
Abstract
The impact of epigenetics in the field of radiation oncology and the DNA damage response is an emerging area of research. Epigenetic mechanisms may potentially play a role in inherent or acquired radioresistance of tumors. In this section, we will discuss what is known about epigenetics, specifically DNA methylation and miRNAs, with regards to the DNA damage response and the exploitation of epigenetics therapeutically. Very little is known about histone modifications and the DNA damage response. Current research in radiation oncology and epigenetics is now at the level of basic science, but is beginning to move to the level of pre-clinical and translational research. The speed of research is accelerating since there are currently epigenetic therapies approved for treatment of certain cancers outside of the radiation oncology clinic.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others

Keywords
12.1 DNA Damage Response
12.1.1 Micro RNAs
Micro RNAs (miRNA) are short RNAs that function post-transcriptionally to regulate protein expression. MiRNAs have been shown to regulate genes involved in tumorigenesis, apoptosis, angiogenesis, and other cancer cell activities [1]. MiRNAs can also regulate tumor suppressors. In the area of radiation, at this writing there are 319 PubMed entries for the search of “miRNA” AND “radiation”. Included in this set, 170 miRNAs have been predicted to target DNA-damage response genes. The number of miRNAs that have been experimentally determined to affect the DNA damage response is 174. The predicted and experimentally determined miRNA list are not identical. These statistics illustrate the early stage at which miRNA research is when it applies to radiation therapy.
A series of profiling studies suggests that exposure to ionizing radiation (IR) results in a response that includes altered expression of miRNAs. A screen of 1,090 miRNAs in human embryonic stem cells (hESCs) exposed to 1 Gy IR resulted in 54 miRNAs differentially expressed 16 h post-IR [2]. The number of up-regulated miRNAs outnumbered down-regulated miRNAs by 5:1. Gene ontology analysis of the predicted target genes for down-regulated miRNAs was performed and overrepresented categories included cell cycle, cell death, transcription, and cell differentiation. Changes in miRNA expression following radiation may represent a broad and specific response that influences DNA repair or cell survival. In one study of miRNAs differentially expressed 30 min and 2 h after radiation, the data suggests down-regulation of miRNAs controlling expression of genes involved in DNA repair [3]. This would be expected to increase expression of DNA repair genes and potentially enhance DNA repair. At 2 h, however, there was an up-regulation of miRNAs controlling expression of apoptosis-related genes – expected to result in decreased expression of apoptosis genes. This is hypothesized to increase cell survival.
The let-7 family of miRNAs are differentially expressed following radiation [4–8]. However, agreement on the direction of change is lacking. This may be partly explained by different cell types, radiation doses, and post-IR analysis times. Let-7f-2 is down-regulated 8 h following 50 cGy treatment in a lymphoblast cell line [5]. Let-7g is up-regulated 6 h after 2 Gy in normal endothelial cells [4]. Let7a-i were up-regulated in Jurkat cells at 4–24 h following 2 Gy, but in TK6 cells (B lymphoblast cells), most let-7 members were down-regulated [7]. Let-7e was up-regulated 3–8 h following 10–400 cGy in normal human skin fibroblasts, while other let-7 family members showed only modest changes [6]. Fractionated radiation treatment of prostate cancer cells also results in increased let-7 miRNA [8]. Let-7 family miRNAs negatively regulates the RAS oncogene, suggesting a mechanism for an influence on radiosensitivity. Over-expression of let-7g in irradiation of endothelial cells results in decreased clonogenic survival, while inhibition of let-7g increases clonogenic survival [4]. This study provides an important link between radiation-induced changes in let-7g expression and the radiation response. If radiation causes increased let-7 miRNA expression and this decreases clonogenic survival, it would not seem that this effect is a protective mechanism for the cell. One possibility is that this response pushes cells with poorly repaired DNA or that have become genomically unstable toward apoptosis.
The effect of radiation on expression of miR-20 and miR-21 are equally variable. Low radiation doses (10–400 cGy) have been shown to up-regulate or down-regulate expression [5, 6]. Up-regulation was observed at 2 Gy [4]. Inhibition of miR-20a had little effect on clonogenic survival following IR. When a biological consequence of the differential miRNA expression can be found, more weight can be assigned to these observations.
Differential expression of miRNAs can be detected in peripheral blood cells of patients following radiotherapy [9]. Three hours following a total body irradiation of 1.25 Gy, let-7f, let-7g, miR-20a, and miR-21 were among 45 up-regulated miRNAs found. Thirty-eight miRNAs were found to be differentially expressed in all seven patients. Detection of miRNAs in peripheral blood cells could be used to test for radiation exposure.
