
Abstract
It has been approximately two decades since we started performing carbon ion radiation therapy (C-ion RT) for non-small cell lung cancer (NSCLC). In 1994, we started conducting clinical trials using the dose-escalation method to determine the optimal dose of radiation. The additional purpose was to develop accurate, reliable, and safe irradiation techniques for C-ion RT.
In a subsequent phase II study of peripheral type stage I NSCLC, the total dose was fixed at 72 GyE in 9 fractions over 3 weeks and at 52.8 GyE for stage IA and at 60 GyE for stage 1B in 4 fractions over 1 week. In this way, the treatment period and fractionation were shortened and decreased from 18 fractions over 6 weeks to 9 fractions over 3 weeks and then further to 4 fractions over 1 week. Finally we were able to administer treatment as a single fraction.
For early-stage central- or hilar-type NSCLC, we conducted trials to identify the best way to preserve the pulmonary function with radical treatment. The prescribed dose for early central squamous cell carcinoma ranged from 54 to 61.2 GyE in nine fractions. For tumors close the hilus, we used 68.4 GyE/12 fractions, with planned target shrinking.
In addition, we also tried to treat locally advanced lung cancer, regional lymph node metastases that occurred after C-ion RT for clinical stage I cancer, and metastatic lung tumors.
This report describes the techniques and clinical trials that have been undertaken at the NIRS and describes the results of the current study. The use of C-ion RT for mediastinal or hilar lymph node metastases and metastatic lung tumors is described in Chap. 22.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
1 Introduction
Non-small cell lung cancer (NSCLC) patients are classified into two groups for radiotherapy (RT). The first group comprises those with advanced lung cancer, including patients with invasion of the chest wall, mediastinum, and/or mediastinal lymph nodes. The other group includes patients with early-stage disease, i.e., peripherally localized T1 or T2 tumors without evidence of lymph node metastases. In general, only early-stage lung cancer patients are expected to have a long survival.
Surgical resection has played a pivotal role in the treatment of peripherally localized lung cancer and can provide a 5-year survival rate of 60 % and a 5-year local control rate of more than 80 % [1, 2]. As a result, the first recommended treatment for early-stage peripheral lung cancer has been surgical resection. However, this is not always feasible, and surgery may have increased morbidity due to the patients’ medical conditions, such as pulmonary or cardiovascular disease. RT has played an important role as an alternative treatment for these patients. However, conventional RT provides relatively poor control of the primary tumor, thus resulting in 5-year survival rates of 30 % at best [3]. Dose escalation is essential to improve the effectiveness of RT, but this involves an increasing risk of normal tissue toxicity, especially pulmonary toxicity [4]. Since this can cause fatal reactions, it limits the applicable dose that can be given to the tumor. The goal of research on RT for lung cancer has therefore been to provide a higher dose to the target and lower doses to normal tissues, such as the lung parenchyma, esophagus, and spinal cord.
As a substitute for conventional RT, which is only a palliative treatment for medically inoperable localized NSCLC, various new modalities of RT have recently been developed, such as stereotactic body radiotherapy using photon beams (SBRT) and ion beam therapy (IBT). SBRT is now spreading worldwide, and a variety of new machines and techniques are being developed [5–9]. The radiation doses for SBRT are usually divided into multiple fractions given in multiple sessions. Hypofractionated SBRT, where few fractions of higher doses are administered, is usually applied for the treatment of peripheral stage I lung cancer [6–10]. Onishi et al. reported the results of SBRT for 257 patients with stage I NSCLC and showed lower toxicity and good local control rates (5.4 % of patients developed pulmonary complications above grade 2, and 14 % had local progression) [9]. Japan is one of the leading countries in the use of hypofractionated SBRT for the treatment of early-stage lung cancer [5].
Ion beams, with their improved dose distribution, are a novel and promising method that allows a higher dose to be applied to the tumor while minimizing the dose to the surrounding normal tissues. In particular, carbon ion radiotherapy (C-ion RT) seems to be an attractive modality due to its excellent dose distribution and increased biological effects in the Bragg peak region. Our clinical trials led us to conclude that irradiation with ion beams, notably carbon ions, offers a significant potential for improving tumor control, without increasing the risk of toxicity [11–17].
The National Institute of Radiological Sciences (NIRS) has conducted clinical trials on C-ion RT for lung cancer for almost two decades. A dose-escalation study using 18 fractions in 6 weeks was started for peripheral early-stage NSCLC in 1994. Between 1994 and 1999, a phase I/II dose-escalation study of the treatment of stage I peripheral NSCLC was conducted to determine the optimal dose and to evaluate if progression to hypofractionated C-ion RT was feasible [11]. Another purpose of these trials was to develop precise and safe irradiation techniques with maximum sparing of normal tissue.
