
Abstract
Purpose
Radiocarpal dislocation fractures (RCDF) are rare injuries that usually occur in a violent trauma setting. Our work aimed to analyze our patients’ functional and radiological results after surgery and identify potential medium- and long-term complications while reviewing other series previously reported in the literature.
Methods
We have performed a retrospective study over five years at our university hospital, eleven patients were selected, and the mean follow-up was about 33 months. We used Dumontier’s and Moneim’s classifications for classifying the injuries. All the patients underwent surgery followed by cast immobilization. The QuickDash score and Green O’Brien score modified by Cooney were used to assess the functional result, while the radiological result was judged on standard wrist radiographs.
Results
Out of the eleven patients, only one described a Dumontier type I radiocarpal dislocation; all the others were type II. Following the Moneim classification, two patients were type II. Most cases showed posterior displacement. In 80% of cases, the radiocarpal fracture-dislocation was combined with other bone or ligament injuries. All patients received surgical treatment followed by cast immobilization for 45 days.
The mean loss of range of motion at the last follow-up was about 39%, keeping the arch intact in most cases. Quick dash score was 29.54, and Green O’Brien’s score was 71.1. Three of the patients showed osteoarthritic remodeling.
Conclusion
A careful clinical and radiological evaluation, followed by an anatomic surgical reduction of the articulating surface of the distal radius, as well as the handling of the associated lesions, are major conditions for a satisfactory clinical result.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Radiocarpal dislocations fractures (RCDF) are rare and represent 0.2% of traumatic wrist injuries [1]. They generally result from severe trauma. From an anatomical point of view, it consists of a loss of contact between the radial glenoid and the proximal row of the carpus [2]. The displacement in RCDF is usually dorsal, commonly associated with a radial or ulnar styloid fracture, and exceptionally pure [3]. The most widely used classification is the one proposed by Dumontier et al. in 2001 [4]. The treatment is often surgical, consisting of reduction and osteosynthesis of the fractures. A radiocarpal pinning may be necessary in some cases in combination with a plaster cast or an external fixator immobilization [5,6,7].
The purpose of our paper is to review the functional outcome obtained according to the initial injury assessment and the proposed treatment while revising the other series of literature, in which the number of cases is often limited, to improve the comprehensive management of this uncommon entity of fracture-dislocation.
Patients and methods
We conducted a retrospective study in our hospital from March 2016 to February 2021; during this period, we admitted eleven patients with RCDF. The exclusion criteria were age under 16 years, the absence of an initial radiograph documenting the dislocation, and displaced marginal fracture of Lenteur and barton [8]. For the epidemiological data, age; sex; and affected side were reported. The radiological evaluation systematically included radiographs of the wrist and hand in anteroposterior and side xray projections , with the use of CT scans in five cases. After analysis of all bone and ligament injuries, we categorized the patients according to the classifications of Dumontier [4] and Moneim [9]. All our patients were treated surgically, under locoregional or general anesthesia, and using fluoroscopic guidance. The QuickDASH [10] and the Green and O’Brien scoring modified by Cooney [11] (Table 1) were both used to assess the functional outcome. Given the unavailability of the Jamar dynamometer, we compared the grip strength of both hands to evaluate the strength loss. Standard radiographs were used to evaluate the bone healing; the ulnar translation of the carpus measured by the CUDR, Carpal Ulnar Distance Ratio (ratio of the distance between the centre of the capitate head and the axis of the ulna to the length of the third metacarpal, the normal value being 0.30 ± 0.03. A decrease in this ratio corresponds to an ulnar translation of the carpus); and the presence of radiocarpal, intracarpal, and distal radioulnar osteoarthritis.
Result
The average follow-up at the time of the study was 33 months (9–71months); most of the patients were males: nine males to two females, the mean age was 34.4 years (21–54), all were right-handed, the nondominant left side was affected only in two cases. The injury was due to high energy impact: eight times it was caused by a traffic accident, in two situations by falling from a height, while only one case was due to a sports accident. On admission, all patients suffered from pain and functional disability. Two patients had paresthaesia of the median nerve (Case No 3,7), and none showed a cutaneous opening.
