic radiotherapy), skillfulness of individual service engineer, skillfulness of the personnel at the department (potential inexpert linac handling) and local conditions (e.g. service engineer is part of the personnel or his residence is very close to the department). There is also a variation in linac downtime percentage across the individual linacs at the departments.
Statistical analysis shows that the differences between the mean of downtime percentage for vendor No. 1 and 2 are not statistically significant at the alpha level of 0.05. Unscheduled downtime per linac of vendor No. 1 per year ranged from 0.2 to 5.4% (mean = 2.3%, median = 2.1%). Unscheduled downtime per linac of vendor No. 2 per year was higher and ranged from 1.0 to 7.6% (mean = 3.6%, median = 2.4%).
There is no relation between the age of the linacs and the downtime percentage and also there is no relation between the type of service contract (full service contract versus no service contract) and downtime percentage.
On the basis of the detailed investigation of downtime, it can be mentioned that lower downtime was a little more often observed at linacs with a higher proportion of 3DCRT plans in relation to more complex techniques such as IMRT or VMAT. Conclusive findings related to downtime would require longer period of the study, e.g. 4 or 5 years.
For all failures leading to linac downtime we separated downtime into five items: time elapsed from occurrence of failure to sending a report on failure to service organization, time elapsed from sending a report to arrival of service engineer, time to repair, time of linac performance testing after the repair and time of the repairs performed by local physicists. We added up these partial times for all failures at all 13 departments and founded that 59% of the total downtime (calculated from all 13 departments) makes up the time to repair and 31% of the total downtime makes up the time to the arrival of service engineer. Contribution of the time of the repairs performed by local physicists to the total downtime is 6%, contribution of the time to the report on failure and contribution of the time of linac performance testing after the repairs is only 2%.
4.2 Clinical Impacts
The number of treatment cancellations depends on the fact whether the departments have another matched linac where in case of linac downtime patients could be transferred without the need of treatment plan recalculation. Two departments without treatment cancellations (department No. 1 and 10, see Fig. 2) have the matched linacs and transferred patients to the matched linacs. On the contrary, two departments with the highest number of treatment cancellations (department No. 9 and 2, see Fig. 2) do not have matched linacs, therefore could not transfer patients to the matched linacs.
For eliminating clinical impacts of downtime some departments had to add extra work shifts and at some departments performing linac quality assurance had to be rescheduled, e.g. on the weekend or on late in the evening.
Recording of clinical impacts related to downtime was too complicated and too time consuming at some departments, thus they did not provide these data.
5 Conclusion
Within the study, 29 out of 47 linacs were analysed. Hereby the overview of linac downtime in the Czech Republic was obtained. Unified methodology enabled objective comparison of linac downtime at particular radiotherapy departments.
The study confirmed usefulness of having minimally two matched linacs at a department. This, in case of linac downtime, enables transfer patients to another linac without the need of treatment plan recalculation and, as a result, decreases the number of treatment cancellations.
The results of this study could help radiotherapy departments negotiate better service contract. The specification of maximum guaranteed downtime together with the specification of linac operating hours in the service contract should be a good practice. Specified linac operating hours should be used for downtime evaluation. Each department should itself evaluate linac downtime and should require penalty in case of exceeding the guaranteed downtime.
The results of this study could also push service organizations forward to improve their service quality. Downtime should be one of the service quality indicators.
Recording of clinical impacts related to linac downtime was too complicated and too time consuming at some departments. Vendors should try to develop tools enabling simple evaluation of linac downtime and related clinical impacts.
Acknowledgements
This work was done under a contract by the State Office for Nuclear Safety of the Czech Republic. The authors would like to thank the medical physicists and other personnel from radiotherapy departments who took part in this study for their cooperation.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Ethics declarations
The authors declare that they have no conflict of interest.
Rights and permissions
Copyright information
© 2019 Springer Nature Singapore Pte Ltd.
About this paper

Cite this paper
Dufek, V., Horakova, I. (2019). Evaluation of Downtime of Linear Accelerators Installed at Radiotherapy Departments in the Czech Republic. In: Lhotska, L., Sukupova, L., Lacković, I., Ibbott, G. (eds) World Congress on Medical Physics and Biomedical Engineering 2018. IFMBE Proceedings, vol 68/3. Springer, Singapore. https://doi.org/10.1007/978-981-10-9023-3_63
Download citation
DOI: https://doi.org/10.1007/978-981-10-9023-3_63
Published:
Publisher Name: Springer, Singapore
Print ISBN: 978-981-10-9022-6
Online ISBN: 978-981-10-9023-3
eBook Packages: EngineeringEngineering (R0)