
Abstract
Bending the neck and turning the head respecting to the body cause the stimulation of the cervical proprioceptors. This kind of receptors activates a pathway projecting to the vestibular nuclei.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others

Keywords
- Cervical Proprioception
- Vestibular Nuclei
- Superficial Electrical Stimulation (SES)
- Cervical Paravertebral Muscles
- Left Trapezius
These keywords were added by machine and not by the authors. This process is experimental and the keywords may be updated as the learning algorithm improves.
1 Introduction
Bending the neck and turning the head respecting to the body cause the stimulation of the cervical proprioceptors. This kind of receptors activates a pathway projecting to the vestibular nuclei.
The impulses are reflected through the nucleo-reticular formation and then to the spinal cord. Such activation allows movements of the neck to influence the postural set and to modify the activation of the antigravity muscles of the lower limbs.
This pattern of muscular activation is hypnotized on the basis of the so-called neck-postural reflexes, or better named cervico-spinal reflex [1]. During the contraction of the paravertebral muscles of the neck, there is a response characterized by inhibition of ipsilateral soleus in respect to the side of neck stimulation and facilitation of the contralateral muscles [2, 3]. During the superficial electrical stimulation (SES), the paraspinal muscles are also activated and there are previous studies that show that SES is able to reduce vertigo and dizziness [4]. This kind of stimulation is also able to evoke changes in activity of the muscles of the legs. We used a neurophysiological test named H-reflex to control this modification. It holds special interest because it can attest the activation of the vestibular-spinal way during the stimulation of the paraspinal muscles through the modification of excitability of the motoneuron. Under appropriate conditions, a single electrical shock to the tibial nerve will evoke two discrete motor action potentials in the calf muscles. The first potential, the M-wave, results from direct stimulation of motor nerve fibers. The second potential, the H-wave, is the expression of a monosynaptic reflex, which runs in afferent fibers (I1 a) from the neuromuscular spindles and back again through motor afferents. Since no interneurons are involved, the size of the second action potential will provide a measure of motoneuron excitability under a variety of experimental conditions [5, 6].
2 Material and Methods
Eight normal subjects (5 females and 3 males), aged between 20 and 33 years old, were admitted to the study. Subject did all sit in a comfortable armchair, with cervical spine at rest position with non-flexion, extension, or lateral bending and head support and not rotated with respect to the trunk.
Legs were at rest and supported, the hips were flexed at 90°, the knees were flexed at 120°, and the ankles were flexed at 90°. Patients were in a quiet room and were awake and relaxed with eyes closed.
Recording of the H-reflex was obtained with pregelled surface electrodes. Active electrode was fixed on the distal on the belly of soleus muscle, while reference electrode was fixed 30 mm below. Stimulation of the tibial nerve was performed with surface electrodes at the popliteal fossa. Interelectrodes distance was 25 mm. Stimulus duration was 1 ms. All this is in accordance with the indication of the literature [5]. Stimulus intensity was between 5 and 21 mA at the intensity needed to evoke the maximum amplitude of the H-reflex (H Max) for each subject.
H Max from soleus muscle right and left legs was recorded every 5 min before, during, and after the stimulation of the muscles. In particular superficial electrical stimulation (SES) of neck paravertebral muscles and contemporary contralateral upper part of the trapezius was applied. SES of the neck muscles was applied with pulse rate of 80 Hz and a pulse width randomly modulated between 100 and 200 ps of duration (so-called vestibular electrical stimulation – VES – see Chap. 30). First VES application was performed for 15 min contemporaneously on the right paravertebral muscles of the neck and on the left upper part of trapezius muscle. After 30 min VES was applied to the contralateral paravertebral of the neck and trapezius muscle for a duration of 15 min. The recordings of the H Max were obtained by left and right leg. We calculated mean (M) and standard deviation (SD) of the five consecutive H Max responses, and obtained values were tabulated. Measures of H Max value were done every 5 min. For each subject were recorded one H Max basal value before application VES, 3 H Max were obtained every 5 min during VES applied to the right paravertebral and left trapezius muscle; 3–6 H Max during to recovery phase, 1 H Max basal, 3 H Max values during VES applied to the left paravertebral muscle and right trapezius muscle, and 3–6 H Max values obtained during a second recovery phase. Statistical analysis was performed with the Student’s t-test comparing H Max recorded before, during, and after each VES application.
3 Results
They were homogeneous in all subjects both for the stimulation patterns. The contemporary VES of the left paravertebral cervical muscles and of the right trapezius was enhanced in all subjects after 10 min, H Max amplitude (14 % of the maximum amplitude; p = 0.02) of the right soleus muscle, and reduced after 15 min, H Max amplitude (−20 %; p = 0.001) of the soleus muscles. H Max amplitude returned to the basal values 10 min after the end of the stimulation on the right soleus and was still reduced (−36 %; p = 0.001) 10 min after the end of SES on the left soleus. In some subjects H Max values lasted less than normal for 30 min after the end of VES. Recording from the right soleus showed that 10 min after the end of VES amplitude was still decreased (27 %; p = 0.001) in some subject inhibition of the H-reflex that lasted over 30 min (Fig. 31.1).