All the patients had undergone standard radiography, and five had undergone additional imaging by computed tomography (CT). Based on Dumontier’s classification [4], ten of our patients belonged to type II, and only one to type I, which presented a minor detachment of the tip of the radial styloid that did not exceed 1/3 of the radial glenoid (Fig. 1A). For Moniem’s classification (Fig. 1B) [9], nine patients were in group I and two in group II. The clinical and radiological data and the following treatment are reported in (Table 2).

A Dumentier’s classification ( type I: detachment of the tip of radial styloid, type II styloid fragment exceeding 1/3 of radial articular aspect). B Moneim’s classification ( Group I without carpal involvement, Group II with carpal bone involvement)
All patients were treated surgically by different operators. After reduction by external manoeuvres under fluoroscopic control, eight patients were treated by percutaneous pinning of the radial styloid (Fig. 2); this procedure was associated with the pinning of the ulnar styloid in case (No 11) due to the considerable size of the detached fragment. Three patients underwent open reduction. In (case No 2), a dorsal approach of the wrist was used for the removal of the intra-articular osteocartilaginous fragment blocking the reduction, followed by pinning of the radial styloid. The patient (case No 4) underwent open reduction of his radiocarpal dislocation and the associated distal ulnar dislocation (DRU) via the same approach (Fig. 3). The patient (No 8), the unique Dumontier’s type I RCD, underwent an anterior surgical approach after failed reduction by external maneuver; the radio-scapho-capitate ligament complex was repaired with sutures, with the stabilization of associated lunotriquetral dislocation by pinning. Nine patients had a plaster cast immobilization, and two had an anterior splint. The average duration of immobilization was six weeks.

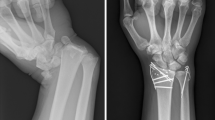
Front and side wrist radiographs of case N°1 showing radial and ulnar styloid fracture with posterior radiocarpal dislocation, followed by radiographs after reduction of the dislocation and percutaneous pinning of the radial styloid

Case N 1 wirst radiography at the 36th month of the trauma showing the absence of radiocarpal degenerations and the absence of ulnar translation, followed by a clinical image showing the recovery of the articular rang of motion corresponding to a good functional result
The QuickDash score [10] was 29.54 on average, and the mean Green O’Brien modified by Cooney [11] was at 71.1: the overall results were satisfactory (Fig. 4), with three good to excellent outcomes, six intermediate and two poor (Table 3). All patients were able to return to work.

Radiographs of the wrist in front and in profile of case N°4 showing the fracture of the radial styloid with posterior radiocarpal dislocation and dislocation of the radioulnar joint, followed by an image showing the posterior approach of the wrist with the rupture of the capsulo-ligamentary tissue, and finally the radiographs after the reduction of the dislocation and the pinning
At the last follow-up, the radiological assessment revealed radiocarpal osteoarthritis in three patients. In one case, it was an aggravation of pre-existing osteoarthritis on scaphoid malunion (case No 11). The second case (No 8) was our unique Dumontier type I LRC. The third was the patient (No 4) who showed distal radio-ulnar and intra-carpal osteoarthritis (Fig. 5). No ulnar translation was noted.

X-ray of the wrist and corn of case N°4 at the 18th month of the trauma showing the presence of radiocarpal and intracarpal osteoarthritis, followed by clinical image showing major limitation of articular rang of motion corresponding to a poor functional outcome
During the follow-up of our patients, one case of denervation of the wrist was performed on a housewife (patient No 8) who presented symptomatic radiocarpal osteoarthritis; and in one other case, arthrodesis of the wrist was proposed (case No 4) given that the patient carried out a manual job involving considerable force. All the clinical and radiological results have been reported in Table 3.
Discussion
Radio-carpal fractures are rare [1]; their annual incidence for us was 2.2 for a hospital facility that covers more than 2 million people. They concern young and active people, and the average age was 34 years, comparable to other series, 31 years in Dahmani’s series [12], 38 years for Spiry [7], and 42 years for Cornu [9]. They often result from a high-energy trauma: traffic accident or fall from a height [4,5,6,7, 12, 13].
