
Abstract
Radiocarpal fracture-dislocations are the most debatable of carpal dislocations. The term radiocarpal fracture-dislocations has been used incorrectly for many previously reported cases. Thus, many questions arise concerning their incidence, terminology and classification. In this chapter, an attempt is made to determine the criteria based on which an injury can be classified as radiocarpal fracture-dislocation. Additionally, the surgical treatment of radiocarpal fracture-dislocations with combined access, allows for a relatively accurate description of osteoligamentous injuries, both on the palmar and on the dorsal side of the wrist. Four types of injuries in the dorsal and two types of injuries in the palmar dislocations are portrayed. Furthermore, a new classification is proposed based on five parameters: those of chronicity, pathoanatomy, direction, associated injuries and complexity. The staged-reconstruction, the outcome and potential complications of this rare type of injuries are also analyzed with great emphasis on ulnar translation, for which a method of reconstruction using a tendon graft in cadavers is described.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others



Keywords
These keywords were added by machine and not by the authors. This process is experimental and the keywords may be updated as the learning algorithm improves.
1 Introduction
Until the description of the fractures of the distal radius by Claude Pouteau in 1783, the radiocarpal (RC) dislocations were the only known carpal injuries. Dupuytren was the first, who in 1834 recognized their rarity. The RC dislocation injury was first recognized and described by Malle in 1838, when he identified a volar RC fracture-dislocation. Shortly thereafter, Marjolin and Voillemier identified and reported dorsal RC fracture-dislocations. All these observations were made from examination of postmortem specimens [1, 2]. Destot [3] reported the first radiographically documented case of a RC fracture-dislocation in 1926.
RC fracture-dislocations are relatively rare injuries, whose exact frequency is unknown. Gui [4] reported that these dislocations represent 0.2 % of all dislocations (quoted by Rosado [5]), while Dunn [6], from 112 fracture-dislocations of the wrist, reported 6 RC dislocations, i.e., a percentage of 5.3 (quoted by Bilos et al. [7]). However, it was later disputed, whether three of those cases actually belonged to the category of RC dislocations [8]. Moneim et al. [9] reported that within a 13-year period, he treated 7 cases of RC dislocations and that this number represented 20 % of all carpal dislocations, encountered during that period. Between these two extremes (0.2–20 %), Ilyas’ et al. [10] estimation of 2.7 % (12 out of 438 patients with distal radius fracture or wrist dislocation) and 0.46 % with pure ligamentous dislocations, seems to be more realistic. We will probably never find out the true incidence of these injuries, since there is no consensus as to which injuries should be named RC fracture-dislocations.
Due to the rarity of the injury of most references, describe a relatively small number [7, 9, 11–15] or isolated cases [16–34]. At present only a few reports involve more than 10 patients: the report by Nyquist and Stern [35] with 10 cases, by Mudgal et al. [36] with 12 cases, by Girard et al. [37] with 12 cases, and by Dumontier et al. [38] with 27 cases throughout a 23-year period.
The literature reveals that pure RC dislocations are rare injuries, while the RC fracture-dislocations involving radial styloid fractures are the most frequent. In addition, the dorsal RC fracture-dislocations are much more common than their palmar counterpart [36, 38, 39], although it seems the opposite is true for pure RC dislocations. By reviewing the literature, Table 8.1 shows the number of cases of pure dislocations (dorsal, volar, and multidirectional) that have been reported so far and the subtype of volar dislocations associated with the ulnovolar fragment of the distal radius.
As for more violent traumas, these injuries have been reported mainly in males and usually of young age. In our series of 26 patients, the average age was 33.7 (range, 19–60) and only one was a woman, while in Dumontier’s [38] series the percentage male/female was 4/1.
2 Restraints of the Radiocarpal Joint
We know that wrist motion along the transverse plane (pronation-supination) is only possible if the wrist is not loaded. The range of passive rotational motion between radius and carpus varies from 40° to 45° [40–43] and extrinsic tendon loading affects significantly the rotational stability of the wrist: the passive pronosupination laxity of the RC and midcarpal joint decreases from 45° to 10° by clenching the fist [40].
Many daily manual tasks are performed by rotation of the forearm. To perform these rotational tasks adequately, the relative motion between the radius and the carpus must be constrained within a limited amount of laxity. These constraints to rotation (which at the same time provide stability to the RC joint) consist of the concavity of the radial fossas, the dorsal and palmar capsuloligamentous structures that link the forearm to the carpus, and the extrinsic tendons that cross the RC joint.
2.1 Ligamentous Structures
Ligamentous structures provide constraints in both rotational (pronosupination between radius and carpus) and translational (dorsopalmar and ulnar) displacement of the wrist.
2.1.1 Rotational Constraints
Ritt et al. [41] stated that ligamentous structures, having a proximal-radial to distal-ulnar course on the dorsal side (DRC ligament) and a proximal-ulnar to distal-radial course on the palmar side (UL, UT ligaments), provide resistance to passive supination of the radiocarpal joint. On the contrary, ligamentous structures having a proximal-radial to distal-ulnar course on the volar side (RSC, LRL, and SRL ligaments) provide resistance to passive pronation of the RC joint with the RSC ligament being the primary pronation constraint. The author supported that ulnarly located structures changed their major constraint contribution with forearm orientation, whereas those with a radial origin had a constant contribution independent of forearm rotation.
Rotational motion between radius and carpus is obviously not restricted to the RC joint alone. The midcarpal joint contributes as well. Gupta and Moosawi [44] stated that active RC pronosupination occurs predominantly at the midcarpal joint with the RC joint contributing only 18 % to supination and 31 % to pronation. In that case, the stabilizing ligaments of the midcarpal joint (SC, TH, TC ligaments) must also contribute significantly to the rotational motion between radius and carpus. Hence, the concept of anti-pronation and anti-supination slings [45] running in opposite directions, could be the main restraining ligamentous construction stabilizing the RC unit during rotational motion (Fig. 8.1).

Supination and pronation constraining ligaments
2.1.2 Dorsopalmar Translation Constraints
The integrity of the palmar RC capsuloligamentous structures seems crucial to RC stability. Katz et al. [46] using fresh-frozen cadaver specimens, found that palmar structures (RSC, LRL, and SRL ligaments) provided greater restraint (61 %) to dorsal translation of the carpus than did dorsal structures (DRC ligament) (2 %). The palmar structures also provided a greater restraint (48 %) to palmar translation of the carpus than did the dorsal structures (6 %). In particular, the SRL ligament is considered by some [11, 47] as the primary soft-tissue restraint against volar translation of the carpus.
Interestingly, the remaining structures (radial and dorsal capsule and UC ligaments) provided 37 % restraint to dorsal translation and 46 % restraint to palmar translation.
2.1.3 Ulnar Translation Constraints
The RC ligaments, both volar (RSC, LRL, SRL ligaments) and dorsal (DRC), having an oblique direction (lateral to medial), constrain the natural tendency of the carpus to slide down the ulnopalmarly inclined distal articular surface of the radius [46, 48, 49]. The extent of ligament injury necessary for an ulnar translation to occur, although not exactly known, is quite substantial [50, 51] and certainly greater than previously reported [52]. In partial injuries, the carpus may translate palmarly rather than ulnarly [50]. Viegas et al. [50] found experimentally that, while the RSC ligament alone was not adequate to stabilize the wrist against ulnar translation, the UC ligaments alone, were. Ilyas and Mudgal [2] stated that ulnar translation in conjunction with loss of the ulnolunate ligaments led to progression of the injury from ulnar translocation to multidirectional instability of the wrist.
The importance of the volar ulnocarpal ligaments (UL, LT, UC) on ulnocarpal stability, has been emphasized in the literature. Munk et al. [53] noted that the rupture of these ligaments produced significant instability not only in deviation but also in rotation of the wrist, while Wiesner et al. [54] stated that sectioning of these ligaments increased significantly the displacement of the carpus in the palmar direction. It has also been reported that the ulnocarpal ligaments can prevent abnormal radioulnar translation of the carpus [55, 56]. Moritomo et al. [57] found that ulnocarpal ligaments are at risk with the wrist in radial extension or hyperextension when associated with axial loading or forearm rotation (or both), a mechanism which has been implicated in RC dislocations.
2.2 Extensor Compartments
Extensor compartments contribute markedly to resisting both pronation and supination at the RC joint [41]. Iwamoto et al. [58] investigated the mechanical strength of each septal attachment on the radius and each of the 6 compartments of the extensor retinaculum. He found that septa 1/2 and 2/3 had the highest stiffness and failure forces, while compartment 3 had the highest stiffness and compartment 2 had the highest failure force. He concluded that large bony attachment sites and a wide breadth of retinaculum fibers may attest to the high stiffness and failure loads of the first 3 compartments.
2.3 Extrinsic Tendons
Capsuloligamentous structures are considered as passive, while extrinsic tendons as dynamic constraints of joints. The interaction between passive and dynamic constraints is now well documented in recent publications that have identified the presence of mechanoreceptors in the joint capsule and carpal ligaments [59]. The neurophysiological mechanisms triggering contraction of certain muscles in order to protect the joint against external forces, have also been defined [60–62]. When a ligament is about to fail, a neuromuscular reflex is triggered that hampers further injury, either by direct contraction of some muscles or by inhibition of some other.
Salva-Coll et al. [63] categorized muscles into two groups: the muscles that pronate the midcarpal joint, (mainly the ECU and in a lesser extent the FCR) and those that supinate the midcarpal joint (the FCU, the ECRL and APL).
3 Correlation Between Articular Fracture Fragments and Ligamentous Attachments
Only few reports are dealing with the association between articular fracture fragments and the attachments of the RC ligaments to the radius [64–66]. Siegel and Gelberman [65] studied the damage that can be caused to the palmar RC ligaments during radial styloidectomy, but they described the regions of ligament origin in absolute dimensions, without taking into account that the areas of origin of the RC ligaments vary in their width when comparing wrists of different sizes. They performed three types of styloidectomies: the short oblique (equated to a fracture of the tip of the radial styloid) corresponds to the interruption of the radial collateral ligament; the vertical oblique (compared to a fracture through the middle of the scaphoid fossa) corresponds to disruption of the RSC ligament origin; and the horizontal styloidectomy (representing a fracture line exiting at the interfacet prominence, proximal to the SL joint) corresponds in addition, to interruption of a major portion (av. 46 %) of the long radiolunate ligament. Hence, in RC dislocations associated with a fracture of only the tip of the radial styloid, the reconstruction of the palmar RC ligaments is mandatory [38]; in RC fracture-dislocations with a fracture of the radial styloid exiting at the level of the SL joint, fixation of the fragment, which contains a major part of the palmar RC ligaments, could probably restore the stability of the wrist.
Berger and Amadio [64] attempted to correlate the size and location of the intraarticular fracture fragments of the distal radius with the palmar RC ligament injuries, while Mandziak et al. [66] by reviewing CT scans of intraarticular distal radius fractures, analyzed the relationship of fracture line locations to known ligament attachments. They found that fracture lines were significantly more likely to occur at the intervals between the ligament attachments than at the ligament attachments themselves and concluded that the ligaments can contribute to the fracture pattern in at least 2 ways: either the intact ligaments avulse the bone fragments or ligaments are shielding the underlying bone. They also noted that the mode of failure depends on patient age. As age increases, so does the modulus of elasticity, stiffness, ultimate tensile strength, and ultimate load, making avulsion-type injuries potentially more common in younger groups and mid-substance tears more likely in older groups.
4 Association Between the Location of an Intraarticular Fracture Fragment and the Stability of the Radiocarpal Joint
The intraarticular fractures of the distal radius, do not equally destabilize the RC joint. Giunta et al. [67] analyzed the subchondral mineralization of the RC joint, by using CT-osteoabsorptiometry. In most cases, two density maxima were found on the articular radial surface, one corresponding to the scaphoid and one to the lunate. These matched the positions of pressure peaks described in reports of research on mechanical models. The density maximum on the articular surface of the radius opposing the scaphoid is, however, rather more dorsally placed, whereas that opposing the lunate lies palmar to the radioulnar midline. This practically means that the volar half of the lunate fossa receives a considerable amount of loads applied to the RC joint and its absence (e.g., after a fracture) would greatly destabilize the RC joint. It is also possible that different anatomical elements contribute to the stability of the RC articulation, in each quarter of the distal articular surface of the radius. At the volar half of the lunate fossa and the dorsal half of the scaphoid fossa, stability is mainly of bone origin, while in the dorsal half of the lunate fossa and the volar half of the scaphoid fossa stability is mainly ligamentous (Fig. 8.2).