The phase I/II study provided the following results:
-
1.
The local control rate was dose-dependent. Local control reached more than 90 % at 90.0 GyE with a regimen of 18 fractions over 6 weeks and at 72.0 GyE with a regimen of 9 fractions over 3 weeks. Both doses were determined to be optimal for each fractionation strategy.
-
2.
The damage to the lung was minimal; grade 3 radiation pneumonitis occurred in 2.7 % of the cases. Respiratory-gated and four-portal oblique irradiation techniques, which excluded opposed ports, proved to be successful for reducing the incidence of radiation pneumonitis.
-
3.
Survival was significantly related to the local control and size of the primary lesion. Local failure, distant metastasis, and malignant pleurisy were associated with decreases in survival.
After the phase I/II study using this optimized schedule, a phase II clinical trial that enrolled a total of 127 patients was initiated in April 1999 and was closed in December 2003 [12, 13]. In the phase II clinical trial, the total dose was fixed at 72.0 GyE in 9 fractions within 3 weeks, at 52.8 GyE for stage IA NSCLC, and at 60.0 GyE for stage IB NSCLC in 4 fractions within 1 week. After confirming the feasibility of irradiating the tumors in four fractions, a phase I/II dose-escalation clinical trial for single-fraction irradiation for peripheral stage I NSCLC was initiated in April 2003. The initial total dose was 28.0 GyE administered in a single fraction using respiratory-gated and four-portal oblique irradiation. The total dose was escalated in increments of 2.0 GyE up to 50.0 GyE. This article describes the preliminary results of the phase I/II clinical trial and the recent results of the phase II clinical trial in terms of the local control and survival rates after C-ion RT.
For locally advanced NSCLC, a dose-escalation study using 16 fractions in 4 weeks was started in 2000. Using respiratory-gated and three- or four-portal oblique irradiation, the optimal dose was found to be 72.0 GyE.
2 Treatment Methodology
2.1 Staging
Computed tomography (CT) scans of the chest and the whole abdomen, enhanced magnetic resonance imaging (MRI) of the brain, bone scans, and bronchoscopy are routinely performed to permit staging. Enrollment in clinical trials is subject to a clear pathological diagnosis of NSCLC based on transbronchial tumor biopsy (TBB), transbronchial aspiration cytology (TBAC), or CT-guided percutaneous needle biopsy (PCNB). If regional lymph nodes are greater than 1 cm in the short axis on contrast-enhanced CT images, as well as being positive on a 11C-methionine positron emission tomography (PET) scans, the regional lymph nodes are considered to be positive for metastasis [18]. Endobronchial ultrasound-guided transbronchial needle aspiration (EBUS-TBNA) for hilar and mediastinal lymph nodes was recently introduced to provide clearer evidence of the metastatic status. Clinical staging is performed according to the UICC TNM classification [19].
2.2 Marker Insertion
Small iridium markers (length: 3 mm, diameter: 0.5 mm) are inserted into the lung to verify the position and direction of a patient’s body during the irradiation. The markers do not interfere with the planning or implementation of the treatment. Routinely, two iridium rods are bronchoscopically placed into the patient’s lung (Fig. 21.1). The markers serve as fiducial landmarks to verify the position of the tumor in the lung. In each treatment session, they are visualized by X-ray radiography.

The treatment system. (A) The tumor shadow and metallic markers are shown by white arrows. (B) Patients receive the carbon ion beams from four directions, as indicated by the arrows. (C) A respiratory-gated irradiation system using infrared from an LED placed on the body surface
2.3 Immobilization
The immobilization devices consist of polyurethane fixtures and thermoplastic plates. The fixtures and plates are personalized for each patient before CT scanning for treatment planning. The patient is usually treated in the supine position. If the tumor is in the posterior lung, the patient assumes a prone position.
Irradiation is typically administered from four directions. As the beam lines are fixed in vertical and horizontal directions, the other two directions are achieved by tilting the patient to the left or right (Fig. 21.1).