The clinical examination constantly reveals wrist deformity and must look for a skin opening, which we have not found in our patients, but described by several authors [12, 14,15,16]. The neurovascular examination may reveal the involvement of the median nerve, which was the case for 18% of our patients; this incidence remains variable depending on the series [6, 14, 17, 18], and the injury is probably due to stretching of the nerve on the deformed skeleton of the wrist; this injury is often regressive. Associated tendinous damage is unusual; Le Nen et al. [18] have described an avulsion of the ulnar extensor of the carpus and a rupture of the extensor digiti quinti proprius in their series.
Standard radiographs allow the diagnosis, but it is also essential to differentiate between the radial styloid fracture with a horizontal line that occurs with radiocarpal dislocation; and the partial sagittal fractures of the distal radius [6], as well as the displaced marginal fractures of Barton and Leteneur [4, 8, 19].
RCFD with posterior displacement is the most frequent form [4, 6, 7, 12,13,14] and was about 90% in our series. The simple form of RCD is exceptional [3, 4, 6, 7, 12,13,14]. Besides the nearly constant radial styloid fracture, 81% of the patients showed other associated bone lesions, especially a posterior marginal fracture in 63.6%, a rate of association similar to other series in the literature [12, 13, 18], and the ulnar styloid fracture in 36.6%. The association of intracarpal lesions is inconstant; the incidence varies from one series to another: Girard [6] and Le Nen [18] did not report any patients, Cornu [13] did not specify in his series, Dahmani [12] reported 11%, Spiry [7] in his series of 41 patients reported 22%; we note 18% in our series. Distal radio-ulnar dislocation is a rare association; we only found one case, Cornu [13] reported two, and Girard [6] reported one case that went unnoticed initially.
RCFD has been classified based on two classifications, the most widely used is that of Dumontier [4] and Moneim’s [9], which completes the Dumontier classification ignoring intracarpal injuries. However, none of the registered classifications take into consideration the involvement of the distal radioulnar joint, despite a very high prognostic impact of this injury.
Forty-five percent (45%) of our patients had further imaging using computed tomography (CT). In our opinion, it is a simple and available examination that allows a better understanding of the bone damage, evaluates the comminution of the marginal fractures, and identifies disorganization of the Gelula’s lines in the carpus; or a distal radio-ulnar incongruence, as well as detecting a minor bone detachment, permitting better planning of the treatment. However, it should not lead to a delay in the treatment. Some authors recommend a preoperative arthro-scanner [20]; or emergency MRI [21] to search for intracarpal lesions, although the gold standard is still dynamic fluoroscopic imaging.
Regarding therapeutic management, opinions vary widely across the literature, with different interpretations of the results by each author, leading to sometimes controversial conclusions. Many authors have reported good results of orthopaedic treatment alone, which consists of a non-surgical conservative treatment by a closed reduction of the dislocation by external maneuver followed by a plaster cast immobilization and pain management [9, 22,23,24,25], but none of those cases were associated with intracarpal lesions. Orthopaedic management holds a limited place when it allows an anatomical reduction, but there is a significant risk of secondary displacement; indeed, Gerard [26] described five secondary displacements out of six orthopaedic reductions.
For some authors, surgery is reserved for reduction failures and/or the presence of intracarpal lesions [27, 28], whereas others advocate surgical treatment for all RCFDs [15, 17, 26, 29], recommending orthopaedic reduction with osteosynthesis of the radial styloid, and a contention of either plaster cast or an external fixator.
Dumontier’s classification [4] is of interest coming to surgical management. For type II RCDF, Dumontier suggests a reduction by dorsal approach and fixation by pinning or screwing associated with immobilization by an external fixator or plaster. For several authors [6, 7, 12, 13], an incision seems unnecessary if satisfactory reduction of the radial styloid is obtained by external maneuvers, allowing percutaneous osteosynthesis, which was the case for eight of our patients. Moneim [9] completed Dumontier’s classification by bringing attention to the intracarpal lesions neglected by the latter; untreated lunotriquetral injuries and scapholunate disjunctions evolved into radiocarpal osteoarthritis, with a poor functional outcome; whereas intracarpal lesions stabilized by open pinning using a combination of both anterior and posterior approaches had a better outcome. In our series (case No 11) was classified as Moneim type II due to his neglected scaphoid malunion, and he was treated without associated procedure in the carpus, at the last follow-up (9 months), he showed signs of radiocarpal osteoarthritis, but his wrist remains asymptomatic except for the limitation ROM comparable to the rest of the patients.