(Electronically processed image) The stability of the RC joint at the volar half of the lunate fossa and the dorsal half of the scaphoid fossa is mainly of bone origin (asterisks), while in the dorsal half of the lunate fossa and the volar half of the scaphoid fossa the stability is mainly ligamentous (arrows). With permission from [127]
It is known that the short radiolunate ligament inserts at the palmar rim of the radius correspondingly to the lunate fossa. The exact functional significance of this ligament is not well known, although it is believed to contribute to the stability of the radiolunate joint [47]. Indirectly, however, its importance is highlighted in fractures of the ulnovolar radial rim where this ligament inserts and which, if not treated, results progressively in volar wrist subluxation (Fig. 8.3a–b).

Fractures of the ulnovolar radial rim destabize the RC joint in volar direction (a, b)
5 Mechanism of Injury
RC dislocations are high-energy injuries (fall from a height, traffic or industrial accidents) and therefore the patients rarely remember the exact mechanism of injury.
This injury is a product of several factors: the anatomy of the articulating units, the strength and elasticity of the RC ligaments, the strength of the bony structures, the magnitude, rate of loading, and position of the RC joint at impact [68, 69].
Bohler [70] in 1930, who originally postulated the mechanism of injury for dorsal RC fracture-dislocations, stated that a compressive and rotational force occurs against a hyperextended and pronated wrist. This mechanism was subsequently confirmed by Weiss et al. [71] in a cadaveric study. They found that a torsional element is essential, since an axial load alone causes fractures of the scaphoid with or without midcarpal dislocations or fractures of the distal radius.
Freeland et al. [23] supported that shear forces at the palmar or dorsal edges of the RC joint, often accompanied by excessive reciprocal rotation force combined between the wrist and forearm, have been implicated as the principal mechanisms causing RC dislocation and instability. The ulnar head appears to act as a fulcrum for the rotational forces. The wrist is typically hyperextended on impact, although hyperflexion [19, 25] or distraction [26] has been cited.
Dorsal dislocation of the RC joint occurs when a torsional force is applied to a hyperextended and ulnarly deviated wrist, while the forearm is fixed in hyperpronation [1, 71, 72].
Dumontier et al. [8] supported that the high frequency of an associated fracture of the ulnar styloid, may indicate that these injuries start to develop from the ulnar side of the wrist, but most authors believe that failure begins on the radial side and progresses to the ulnar side of the wrist [28, 73].
Possibly the magnitude and direction of the rotational force and the axial compression will determine the variable amount of bony and soft-tissue injuries encountered in different forms of dislocations or fracture-dislocations. The compressive and torsional component appears in many cases, where the proximal chondral surfaces of the proximal carpal row bones were stripped-off of the cartilage and the osteochondral fragments were found in various positions intra- or extraarticularly (Figs. 8.4a–c, 8.5a–c).

The compressive and torsional component needed to produce a RC fracture-dislocation is evident in this dorsal RC fracture-dislocation, where the arrow indicates an osteochondral defect from the dorsal surface of the lunate (a); by elevating the fractured dorsal radius fragment, an impacted articular fragment of the distal radius is seen (asterisk), while the arrow indicates the missing osteochondral fragment originating from the dorsal lunate (b); the osteochondral fragment is relocated to its original position (c). With permission from [127]

During palmar approach for open reduction of a dorsoulnar RC dislocation, an osteochondral fragment was found (arrow) (a); the dorsal approach revealed an osteochondral defect mainly of the dorsal scaphoid, comprising also the dorsal SL ligament and a small chondral piece of the dorsal lunate (b); relocation of the osteochondral fragment (c) (asterisk dorsal SL ligament, S scaphoid, R radius) (The case is continued in Figs. 8.11, 8.33). With permission from [127]
It is very possible, that independently of their direction, the pivotal separation of the wrist-forearm toward opposite directions is responsible. Specifically, when at the time of injury the forearm is fixed in pronation and the wrist is violently supinated, a dorsal RC dislocation may develop. Conversely, with the hand being fixed in pronation and the forearm violently supinated, a palmar RC dislocation may develop.
Apart from the rotation and the axial compression which are major components of the mechanism of injury, dorsiflexion and ulnar deviation [29, 31, 68], dorsiflexion and radial deviation [38, 74], or volarflexion and radial deviation [25] of the wrist, have all been implicated in the formation of injury. However, in many cases the mechanism of injury is extremely complex and hard to explain.
Anatomical characters of the wrist joint, such as the negative ulnar variance [52], the degree of inclination of the distal articular surface of the radius [55] or DISI deformity [34], could play an important role in the development of RC instability.
6 Terminology
RC fracture-dislocations are the most debatable of carpal dislocations. The term RC fracture-dislocation has been incorrectly used in a considerable number of cases previously reported [75]. Thus, many questions arise concerning their incidence, terminology, and classification. In a strict manner of speaking, dislocations of the RC joint should be either pure ligamentous injuries or dislocations associated with bony avulsions of ligamentous attachments.
There is agreement on terminology, only for pure ligamentous RC dislocations. Confusion exists concerning the various types of fractures of the distal radius associated with dislocation of the RC joint. Thomsen and Falstie-Jensen [33] critically reviewed past reports of 35 cases with RC dislocations or fracture-dislocations and gave credit to only 13 cases. Similarly, Watanabe and Nishikimi [75] considered reliable only 45 of 124 cases that had been reported in the literature.
Dumontier et al. [38] stated that most of the seventy cases reported in the nineteenth century, were not RC dislocations but intracarpal dislocations, epiphyseal injuries or very displaced wrist fractures.
Various authors adopted different criteria to include injuries to the RC fracture-dislocation group: Dumontier et al. [38] considered as RC fracture-dislocations, patients whose entire carpus had been dislocated volarly or dorsally to the radius, with fractures of the radial styloid more than one-third of the width of the scaphoid fossa, provided that the ulnar half of the distal part of the radius was intact; carpal translations associated with a fracture of the volar or dorsal margin of the radius were excluded. On the contrary, others [2, 9, 68, 73, 75, 76], under the term RC fracture-dislocations comprised injuries characterized by dislocation of the RC joint in either dorsal or volar direction, which can be associated with radial and ulnar styloid as well as marginal rim fractures of the distal radius.
The main injury, from which RC fracture-dislocation must be differentiated, is the shearing marginal articular fractures of the distal radius (Type B according to AO classification or type II according to Fernandez classification) (Table 8.2). This type of injuries includes: volar Barton’s fracture (Fig. 8.6a) [77], Schauffeur’s fracture (Fig. 8.6b) [78], and the sizable ulnopalmar (Fig. 8.3a, b) or radiopalmar (Fig. 8.6c, d) fracture fragments of the distal radius, when accompanied by carpal translation [16, 79, 80]. These injuries should not be confused with true RC fracture-dislocations, since, the fractured fragment containing significant ligamentous attachments, remains in contact with the proximal carpal row and its fixation restores the stability of the RC joint. However, most importantly they constitute one-sided injuries by definition, since the opposite cortex and the extrinsic RC ligaments must be intact [69, 81–83]. Thus, the distinction should not be based on the size of the osseous fragment alone, which either way is a subjective criterion, but whether there is an associated injury opposite the osseous fragment side. On the contrary, fractures of the dorsal radial rim associated with dorsal RC subluxation (frequently referred to as dorsal Barton) merit particular attention, as they are more related to RC fracture-dislocations. Lozano-Calderon et al. [84] examined 20 such patients and found that 18 of them also had a wide spectrum of opposite volar injuries.

