
Abstract
For cardiac catheterization, the most frequently used access to the heart is via the femoral artery and/or vein. Other ways of access are possible or necessary, for instance, if the pulmonary arteries can only be reached via the SVC in patients after a Glenn shunt or in patients having an occlusion of the femoral vessels due to previous catheterizations. The principles of getting access are explained using the femoral vessels. Thereafter alternative ways of access are mentioned which are the access of internal jugular vein, subclavian vein, umbilical vein and artery, and radial artery.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
These keywords were added by machine and not by the authors. This process is experimental and the keywords may be updated as the learning algorithm improves.
For cardiac catheterization, the most frequently used access to the heart is via the femoral artery and/or vein.
Other ways of access are possible or necessary, for instance, if the pulmonary arteries can only be reached via the SVC in patients after a Glenn shunt or in patients having an occlusion of the femoral vessels due to previous catheterizations.
The principles of getting access are explained using the femoral vessels.
Thereafter alternative ways of access are mentioned which are the access of:
-
Internal jugular vein
-
Subclavian vein
-
Umbilical vein and artery
-
Radial artery
1 Femoral Venous and Arterial Access
1.1 Positioning and Landmark
Especially in infants and small children, a small elevation of the bottom, e.g. with a napkin, helps to expose the femoral vessels. The legs should be fixed in a strait and slightly outwards rotated position.
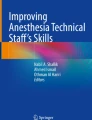
The landmark to be sought is the inguinal ligament which runs between the superior iliac spine and the pubic tubercle (Fig. 11.1).

Landmarks of femoral artery and vein access (From Bergersen [1], with permission)
The pulse of the femoral artery should be sought. The femoral vein runs closely medial to the femoral artery. A useful landmark for this area is the inguinal crease which is located about 1 cm below the inguinal ligament in normal weight children and adolescents, but can be misleading in overweight patients [1, 2].
The femoral pulses should be palpated in both groins to feel whether there is a difference in the quality of pulses. If a pulse is blunted on one side due, e.g. vessel stenosis, the puncture of the contralateral vessel should be preferred.
Marking of the vessels on both sides with a pen is done by many operators before covering the child. These markings help to identify the vessels when the landmarks are more difficult to see when the patient is draped (Fig. 11.2).

Marking of the landmarks for femoral artery and vein access
Delineation of the vessels by 2D ultrasound and Doppler facilitates the puncture of the vessels (Fig. 11.3). By this method, a stenosis or an occlusion of the vessel can be detected. Furthermore, the passage of the needle can be directed under vision into the respective vessel.

Ultrasound-guided femoral vessel access using a linear probe. The pulsating flow of the femoral artery and the needle directing towards the femoral artery are seen
1.2 Technique
-
It is useful always to prepare both sides of the groin.
-
For local anaesthesia, infiltrate a small amount subcutaneously. Always withdraw on the hub of the needle to be sure that you are not injecting into the vessel.
-
Large amounts of lidocaine will distort the underlying vessel. Be aware that the feeling of pain is mainly coming from the skin!
1.3 Femoral Venous Access
-
Usually venous access prior to the arterial one.
-
Palpate femoral artery. The femoral vein lies directly medial to the artery.
-
Introduce the needle into the skin just below the inguinal crease.
-
Angle between needle and skin about 45°.
-
Advance the needle in short 1–2 mm jabs and wait for the backflow into the needle.
-
If advanced too far, withdraw the needle slowly with or without a negative suction on an attached syringe.
-
Having backflow into the needle, hold the needle with the right hand and insert the guide wire into the needle and then into the vessel. The guide wire should get into the vessel smoothly without applying force (Fig. 11.4).
Fig. 11.4 
Introduction of guide wire and sheath into femoral vessel below the inguinal ligament (I) far away from the peritoneal sac (P) (From Mullins [2], with permission)
-
Having the wire in the vessel, make a tiny cut with a blade and insert the sheath with the introducer under a mild rotation into the vein. Thereafter remove the dilator and wire and check appropriate sheath position by withdrawing blood through the side arm of the sheath.

Hints
-
Withdraw guide wire and needle when the wire cannot be advanced easily. Very likely the vessel is not hit properly.
-
When the guide wire is very likely in the vessel, but advancement is not possible, change the needle to a small short cannula and try to aspirate blood by withdrawing the cannula and then re-advance the guide wire.
-
Consider a careful injection of a small amount of contrast medium if there is suspicion of a more distal occlusion of the vessel by, e.g. thrombosis due to previous catheterization [1].
1.4 Femoral Arterial
It is done similar as described for the venous access. When the needle hits the artery, there is a brisk and pulsating backflow. A syringe to aspirate the blood is not needed.
1.5 Complication of Femoral Access
-
Retroperitoneal bleeding if the femoral vessels are punctured above the inguinal ligament [3]!
2 Internal Jugular Vein Access
2.1 Positioning and Landmarks
-
Extend the head backwards by putting a towel underneath the shoulder.
-
Turn the head to the contralateral side.
-
Identify the landmark which is the triangle formed by the sternal and the clavicular head of the sternocleidomastoid muscle and the clavicle. The internal jugular vein lies lateral to the carotid artery which pulse can be felt (Fig. 11.5).
Fig. 11.5 
Landmarks of the internal jugular vein access using the anterior approach (From Bergersen [1], with permission)

