
Abstract
Developmental hip dysplasia (DHD) is frequently encountered in the pediatric orthopedic practice. DHD is characterized by dislocation of the femoral head in the acetabulum. In Brazil are diagnosed three times more cases than the world average (5–8 cases for 1,000 births). The lack of treatment leads to long-term morbidity, abnormal gait, chronic pain and arthritis. Early detection and treatment with a Pavlik harness results in improved outcomes. After 6 months of age, closed or open reduction with spica casting is required for 4 months to treat a persistent hip dislocation. Plaster is used for orthopedic immobilization due the low cost, moldability and good mechanical resistance. However, there are several risks and complications due to the use of spica cast in DHD treatment: Skin problems due to lack of adequate hygiene (itching, ulceration, dermatitis and infection), formation of pressure areas, plaster fracture (11% of cases) and fever. Digitization techniques have been explored for production of customized hip abduction brace by additive manufacturing. However, it is not possible to keep a child standing still to perform 3D scanning of the hip and legs region. The goal of this research was to develop an alternative approach for acquisition of the external geometry of the infant to create 3D model of an abduction brace. The parameterization technique created includes: The creation of a virtual 3D model of a child’s body using the MakeHuman software; Articulation of the hip region of the model to the position required in the treatment of DHD with the Blender software; Definition of the parameters required for the modeling of a hip abduction brace. A DHD pediatric orthopaedist approved the methodology created. Innovations in the area of assitive technology can bring many benefits to the user in the process of rehabilitation.
Access provided by Autonomous University of Puebla. Download conference paper PDF
Similar content being viewed by others


Keywords
1 Introduction
Several clinical situations in orthopedics require immobilization as a form of treatment, such as developmental hip dysplasia (DHD), Legg Calvé Perthes disease, fractures and others [1]. DHD occurs in infants in the first months of life and is characterized by dislocation of the femoral head of the acetabule. In Brazil, about 5–8 cases are diagnosed for every 1,000 births. Lack of DHD treatment leads to long-term morbidity, abnormal gait, chronic pain, and arthritis in adult life. If DHD is diagnosed in the first month of life, treatment is performed with the Pavlik harness. If the treatment does not work or if the diagnosis of DHD is performed after the sixth month of life, it is necessary to replace the femoral head in the acetabular region surgically and maintain the infant with legs and hip in abduction and flexion with the use of spica casting during a period of 4 months.
Plaster is the most commonly used material for orthopedic immobilization due to its low cost, easy moldability and good mechanical strength. However, there are several risks and complications for to the use of plaster in DHD treatment: skin problems due to lack of proper hygiene, itching, ulceration, dermatitis, infection, formation of pressure areas, plaster fracture in 11% of cases and increase in body temperature.
Some types of orthosis have been investigated to replace the spica casting in the immobilization of the hip and legs in the treatment of DHD [2, 3]. The technology used in this orthotics is outdated, the material is thermoformed in the region to be immobilized, or a pre-cast with plaster is done directly on the patient’s body, production is laborious and time consuming procedure. These orthoses are expensive, the risks and complications due to the use are the same as those found in the spica casting, and there are few studies on their effectiveness [2,3,4,5,6,7].
In recent years, the application of new technologies such as 3D modeling and additive manufacturing (MA) have been explored in the health area in the production of customized orthoses [8, 9], mainly of upper limbs [10,11,12,13,14]. The MA allows the production of solid components from digital models with a 3D printing machine. It allows the manufacture of parts with good mechanical strength, low cost and in a relatively short period of time [15].
An alternative to immobilization in the treatment of DHD might be a custom orthosis constructed from high technology with low cost that can replace the spica casting efficiently. Some digitizing techniques have been explored for 3D modeling and production of a custom infant bracing for hip abduction produced by additive manufacturing (MA). In [16], the external surface of the hip region and legs of a puppet was digitized by a photogrammetry technique and by 3D scanning [8, 9]. Photogrammetry allows the 3D reconstruction of an object from photographs, being a lower cost alternative to laser scanning. The scanning technique was tested only on a static doll, however, 3D scanning of the hip region and legs of a baby are not feasible; because this procedure requires the child to remain in a static position for a few minutes [17].