A RC fracture dislocation must be differentiated from shearing type of fractures, the reduction and fixation of which suffice to restore the RC joint stability: volar Barton’s (a); Schauffeur’s (b); shearing fracture of the palmar part of the scaphoid fossa (c, d). With permission from [127]
The term “transstyloid radiocarpal dislocation” which has been used by some authors [75, 85] is just an indication of the coexistence of a fractured radial styloid with dislocation of the RC joint.
RC fracture-dislocations must also be differentiated from patterns of perilunate ligamentous injuries that have a radial styloid component [68], since they have a different mechanism of injury, pathoanatomy, treatment, and prognosis.
Therefore, we believe that the prerequisite to consider these injuries as radiocarpal dislocations is the dislocation of the entire carpus volar or dorsal to the distal radius without fracture or with avulsion fractures at the insertion site of the ligaments (e.g., tip of the radial styloid, small ulnovolar fragment). Under the term radiocarpal fracture-dislocations we should include patients: (a) with dislocation of the RC joint associated with fractures which involve: the marginal cortical radial rims (volar and/or dorsal), the radial styloid or both, while there must be injuries (osseous and/or ligamentous) to both sides of the RC joint (dorsal and volar), (b) whose radius metaphysis and the main portion of articular surface of the distal radius are intact, and (c) with no associated intercarpal dislocations (the head of the capitate retains normal alignment with the distal lunate).
Idler [86] defined RC dislocation “as loss of articular contact between the proximal carpal row and distal radius not in association with a biomechanically significant fracture of the distal radius”. Although the expression “biomechanically significant” raises much debate, we believe that the definition would be more accurate if the phrase: “and which also requires injury of at least both sides of the RC joint” is also added at the end.
However, there will always be cases in the gray area or questionable cases as to where they belong. These are the cases presented by Capo et al. [87], where the whole proximal carpal row dislocated volarly and disengaged from both the radius and distal carpal row or the case presented by Klein et al. [88], where the dorsally dislocated carpus was associated with a dorsal perilunar dislocation.
Pure RC dislocations are classified as non-dissociative instabilities (CIND) that involve rupture of the extrinsic RC ligaments. In two cases of RC dislocations, the instability is described as complex (Carpal Instability Complex-CIC): in type II RC dislocations according to Moneim et al. [9] and in type II ulnar translocation of the wrist according to Taleisnik [39], where in addition, rupture of the interosseous ligaments of the proximal carpal row is involved. In these cases, the instability is considered as a combination of dissociative (CID) and non-dissociative type (CIND).
In the AO classification, the only type close to RC fracture-dislocations is the B2.3 subtype, which however, involves only the dorsal RC dislocations while dislocations of other directions (palmar, ulnar, radial) are not represented in any subgroup. In the classification by Fernandez et al. [68], based on the mechanism of injury, RC dislocations belong to the IV type and must be differentiated from the II type, which involves the shearing fractures that are associated with carpal subluxation.
7 Pathologic Anatomy of the Injury
Understanding the pathologic anatomy of RC dislocations or fracture-dislocations is dependent on findings at surgical exposure. Since, only few cases have been treated operatively with detailed description of their osseoligamentous injuries, the magnitude and spectrum of injuries are not exactly known. As a result, the extent of tissue compromise is often underestimated, leading to undertreatment and inferior results.
Many authors based on clinical observations [11, 52, 75, 86] or cadaveric studies [50, 89] supported that, dislocation of the proximal row of the carpus from the distal radius and ulna requires complete disruption of the volar RC ligaments in addition to capsuloperiosteal avulsion of the dorsal RC ligaments.
Arthroscopic evaluation, despite the limitations, has been attempted in few cases allowing a precise intraarticular observation [25, 90].
Dumontier et al. [38] presumed that in pure RC dislocations or those accompanied by fracture of the tip of the radial styloid, all volar RC ligaments were torn or presented avulsion fractures at the insertion site of the ligaments. Dorsally, the ligamentous injury presented most often as a capsuloperiosteal avulsion rather than as a rupture of the dorsal RC ligaments. In RC fracture-dislocations, the volar RC ligaments are probably intact and remain attached to the fractured radial fragment, which is probably secondary to impaction of the carpus into the radius. This fracture usually includes all of the scaphoid fossa and may continue on the dorsal margin.
Freeland et al. [23] supported that the specificity, sequence, and extent of extrinsic RC and ulnocarpal traumatic ligament disruptions are not fully understood, vary with injury severity and may differ in cases of dorsal as opposed to palmar subluxation or dislocation.
RC fracture-dislocations are frequently associated with ulnar-sided injuries and only a few cases have been reported in the literature, where this injury was associated with dislocation of the distal radioulnar joint [7, 22, 38, 71, 85]. Fourteen of 27 patients reported by Dumontier et al. [38] presented with an injury of the ipsilateral distal radioulnar joint and one of them had an irreducible dislocation due to the interposition of the flexor digitorum profundus of the small finger. Extensor carpi ulnaris [85], the dorsal part of the sigmoid notch where the dorsal radioulnar ligament is attached [71], or the flexor profundus tendons and the ulnar nerve and artery [22], have all been implicated as possible causes obstructing the reduction. Graham [73] supported that the association of RC dislocation with ulnar-sided injuries, indicates even more severe tissue trauma and that the path of injury propagates from the radial to ulnar side with the forces not fully dissipated to the RC joint, ongoing ulnarly and producing the ulnar-sided injuries. He also stated that ulnar-sided injuries were more common in the small fragment variant compared to the large fragment fractures, in almost a 2:1 ratio. Since, the ulnocarpal ligaments do not have proximal osseous insertion but take origin from the volar radioulnar ligament, they either rupture in their mid-substance or avulse with or without osseous fragments from their insertion at triquetrum or lunate bones.
It is generally accepted that there are four distinct fracture types of the ulnar styloid process (tip, midportion, base horizontal, and base oblique) and the level of the styloid fracture is relevant to the risk of instability development of the DRUJ [91]. Nakamura et al. [92] assessed the relevance of each of the four levels of ulnar styloid fracture on DRUJ stability in cadaveric wrists and found no instability in the styloid tip or midportion fractures, up to a 20 % loss of stability in basal horizontal fractures, while basal oblique fractures produced up to 70 % loss of stability, as it is more likely to disturb the foveal attachment of the radioulnar ligaments. Wide displacement of any type of ulnar styloid fracture was also recognized as a significant risk for development of DRUJ instability [91, 93]. However, it is believed that the presence of an ulnar styloid fracture is no longer considered an absolute indicator of DRUJ instability regardless of the fragment size and displacement [94, 95], but only as a risk factor [96]. Atzei and Luchetti [97] classified the peripheral tears of the TFCC (of the deep and the superficial limbs of both dorsal and palmar radioulnar ligaments) and their relation to the fractures of the ulnar styloid. A small number of cases has been reported in the literature where RC dislocation was associated with dislocation of the distal radioulnar joint [7, 18, 22, 71, 85].
By excluding patients treated with methods that preclude the ability to describe the pathoanatomy of the injury, i.e., conservative treatment (5 patients) or closed reduction, percutaneous wires and/or external fixation (4 patients), twenty six patients were treated operatively, mostly with combined approach and their surgical findings were recorded. A single approach (1 volar and 1 dorsal) was used in 2 patients, a double approach (dorsal and volar) in 18, and a triple approach (dorsal, volar, ulnar) in 6 patients.
Four patients presented RC dislocations and 22 patients were of RC fracture-dislocation type. According to the direction of the dislocation, there were 19 dorsal (12 pure dorsal, 4 dorsoradial, 3 dorsoulnar), 5 volar, and 2 multidirectional dislocations. All were closed injuries.
7.1 Surgical Findings
-
1.
In all cases, the ligamentous or osseo-ligamentous injuries involved both the dorsal and volar sides of the RC joint.
-
2.
Of 22 patients with RC fracture-dislocations, 19 had fractures of the radial styloid, two patients had an osseous avulsion of the dorsoulnar corner of the distal radius and one patient had a combination of the above injuries.
-
3.
Of 20 patients with fractures of the radial styloid, no one had fractured the entire radial styloid in dorsovolar dimension, independently of its width. The dorsal styloid segment was involved in 6 patients, the volar styloid segment in 3 patients, and a combination of both segments was found in 11 patients (Fig. 8.7a–e). It was difficult to detect radiographically the combined segments of the fractured radial styloid; it was feasible only operatively. Concerning the size of the radial styloid fragment we considered as: Type I the fracture of the tip of radial styloid, type II the fracture through the scaphoid fossa, and type III the fracture exiting at the level of the scapholunate interval. Postreduction X-rays (PA view) revealed that in the dorsal styloid segment fracture type there were 5 type III and 1 type II fractures, in the volar styloid segment fracture type all three fractures were of type II and in the combined segments group there were 4 type II and 7 type III fractures (Fig. 8.8).
Fig. 8.7 
A seemingly entire radial styloid fracture in a dorsal RC fracture dislocation (a) concerned only the dorsal part (b), while volarly the RC ligaments deracinated from the volar radial rim (arrows) (c); 8 years after open reduction and internal fixation with combine approach, stenosis of the radiolunate joint was noticed (d, e)
Fig. 8.8 
Correlation between the 3 types of radial styloid fractures with the ligamentous attachments of the volar RC ligaments. With permission from [127]
-
4.
Fractures of radial rims were either of compression or avulsion type depending on the direction of the dislocation. The direction of the dislocation coincided with the compression side of the radial rim, while the opposite radial rim had an avulsion type of fracture (Fig. 8.9a–h). Usually the osseous injury of the dorsal radial rim was double: there was a larger sized fragment from the dorsal half of the radial styloid and a smaller sized simple or comminuted fracture of the radial rim, ulnar to the Lister’s tubercle which involves the attachment of the DRC ligament (Fig. 8.10). In 3 of our cases, the wrist was displaced in dorsal and ulnar direction and in all 3 cases, apart from other injuries, an avulsed osseous fragment was noticed, originating from the dorsal rim of the sigmoid notch, causing serious derangement of the DRUJ (Fig. 8.11a–d). The osseous fragments from the volar radial rim were sometimes rotated by 90°–180°, since the volar are shorter than the dorsal RC ligaments (see Fig. 8.9b). There were 10 dorsal rim fractures, 4 volar and 4 combined dorsal and volar rim fractures.
Fig. 8.9 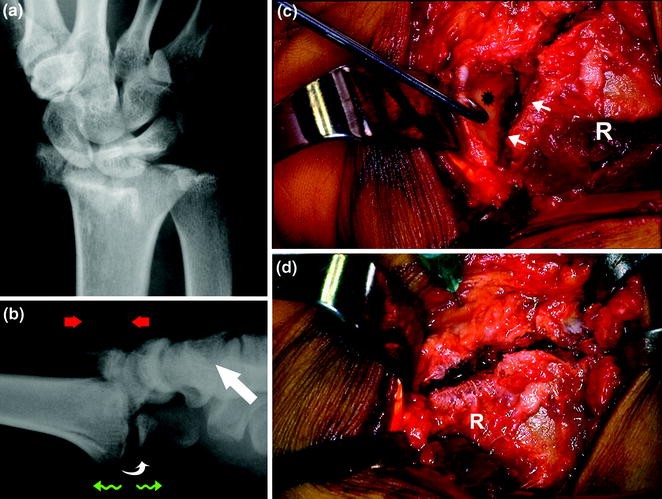

A dorsally directed RC fracture-dislocation produced compression to the dorsal radial rim, while the distracted volar radial rim was rotated by 180° (curved arrow) (a, b), so that the articular cartilage was facing the fractured surface of the distal radius (asterisk) (c); derotation of the fragment (d); postoperative radiographic appearance indicated the wire-loop fixation, used for the stabilization of the rotated ulnovolar fragment (e, f); final x-rays 9 years postoperatively (g, h). With permission from [127]
Fig. 8.10 
In dorsal RC fracture dislocations, the osseous injury is frequently comprised of a larger fragment, which corresponds to the dorsal part of the radial styloid and a smaller, simple, or comminuted fragment concerning the dorsoulnar radial rim. With permission from [127]
Fig. 8.11 
Male, 27 years old, polytrauma patient with a dorsoulnar RC dislocation. White arrows indicate an avulsed osseous fragment from the dorsal rim of the sigmoid notch, while black arrows indicate an osteochondral fragment originating from the dorsal surface of the SL complex (see Fig. 8.5) (a, b); the dorsal approach revealed the avulsed fragment from the dorsal sigmoid notch (asterisk), while the black arrow indicates the ulnar head (c); postop x-ray (d). With permission from [127]
-
5.
A wide range of injuries of the proximal carpal row was noticed in 11 patients (42 %), all of which were discovered intraoperatively: (a) Osteochondral defects of adjacent bones of the proximal carpal row comprising the interosseous ligaments (3 patients; two at scapholunate junction and one at lunotriquetral junction) (Figs. 8.12, 8.5c), (b) isolated rupture of the interosseous ligaments (4 patients; two of scapholunate and two of lunotriquetral ligament) (Fig. 8.13a–c), (c) chondral defects of isolated bones (2 patients; at proximal scaphoid and at proximal lunate respectively) (Figs. 8.13a–c, 8.4a), (d) fractured bones (2 patients; lunate and triquetrum respectively) (Fig. 8.14a–k).
Fig. 8.12 
Male, 28 years old. In a volar RC fracture dislocation the dorsal approach disclosed an osteochondral fragment from the dorsal surface of the LT complex, comprising the dorsal LT ligament (asterisk) (T triquetrum, L lunate, R radius) (The case is also illustrated in Fig. 8.25)
Fig. 8.13 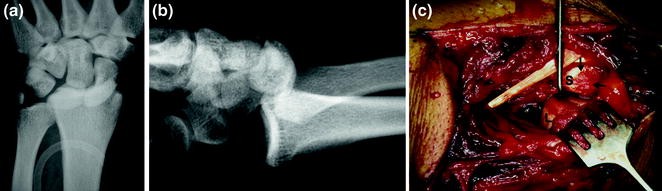
Male, 24 years old with a dorsal RC dislocation (a, b); the dorsal approach revealed a ruptured SL ligament and a chondral defect from the dorsal scaphoid (arrows) (S scaphoid, L lunate) (c). With permission from [127]
Fig. 8.14 

Male, 21 years old, polytrauma patient. PA view of a reduced volar RC fracture dislocation. The arrow indicates a dubious fracture of the lunate(a); different stress views revealed that the RC joint was stable only in dorsal direction (b), while in volar (c), ulnar (d), and radial direction (e) the instability of the joint was apparent; during dorsal approach, a comminuted fracture of the lunate was found (arrows) in association with a fracture of the radial styloid (asterisk) (f); the palmar approach revealed a comminuted fracture of the volar radial rim (arrows) (g); postoperative radiographic views (h, i); the final x-ray views 4 years later (j, k)
-
6.
In six patients, free osteochondral fragments were found intra- or extraarticularly, originating either from carpal bones or from the distal radius. In 2 cases of dorsal RC fracture-dislocations, during radiological examination, two sizable fragments were detected at the volar surface of the joint. Indeed, the palmar approach revealed the existence of osteochondral fragments at the level of the RC joint; however, detection of their source was difficult. The dorsal approach in both cases revealed that these osteochondral fragments originated in one case from the dorsoulnar rim of the distal radius (Fig. 8.15a–g), while in the other case from the dorsal surface of the scapholunate complex (see Figs. 8.5, 8.11). The fact that dorsal anatomical structures were found palmarly (also the opposite possibly applies), is on one hand of surgical interest, but on the other hand, it is indicative of the amplitude of the applied forces and of the complexity of the mechanism of injury.
Fig. 8.15 