Note:
The right internal jugular vein is preferred over the left one since:
-
The apex of the lung is lower on the right side.
-
The path to the atrium is more direct.
-
Less risk of damaging the thoracic duct.
2.2 Ultrasound-Guided Approach
-
Clear delineation of carotid artery and internal jugular vein is possible.
-
When applying slight external compression the vein, collapses while the artery does not.
2.3 Anterior Approach
-
The entry site of the needle is lateral to the carotid artery in the middle of the triangle formed by the carotid artery, the mandible and the sternocleidomastoid muscle.
-
The degree of the needle to the skin is about 45° aiming to the ipsilateral nipple.
2.4 Posterior Approach
-
The needle is inserted at the border of the sternocleidomastoid muscle midway between the angle of the mandible and the clavicle.
-
The needle has an angle of 30° to the skin and is directed towards the sternal notch.
2.5 Central Approach
-
Enter the site with the needle at the border of the sternocleidomastoid muscle midway between the angle of the mandible and the clavicle.
-
Needle has an angle of 30° to the skin and is directed towards the sternal notch.
3 Subclavian Vein Access
3.1 Positioning and Landmarks
-
Entry is possible on both sides. Some operators prefer the on left side, since the course of the wire and catheter is easier to the heart.
-
The arm on the ipsilateral side should be straight downwards along the thorax.
-
Small elevation of the shoulders by a towel and head turned to the contralateral side.
-
Landmarks are the clavicle and the suprasternal notch.
The subclavian vessels are situated underneath the clavicle. The subclavian artery runs closely cephalad to the subclavian artery (Fig. 11.6).

Landmarks of the subclavian vein access (From Bergersen [1], with permission)
3.2 Technique
-
Needle entry is at the lateral third of the clavicle about 2 cm below the clavicle aiming to the suprasternal notch.
-
Advance of the needle under continuous aspiration with an attached syringe.
-
When free blood flow is visible, advance a long flexible guide wire to be sure that you are is in the venous structures (SVC, RA) or in PA in the Glenn circulation.
3.3 Complications and Avoidance
-
Puncture of subclavian artery and subsequent haematothorax.
Avoid medial entry of the needle; otherwise the site of the puncture cannot be compressed against the first rib.
-
Pneumothorax
The apex of the lungs is situated under the first rib. The needle should not go too deep, rather aiming with an angle of about 30° towards the suprasternal notch. All these landmarks must be identified before draping the patient [1].
4 Umbilical Venous Access
Catheterization of the umbilical vessels (two arteries and one vein) is well described in neonatal text books and is a standard procedure in the neonatal care.
The catheterization of the vessels is performed with a 3.5 or 5 F umbilical catheter. The 3.5 F catheter takes a 0.021″ and the 5 F catheter a 0.025″ guide wire.
If these catheters are in place, they can be cut with a scalpel short above the umbilicus and the sheath needed can be inserted over a guide wire.
4.1 Problems
-
Umbilical vein
The guide wire and catheter are difficult to manoeuvre into the ductus venosus because you are the entering the portal vein.
Withdraw the catheter into the umbilical vein and give a small injection of contrast to delineate the course of the ductus venosus into the IVC.
-
Umbilical artery
It might be difficult to advance the guide wire into the aorta due to the tight curves of the umbilical artery entering the iliac arty. A normal straight guide may be more suitable than a torque guide wire which has a stiff shoulder.
5 Radial Artery Access
5.1 Positioning and Landmarks
-
The arm is abducted 90° and positioned on an arm support.
-
Slightly elevate the wrist by a cotton swab and fixate the hand.
-
The landmarks are the distal ends of the radial and ulnar bone and the radial pulse.
5.2 Technique
-
Insert the needle superficially with a 30° angle. No syringe attached. Advance until jerks of pulsating blood will flow.
References
Bergersen L (2009) Vascular access. In: Bergersen L, Foerster S, Marshall AC, Meadows J (eds) Congenital heart disease the catheterization manual. Springer Science + Business Media, New York, pp 21–34
Mullins CE (2006) Vascular access: needle, wire, sheath/dilator and catheter introduction. In: Mullins CE (ed) Cardiac catheterization in congenital heart disease. Blackwell Publishing, Malden, USA, pp 100–162
Wilson N (2009) Complications of vascular access. In: Hijazi MZ, Feldmann T, Cheatham JP, Sievert H (eds) Complications during percutaneous interventions for congenital and structural heart disease. Informa Healthcare, London: UK, pp 41–46.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2015 Springer-Verlag Italia
About this chapter
Cite this chapter
Weil, J. (2015). The Usual Vascular Access. In: Butera, G., Chessa, M., Eicken, A., Thomson, J. (eds) Cardiac Catheterization for Congenital Heart Disease. Springer, Milano. https://doi.org/10.1007/978-88-470-5681-7_11
Download citation
DOI: https://doi.org/10.1007/978-88-470-5681-7_11
Published:
Publisher Name: Springer, Milano
Print ISBN: 978-88-470-5680-0
Online ISBN: 978-88-470-5681-7
eBook Packages: MedicineMedicine (R0)