Effects of electrical stimulation on H-reflexes
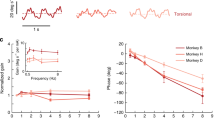
The stimulation by VES of the right paravertebral cervical muscles and left trapezius induced, after 5 min, an increase of the left side values (20 %; p = 0.001) and reduced, after 15 min, the amplitude of the right values (−32 %; p = 0.001). In a short time after the end of the SES, left H-reflex returns to basal values. When a paradoxal second phase begins, H-reflex decreases slowly but progressively reaching a new “basal” value that is significantly (p = 0.001) lower. Right H-reflex remains reduced at least 10 min after the end of SES (−27 %; p = 0.001) (Fig. 31.2).

Effects of electrical stimulation on H-reflexes
4 Conclusions
The results of the present study showed that VES of the neck muscles clearly influenced the excitability of the motor neurons of the lower limbs.
It is important to underline that VES at the intensity to which was applied never evoked muscles contraction. On the contrary VES was applied in the same frequency range (80 Hz) which is able to activate muscles spindles by vibratory stimulation. Thus, it is likely that VES activate the same spinal pathways activated from the cervico-spinal reflexes, modulating in the same way the postural reflexes of the lower limbs. This action is probably mediated from proprioceptive input originated in the spindles of the neck muscles [7]. Otherwise we cannot exclude the action of skin receptors mediating the vibratory sense.
Proprioceptive afferent input evoked from VES of the neck muscles could reach also contralateral Deiters vestibular nuclei and cortex, probably by mean of reticular pathways. In such way SES may influence the equilibrium system. It is known [8] that if vestibular apparatus is damaged, the reflexes of the neck, limb, and eyes muscles become prominent. Therefore it is possible that VES action in treatment of vertigo and dizziness is based on the modulation of the proprioceptive input from neck muscles.
At last there is the observation that inhibitory effect is more pronounced and long lasting than the excitatory one. Supraspinal pathway activation [9] may give account of this phenomenon, but further investigations are needed to verify such hypothesis.
References
Ghez C (1991) Posture. In: Kaendel ER, Schwartz JH, Jessell TM (eds) Principles of neural sciences, 3rd edn. Elsevier, New York/Amsterdam/London/Tokyo, pp 596–607
Angel RW, Hofmann WW (1963) The H reflex in normal, spastic and rigid subjects. Arch Neurol 8:591–596
YaM K (1979) The organization of voluntary movement. Neurophysiological mechanisms, vol II. Plenum Press, New York/London, pp 27–503
Alpini D, Cesarani A, Barozzi S (1992) Non pharmacological treatment of acute vertigo. In: Claussen CF, Kirtane MV, Schneider D (eds) Diagnostic procedures and imagining techniques used in neurotology. Proceedings of the XVI NES Congress. Werner Rudat & Co, Nachf ed m + p, Hamburg, pp 337–340
Thompson AK, Chen XY, Wolpaw JR (2013) Soleus H-reflex operant conditioning changes the H-reflex recruitment curve. Muscle Nerve 47(4):539–544
Oliveira MI, Machado AR, Chagas VG, Granado TC, Pereira AA, Andrade AO (2012) On the use of evoked potentials for quantification of pain. Conf Proc IEEE Eng Med Biol Soc 2012:1578–1581
Shields RK, Dudley-Javoroski S (2013) Fatigue modulates synchronous but not asynchronous soleus activation during stimulation of paralyzed muscle. Clin Neurophysiol 11:S1388-2457(13)00278-2
Okuma Y, Bergquist AJ, Hong M, Chan KM, Collins DF (2013) Electrical stimulation site influences the spatial distribution of motor units recruited in tibialis anterior. Clin Neurophysiol 18: S1388-2457(13)00315-5
Lagerquist O, Mang CS, Collins DF (2012) Changes in spinal but not cortical excitability following combined electrical stimulation of the tibial nerve and voluntary plantar-flexion. Exp Brain Res 222(1–2):41–53
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2014 Springer-Verlag Italia
About this chapter
Cite this chapter
Osio, M., Brunati, L., Abello, G., Mangoni, A. (2014). The Neurophysiological Basis of Vestibular Electrical Stimulation. In: Alpini, D., Brugnoni, G., Cesarani, A. (eds) Whiplash Injuries. Springer, Milano. https://doi.org/10.1007/978-88-470-5486-8_31
Download citation
DOI: https://doi.org/10.1007/978-88-470-5486-8_31
Published:
Publisher Name: Springer, Milano
Print ISBN: 978-88-470-5485-1
Online ISBN: 978-88-470-5486-8
eBook Packages: MedicineMedicine (R0)