Male, 23 years old, with a dorsal RC fracture dislocation. An osseous fragment of unknown origin (arrow) and a fracture of the radial styloid were apparent in the initial (a, b) and reduced (c) x-ray views; the volar approach with the joint dislocated showed the osteochondral fragment (arrow) located distal to the lunate fossa (asterisk) (d); dorsally, a large fractured fragment of the radial styloid and two smaller osseous fragments of the dorsoulnar radial rim were apparent. The arrow indicates the fragment that was found volarly after its relocation (e); postoperative x-rays (f, g). With permission from [127]
-
7.
The RC ligaments were usually avulsed from the volar or dorsal radial rims, but in 7 patients they were avulsed from carpal bones with or without small osseous fragments. Specifically, the short radiolunate ligament was avulsed from the lunate (5 patients) and the dorsal RC ligament was avulsed from the triquetrum (2 patients) (Fig. 8.16a–g).
Fig. 8.16 
Male, 56 years old, with a dorsal RC fracture dislocation (a, b); volarly the radiocarpal ligaments were deracinated from their attachments to the distal radius (white arrows), while the short RL ligament was avulsed with an osseous fragment from the lunate (black arrows) (c) (R radius, L lunate); bone anchors were used for reconstruction (d, e); radiographic appearance after 7 years (f, g). With permission from [127]
-
8.
In 3 patients (2 with volar and 1 with multidirectional dislocation) there was an extensive rupture of the floor of the dorsal retinaculum (Fig. 8.17a–f), while in the patient with the multidirectional dislocation, the extensor and abductor pollicis longus were ripped-off from their musculotendinous junction (Fig. 8.18a–h), a finding indicative of the rotational component of the mechanism of injury.
Fig. 8.17 
Female, 60 years old, polytrauma patient. In a volar RC fracture dislocation (a, b); the dorsal approach revealed an osteoperiosteal avulsion from the 1st extensor compartment (curved arrow) that resulted in exposition of the corresponding tendons, while the DRC ligament was avulsed from the dorsal radial rim (small arrow) (c); the volar radial rim was comminuted (arrows) (asterisk pronator quadrates) (d); radiographic appearance 6 months later (e, f). With permission from [127]
Fig. 8.18 

Male, 57 years old. Multidirectional closed RC dislocation, produced in an effort to release the hand that was trapped in an agricultural machine. The PA view showed avulsion fractures of both radial and ulnar styloids and overlapping of the LT joint (a); the L view demonstrated that the wrist was displaced volarly and a sizeable osseous fragment that was proven to have come from the dorsal surface of the triquetrum (b); the dorsal approach revealed that the EPL and APL extensor tendons were ripped-off their musculotendinous junction (arrows) (c); the RC joint was unstable in all directions; the osseous fragment from the dorsal side of the triquetrum (curved arrow), the fracture of the radial styloid (small arrow), the ripped-off tendon (double arrows), and the articular surface of the distal radius (asterisk), were demonstrated through the dorsal approach (d); postoperative x-rays (e, f); the final radiographic appearance 13 years later (g, h). With permission from [127]
-
9.
Seventeen patients (65.3 %) had associated injury of DRU joint (fracture through the base of the ulnar styloid in 14 patients, an osseous avulsion from the dorsal sigmoid notch of the dorsal radioulnar ligament in 3 patients, and a Type IV rupture of the TFC in 1 patient).
-
10.
The two multidirectional and one volar dislocation had in addition a complete rupture of the volar ulnocarpal ligaments (Fig. 8.19).
Fig. 8.19 
The rupture of the ulnocarpal ligaments (arrows) that was found in 3 of our cases (mainly multidirectional dislocations) (T triquetrum, L lunate). With permission from [127]

















Based on our surgical findings, we could define the pattern of osseo-ligamentous disruption as follows (Fig. 8.20):

The pattern of osseous (red lines) and ligamentous (green lines) disruption that was found in different types of dorsal, volar, and multidirectional dislocations (see text for details)
In dorsal dislocations, there were roughly 4 types of injuries:
- Type I (4 cases):
-
Dorsally, a double osseous injury (separate fragments, radially and ulnarly to Lister’s tubercle) and volarly a purely ligamentous injury
- Type II (7 cases):
-
Dorsally a double osseous injury and volarly a double osseoligamentous injury. Usually the RC ligaments were detached from the ulnar side of the volar radial rim, while the radial side showed an avulsion fracture fragment. Less often, the reverse was true
- Type III (3 cases):
-
Double osseous or comminution on both dorsal and volar sides
- Type IV (5 cases):
-
Dorsal and volar, mainly ligamentous injuries, which were sometimes associated with small osseous fragments of avulsion type, originating from the radial styloid (either side) or from the dorsoulnar side of the radius
In volar dislocations we found 2 types of injuries:
- Type I (4 cases):
-
Dorsally, purely ligamentous and volarly a double or comminuted osseous injury
- Type II (1 case):
-
Purely ligamentous injuries on both sides
In the 2 cases with multidirectional dislocations, we found a purely ligamentous injury on both sides with rupture of the ulnocarpal ligaments. One of those cases exhibited fracture of the tip of the radial styloid.
8 Classification
Two classification schemes have been discussed extensively in the literature: Dumontier et al. [38] classified RC dislocations into two types: type 1 included pure dislocations with or without fracture of only the tip of the radial styloid, a fracture involving less than one-third of the width of the scaphoid fossa, postulating that the RC ligaments were torn off the radius; type 2 included dislocations with associated fracture of the radial styloid involving more than one-third of the scaphoid fossa, postulating that most of the RC ligaments were still intact and attached to the radial styloid fragment.
Moneim et al. [9] classified these injuries into type 1 and type 2 according to the integrity of the intracarpal ligaments. In type I dislocation, the carpus moves as one unit on the distal radius whereas in type II, an associated intercarpal dislocation is also present. He presented 7 cases and 3 of them were characterized as type II dislocations. According to the author, type II dislocations represent a more complex pattern, with a graver prognosis. It should however, be noted, that all 3 cases characterized as type II RC dislocations were in fact trans-styloid perilunate injuries with volar dislocation of the lunate, from which RC fracture dislocations must be differentiated.
The frequent occurrence of intracarpal injuries along with a RC dislocation is undeniable, but they are just associated injuries and do not deserve to constitute a particular type of injury. Besides, all these injuries from our series were discovered intraoperatively and none was recognizable by the preoperative x-rays.
Since both the aforementioned classifications are based on radiographic findings and do not take into account the pattern of osseoligamentous injuries, the direction of the dislocation or the ulnar-sided pathology, it is obvious that both must be modified.
A third classification was that of Graham [73] who considered RC dislocations as “inferior arc” injuries, in addition to the existing injury patterns: the “greater” and “lesser arc” injuries. He stated that RC dislocations could be classified as: (a) purely ligamentous disruptions, (b) dislocations with a “large fragment” styloid fracture, starting in the area of the previous physeal scar and entering the joint near the crista separating the scaphoid and lunate fossae, and (c) dislocations with a “small fragment” fracture, which represents avulsion or impaction injuries of the volar or dorsal margins of the distal radius.
Bilos et al. [7] classified these injuries into four general types: dorsal, volar, radial, and ulnar, depending on the direction in which the carpus is displaced.
Bozentka and Beredjiklian [98] commented on the need to include in the classification schemes other important factors, such as the direction, the presence of associated neurovascular injury, and the presence of associated intercarpal ligamentous injuries.
Mainly relying on surgical findings we propose a new classification based on five parameters (chronicity, pathoanatomy, direction, associated wrist injuries, and complexity). Using this classification, a RC dislocation or fracture-dislocation should be presented with information on all five parameters (Table 8.3).
Chronicity: RC dislocations or fracture-dislocations are differentiated into acute and gradually developed. The latter group includes ulnar translation as sequelae of an already treated RC dislocation or a remote consequence after a subtle RC ligament rupture. Special mention deserve those cases presented in the literature, where the RC subluxation or dislocation was associated with a small fragment from the ulnovolar articular surface of the distal radius [11, 16, 23, 30, 33, 99, 100]. Since all these cases were closely reduced and after a period of time the subluxation recurred, they could belong to the gradually developed group (Fig. 8.21a–l).


Male, 32 years old, motorcycle injury. A case of a gradually developed RC subluxation after fracture of the ulnovolar radial rim. The PA view demonstrated an avulsed fragment from the triquetrum (a); L view showed an undisplaced fracture of the volar radial rim (b); he was treated initially with a splint for 3 weeks. The symptoms persisted after splint removal and physiotherapy was recommended. Six months post-injury, the PA view showed radiocarpal joint overlapping, volar RC subluxation, and new bone formation in association with the displaced ulnovolar fragment was detected (double arrows) (c, d); a CT-scan showed the displaced fragment from the triquetrum (e); the volar approach revealed the articular step-off (double arrows), the new bone formation (asterisk), and the raised capsuloligamentous flap (curved arrow) (f); with intraarticular osteotomy the ulnovolar fragment was raised (curved arrow) (g); it was reduced and fixated using 2 K-wires (h); the RC joint was reduced and stabilized with a transfixing pin and the wrist joint immobilized with an external fixator; postoperative x-rays (i, j); final radiographic appearance 18 months later (k, l). With permission from [127]
Pathoanatomy. RC dislocations are differentiated into purely ligamentous or equivalent, which include, the tip of the radial styloid or a small ulnovolar fragment. RC fracture-dislocations are differentiated according with the location of the fracture into: radial styloid (dorsal or volar part or combinations), radial rim (dorsal or volar or combined rims), and dorsoulnar fragment.
Direction. The direction of the dislocation allows us to assume in a great extent the underlying lesions. Thus, these injuries are divided into dorsal, volar, ulnar, combinations (dorsoradial, dorsoulnar, radiovolar, or ulnovolar), and multidirectional.
Associated injuries. These are related to concomitant injuries located in the vicinity of the dislocated wrist. They may concern: DRUJ, ulnocarpal or interosseous ligaments, osteochondral fragments, fractured carpal bones, ruptured tendons or muscles, neurovascular injuries, and the status of the dorsal retinaculum.
Complexity. This parameter clarifies if the dislocation is reducible or not and if the dislocation is open or closed.
9 Diagnosis
As for most violent traumas, these injuries have been reported mainly in males and usually of young age.
The patient with RC dislocation typically presents with a painful, swollen, and deformed wrist. The unreduced RC dislocation results in a significant deformity, with the wrist and hand being displaced dorsally or volarly in relation to the forearm axis (Fig. 8.22). Most commonly these injuries are the result of high-energy injuries (fall from height, traffic accidents, industrial injuries).

The dislocated RC joint showed considerable deformation. With permission from [127]
Graham [73] highlighted three basic physical findings in a reduced RC dislocation: the amount of swelling, pain on both the radial and ulnar sides of the wrist, and a semi-supinated posture of the wrist-hand unit at rest.
For radiological diagnosis the P-A and the L neutral rotation views seem to be sufficient. The characteristic findings in the P-A projection are the carpus overlapping the distal radius and the frequent occurrence of fractures of the radial and/or ulnar styloids (see Fig. 8.18a). The L view demonstrates the direction of the RC dislocation while marginal rim fractures are best evaluated on the L view.
Although the dislocated wrist reveals the magnitude of the injury and is treated with the utmost significance, particular attention must be drawn to those cases that were spontaneously reduced and are in danger to be treated superficially with the application of a simple splint. In such cases the injury must be suspected based on the history and clinical findings, while the presence of palmar carpal subluxation and/or ulnar translation are an indication of the magnitude of such an injury. On the P-A view, alignment of the wrist is evaluated by examining the position of the lunate relative to the radius, with a minimum of two thirds of the lunate articulating with the distal radius [2]. Any disruption of the three Gilula’s arcs [101] must be recorded and properly evaluated.
Periarticular rim fractures of the distal radius and/or radial and ulnar styloid avulsion fractures may also be present [73], as well as residual subluxation of the wrist. Distraction films under local or general anaesthesia will better reveal the magnitude of the injury (Fig. 8.23).