Dumontier’s type I RCD suggests a disruption of the anterior radiocarpal capsuloligamentous complex, leading to a disorganization of the carpus and pathological ulnar translation in the absence of repairing. Dumontier proposes a volar approach for this type, with a suture of the radiolunate and/or radioscapho-capitat ligaments; and a radiolunate pinning or an external fixation to protect the ligamentous suture.
For Spiry [7], a dorsal approach for the removal of intra-articular osteocartilaginous fragments, and a capsuloligamentary repair, along with a radioscaphoid and radiolunate pinning kept for two months, seems to be sufficient, While Cornu [13] has not performed any capsuloligamentary repair on any of the patients of his series, including the three cases of type I, and has reported satisfactory outcomes, leaving the question of capsuloligamentary repair in type I a subject of controversy regarding the necessity of repair as well as the choice of the approach.
In addition, this reparation only allows the control of ulnar translation without any effect on the development of radiocarpal osteoarthritis [6]. The type I RCD in our series (case No 8) benefited from an open palmar capsuloligamentary repair with lunotriquetral pinning for associated injuries, without radiolunat pinning. After nine months of follow-up, neither ulnar translation nor residual instability was registered; however, symptomatic radiocarpal osteoarthritis was noted, for which the patient benefited from a procedure of wrist denervation. Based on our results, we cannot comment on the necessity or otherwise of ligament repair, given the rarity of type I in our series and the literature in general.
Distal radioulnar dislocations should be carefully sought and stabilized by pinning. If left untreated, these lesions progress to distal radioulnar osteoarthritis, which is associated with a poor outcome [6, 7, 12, 13]. In our series, the case (No 4) was similar to the patient reported by Jardin [30], who presented with RCFD type II with distal radio-ulnar dislocation, despite the proper initial management, the evolution was towards radiocarpal and radio-ulnar osteoarthritis and a poor clinical outcome; so radiocarpal arthrodesis with Suave-Kapandji procedure was proposed for the patient.
In terms of clinical outcome, we noted an average loss of joint range of motion of about 39%, with preservation of the functional arch for the majority of patients without osteoarthritic remodeling, the average QuickDASH score was 29.54 and the Green O’Brien scoring modified by Cooney of 71.1, comparable to other literature series (Table 4).
Regarding the radiological evolution, three cases (27.2%) of radiocarpal osteoarthritis were found (cases No: 4, 8, 11). This rate of radiocarpal arthrosis varies in the literature from 11 to 83%; Dahmani reports 22.2%, Girard 25% [6], Yuan et al. found 31% [5], Conru 42.8%, Le Nen et al. [18] presented 83%. This variation can be explained by the variable rates of the associated lesions, particularly the intracarpal ones, and the therapeutic attitude adopted differently in each series.
A radiocarpal arthrodesis was necessary for a second time for six patients in Spiry’s series (14.63%), one of those following pseudarthrosis of the scaphoid and five following ulnar translation. Of the six cases, three also showed comminuted marginal fractures. For Le Nen [18], one patient needed a Suave kapandji for distal radio-ulnar osteoarthritis on neglected dislocation.
After analyzing both our findings and those of the literature, it appears that the prognosis of RCDF is related to the existence or not of involvement of the distal radioulnar joint, intra-carpal lesions, and initial skin or nerve involvement [9, 15, 28]. Radiocarpal osteoarthritis may be secondary to a malreduction of the radial styloid, to imperfect healing of the radiocarpal caspulo-ligamentous tissue resulting in ulnar translation, and to osteo-chordal injury during the initial trauma.
Conclusion
Radiocarpal fracture dislocation are rare and not easy to manage. The initial radiological analysis is a fundamental part of the management; the involvement of the distal radio-ulnar joint and intra-carpal lesions left unnoticed and untreated undoubtedly leads to poor outcomes. The available classifications are helpful but seem to be incomplete in terms of description of associated lesions with a prognostic importance such as distal radio-ulnar involvement and marginal fractures. For type II, the management is pretty much the same for all of the authors, it consists of an anatomical reduction of the radial styloid with stabilization of the intracarpal and distal radioulnar lesions if present, for type I, there is no consensus on the necessity of repairing the radiocarpal capsuloligamentous complex nor on the approach in case of its repair, which is likely due to the scarcity of this variant of RCD.