A virtual model of the infant can be created by means of a parametrization technique, without the need of plaster cast or 3D scanning. This approach may allow the creation of an orthosis for the treatment of DHD without the need to digitize its structure. In this study, a methodology will be described for the acquisition of the geometry of the infantile hip and that can be substituted for the techniques of photogrammetry and scanning. The objective of this research is to develop an alternative approach for the acquisition of the external geometry of a baby, through the creation of a virtual model of an infant, for the 3D modeling of an abduction orthosis for DHD, through of a parameterization technique.
2 Materials and Methods
The MakeHuman open source software is a database of 3D humanoid models based on anthropometric measurements. The software allows the creation of parameterized customized models and some functions allows to export a humanoid model to the free software Blender so that it can be articulated. Thus it would be possible to position a virtual model in the required position in the DHD treatment. In cases of DHD, each child needs to be immobilized in a different position with the angle of hip flexion from 40º to 45º, abduction angle of the legs between 100º and 110º and angle of knee flexion varying from 80º to 90º.
In this study, a parametrization technique was developed to transfer patient measurements to a virtual humanoid model. The technique ensures that the patient’s measurements are more accurate than those obtained by scanning from the technique of photogrammetry or scanning that require the baby not to move. A parametrization approach was developed in three stages:
-
(1)
Creation of an articulated 3D model of the infantile body (avatar) with the software MakeHuman and a skeletal mesh deformation: A humanoid infant model was selected (Age: 1, Muscle: 50%, Weight: 100%, Height: 50.22 cm (Fig. 4) and also the skeleton model most appropriate to the project (“Cmu mb” model with only 31 bones) was selected.
-
(2)
Articulation of the hip and legs of the avatar to the position required in the treatment of DHD using the free software Blender: The positioning of the thigh and legs required in the treatment of DHD was represented with the help of the tool plugin BlenderTools. The template file exported in MakeHuman was then imported with the extension “.mhx”. In Blender the position of the object was modified using the rotation cursor in the “pose mode” option. The bone corresponding to the member that was to be modified was selected. The “bone” corresponding to the thigh was selected and the green line of the rotation cursor moved to the desired abduction angle, in this case approximately 110º. The “bones” corresponding to the legs were selected, so the green line of the rotation cursor was moved, thus leading to knee flexion, positioned at 90º. Other adjustments such as rotation on the Y-axis of the thigh were required. Finally, an articulated doll model was created and could be positioned as needed.
-
(3)
3D modeling of the child’s avatar and definition of a minimum number of parameters for the 3D modeling of a bracing: Once the doll is in the desired position, it was possible to determine the measures of the hip region and legs, which will be the measures taken of a patient. With the help of the Meshmixer software, some functions analyze and correct where there is a vector mesh error, closing the cloud of open points. With only the part of interest of the hip, in Blender, the hip object was solidified in the option “edit” with the function “make solid”. After this step the object could be modeled and parameterized. The dummy object is placed in the desired position with the help of the Blender tool, in case it was placed in the treatment position for DHD to exemplify. In this way, a humanoid model was created articulated and positioned to be produced in the future, a customized orthosis model for a patient.
3 Results
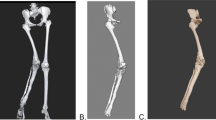
The humanoid model created in the MakeHuman software was dimensioned with age, weight and height close to an infant, to represent its body geometry (Figs. 1, 2, 3). A set of bones was added to the model (Fig. 1), to create a skeleton in which it was possible to articulate the doll later. In the Blender software, the articulating doll (Fig. 2) was imported. With the aid of the skeleton previously inserted with a doll, the modifications can be made (Fig. 3), starting with the bone representing the femur, following the bone that moves the leg.