The distraction view provides useful information for the injury. Excessive widening of the RC joint indicates the magnitude of the RC ligaments’ injury, while arrows indicate the fracture of the radial styloid and an osseous fragment from the volar radial rim
Although not mandatory, a CT scan can assist in the evaluation of cortical rim fractures, fracture depression of the articular surface, and the configuration of the DRUJ.
10 Associated Injuries
Since these injuries are usually the result of high-energy injuries, open wounds [3, 7, 15, 22, 34–36], and associated injuries (often life-threatening) to other organ systems are common. The percentage of such injuries in the literature ranges between 41.6 and 80 % [9, 35, 36, 38]. Associated injuries within the same limb are not uncommon [7, 19, 74]. In our series 38.4 % (10 of 26) of the patients had associated injuries from other organs and 11.5 % (3 of 26) had associated injuries of the same limb.
Usually the median and less common the ulnar nerve may be involved [7, 9, 12, 15, 18, 22, 28, 31, 34, 35, 68, 71], but following reduction, they are usually fully restored [7, 9]. Even acute hand ischemia [7, 12, 15, 28, 35] and compartment syndromes of the hand and forearm [102] have also been reported.
The magnitude of rotational force required for RC dislocations may be of such amount, that it may result in tendon rupturing or detachments. Le Nen et al. [12] reported ruptures of the extensor carpi ulnaris and of the corresponding extensor of the little finger. Others [22, 35] presented a case of flexor tendon rupture or even a case with detachment of the pronator quadratus [15]. In one of our cases, the extensor and abductor pollicis longus were deracinated from their musculotendinous junction (see Fig. 8.18c).
11 Management
There have been reports of successful treatment with: closed reduction and casting [11, 20, 29, 38, 103], closed or open reduction and percutaneous pinning [5, 9, 15, 21, 31, 38], open reduction and casting [34, 104], open reduction and internal fixation with ligamentous repair [7, 9, 12, 16, 38, 52, 71, 75, 102]. Due to the rarity of these injuries, there is no unanimously accepted method for their management.
The majority of these dislocations are relatively easy to reduce, there are therefore cases that, being spontaneously reduced, escape diagnosis. The reported cases of a non-reducible dislocation are rare. In one case there was tendon interference [22], whereas in two other cases there was bone fragment interference [32, 71]. Inability to perform closed reduction in 4 out of 6 cases, due to interference of ligamentous or bone origin has also been reported [15].
In several literature reports, mostly of isolated cases, closed reduction, and cast immobilization are advised [9, 11, 20, 29, 33], in dorsiflexion for the dorsal and in palmarflexion for the palmar dislocations [33, 39]. However, RC dislocations treated nonsurgically have been reported to develop palmar subluxation, ulnar translation DISI or VISI instabilities [11, 14, 17, 20, 21, 26, 29, 30, 75]. Certainly everyone agrees that open, non-reducible dislocations and those accompanied by neurovascular injury must be managed with open reduction [1, 15]. Moneim et al. [9] suggests the attempt of closed reduction and casting for type I injuries and open reduction, internal fixation, and ligamentous repair for type II injuries. However, many reports [35, 36, 38, 68, 105–107], plead for open reduction since, if the RC ligamentous mechanism is not repaired, wrist function will be severely compromised with instability and/or subluxation later [102].
The concern whether these injuries should be managed conservatively or surgically, is directly related to the unstable nature of these injuries (Fig. 8.24a–d). There are many cases in the literature that were initially managed with closed reduction and casting, but the wrist was subluxated early or late [9, 15, 21, 38]. In our series 7 out of 26 patients lost their reduction and were treated operatively with a delay of 4–20 days. Schoenecker et al. [15], supports that even with open reduction, maintaining the anatomical reduction is difficult, especially when a compressive fracture of the dorsal radial rim coexists. Conversely, Fernandez et al. [68] rationale was based on the fact that rupture of the palmar RC ligaments predisposes the wrist to ulnar translocation, which will be observed if there is no ligamentous repair. In addition, one more reason supporting surgical management is for the removal of small cartilaginous and osteochondral fragments, which frequently interfere in the joint and obstruct its reduction.

A dorsal RC fracture-dislocation which was treated with closed reduction and cast application (a, b), resulted in VISI malalignment (c, d)
If for any reason closed reduction is chosen, a basic requirement is to ensure that during the healing period, the anatomical alignment of the bones and joints will be preserved, in order for intraarticular fractures to be united without articular incongruity and most importantly, the RC joint to be axially aligned so that the ruptured ligaments can heal with proper tensioning. Prerequisites for the above are: frequent radiological control, good application of the cast, prompt identification of wrist displacement (palmar, ulnar or dorsal), detection of possible injuries of the interosseous ligaments, and sufficient time for immobilization (6–8 weeks). Alternatively, following closed reduction and once we have ensured that the RC joint has been anatomically reduced, we can immobilize the joint using K-wire or external fixation.
There is no consensus as to which is the most appropriate approach for open reduction. The approach should be dictated by the direction of the dislocation, the fracture pattern, the associated carpal bone injuries, the presence of neurovascular injury and if we are dealing with an open or closed injury. Moneim et al. [9] for cases necessitating open reduction proposed combined approaches. Mudgal et al. [36] advised the use of palmar approach in the presence of a neurological defect, dorsal approach if the dorsal radial rim is involved and ulnar approach when the ulnar styloid requires fixation. Dumontier et al. [38] believed that group 1 patients should be treated with reattachment of the ligaments through a volar approach. In group 2 patients, the ligaments are still attached to the radial fragment and in this group of patients, exact articular reduction should be performed through a dorsal approach. Lipton and Jupiter [102] supported an extended palmar approach in cases of dorsal RC dislocation with neurovascular compromise, in order to repair in addition the volar ligaments, whereas if there are dorsal avulsion fractures or if the dislocation is volarward, then the surgical approach is through an extensive dorsal approach. The Mayo clinic group, as quoted by Idler [86], has recommended palmar and dorsal approaches for ligament repair of the radiocapitate, long radiolunate, ulnocarpal, and dorsal radiotriquetral ligaments.
Considering that by definition, RC dislocations or fracture-dislocations constitute double-sided injuries and that structures important for wrist stability are located both dorsally and volarly, we regard the combined approach as the most appropriate. In any case of an acute dislocation or fracture dislocation, regardless of its direction, we consider the palmar approach most important in order to repair the volar RC and ulnocarpal ligaments as well as any fractures of the volar radial rim, since these structures are crucial for wrist stability. In the majority of cases dorsal approach is also required, especially in cases of compressive fractures of the dorsal radial rim, for the fixation of a potential dorsal part of a fracture of the radial styloid or to evaluate the integrity of proximal carpal row bones. Sometimes, when dorsally the injuries are purely ligamentous or are associated with small avulsed fragments or with subperiosteal detachment of the dorsal extensor compartments, then dorsal approach may be avoided, on the premise that the volar structures have been restored and the RC joint is maintained reduced and properly aligned for 6–8 weeks.
In cases of DRUJ instability or of a displaced fracture at the base of the ulnar styloid, a separate ulnar approach is frequently necessary.
Based on the literature and on personal experience, we consider the following steps as necessary for open reduction:
-
The patient is positioned supine on the operating table. An arm table is positioned beneath the affected extremity and the procedure is performed under tourniquet control. During anesthesia, useful information concerning the magnitude and direction of dislocation can be acquired under image intensifier, through manipulation of the wrist (longitudinal traction and dorsal, volar, radial, and ulnar displacement) with the forearm stabilized (Fig. 8.25a–h). In addition, PA and L radiographs with the RC fracture dislocation reduced are recommended.
Fig. 8.25 

Male, 28 years old. Volar RC fracture-dislocation (a, b); stress views in different directions showed that the RC joint was stable only in dorsal direction (c–f); in volar displacement view, the osseous fragment indicated with arrows, was shown to have originated from the dorsal LT complex (see Fig. 8.12); postoperative X-rays (g, h)
-
Depending on the nature and the time elapsed from injury, an external fixator may be applied from the initial stages of operation, so that the wrist is kept in gross alignment and mild distraction, as it facilitates the exposure of the capsuloligamentous structures. The more delayed the injury’s treatment is, the greater the need for the application of the external fixator at the initial stages of the operation. Its placement on the radial side of the wrist does not obstruct the impending approach.
-
The extended carpal tunnel approach is used to decompress both the carpal tunnel and Guyon canal if needed and to fully evaluate the radio-volar injuries by displacing the FPL and the median nerve radially and the remaining flexor tendons ulnarly. The ulnovolar injuries are assessed by displacing the flexor tendons radially. Less often and depending on the extent of injuries, Henry’s approach is sufficed. The joint is irrigated and the osseoligamentous lesions are recorded in detail. The palmar RC ligaments are either detached from their insertions to the volar radial rim or from carpal bones (usually the lunate) or avulsed with a small osseous fragment from their insertions. The reattachment of ligaments is achieved using nonabsorbable sutures through transosseous holes or bone anchors that are inserted at the sites where the ligaments were detached (Fig. 8.26a–h). Depending on the size of the fractured fragments of the volar rim, their fixation is achieved using K-wires, small plates, or a wire-loop [108] (Figs. 8.27a, b and 8.9g–h). The possibility of fragmentation of the bone fragments must always be kept in mind, both during manipulation and stabilization.
Fig. 8.26 

Male, 31 years old. Dorsal RC fracture-dislocation (a, b); with the dorsal approach, a double osseous injury of the dorsal radial rim (arrows) was evident after raising the dorsal capsuloligamentous flap (c); volarly, the RC ligaments were deracinated from the volar radial rim, except for the short RL ligament that was detached with an osseous fragment from the lunate (arrows) (d); reconstruction was accomplished using bone anchors (e, f); final x-rays 1 year later (g, h). With permission from [127]
Fig. 8.27 
The wire-loop technique which was used for the fixation of an avulsed small ulnovolar fragment (arrow)





In cases where the healing capacity of the volar RC ligaments is questionable, especially in delayed cases, augmentation using tendon grafts is an option. Originally Rayhack et al. [52] and more recently Maschke et al. [89] described a cadaveric model for reconstructing the radioscaphocapitate using the brachioradialis tendon, while Obafemi and Pensy [109] applied the same technique in a patient with palmar RC dislocation, in order to reconstruct the radioscaphocapitate ligament and to reinforce the dorsal capsular repair.
-
The dorsal approach is longitudinal over Lister’s tubercle, the third compartment is exposed if intact and the EPL tendon is displaced radially. The integrity of the dorsal retinaculum is recorded; if it is intact, subperiosteal elevation of the second and fourth compartments allow for a full evaluation of the dorsal injuries, since the dorsal capsule is already ruptured. At this stage and after joint irrigation, the injuries of the dorsal surface of the radius (from radial to ulnar) and the integrity of the chondral surfaces and the interosseous ligaments of the proximal carpal row bones are evaluated. Any entrapped chondral or osteochondral fragments are debrided or preserved for later transfixation. The integrity of the dorsal RC ligament must be checked throughout its course. In cases of compressive fractures of the dorsal radial rim, the insertion of cancellous bone grafting is necessary to support the articular surface, using small buttress plates for fixation [36, 102, 110] (Fig. 8.28a–d). In cases with purely ligamentous injuries, small osseous fragments or subperiosteal detachment of the dorsal cortex, there are many alternative stabilizing methods including K-wires, bone anchors, screws or tension band wiring (Fig. 8.29a–d). Any injury of the proximal carpal row bones is treated accordingly and stabilized with K-wires.
Fig. 8.28 
A dorsal RC fracture dislocation (a, b); the sizable dorsal osseous fragments were reduced and fixated using 2 small buttress plates (c, d). With permission from [127]
Fig. 8.29 
Male, 23 years old. Motorcycle injury. A dorsal RC fracture-dislocation (a, b); a cannulated screw; and bone anchors were used for stabilization after combined approach (c, d)
-
As we previously noted, the fracture at the base of the ulnar styloid may indicate a destabilization of the DRUJ. This however is not absolute, as it is not certain that the fracture of the tip of the radial styloid has no effect on joint stability. Consequently, at the end of a stable reconstruction of the RC joint, the stability of the DRUJ is assessed. This information will be provided with passive anteroposterior glide of the distal ulna relative to the distal radius in positions of neutral rotation, full pronation and full supination, and whether the ballottement test demonstrates or not a hard end point. Thus, in cases of DRUJ instability or displaced fracture of the base of the ulnar styloid, tension band wiring, or TFCC suturing are recommended [36, 102]. An additional type of fracture which is always associated with instability of the DRUJ and need to be fixated, is an avulsion fracture of the dorsal sigmoid notch, which pertains the TFCC (usually accompanies the dorsoulnar RC dislocations). In such cases a radioulnar transfixing pin is required.
-
It is necessary, using the external fixator, to maintain the RC joint in a reduced position throughout the healing process for 6–8 weeks and to protect the reconstructed RC ligaments from slackening. In highly unstable injuries or when the reconstruction is suboptimal, an additional RC pinning is essential and is usually inserted percutaneously or through a small incision (protecting the sensory branches of the radial nerve), from the radial aspect of the radius and through the lunate towards the wrist (Fig. 8.30a–i).
Fig. 8.30 

Male, 32 years old, with a dorsal RC fracture-dislocation (a, b); the uprooted volar RC ligaments were reattached with transosseous sutures (c, d, e); the RC joint was stabilized using RC pinning (f, g); final x-rays after 2 years (h, i). With permission from [127]
-
The immobilization of the RC joint is maintained for 6–8 weeks and physiotherapy consisting of active and passive wrist mobilization, must be initiated.