References
Dunn AW (1972) Fractures and dislocations of the carpus. Surg Clin North Am 52(6):1513–1538. https://doi.org/10.1016/s0039-6109(16)39895-4
Weiss C, Laskin RS, Spinner M (1970) Irreducible radiocarpal dislocation. A case report. J Bone Joint Surg . Am 52(3):562–564
Loubignac F, Colomb F, Thiry A, Nasr Z, Lovet J (1999) La luxation radio-carpienne pure. A propos d'un cas et revue générale de la littérature [Isolated radiocarpal luxation. A case report and general review of the literature]. Revue De Chirurgie Orthopedique Et Reparatrice De L'appareil Moteur 85(4):393–396
Dumontier C, Zu Reckendorf GM, Sautet A, Lenoble E, Saffar P, Allieu Y (2001) Radiocarpal dislocations: classification and proposal for treatment. A review of twenty-seven cases. J Bone Joint Surg Am 83(2):212–218. https://doi.org/10.2106/00004623-200102000-00008
Yuan BJ, Dennison DG, Elhassan BT and Kakar S (2015) Outcomes after radiocarpal dislocation: a retrospective review. Hand (New York, N.Y.) 10(3):367–373. https://doi.org/10.1007/s11552-014-9736-5
Girard J, Cassagnaud X, Maynou C, Bachour F, Prodhomme G, Mestdagh H (2004) Luxation radio-carpienne: à propos d'une série de 12 cas et revue de la littérature [Radiocarpal dislocation: twelve cases and a review of the literature]. Revue de chirurgie orthopedique et reparatrice de l'appareil moteur 90(5):426–433. https://doi.org/10.1016/s0035-1040(04)70169-5
Spiry C, Bacle G, Marteau E, Charruau B, Laulan J (2018) Radiocarpal dislocations and fracture-dislocations: injury types and long-term outcomes. Ortho Traumatol , Surg Res OTSR 104(2):261–266. https://doi.org/10.1016/j.otsr.2017.12.016
Harness N, Ring D, Jupiter JB (2004) Volar Barton’s fractures with concomitant dorsal fracture in older patients. J Hand Surg 29(3):439–445. https://doi.org/10.1016/j.jhsa.2003.12.009
Moneim MS, Bolger JT, Omer GE (1985) Radiocarpal dislocation--classification and rationale for management. Clin Ortho Related Res 192:199–209
Hudak PL, Amadio PC, Bombardier C (1996) Development of an upper extremity outcome measure: the DASH (disabilities of the arm, shoulder and hand) [corrected]. The Upper Extremity Collaborative Group (UECG). Am J Indust Med 29(6):602–608. https://doi.org/10.1002/(SICI)1097-0274(199606)29:6<602::AID-AJIM4>3.0.CO;2-L
Cooney WP, Bussey R, Dobyns JH, Linscheid RL (1987) Difficult wrist fractures. Perilunate fracture-dislocations of the wrist. Clin Ortho Related Res 214:136–147
Dahmani O, Elbachiri M, Shimi M, Elibrahimi A, Elmrini A (2013) Radiocarpal dislocation (about nine cases). Chir Main 32:30. https://doi.org/10.1016/j.main.2012.12.005
Cornu A, Sturbois-Nachef N, Baudoux M, Amouyel T, Saab M, Chantelot C (2019) Luxation radio-carpienne : étude rétrospective de 14 patients. Revue de Chirurgie Ortho Traumatol 105:1048–1054
Ilyas AM, Mudgal CS (2008) Radiocarpal fracture-dislocations. J Am Acad Ortho Surg 16(11):647–655. https://doi.org/10.5435/00124635-200811000-00005
Nyquist SR, Stern PJ (1984) Open radiocarpal fracture-dislocations. J Hand Surg 9(5):707–710. https://doi.org/10.1016/s0363-5023(84)80018-0
Fernandez DL, Jupiter JB (1996) Radiocarpal fracture-dislocation. In: Fractures of the Distal Radius. Springer, New York, NY, pp 221–234. https://doi.org/10.1007/978-1-4684-0478-4_8
Bilos ZJ, Pankovich AM, Yelda S (1977) Fracture-dislocation of the radiocarpal joint. J Bone Joint Surg Am 59(2):198–203