Studies targeting specific miRNAs and the effect on radiation resistance have measured biological effects. MiR-148b is up-regulated by IR and overexpression radiosensitized lymphoblastoid Raji cells by enhancing apoptosis [10]. MiR-34b overexpression radiosensitized lung cancer cell lines but no difference in apoptosis was observed [11]. Induction of miR-99 by IR prevented an increase in the chromatin remodeling factor SNF2H [12]. Recruitment of BRCA1 to DNA damage sites was also reduced, leading to reduced repair efficiency.
PTEN is downregulated in late stage nasopharyngeal carcinoma and expression is regulated by miR-205. Following radiotherapy, miR-205 is up-regulated and ectopic overexpression reduced radiation-induced apoptosis [13]. The conclusion is that miR-205 expression contributes to radioresistance through PTEN, and its induction by radiotherapy may confer some degree of radioresistance on cells. The correlation between miR-205 and radioresistance suggests miR-205 could be used as a biomarker for determining the response to radiotherapy.
MiR-18a expression down regulates ATM expression [14]. ATM is an early sensor of DNA damage following IR and initiates signaling to result in DNA repair. In primary breast cancer tissue, miR-18a was found to be up-regulated and ectopic expression of miR-18a in breast cancer cells radiosensitized them through reduced DNA repair capacity. This potentially important finding demonstrates that miRNAs that regulate DNA repair could be new therapeutic targets.
These studies on miRNAs and radiation therapy hold promise in explaining contributors to radioresistance and offer potential novel targets for therapeutics. However, an interesting study that shows more work needs to be done investigates the effect of knockdown of the machinery required for miRNA processing and activity on radiation sensitivity [15]. Knockdown of Dicer, Drosha, and Ago2 did not result in radiosensitization of lung cancer cells. These proteins are essential for knockdown of mRNAs by miRNA or siRNA. One caveat to all RNAi experiments is whether the degree of knockdown is sufficient to observe a biological effect. Remaining low levels of the target protein may be enough to maintain much of the activity one is attempting to eliminate. This study used apoptosis as a measure of radiation sensitivity. Clonogenic survival is a more robust assay for determining the impact of radiation. This may account for the differences between the studies described.
12.1.2 DNA Methylation
There is little information on DNA methylation response following exposure to IR or the impact of DNA methylation on the DNA damage response. It has been shown that IR results in global DNA hypomethylation in some normal tissues, but not others, as well as in cell lines [16–18]. Others have failed to find significant changes in DNA methylation in normal cells exposed to radiation after a 7 day recovery [19]. Decreased global DNA methylation was observed following fractionated radiation and this was accompanied by a loss of histone H4-Lys20 trimethylation [20]. These data were later extended to show locus-specific changes in DNA methylation following regrowth of MCF7 breast cancer cells following IR [21]. These changes were found 14 days following irradiation and included differential DNA methylation of FOXC1 and TRAPPC9. Our group has found global loci-specific changes in DNA methylation following IR (unpublished data). This response initiated as soon as 1 h after IR and extended over 3 days, and varied according to radiation dose. The preponderance of evidence thus far suggests either a DNA methylation response to IR and/or an involvement in DNA methylation in radioresistance. However, the functional significance of global changes in DNA methylation is yet to be deciphered.
Hyper- or hypomethylation of specific genes may partly account for the radioresistant phenotype. DNA methylation profiles have been compared in radiosensitive and radioresistant cells and suggest involvement in maintenance or induction of radioresistance [18, 22]. In a comparison of a radioresistant and radiosensitive lung cancer cell line, 1,091 differentially methylated genes were discovered [22]. Among these, SERPINB5 and S100A6 were found to be hypermethylated in the radioresistant cell line while CAT and BNC1 were hypomethylated in the radioresistant cell line. SERPINB5 and S100A6 were more highly expressed in the radiosensitive line and upon RNAi, the cells became more radioresistant. Conversely, RNAi of CAT and BNC1 in the radioresistant cell line sensitized them to IR. This study is limited by the fact that two different cell lines were compared instead of isogenic cell line pairs. It is likely that many differences in DNA methylation between the two cell lines exist without an impact on radiation resistance. In fact, in the two cell lines compared, one was p53 wild type and the other was p53 negative. Nevertheless, the genes investigated had some impact on radioresistance under their experimental context. Additional studies using other models may be more revealing.