12 Outcome
The conclusions concerning the outcome of these injuries present three drawbacks: First, there are no large series with patients with RC dislocations; second, the existing studies are dealing with mixed type of injuries, which are treated with various methods; and third, there are no long-term follow-up reports on the outcome.
Despite being complex injuries, favorable clinical results have been reported with both methods, closed or open. However, there is discrepancy between clinical and radiological results, with the latter being clearly worse, something which renders unknown the long-term consequences. The anatomical reduction and maintenance of the proper alignment of the RC joint throughout the healing process, are the factors that will ensure a good functional result, regardless of the method chosen.
Factors predictive of an inferior clinical and/or radiological outcome include: open injuries, associated severe nerve injuries, purely ligamentous dislocations, intercarpal ligamentous injuries that are initially missed and remain untreated and associated DRUJ injuries. The compressive type of fractures of the radial rims have worse prognosis than avulsion fractures, since the former, could be associated with articular cartilage injury or collapsing due to comminution or osteonecrosis, because of devascularization of small fragments (Fig. 8.31a–k). In addition, fracture fragments associated with unfavorable results if ignored or inadequately treated, are the ulnovolar (Fig. 8.32a–k) and the dorsoulnar fragments of the distal radius. Both are implicated in ulnar translocation and the latter in DRUJ subluxation.


Male, 26 years old, after a motorcycle injury with a volar RC fracture-dislocation (a, b). He was treated elsewhere with a dorsal approach, while K-wires were used in an effort to fixate the fractured fragments. In addition a tension band wire was used for the minimally displaced ulnar styloid fracture. On the 3rd postop day and despite the external fixation, the RC joint displayed volar subluxation and the patient was sent for further treatment (c, d); with palmar approach the fractured fragments were reduced and fixated using K-wires. An additional K-wire was used percutaneously for a suspected SL ligament injury (e, f). 12 years later the x-rays showed fragmentation and osteonecrosis of the radial styloid (g, h), while the patient had a satisfactory ROM with only cold weather symptoms (i–k). With permission from [127]


Female, 27 years old. Car accident. Despite the initial radiographs which were indicative of RC joint instability (overlapping of radioscaphoid joint and fracture of the ulnovolar fragment) (arrows) (a, b), she was treated with a below elbow cast for 3 weeks. Three months later the volarly subluxated RC joint and the displaced ulnovolar fragment (arrows) were depicted in x-rays (c), 3D CT-scan (d, e) and CT-scan (f); the palmar approach revealed that the short RL ligament (asterisk) was attached to the ulnovolar fragment (arrow), which was detached (g) and reconstructed with 2 bone anchors (h); an external fixator was used for stabilization of the RC joint for 6 weeks (i); final x-rays 2 years postoperatively (j, k). With permission from [127]
Large series in the literature indicate that an overall 30–40 % decrease in total arc of wrist flexion–extension and 20–30 % of grip strength, can be expected following open treatment [2, 35, 38]. Howard et al. [26] highlighted the possibility of weakness development in pronation and supination, which may be the result of residual global laxity of the extrinsic wrist ligaments.
Dumontier et al. [38] concluded that patients with pure RC dislocations (group I) present with good mid-term results, but long-term results are doubtful, since the majority of these patients presented with varying severity of ulnar translocation of the wrist, regardless of the method applied for their management. Conversely, in patients with RC fracture-dislocations (group II), ulnar or palmar displacement of the wrist does not seem to constitute a problem, while long-term results depend upon the quality of fracture reduction.
Schoenecker et al. [15] reported 4 patients out of 6 with arthrosis at 3-year follow-up. The results of Le Nen’s et al. [12] patients showed that 5 out of 6 patients had some narrowing of the RC interval with a follow-up ranging from 3 months to 11 years. Fernandez et al. [68] reported a series of 12 patients treated operatively and after a follow-up of 36 months, 3 of them had radiographic evidence of grade I arthritic changes. Mudgal et al. [36] reporting on a series of 12 patients and after a mean follow-up of 36 months, identified 3 patients as presenting evidence of RC arthritis. Dumontier et al. [38] reported that 6 out of 18 patients that were followed-up for 44 months average, developed RC arthritis (1 out of 5 patients belonging to group I and 5 of 13 patients belonging to group II). Patee and Thomson [111] after a follow-up of 3.2 years reported that 13 of 20 patients (65 %), who were treated with a variety of methods, presented with roentgenographic evidence of posttraumatic arthritis.
Oberladstatter et al. [76] examined 8 patients (9 cases) with Moneim I RC fracture dislocations, who were treated operatively. After an average follow-up of 4.1 years and using the classification system described by Knirk and Jupiter [112], 5 patients (56 %) had stage 1 arthritic changes, three (33 %) had stage 2 arthritis, and 1 patient (11 %) had stage 3 arthritis with total loss of the RC joint space.
Twenty of 26 patients in our series returned for evaluation at a mean of 57.6 months (range, 12–158.8 months). All of them had returned to their original jobs. Eight patients were free of pain, 7 had cold weather symptoms, and 5 patients noted mild pain only with heavy labor. The mean grip strength was 82.7 %, and the flexion–extension arc was 80 % of the contralateral healthy wrist. Four patients had grade 1 arthritic changes (3 with dorsal and 1 with volar RC fracture-dislocations) (Fig. 8.33a, b), 3 patients developed mild ulnar translation (1 with multidirectional dislocation and 2 with dorsal RC fracture-dislocations) (Fig. 8.34a, b), 1 patient developed mild radial translation due to malalignment of the radial styloid, and 1 patient developed VISI malalignment due to disruption of the LT joint.


13 Complications
Limitations in the range of motion and reduction in grip strength are common occurrences regardless of the treatment method applied for these injuries. In addition, posttraumatic arthritis, instability findings and residual volar, dorsal, or ulnar subluxation of the wrist, have been reported as possible complications after the management of these injuries [2, 15, 38, 86].
13.1 Ulnar Translation or Ulnar Translocation
Ulnar Translation [113] or Ulnar Translocation [39] is observed in cases of serious and generalized ligamentous injuries of both the palmar and dorsal sides of the wrist. It could be manifested as either pure ulnar translocation [17, 52, 90, 114, 115] or as sequelae of reduced palmar [23, 26, 30] or dorsal [27] RC dislocations, which were treated with closed or open reduction and inadequate reconstruction of the volar RC and ulnocarpal ligaments (Fig. 8.35a–k). Ulnar translocation of the wrist is more common with purely ligamentous injury patterns [21, 26, 30, 33, 38], while excessive minus variance of the ulna with deficient ulnar buttressing by the TFCC, may be a predisposing factor [52, 116].


Male, 22 years old. Motorcycle accident that resulted in hip dislocation and a wrist injury with an initially normal PA view (a); during examination the wrist was found unstable in multiple directions (b, c, d); the volar RC ligaments (e) and the dorsal capsule including the DRC ligament (f) were deracinated from the radial rims, while the ulnocarpal ligaments were also ruptured (arrows) (g); three absorbable bone anchors were placed volarly and one metallic bone anchor was introduced dorsally, while a small external fixator was used to stabilize the RC joint leaving the midcarpal joint unobstructed for early initiation of dart-throw motion (h, i); 5 years later, the patient although symptoms-free, displayed radiographically ulnar translation (j, k)
Taleisnik [39] distinguished 2 types of ulnar translocation: In type I, the entire carpus, including the scaphoid, is displaced and the distance between the radial styloid and the scaphoid is widened. In type II, the relationship between the distal row, the scaphoid, and the radius remains normal; the scapholunate space is widened and the lunate-triquetrum complex is ulnarly translocated. The distinction between the two types is essential since type I ulnar translocation constitutes a CIND type of instability, while type II is a combination of CIND and CID (SL dissociation) type of instabilities, hence a complex (CIC) type of instability. In type I injuries the failure concerns all RC ligaments, while in type II translocation the radioscaphocapitate ligament is intact but there is complete disruption of the scapholunate and radiolunate ligaments [117].
Schernberg [116] identified four grades of ligamentous lesions leading to complete ulnar translocation. In grade I injury there is only partial disruption of the involved ligament and the joint remains stable under dynamic radiographic examination. A grade II injury corresponds to complete disruption of the involved ligament but does not cause any displacement of the wrist and standard radiographs remain normal. Only passive stress views must be used to reveal this abnormality. Grade III lesions consist of complete disruption of the relevant ligament(s) and permanent displacement of the wrist, which is obvious in the standard radiographs. As there is some contact between the remaining articular surfaces, this condition is also called subluxation. Finally, Grade IV injuries present with dislocation, i.e., complete loss of joint contact between the involved carpal elements. Grade II injuries represent a dynamic pattern of ulnar translocation, while grades III and IV represent static patterns of the instability. Such dynamic patterns of ulnar translocation have been reported [118–120]. A seemingly minor dynamic ulnar translation pattern may progress with time to a major static displacement, as it was clearly demonstrated in at least 3 out of 8 cases presented by Rayhack et al. [52].
Palmar translation of the wrist was found with less ligament disruption than that required for ulnar translation, whereas in all cases of ulnar translation, there was a component of palmar wrist displacement [50, 117].
Different methods of assessing ulnar translation have been reported. The methods using the center of the capitate head [121–123] as a carpal reference should not be used in type II injuries, because only the lunate-triquetrum complex is significantly displaced in these cases. In contrast, when using the lunate as a reference [124–126], if the wrist is slightly radially or ulnarly deviated, the measurements may be unreliable [117].
T he diagnosis of ulnar translation is usually delayed and this renders a difficult problem to be effectively treated [52]. In acute injuries and using a combined approach, the RC ligaments (both palmar and DRC) are repaired or reattached to the distal radius or to the carpal bones using bone tunnels or suture anchors. The palmar ulnocarpal ligaments must also be repaired and during the healing process, i.e., 6–8 weeks, the alignment of the RC joint is maintained by pinning of the radioscaphoid and radiolunate articulation. An additional external fixator may be necessary.
Delayed ligament repairs usually have disappointing results. In such cases ligament repair alone is insufficient to prevent recurrent ulnar translation, while radiolunate fusion after reduction of the carpus, has been described as the most effective form of treatment [39, 52, 68, 116] (Fig. 8.36a–f). However, in patients whose deformity can be passively corrected and without arthritic changes, ligaments augmentation with a tendon strip can be carried out [115]. Maschke et al. [89] using a brachioradialis tendon tried to recreate the stabilizing effect of the RSC ligament in cadavers while Obafemi and Pensy [109] applied the same technique in a patient with a palmar, 2 weeks old RC dislocation, in order to augment the reconstructed palmar and dorsal RC ligaments. Both authors used the same technique (with minor modifications) in which the brachioradialis tendon was stripped proximally of its muscle, leaving the distal insertion at the radial styloid intact. Then a 3.5 mm drill hole was created in the center of the capitate, with passage of the tendon graft through this drill hole from palmar to dorsal and secured to the dorsum of the distal radius with a 4.5 mm suture anchor just distal to Lister’s tubercle.