Le Nen D, Riot O, Caro P, Le Fevre C and Courtois B (1991) Luxation-fractures de la radio-carpienne. Etude clinique de six cas et revue générale [Luxation-fractures of the radiocarpal joint. Clinical study of 6 cases and general review]. Annales de chirurgie de la main et du membre superieur : organe officiel des societes de chirurgie de la main = Annals of hand and upper limb surgery 10(1):5–12
Pattee GA, Thompson GH (1988) Anterior and posterior marginal fracture-dislocations of the distal radius. An analysis of the results of treatment. Clin Ortho Related Res 231:183–195
Bellinghausen HW, Gilula LA, Young LV, Weeks PM (1983) Post-traumatic palmar carpal subluxation. Report of two cases. J Bone Joint Surg Am 65(7):998–1006
Howard RF, Slawski DP, Gilula LA (1997) Isolated palmar radiocarpal dislocation and ulnar translocation: a case report and review of the literature. J Hand Surg 22(1):78–82. https://doi.org/10.1016/S0363-5023(05)80183-2
Fahey JH (1957) Fractures and dislocations about the wrist. Surg Clin North Am 37(1):19–40. https://doi.org/10.1016/s0039-6109(16)35081-2
Freund LG, Ovesen J (1977) Isolated dorsal dislocation of the radiocarpal joint. A case report. J Bone Joint Surg Am 59(2):277
Reynolds IS (1980) Dorsal radiocarpal dislocation. Injury 12(1):48–49. https://doi.org/10.1016/0020-1383(80)90076-5
Tanzer TL, Horne JG (1980) Dorsal radiocarpal fracture dislocation. J Trauma 20(11):999–1000. https://doi.org/10.1097/00005373-198011000-00020
Gerard Y, Schernberg F, Elzein F (1981) Les luxations-fractures postérieures de la radio-carpienne. Rev Chir Orthop 6(suppl. II):92–96
Antuña SA, Mendez JG, Paz Jimenez J (1994) Displaced radiocarpal dislocation with multiple associated fractures. Acta Ortho Belgica 60(4):430–431
Lahtaoui A, el Bardouni A, Ismael F, Jellali T, Bahri A, el Yaacoubi M, el Manouar M (2002) Les luxations-fractures radiocarpiennes postérieures (à propos de huit cas) [Posterior radiocarpal fracture-dislocation (eight case reports)]. Chirurgie de la main 21(4):252–257. https://doi.org/10.1016/s1297-3203(02)00120-8
Schoenecker PL, Gilula LA, Shively RA, Manske PR (1985) Radiocarpal fracture--dislocation. Clin Ortho Related Res 197:237–244
Jardin E, Pechin C, Rey PB, Gasse N, Obert L (2016) Open volar radiocarpal dislocation with extensive dorsal ligament and extensor tendon damage: a case report and review of literature. Hand Surg Rehab 35(2):127–134. https://doi.org/10.1016/j.hansur.2016.02.003
Acknowledgement
We thank our colleagues who provided insight and expertise that greatly assisted the research.
Code availability
Not applicable
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Ethical approval
Not applicable
Consent to Participate
Written informed consent was obtained from all patients prior to study participation
Consent to Publish
Consent was obtained from the patients for publication of this peaper and accompanying images. A copy of the written consent is available for review by the Editor-in-Chief of this journal on request
Competing Interests
The authors have declared no conflicts of interest.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Level of evidence: IV, retrospective
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Sadougui, M., Amahtil, M., Bouziane, W. et al. Fracture-dislocation of the radiocarpal joint: bony and capsulo-ligamentar management, outcomes and long-term complications. International Orthopaedics (SICOT) 47, 2917–2925 (2023). https://doi.org/10.1007/s00264-023-05839-1
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00264-023-05839-1