12.2 Radiosensitization by DNA Demethylation
A number of compounds demethylate DNA by inhibiting DNA methyltransferases, in particular DNA methyltransferase 1 (DNMT1). DNMT1 is the predominant DNMT that methylates DNA following replication. DNMT inhibitors fall into two classes: nucleoside analogs (5-azacytidine, 5-aza-2′-deoxycytidine, 5,6-dihydro-5-azacytidine, zebularine) and non-nucleoside analogs (hydralazine, RG108, procainamide, procaine, SGI-1027). There is active research taking place to develop new inhibitors of both the nucleoside analog and non-nucleoside analog classes due to some of the caveats described below [23, 24].
DNMT inhibition by nucleoside analogs occurs through incorporation into the DNA whereby the DNMT is trapped by the modified pyrimidine and targeted for degradation by the proteasome [25]. A decrease in DNMT1 leads to lower levels of DNA methylation of newly synthesized DNA during cell proliferation. Thus, DNA demethylation results not from active removal of methyl groups from DNA, but more accurately, the dilution of existing methylated DNA by newly synthesized unmethylated DNA. DNA replication is a necessary requirement for the DNA to become demethylated. Toxicity in this class is greatest with 5-azacytidine (5AC). This may partially be due to the fact that 5AC can be incorporated into both DNA and RNA and thus has some effect in non-dividing cells. Decitabine (5-aza-2′-deoxycytidine) and zebularine have lower toxicity. Zebularine, 5AC, and decitabine have been approved for treatment of myelodysplatic syndromes.
The mechanisms of non-nucleoside analog inhibitors of DNMT are more diverse. Procaine prevents DNMT binding to CpG DNA sequences by binding those sequences itself [26]. Hydralazine and procainamide are thought to have similar mechanisms but may also interact with amino acid residues in DNMT and inhibit catalytic activity. RG108 is a rationally designed inhibitor of DNMT and unlike other inhibitors does not require DNMT to bind DNA to exert its activity. RG108 has low cytotoxicity and is considered a promising candidate to bring forward.
Many tumors are resistant to radiation and ways to enhance the effectiveness of treatment by reducing tumor radioresistance is an avid area of study. The effectiveness of radiotherapy is a function of the radioresistance of the tumor versus the radiosensitivity of normal tissue which limits radiation dose. Thus, drugs which decrease the inherent radioresistance of tumors potentially improve the therapeutic ratio of radiotherapy.
Zebularine was the first DNMT inhibitor to be shown to radiosensitize cancer cells [27]. Pancreatic, glioblastoma, and prostate cancer cell lines were exposed to zebularine for 24 or 48 h before irradiation. Clonogenic assays were used to assess radioresistance and it was found that incubation with zebularine for 24 h resulted in an average radiation enhancement factor of 1.2, which is a moderate increase in radiation sensitivity. However, after a 48 h incubation with zebularine a high level of radiosensitization was observed, with an average radiation enhancement factor of 1.6. In glioblastoma xenografts, treatment with 350 mg/kg zebularine every 8 h for 3 days led to a significant tumor growth delay that was equivalent to a single 4 Gy dose of radiation. When zebularine and radiation were combined, the growth delay was significantly longer. No obvious toxicity was observed in mice treated with zebularine.
Although the first study combining a DNMT inhibitor with radiation was done with zebularine, subsequent studies by other groups have predominantly investigated 5AC and decitabine. Hofstetter et al. [28] demonstrate strong radiosensitization of colorectal carcinoma by 5AC in vitro. Decitabine has been shown to radiosensitize breast, head and neck, and gastric cancer cell lines [29–31]. In gastric cancer, 2 of 4 cell lines showed modest radiosensitization and in the breast cancer study, MDA-MB-231 cells were strongly sensitized. A study of medulloblastoma cell lines, however, showed no increased radiosensitivity following decitabine treatment [32]. One concern about negative results is that 5AC and decitabine have a very short half-life in solution. The half-life of 5AC at 37 °C may be as short at 7 h [33]. This means that in vitro studies may require addition of fresh drug multiple times over a several day experiment. Storage and handling of the drugs are also important in order to maintain activity over many months. Head and neck cancer cell lines have been shown to be radiosensitized by decitabine and the effect was enhanced further by combined treatment with a histone deacetylase inhibitor [31]. The above in vitro studies have not yet been followed up with careful animal studies to determine the effect in vivo.