Male, 31 years old, with injury by a press machine. A dorsoulnar RC fracture dislocation with a sizeable fragment comprising the dorsal part of the lunate fossa and the dorsal sigmoid notch, while the DRUJ was subluxated (a, b); he was treated elsewhere with closed reduction, percutaneously inserted K-wires under image intensifier to stabilize the fractured fragment and an external fixator (c); seven months postinjury he was referred to us for pain, wrist stiffness and restriction of forearm supination (d); the patient was treated with radiolunate fusion, associated with matched distal-ulnar resection
We used a modification of this technique in cadavers using the brachioradialis tendon to recreate the stabilizing effect of the DRC, palmar LRL, and the palmar ulnocarpal ligaments, using the triquetrum instead of capitate as the anchored bone for the tendon graft (Fig. 8.37a–f). In the first version the tendon graft exiting from the volar triquetrum was inserted into a bony tunnel created at the radiovolar surface of the distal radius. In the second version and given that the proximal stump of the brachioradialis tendon graft is wide enough, we splitted the exited graft from the volar triquetrum in one radial and one ulnar component. The radial part, substituting the LRL ligament, was inserted into the above mentioned bony tunnel of the distal radius, while the ulnar part, substituting the volar UC ligaments, was inserted into a bony tunnel created at the ulnar fovea, where the UC ligaments are mainly attached.

A bony tunnel was created just proximal to the brachioradialis insertion exiting dorsally, where the DRC ligament is attached to the radius (a); the tendon graft was passed through the tunnel exiting ulnar to Lister’s tubercle (b); the tendon graft was inserted into a bone tunnel created at the triquetrum dorsally to volarly (c); the graft exiting from the volar surface of the triquetrum (d); in the first version, the tendon graft was inserted into a bony tunnel created where the LRL ligament attaches to the radius (e); in the second version the graft was splitted and its radial part was inserted as previously mentioned, while its ulnar part was inserted and fixed into a bone tunnel at the ulnar fovea (f)
By manually testing the stability of the RC joint, particularly the second version of the above-mentioned tenodesis proved to be effective, but further studies are needed (Fig. 8.38a, b).