Selected template in MakeHuman representing the geometry of a child

Skeleton selected for posterior articulation of the humanoid model

Articulated doll with hip in the DHD treatment position
The virtual doll in anatomical position and the virtual doll already positioned for DHD treatment were parameterized (Fig. 4). The 3D model of a created infant allows the high fidelity representation of the kinematics of the whole body using the definition of anatomical and reproducible bone segment.

Circumference of: TC (thorax), WC (waist), PC (pelvis), PTC (proximal thigh), MTC (mean thigh), DTC (distal thigh), KC (Knee), CC (calf), SC (supramaleolar). Length of: TPL (thoraco-perineal), TAL (thoraco-anal), ATL (anterior thigh), PTL (posterior thigh), ALL (anterior leg), PLL (posterior leg), SPL (special pelvic), LTPL (lateral thoraco-pelvic), PRL (perineal region), ARL (anal region)
4 Discussion
The plaster used in orthopedics is efficient in its immobilization function, however, the burdens entailed by its use are far greater than the benefits. The child who uses the plaster can not sit down, take a bath, it goes through anesthetic precedence for the placement of the plaster and other problems. There are studies and technologies capable of creating customized orthoses to eliminate the problems generated by the use of plaster. These technologies can be used in an even more efficient and practical way with the use of the parametrization technique developed in this research.
MakeHuman has proven to be a good tool for acquiring ready-made models, without the need for digitization, either from dolls or from the patient itself. MakeHuman is commonly used in computer animation for games and movies. However, no study was found using the software in the creation of a parameterized virtual model for the development of personalized orthotics. Based on literature searches, it was possible to observe that there is not much information on anthropometric parameterization. The difficulty of making a personalized orthosis in children who move unconsciously motivated the creation of an innovative methodology. This technique was created for the development of hip orthoses but can be used for any structure of the body acting in the creation of orthoses by additive manufacture.
The acquisition of human geometry, for the production of orthoses, through preexisting models is possible. But the positioning of the 3d puppet is a difficult task because each clinical case requires a different and crucial pose for a favorable prognosis of the treatment. Subsequently, it is practicable to manipulate this geometry, to create a bracing. This methodology can aid in new protocol research, so that specific, precise and specialized methodologies for the production of orthoses can arise, as well as the creation of orthoses for various regions of the human body, as well as for animals. This research is being developed and evaluated with the participation of a medical team from the orthopedics of a large public hospital. The approach requires little contact time with the infant, and the time to produce a hip abduction orthosis can be optimized and can bring many benefits for the babies in the DHD rehabilitation process.
5 Conclusion
Personalized technological innovations in the area of orthosis can bring many benefits for users and caregivers, generally aiding in the process of rehabilitation. It is possible to use pre-created humanoid models to efficiently represent the geometry of the external anatomy of the human body. The acquisition of anatomical hip geometry and modeling may allow the production of orthoses for the treatment of DHD without the need for 3D scanning. Using the parametrization technique in humanoid models to create scripts of the geometry of an infant can allow the creation of personalized products as an abductor orthosis. These technologies allow you to produce low-cost orthoses, so that they fit perfectly to the hip with a safety margin for comfort.
References
Campion JC, Benson MK. Developmental dysplasia of the hip. Surgery (Oxford), 2007;25(4):176–180.
Wilkinson AG, et al. The efficacy of Pavlik harness, the craig splint and the von Rosen splint in the management of neonatal dysplasia of the hip. JBone & Joint Surgery. 2002;84(5):716–719.
Hedequist D, et al. Use of an abduction brace for developmental dysplasia of the hip after failure of Pavlik harness use. Journal of Pediatric Orthopedics. 2003;23(2):175–177.
Ibrahim DA, et al. Abduction bracing after Pavlik harness failure. JPediatric Orthop. 2013;33(5):536.
Uras I, et al. The efficacy of semirigid hip orthosis in the delayed treatment of developmental dysplasia of the hip. Journal of Pediatric Orthopaedics B. 2014, 23(4):339–342.
Dyskin E, Ferrick M. Semirigid abduction bracing is effective treatment of reducible developmental dysplastic hips after failure of Pavlik harness. Annals of Orthopedics & Rheumatology. 2015;3(2):1045.
Wahlen R, Zambelli P. Treatment of the developmental dysplasia of the hip with an abduction brace in children up to 6 months old. Advances in orthopedics. 2015:1–6.
Toledo I, et al. Metodologia para produção de órteses por meio de fotogrametria, modelagem 3D e manufatura aditiva. XVII Congresso Brasileiro de Biomecânica CBB e I Encontro Latino Americano de Biomecânica, 2017, Porto Alegre. p. 564–465.
Mavroidis C et al. Patient specific ankle-foot orthoses using rapid prototyping. Journal of Neuroengineering and Rehabilitation. 2011;8(1):1–11.
Jumani MS, et al. Fused deposition modelling technique (FDM) for fabrication of custom-made foot orthoses: a cost and benefit analysis. Scientific International (Lahore). 2014;26(5):2571–2576.
Paterson AMJ, Bibb RJ, Campbell RI. A review of existing anatomical data capture methods to support the mass customisation of wrist splints. Virtual and Physical Prototyping. 2010;5(4):201–207.
Paterson A. Digitisation of the splinting process: exploration and evaluation of computer aided design approach to support additive manufacture [thesis]. Leicestershire: Loughborough University; 2013.
Paterson AM, Donnisson E. Computer-aided design to support fabrication of wrist splints using 3D printing: A feasibility study. Hand Therapy. 2014;19(4):102–103.
Paterson AM et al. Comparing additive manufacturing technologies for customised wrist splints. Rapid Prototyping Journal. 2015; 21(3):230–3.
Cano APD. Parametrização e produção de órtese termomoldável para imobilização de punho produzida por manufatura aditiva. 102p. Trabalho de Conclusão de Curso de Engenharia Biomédica (TCC) - Universidade Federal de São Paulo. 2017.
Meidanshahy T. Feasibility of using 3D printing in the manufacture of orthotics componentry. Diss. Flinders University, Adelaide, Australia 2014.
Munhoz R, Moraes CADC, Tanaka H, Kunkel ME. A digital approach for design and fabrication by rapid prototyping of orthosis developmental dysplasia of the hip. Research on Biom Eng. 2016;32(1),63–73.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2019 Springer Nature Singapore Pte Ltd.
About this paper

Cite this paper
Santos, N.A., Artioli, B.O., Goiano, E., Gonçalves, M., Kunkel, M.E. (2019). A Parametrization Approach for 3D Modeling of an Innovative Abduction Brace for Treatment of Developmental Hip Dysplasia. In: Lhotska, L., Sukupova, L., Lacković, I., Ibbott, G. (eds) World Congress on Medical Physics and Biomedical Engineering 2018. IFMBE Proceedings, vol 68/3. Springer, Singapore. https://doi.org/10.1007/978-981-10-9023-3_41
Download citation
DOI: https://doi.org/10.1007/978-981-10-9023-3_41
Published:
Publisher Name: Springer, Singapore
Print ISBN: 978-981-10-9022-6
Online ISBN: 978-981-10-9023-3
eBook Packages: EngineeringEngineering (R0)