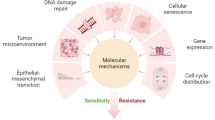
The mechanism of radiosensitization is still to be determined (Fig. 12.1). Since DNMT inhibitors reduce global DNA methylation, it has been hypothesized that they may alter expression of genes related to cell cycle or the DNA repair capacity of a cell. Some evidence supports a role for a change in cell cycle. An increase in G2/M cells is observed in many cell lines following decitabine or zebularine treatment [29, 31], but this did not correlate with the radiosensitization effect seen by clonogenic assay [27, 30]. In colorectal cancer cells, 5AC alone did not cause a G2 arrest but did potentiate the G2-arrest seen after radiation treatment [28]. In contrast, zebularine has been shown to inhibit the G2 arrest induced by radiation [34]. These disparate reports ultimately lend little support to the hypothesis that DNMT inhibitors radiosensitize cells due to an influence on cell cycle. Additional studies may shed more light on this question.

Decitabine treatment in combination with radiation reduces clonogenic survival and induces radiosensitivity by causing DNA hypomethylation, cell cycle perturbation, increased apoptosis, and decreased DNA repair
Cells treated with decitabine may become more susceptible to apoptosis triggered by radiation. When gastric cancer cells were treated with decitabine alone, no increase in apoptosis was observed, but when decitabine was combined with radiation, the percentage of cells undergoing apoptosis increased [30]. Furthermore, cell lines which exhibited radiosensitization also showed increased apoptosis. DNMT inhibitor effects on apoptosis sensitivity are commonly cited in studies of DNMT inhibitors used alone for treatment of cancer [35].
The other potential mechanism of radiosensitization that has been investigated is the DNA repair activity in the cell (Fig. 12.1). The formation and resolution of nuclear γH2AX foci is an indicator of DNA damage signaling and the repair process. If DNA is repaired slowly, the time required for γH2AX resolution is delayed. Under normal conditions, γH2AX foci are largely resolved at 24 h post-irradiation. In cancer cells treated with radiation combined with decitabine or zebularine, however, γH2AX foci were still present after 24 h [27, 29, 34]. That delayed kinetics were observed by multiple groups across disparate cell lines and inhibitors strengthens the hypothesis that the ability of cells to repair DNA damage is impaired by DNMT inhibitors or the associated changes in gene expression that accompany DNA demethylation.
DNMT1 may not be the primary target through which DNMT inhibitors affect radiosensitization. DNMT1 deficient cells were no more sensitive to radiation than parental cells carrying wild type DNMT1 [28]. However, cells deficient in DNMT3b were more radiosensitive than their parental counterparts. The caveat to this study is that global DNA methylation differences between the cell lines were not measured. Nor was there a measurement of specific gene methylation differences. It is important to resolve this issue as studies go forward since the DNMT inhibitors have different activity towards DNMT1, DNMT3a, and DNMT3b [34].
Although DNA methylation is globally reduced by treatment with zebularine and other DNMT inhibitors, the effect on a gene-by-gene basis is variable. The 14-3-3σ and RASSF1A gene promoters are demethylated in breast, prostate, pancreatic and glioblastoma cells following treatment with zebularine or decitabine [27, 29]. Both of these genes are tumor suppressors that play a role in cell cycle and/or the DNA damage response through the various signaling pathways they interact with. Promoter demethylation was associated with an increase in gene expression [27]. In colon cancer cells, promoter regions for p16, hMLH1 and hTERT were demethylated by 5AC treatment and persisted for 7 days following removal of drug [28]. In studies focusing on gene expression, p53, caspase 6, DAPK1, DAPK2, and DAPK3 were shown to be increased following decitabine treatment. Only DAPK1 was increased by radiation alone but the highest expression of all five genes was observed under the combined treatment of decitabine and radiation [30]. The DAPK proteins are involved in cell survival, apoptosis, and autophagy. These data lend further support to increased susceptibility to apoptosis as a potential mechanism of DNMT inhibitor radiosensitization.
DNMT inhibitors that lead to global DNA demethylation are being studied as a class of drugs with radiosensitizing activity in a variety of cancers. Some of these compounds are already approved for treatment of some malignancies in their own right and new inhibitors are being developed with a more favorable stability and toxicity profile. The mechanism of radiosensitization remains elusive but may center around DNA repair and apoptosis.