2.4 Respiratory Gating
CT images for treatment planning are taken in synchronization with the respiratory motion. Because the displacement of a tumor is generally lowest at the end of the expiratory phase, this timing is applied for the actual irradiation. The respiratory sensing system uses a position-sensitive detector (PSD) as a camera, along with an infrared light-emitting diode (LED). The LED is attached to the patient’s body around the chest wall, and the light spot from the LED is focused on the PSD through a lens system [20]. A change in position is amplified by the zoom lens of the camera. The analog signals of the PSD are directly proportional to the spot position, without the need for a software program to calculate the position. The camera is typically mounted on the treatment couch at the feet of the patient, where it does not disturb the irradiation and does not interfere with the patient’s fixation device. Setup of the respiratory sensor takes less than 30 s (Fig. 21.1). Prompt starting and stopping of the beam extraction according to the gate signal are achieved by a special extraction method that provides an efficiency of more than 85 % of that of the standard extraction at the heavy ion medical accelerator in Chiba (HIMAC)[20, 21].
2.5 Irradiation
For patient positioning, fluoroscopic images are used, along with the superposition of the respiration waveform. Each treatment room of the HIMAC has a pair of orthogonal fluoroscopic devices. Fluoroscopic images of the patient in the optimal position are digitized and transferred to the positioning computer. They are displayed on the computer monitor screen, together with reference images, such as simulation images or digital reconstruction radiography, which are calculated based on the planning CT images. Fluoroscopy is performed from the beam’s eye view. The patient’s respiration waveform and the gate signal are also superimposed on the TV screen. The treatment couch is then moved to the matching position until the largest deviation from the field edge and the isocenter position is less than 2 mm. The whole procedure, including irradiation, takes about 20–30 min.
2.6 Follow-Up
Most patients underwent clinical examinations for follow-up, and CT scans of the thorax were carried out at our institute. Patients in whom follow-up testing could not be carried out until completion underwent periodic CT scanning at another institute. The clinical outcomes of all patients have been confirmed.
The first follow-up examinations were performed 4 weeks after C-ion RT and were repeated every 3–4 months. It is difficult to distinguish the changes in normal tissues due to radiation from tumor regrowth. We therefore defined transitorily enlarged densities observed after approximately 3 months as locally controlled tumors. Local recurrence was defined by an enlarging tendency of the tumor, as well as based on the findings of CT images, PET scans, tumor marker levels, and biopsy results.
3 Stage I Non-small Cell Lung Cancer
3.1 Stage I Peripheral Type Tumors
3.1.1 Treatment Planning
The targets are typically irradiated from four oblique directions without prophylactic elective nodal irradiation. A margin greater than 10 mm is set outside the gross target volume (GTV) to determine the clinical target volume (CTV). Spicular formations and pleural indentations are included in the CTV where possible. An internal margin (IM) is set outside the CTV in order to allow for target motion during gating. The planning target volume (PTV) is defined as the CTV plus IM. Three-dimensional treatment planning is performed using the HIPLAN software program, which was developed at the NIRS [22]. The IM is determined by extending the target margin in the head and tail directions by a width of 5 mm, which has resulted in the successful prevention of marginal recurrences caused by respiratory movement [23].
Compared with the pulmonary damage reported in stereotactic radiotherapy for stage I NSCLC [24, 25], the incidence and severity of the damage in our patients seem to be low. These mild adverse effects for the lung were achieved as a result of the small irradiated volume (V20 #9802 T1 (n = 30) mean 5.5 % (2.3–11.6), T2 (n = 21) mean 7.6 % (2.6–13.9), #0001 T1 (n = 41) mean 4.8 % (1.1–13.2), T2 (n = 39) mean 6.4 % (1.0–12.3)) achieved with the excellent dose distribution provided by the carbon ion beams due to the formation of a Bragg peak, which is in contrast to the results when X-rays are used as the permeating beam (Fig. 21.2).

The DVH of the phase II study (9802)
3.1.2 A Representative Case of Single Fraction C-Ion RT
An 83-year-old Japanese male was referred to the NIRS hospital with a diagnosis of primary lung cancer, of which the initial stage was T2N0M0 and the pathology was squamous cell carcinoma. The CT scan demonstrated that the tumor was located in the upper lobe (S3) of his right lung (Fig. 21.3).

The dose distribution of the planning CT and CT images pre- and postirradiation
CIRT was performed with four ports in four directions, and the total dose was 46.0 GyE in a single fraction. Twelve months later, the tumor demonstrated by the follow-up CT was noted to have decreased in size. The patient is still alive without any recurrence or metastasis 3 years after the CIRT.