The wrist was manually translated in ulnar direction after sectioning of the DRC, volar RC, and volar UC ligaments (a); the wrist stability seemed to be restored after rerouting the brachioradialis tendon (second version) (b)
References
Fernandez DL, Jupiter JB (2002) Fracture of the distal end of the radius: a historical perspective. In: Fernandez DL, Jupiter JB (eds) Fractures of the distal radius. A practical approach to management, Chap 1, 2nd edn. Springer, New York, pp 1–22
Ilyas A, Mudgal C (2008) Radiocarpal Fracture-dislocations. J Am Acad Orthop Surg 16:647–655
Destot E (1926) Injuries of the wrist: a radiological study. Hoeber, New York
Gui L (1957) Fratture e lussazioni. Edizioni scientifiche Instituto Ortopedico toscano, Firenze, p 510
Rosado AP (1966) A possible relationship of radiocarpal dislocation and dislocation of the lunate bone. J Bone Joint Surg Am 48:504–506
Dunn AW (1972) Fractures and dislocations of the carpus. Surg Clin North Am 52:1513–1518
Bilos ZJ, Pankovich AM, Yelda S (1977) Fracture-dislocation of the radiocarpal joint. J Bone Joint Surg Am 59:198–203
Dumontier C, Lenoble E, Saffar P (1995) Radiocarpal dislocations and fractures-dislocations. In: Saffar P, Cooney WP (eds) Fractures of the distal radius. Martin Dunitz, London, pp 267–278
Moneim MS, Bolger JT, Omer GE (1985) Radiocarpal dislocation–classification and rationale for management. Clin Orthop 192:199–209
Ilyas AM, Williamson C, Mudgal CS (2011) Radiocarpal dislocation: is it a rare injury? J Hand Surg [Eur] 36(2):164
Bellinghausen HW, Gilula LA, Young LV et al (1983) Post-traumatic palmar carpal subluxation. Report of two cases. J Bone Joint Surg Am 65:998–1006
Le Nen D, Riot O, Caro P et al (1991) Luxation-fractures of the radiocarpal joint. Clinical study of 6 cases and general review. Ann Chir Main Memb Super 10:5–12
Mourikis A, Rebello G, Villafuente J et al (2008) Radiocarpal dislocations: review of the literature with case presentations and a proposed treatment algorithm. Orthopedics 31:386
Naranja RJ, Bozentka DJ, Partington MT et al (1998) Radiocarpal dislocation: a report of two cases and a review of the literature. Am J Orthop 27(2):141–144
Schoenecker PL, Gilula LA, Shively RA et al (1985) Radiocarpal fracture-dislocation. Clin Orthop 197:237–244
Apergis E, Dimitrakopoulos K, Chorianopoulos K (1996) Late management of post-traumatic palmar carpal subluxation: A case report. J Bone Joint Surg Br 78:419–421
Arslan H, Tokmak M (2002) Isolated ulnar radiocarpal dislocation. Arch Orthop Trauma Surg 122:179–181
Ayekoloye CI, Shah N, Kumar A et al (2002) Irreducible dorsal radiocarpal fracture dislocation with dissociation of the distal radioulnar joint: a case report. Acta Orthop Belg 68(2):171–174
Dodd CA (1987) Triple dislocation in the upper limb. J Trauma 27:1307
Fehring TK, Milek MA (1984) Isolated volar dislocation of the radiocarpal joint. A case report. J Bone Joint Surg Am 66:464–466
Fennell CW, McMurtry RY, Fairbanks CJ (1992) Multidirectional radiocarpal dislocation without fracture: a case report. J Hand Surg [Am] 17:756–761
Fernandez DL (1981) Irreducible radiocarpal fracture-dislocation and radioulnar dissociation with entrapment of the ulnar nerve, artery and flexor profundus II-V-case report. J Hand Surg [Am] 6:456–461
Freeland A, Ferguson CA, McCraney WO (2006) Palmar radiocarpal dislocation resulting in ulnar radiocarpal translocation and multidirectional instability. Orthopedics 29(7):604–608
Freund LG, Ovesen J (1977) Isolated dorsal dislocation of the radiocarpal joint. J Bone Joint Surg Am 59:277
Hardy P, Welby F, Stromboni M et al (1999) Wrist arthroscopy and dislocation of the radiocarpal joint without fracture. Arthroscopy 15(7):779–783
Howard RF, Slawski DP, Gilula LA (1997) Isolated palmar radiocarpal dislocation and ulnar translocation: a case report and review of the literature. J Hand Surg [Am] 22(1):78–82
Jebson PJL, Adams BD, Meletiou SD (2000) Ulnar translocation instability of the carpus after a dorsal radiocarpal dislocation; a case report. Am J Orthop 29(6):462–464
Matthews MG (1987) Radiocarpal dislocation with associated avulsion of the radial styloid and fracture of the shaft of the ulna. Injury 18:70–71
Moore DP, McMahon BA (1988) Anterior radio-carpal dislocation: an isolated injury. J Hand Surg [Br] 13:215–217
Penny WH III, Green TL (1988) Volar radiocarpal dislocation with ulnar translocation. J Orthop Trauma 2:322–326
Reynolds ISR (1980) Dorsal carpal dislocation. Injury 12:48–49
Tanzer TL, Horne JG (1980) Dorsal radiocarpal fracture dislocation. J Trauma 20:999–1000
Thomsen S, Falstie-Jensen S (1989) Palmar dislocation of the radiocarpal joint. J Hand Surg [Am] 14:627–630
Varodompun N, Limpivest P, Prinyaroj P (1985) Isolated dorsal radiocarpal dislocation: case report and literature review. J Hand Surg [Am] 10:708–710
Nyquist SR, Stern PJ (1984) Open radiocarpal fracture-dislocations. J Hand Surg [Am] 9:707–710
Mudgal CS, Psenica J, Jupiter JB (1999) Radiocarpal fracture-dislocation. J Hand Surg [Br] 24:92–98
Girard J, Cassagnaud X, Maynou C et al (2004) Radiocarpal dislocation: Twelve cases and a review of the literature. Rev Chir Orthop 90:426–433
Dumontier C, Zu Reckendorf GM, Sautet A et al (2001) Radiocarpal dislocations: classification and proposal for treatment (a review of twenty-seven cases). J Bone Joint Surg Am 83:212–218
Taleisnik J (1985) The wrist. Churchill Livingstone, New York
Kapandji IA (1991) Etude du carpe au scanner a trois dimensions sous contraintes de pronosupination. Ann Chir Main 10:36–47
Ritt MJPF, Stuart PR, Berglund LJ et al (1995) Rotational stability of the carpus relative to the forearm. J Hand Surg [Am] 20(2):305–311
Roux JL (1992) La rotation longitudinale radio-metacarpienne. Thesis. Montpellier, France
Taleisnik J (1978) Wrist: anatomy, function, and injury. AAOS Instr Course Lect 27:61–68
Gupta A, Moosawi NA (2005) How much can carpus rotate axially? An in vivo study. Clin Biomech 20(2):172–176
Heras-Palou C (2009) Midcarpal instability. In: Slutsky DJ, Osterman AL (eds) Fractures and injuries of the distal radius and carpus. The Cutting edge. Saunders, Philadelphia, pp 417–423
Katz DA, Green JK, Werner FW et al (2003) Capsuloligamentous restraints to dorsal and palmar carpal translation. J Hand Surg [Am] 28(4):610–613
Berger RA, Landsmeer JM (1990) The palmar radiocarpal ligaments: a study of adult and fetal human wrist joints. J Hand Surg [Am] 15:847–854
Berger RA (1997) The ligaments of the wrist. Hand Clin 13(1):63–82
Garcia-Elias M (1997) Kinetic analysis of carpal stability during grip. Hand Clin 13:151–158
Viegas SF, Patterson RM, Ward K (1995) Extrinsic wrist ligaments in the pathomechanics of ulnar translation instability. J Hand Surg [Am] 20:312–318
Werner FW, Sutton LG, Allison MA et al (2010) Scaphoid and lunate translation in the intact wrist and following ligament resection: a cadaver study. J Hand Surg [Am] 36(2):291–298
Rayhack JM, Linscheid RL, Dobyns JH et al (1987) Posttraumatic ulnar translation of the carpus. J Hand Surg [Am] 12:180–189
Munk B, Jensen SL, Olsen BS et al (2005) Wrist stability after experimental traumatic triangular fibrocartilage complex lesions. J Hand Surg [Am] 30(1):43–49
Wiesner L, Rumelhart C, Pham E et al (1996) Experimentally induced ulno-carpal instability. A study on 13 cadaver wrists. J Hand Surg [Br] 21(1):24–29
Allieu Y, Garcia-Elias M (2000) Dynamic radial translation instability of the carpus. J Hand Surg [Br] 25(1):33–37
Yin Y, Mann FA, Hodge JC et al (1996) Roentgenographic interpretation of ligamentous instabilities of the wrist. In: Gilula LA, Yin Y (eds) Imaging of the wrist and hand. WB Saunders, Philadelphia, pp 203–224
Moritomo H, Murase T, Arimitsu S et al (2008) Change in the length of the ulnocarpal ligaments during radiocarpal motion: possible impact on triangular fibrocartilage complex foveal tears. J Hand Surg [Am] 33(8):1278–1286
Iwamoto A, Morris RP, Andersen C et al (2006) An anatomic and biomechanic study of the wrist extensor retinaculum septa and tendon compartments. J Hand Surg [Am] 31(6):896–903
Hagert E, Persson JKE, Werner M et al (2009) Evidence of wrist proprioceptive reflexes elicited after stimulation of the scapholunate interosseous ligament. J Hand Surg [Am] 34:642–651
An KN, Horii E, Ryu J (1991) Muscle function. In: An KN, Berger EJ, Cooney WP (eds) Biomechanics of the wrist joint. Springer, New York, pp 157–169
Brand PW (1981) Relative tension and potential excursion of muscles in forearm and hand. J Hand Surg [Am] 6:209–219
Hagert E, Forsgren S, Ljung BO (2005) Differences in the presence of mechanoreceptors and nerve structures between wrist ligaments may imply differential roles in wrist stabilization. J Orthop Res 23:757–763
Salva-Coll G, Garcia-Elias M, Leon-Lopez MT (2011) Effects of forearm muscles on carpal stability. J Hand Surg [Eur] 36(7):553–559
Berger RA, Amadio PC (1994) Predicting palmar radio-carpal ligament disruption in fractures of the distal articular surface of the radius involving the palmar cortex. J Hand Surg [Br] 19:108–113
Siegel DB, Gelberman RH (1991) Radial styloidectomy: an anatomical study with special reference to radiocarpal intracapsular ligamentous morphology. J Hand Surg [Am] 16:40–44
Mandziak DG, Watts AC, Bain GI (2011) Ligament contribution to patterns of articular fractures of the distal radius. J Hand Surg [Am] 36(10):1621–1625
Giunta R, Lower N, Kierse R et al (1997) Stress on the radiocarpal joint. CT studies of subchondral bone density in vivo. Handchir Mikrochir Plast Chir 29:32–37
Fernandez DL, Jupiter JB, Ghillani R (2002) Radiocarpal fracture-dislocation. In: Fernandez DL, Jupiter JB (eds) Fractures of the distal radius. A practical approach to management, Chap 8, 2nd edn. Springer, New York, pp 253–264
Ilyas A, Mudgal C, Jupiter J (2009) Volar rim and Barton’s fracture. In: Slutsky DJ, Osterman AL (eds) Fractures and injuries to the distal radius and carpus, Chap 14. Saunders Elsevier, pp 157–163
Bohler L (1930) Verrenkungen der Handgelenke. Acta Chir Scand 67:154–177
Weiss C, Laskin RS, Spinner M (1970) Irreducible radiocarpal dislocation. J Bone Joint Surg Am 52:562–564
Bohler L (1956) The treatment of fractures. Grune & Stratton, New York, pp 826–854
Graham TJ (2003) The inferior arc injury: an addition to the family of complex carpal fracture-dislocation patterns. Am J Orthop 32(9):10–19
Sivan M, Davies N, Archibald C et al (2005) An unusual combination of radiocarpal fracture dislocation, scaphoid fracture and posteromedial elbow dislocation. Injury Extra 36:312–315
Watanabe K, Nishikimi J (2001) Transstyloid radiocarpal dislocation. Hand Surg 6(1):113–120
Oberladstätter J, Arora R, Dallapozza C et al (2010) Radiological radio-carpal and mid-carpal motion after operative treatment of dorsal radio-carpal fracture dislocations. Arch Orthop Trauma Surg 130:77–81
Jupiter JB, Fernandez DL, Toh CL et al (1996) Operative treatment of volar intra-articular fractures of the distal end of the radius. J Bone Joint Surg Am 78(12):1817–1828
Helm RH, Tonkin MA (1992) The chauffeur’s fracture. Simple or complex? J Hand Surg [Br] 17(2):156–159
Apergis E, Darmanis S, Theodoratos G et al (2002) Beware of the ulno-palmar distal radial fragment. J Hand Surg [Br] 27:139–145
Harness NG, Jupiter JB, Orbay JL et al (2004) Loss of fixation of the volar lunate facet fragment in fractures of the distal part of the radius. J Bone Joint Surg Am 86(9):1900–1908
Cohen MS, McMurtry RY, Jupiter JB (1998) Fractures of the distal radius. In: Browner BD, Jupiter JB, Levine AM, Trafton PG (eds) Skeletal Trauma, 2nd edn. WB Saunders, Philadelphia, p 1385
Fernandez DL, Jupiter JB (2002) Articular marginal shearing fractures. In: Fernandez DL, Jupiter JB (eds) Fractures of the distal radius. A practical approach to management, Chap 6, 2nd edn. Springer, New York, pp 188–212
King RE (1959) Barton’s enigma. J Bone Joint Surg Am 41:753–769
Lozano-Calderón SA, Doornberg J, Ring D (2006) Fractures of the dorsal articular margin of the distal part of the radius with dorsal radiocarpal subluxation. J Bone Joint Surg Am 88(7):1486–1493
Stoffelen D, Fortems Y, De Smet L et al (1996) Dislocation of the distal radioulnar joint associated with a transstyloid radiocarpal fracture dislocation a case report and review of the literature. Acta Orthop Belg 62(2):52–55
Idler RS (2001) Carpal dislocations and instability. In: Watson HK, Weinzweig J (eds) The Wrist, vol 1. Lippincott Williams & Wilkins, pp 203–229
Capo JT, Armbruster ED, Hashem J (2010) Proximal carpal row dislocation: a case report. Hand 5:444–448
Klein A, Bohrer SP, Martin W III (1986) Dorsal dislocation of the radiocarpal joint with associated dorsal perilunar dislocation. Can Assoc Radiol J 37(3):201–202
Maschke S, Means KR, Parks BG et al (2010) A radiocarpal ligament reconstruction using brachioradialis for secondary ulnar translation of the carpus following radiocarpal dislocation: a cadaver study. J Hand Surg [Am] 35(2):256–261
Kamal RN, Bariteau JT, Beutel BG et al (2011) Arthroscopic reduction and percutaneous pinning of a radiocarpal dislocation. A case report. J Bone Joint Surg [Am] 93(15):1–5
Campbell DA (2009) Ulnar head and styloid fractures. In: Slutsky DJ, Osterman AL (eds) Fractures and injuries to the distal radius and carpus. The cutting edge, Chap 28. Saunders, Philadeiphia, pp 297–308
Nakamura T, Moy OJ, Peimer CA (2003) Relationship between the ulnar styloid fracture and DRUJ instability. J Hand Surg [Br] 28(1):48
Gabl M, Lener M, Pechlaner S (1993) Destabilization of the discus articularis with rupture of the ulnar styloid apex in distal radius fracture. Diagnosis with dynamic MR. Unfallchirurgie 19:108
Lindau T, Adlercreutz C, Aspenberg P (2000) Peripheral tears of the triangular fibrocartilage complex cause distal radioulnar joint instability after distal radial fractures. J Hand Surg [Am] 25(3):464–468
Souer JS, Ring D, Matschke S et al (2009) Effect of an unrepaired fracture of the ulnar styloid base on outcome after plate-and-screw fixation of a distal radial fracture. J Bone Joint Surg Am 91(4):830–838
May MM, Lawton JN, Blazar PE (2002) Ulnar styloid fractures associated with distal radius fractures: incidence and implications for distal radioulnar joint instability. J Hand Surg [Am] 27(6):965–971
Atzei A, Luchetti R (2011) Foveal TFCC tear classification and treatment. Hand Clin 27(3):263–272
Bozentka DJ, Beredjiklian PK (2001) Classification of radiocarpal dislocations and appropriate treatment. J Bone Joint Surg Am 83(10):1587–1588
Hofmeister EP, Fitzgerald BT, Thomson MA et al (2008) Surgical reconstruction of a late-presenting volar radiocarpal dislocation: a case report. Am J Orthop 37(2):96–99
Takase K, Yamamoto K, Yoshino S et al (2004) Palmar dislocation of the radio-carpal joint: a case report. J Orthop Surg 12(2):258–262
Gilula LA (1979) Carpal injuries: analytic approach and case exercises. Am J Roentgenol 133:503–517
Lipton HA, Jupiter J (2001) Open reduction and internal fixation of distal radius fractures. In: Watson HK, Weinzweig J (eds) The wrist. Lippincott Williams & Wilkins, pp 333–335
Antuna SA, Mendez JG, Paz Jimenez J (1994) Displaced radiocarpal dislocation with multiple associated fractures. Acta Orthop Belg 60:430–431
Lourie JA (1982) An unusual dislocation of the lunate and the wrist. J Trauma 22:966–967
Berger RA, Weiss AP (2004) Hand Surgery. Lippincott Williams & Wilkins
Cooney WP, Linscheid RL, Dobyns JH (1998) The Wrist. Diagnosis and operative treatment. Mosby, St. Louis
Watson HK, Weinzeig J (2001) The Wrist. Lippincott Williams & Wilkins
Chin KR, Jupiter JB (1999) Wire-loop fixation of volar displaced osteochondral fractures of the distal radius. J Hand Surg [Am] 24:525–533
Obafemi A, Pensy R (2012) Palmar radiocarpal dislocation: a case report and novel treatment method. Hand 7:114–118
Schweitzer G (1987) Radiocarpal fracture-dislocation [letter]. Clin Orthop 216:298–299
Patee G, Thomson G (1988) Anterior and posterior marginal fracture-dislocations of the distal radius. An analysis of the results of treatment. Clin Orthop 231:183–195
Knirk JL, Jupiter JB (1986) Intra-articular fractures of the distal end of the radius in young adults. J Bone Joint Surg Am 68(5):647–659
Dobyns JH, Linscheid RL, Chao EYS et al (1975) Traumatic instability of the wrist. In: AAOS instructional course lectures, vol 24. CV Mosby, St Louis, pp 182–199
Berschback JC, Kalainov DM, Husain SN et al (2012) Traumatic ulnar translocation of the carpus: early recognition and treatment. J Hand Surg [Eur] 37(8):755–764
Mulier T, Reynders P, Broos P et al (1992) Posttraumatic ulnar translation of the carpus. Acta Orthop Scand 63(1):102–103
Schernberg F (1996) Ulnar translation of the carpus: a rare type of wrist instability. In: Buchler U (ed) Wrist instability, Chap 23. Martin Dunitz, Philadelphia, pp 175–179
Garcia-Elias M (1999) Carpal instabilities and dislocations. In: Green DP, Hotchkiss RN, Pederson WC (eds) Green’s operative hand surgery,Chap 28, vol 1. Churchill Livingstone, New York, pp 865–928
Rettig AC, Rettig LA, Jelinek JA (2010) Ulnar translocation of the wrist in a professional quarterback: a case report. Am J Sports Med 38(3):608–612
Rutgers M, Jupiter J, Ring D (2009) Isolated posttraumatic ulnar translocation of the radiocarpal joint. J Hand Microsurg 1(2):108–112
Stabler A, Baumeister RGH, Szeimies U et al (1994) Rotatory palmar subluxation of the lunate in post-traumatic ulnar carpal translocation. Skeletal Radiol 23:103–106
Chamay A, Della Santa D, Vilaseca A (1983) Radiolunate arthrodesis. Factor of stability for the rheumatoid wrist. Ann Chir Main 2:5–17
DiBenedetto MR, Lubbers LM, Coleman CR (1990) A standardized measurement of ulnar carpal translocation. J Hand Surg [Am] 15:1009–1010
McMurtry RY, Youm Y, Flatt AE et al (1978) Kinematics of the wrist. II. Clinical applications. J Bone Joint Surg Am 60:955–961
Bouman HW, Messer E, Sennwald G (1994) Measurement of ulnar translation and carpal height. J Hand Surg [Br] 19:325–329
Gilula LA, Weeks PM (1978) Post-traumatic ligamentous instabilities of the wrist. Radiology 129:641–651
Schuind FA, Linscheid RL, An KN et al (1992) A normal data base of posteroanterior roentgenographic measurements of the wrist. J Bone Joint Surg Am 74:1418–1429
Apergis E (2004) καταγματα-εξαρθρήματα του καρπου. Konstantaras Medical Books, Athens
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
Copyright information
© 2013 Springer-Verlag Italia
About this chapter
Cite this chapter
Apergis, E., Palamidi, A. (2013). Radiocarpal Dislocations or Fracture-Dislocations. In: Fracture-Dislocations of the Wrist. Springer, Milano. https://doi.org/10.1007/978-88-470-5328-1_8
Download citation
DOI: https://doi.org/10.1007/978-88-470-5328-1_8
Published:
Publisher Name: Springer, Milano
Print ISBN: 978-88-470-5327-4
Online ISBN: 978-88-470-5328-1
eBook Packages: MedicineMedicine (R0)