12.3 Conclusions
DNA methylation and miRNAs clearly impact the radiation response and influence the radiation resistance of cancer cell in vitro. The challenge is determining how epigenetics may be manipulated to enhance the effectiveness of radiation therapy. Specific targeting of the effect may still be an issue with interventions utilizing epigenetic therapy, however, the opening of a new angle of attack against cancer offers opportunity.
References
Lages E, Ipas H, Guttin A, Nesr H, Berger F et al (2012) MicroRNAs: molecular features and role in cancer. Front Biosci 17:2508–2540
Sokolov MV, Panyutin IV, Neumann RD (2012) Unraveling the global microRNAome responses to ionizing radiation in human embryonic stem cells. PLoS One 7:e31028
Maes OC, An J, Sarojini H, Wu H, Wang E (2008) Changes in microRNA expression patterns in human fibroblasts after low-LET radiation. J Cell Biochem 105:824–834
Wagner-Ecker M, Schwager C, Wirkner U, Abdollahi A, Huber PE (2010) MicroRNA expression after ionizing radiation in human endothelial cells. Radiat Oncol 5:25
Cha HJ, Seong KM, Bae S, Jung JH, Kim CS et al (2009) Identification of specific microRNAs responding to low and high dose gamma-irradiation in the human lymphoblast line IM9. Oncol Rep 22:863–868
Chaudhry MA, Omaruddin RA, Kreger B, de Toledo SM, Azzam EI (2012) Micro RNA responses to chronic or acute exposures to low dose ionizing radiation. Mol Biol Rep 39:7549–7558
Chaudhry MA (2009) Real-time PCR analysis of micro-RNA expression in ionizing radiation-treated cells. Cancer Biother Radiopharm 24:49–56
John-Aryankalayil M, Palayoor ST, Makinde AY, Cerna D, Simone CB 2nd et al (2012) Fractionated radiation alters oncomir and tumor suppressor miRNAs in human prostate cancer cells. Radiat Res 178:105–117
Templin T, Paul S, Amundson SA, Young EF, Barker CA et al (2011) Radiation-induced micro-RNA expression changes in peripheral blood cells of radiotherapy patients. Int J Radiat Oncol Biol Phys 80:549–557
Wu Y, Liu GL, Liu SH, Wang CX, Xu YL et al (2012) MicroRNA-148b enhances the radiosensitivity of non-Hodgkin’s Lymphoma cells by promoting radiation-induced apoptosis. J Radiat Res 53:516–525
Balca-Silva J, Sousa Neves S, Goncalves AC, Abrantes AM, Casalta-Lopes J et al (2012) Effect of miR-34b overexpression on the radiosensitivity of non-small cell lung cancer cell lines. Anticancer Res 32:1603–1609
Mueller AC, Sun D, Dutta A (2012) The miR-99 family regulates the DNA damage response through its target SNF2H. Oncogene 32(9):1164–1172
Qu C, Liang Z, Huang J, Zhao R, Su C et al (2012) MiR-205 determines the radioresistance of human nasopharyngeal carcinoma by directly targeting PTEN. Cell Cycle 11:785–796
Song L, Lin C, Wu Z, Gong H, Zeng Y et al (2011) miR-18a impairs DNA damage response through downregulation of ataxia telangiectasia mutated (ATM) kinase. PLoS One 6:e25454
Surova O, Akbar NS, Zhivotovsky B (2012) Knock-down of core proteins regulating microRNA biogenesis has no effect on sensitivity of lung cancer cells to ionizing radiation. PLoS One 7:e33134
Tawa R, Kimura Y, Komura J, Miyamura Y, Kurishita A et al (1998) Effects of X-ray irradiation on genomic DNA methylation levels in mouse tissues. J Radiat Res 39:271–278
Kalinich JF, Catravas GN, Snyder SL (1989) The effect of gamma radiation on DNA methylation. Radiat Res 117:185–197
Chaudhry MA, Omaruddin RA (2012) Differential DNA methylation alterations in radiation-sensitive and -resistant cells. DNA Cell Biol 31:908–916
Lahtz C, Bates SE, Jiang Y, Li AX, Wu X et al (2012) Gamma irradiation does not induce detectable changes in DNA methylation directly following exposure of human cells. PLoS One 7:e44858
Pogribny I, Koturbash I, Tryndyak V, Hudson D, Stevenson SM et al (2005) Fractionated low-dose radiation exposure leads to accumulation of DNA damage and profound alterations in DNA and histone methylation in the murine thymus. Mol Cancer Res 3:553–561
Kuhmann C, Weichenhan D, Rehli M, Plass C, Schmezer P et al (2011) DNA methylation changes in cells regrowing after fractioned ionizing radiation. Radiother Oncol 101(1):116–121
Kim EH, Park AK, Dong SM, Ahn JH, Park WY (2010) Global analysis of CpG methylation reveals epigenetic control of the radiosensitivity in lung cancer cell lines. Oncogene 29:4725–4731
Datta J, Ghoshal K, Denny WA, Gamage SA, Brooke DG et al (2009) A new class of quinoline-based DNA hypomethylating agents reactivates tumor suppressor genes by blocking DNA methyltransferase 1 activity and inducing its degradation. Cancer Res 69:4277–4285
Plitta B, Adamska E, Giel-Pietraszuk M, Fedoruk-Wyszomirska A, Naskret-Barciszewska M et al (2012) New cytosine derivatives as inhibitors of DNA methylation. Eur J Med Chem 55:243–254
Ghoshal K, Datta J, Majumder S, Bai S, Kutay H et al (2005) 5-Aza-deoxycytidine induces selective degradation of DNA methyltransferase 1 by a proteasomal pathway that requires the KEN box, bromo-adjacent homology domain, and nuclear localization signal. Mol Cell Biol 25:4727–4741
Lin X, Tascilar M, Lee WH, Vles WJ, Lee BH et al (2001) GSTP1 CpG island hypermethylation is responsible for the absence of GSTP1 expression in human prostate cancer cells. Am J Pathol 159:1815–1826
Dote H, Cerna D, Burgan WE, Carter DJ, Cerra MA et al (2005) Enhancement of in vitro and in vivo tumor cell radiosensitivity by the DNA methylation inhibitor zebularine. Clin Cancer Res 11:4571–4579
Hofstetter B, Niemierko A, Forrer C, Benhattar J, Albertini V et al (2010) Impact of genomic methylation on radiation sensitivity of colorectal carcinoma. Int J Radiat Oncol Biol Phys 76:1512–1519
Wang L, Zhang Y, Li R, Chen Y, Pan X et al (2013) 5-aza-2′-Deoxycytidine enhances the radiosensitivity of breast cancer cells. Cancer Biother Radiopharm 28(1):34–44
Qiu H, Yashiro M, Shinto O, Matsuzaki T, Hirakawa K (2009) DNA methyltransferase inhibitor 5-aza-CdR enhances the radiosensitivity of gastric cancer cells. Cancer Sci 100:181–188
De Schutter H, Kimpe M, Isebaert S, Nuyts S (2009) A systematic assessment of radiation dose enhancement by 5-Aza-2′-deoxycytidine and histone deacetylase inhibitors in head-and-neck squamous cell carcinoma. Int J Radiat Oncol Biol Phys 73:904–912
Patties I, Jahns J, Hildebrandt G, Kortmann RD, Glasow A (2009) Additive effects of 5-aza-2′-deoxycytidine and irradiation on clonogenic survival of human medulloblastoma cell lines. Strahlenther Onkol 185:331–338
Stresemann C, Lyko F (2008) Modes of action of the DNA methyltransferase inhibitors azacytidine and decitabine. Int J Cancer 123:8–13
Kim HJ, Kim JH, Chie EK, Young PD, Kim IA et al (2012) DNMT (DNA methyltransferase) inhibitors radiosensitize human cancer cells by suppressing DNA repair activity. Radiat Oncol 7:39
Ghanim V, Herrmann H, Heller G, Peter B, Hadzijusufovic E et al (2012) 5-azacytidine and decitabine exert proapoptotic effects on neoplastic mast cells: role of FAS-demethylation and FAS re-expression, and synergism with FAS-ligand. Blood 119:4242–4252
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2013 Springer Science+Business Media Dordrecht
About this chapter
Cite this chapter
Zielske, S.P. (2013). The Role of Epigenetics in Radiation Therapy and the DNA Damage Response. In: Sarkar, F. (eds) Epigenetics and Cancer. Springer, Dordrecht. https://doi.org/10.1007/978-94-007-6612-9_12
Download citation
DOI: https://doi.org/10.1007/978-94-007-6612-9_12
Published:
Publisher Name: Springer, Dordrecht
Print ISBN: 978-94-007-6611-2
Online ISBN: 978-94-007-6612-9
eBook Packages: Biomedical and Life SciencesBiomedical and Life Sciences (R0)