3.1.3 Results
The local control rate for all patients (trial #9802 and #0001) was 91.5 %, and the rates for T1 and T2 tumors were 96.3 and 84.7 %, respectively. While there was a significant difference (p = 0.0156) in the control rates between T1 and T2 tumors, there was no significant difference (p = 0.1516) between squamous cell carcinomas and non-squamous cell carcinomas. The 5-year cause-specific survival rate was 67.0 % (IA: 84.4 %, IB: 43.7 %), and the overall survival was 45.3 % (IA: 53.9 %, 1B: 34.2 %). No adverse effects greater than grade 2 occurred in the lung in any of the patients.
In a single fractionation trial, the 3-year local control rate for 151 patients was 83.1 %, and the control rates for T1 and T2 tumors were 88.5 and 75.0 %, respectively. The overall survival rate was 75.5 %. No adverse effects greater than grade 2 occurred in the lung in any of these patients.
3.2 Stage I Central-Type Tumors
3.2.1 Treatment Planning
When treating lesions located near the lung hilus, there are concerns about the potential for serious damage to the pulmonary function resulting from bronchial stenosis [26]. During the treatment of peripheral lung tumors in our studies, we observed very little loss of pulmonary function after the C-ion RT [27]. However, any reduction of the pulmonary function is an adverse effect that can significantly impair the quality of life. We have therefore been making an extensive effort to minimize the risk of severe bronchial toxicity during the treatment of central tumors. Adequate target coverage (local control) and the sparing of the airway (unrelated segment bronchus) are necessary. For the airway sparing, using a small CTV (cutting off the bronchus from a large CTV) is important.
3.2.2 Central-Type Early Squamous Cell Lung Cancer
3.2.2.1 Planning in a Representative Case
A 66-year-old male patient with central early lung cancer (squamous cell carcinoma) located from the left main bronchus to the upper lobe bronchus was treated at our hospital. Irradiation with carbon ion beams at 61.2 GyE in 9 fractions within 3 weeks was performed in November of 2001. The treatment planning is shown in Fig. 21.4. Eight years after treatment, he is still alive and well without recurrence. No severe reaction was found on the follow-up CT or bronchoscopic examination.

Endoscopic findings prior to CIRT (left upper panel) and CT images. The tumor is shown by arrows. The planning CT images, where P1:P2:P3:P4 = 2:2:3:2, and P3 is a small target (left lower panel). An endoscopic image 8 years after CIRT (right lower panel)
3.2.3 Early-Stage NSCLC with an Extrabronchial Tumor Near the Hilus
3.2.3.1 Planning in a Representative Case
A 64-year-old male patient with left upper lobe (S4) lung cancer (squamous cell carcinoma) that measured 34 × 24 mm who also had hilar lymph node metastases was diagnosed with cT2N1M0 disease. Carbon ion radiation at 68.4 GyE was performed. As of 4 years after treatment, he is still alive and well, without any recurrence (Fig. 21.5).

The planning CT showing the four-portal irradiation. CT and endoscopic images taken pre- and post-therapy are shown. The arrow indicates the tumor
4 Locally Advanced Lung Cancer
4.1 Treatment Planning
Radiotherapy for advanced lung cancer is generally performed in combination with chemotherapy or surgery. During the CIRT for lung cancer, we treated some locally advanced lung cancer cases with CIRT alone. Because, these patients were unable to receive chemotherapy, or the cases of progressive disease after chemotherapy.
We have been making an extensive effort to minimize the risk of pulmonary, tracheal, and esophageal toxicity associated with the treatment. Using a small CTV for the primary lesion allows us to decrease the prescribed dose for the mediastinum. This will help improve the patients’ overall status, potentially increasing the number of patients who can receive chemotherapy.
4.2 Planning in Representative Cases
Case 1
-
A 75-year-old male patient with right lower lobe (S6) lung cancer (adenocarcinoma) measuring 40 × 38 mm, with chest wall infiltration and nodal metastasis of the right hilum, was diagnosed to have cT3N1M0 stage IIIA disease. Carbon ion beam irradiation at 72.0 GyE in 16 fractions over 4 weeks was performed in January 2004. Figure 21.6 shows a CIRT planning image.
Fig. 21.6 
The left panel shows the CTV and planning dose distribution, including 3D images and the body surface model. The irradiation times of each port were P1:P2:P3:P4 = 4:3:3:6. P4 is the small target for the primary tumor. The right panel shows the pre- and post-CIRT images
-
The entire large target, including the primary tumor, hilum, and mediastinum, was irradiated at 45.0 GyE, and then the primary tumor was irradiated to a final dose of 72.0 GyE. At 4 years after treatment, he was well without any recurrence.

Case 2
-
A 67-year-old male patient with left upper lobe lung cancer (adenocarcinoma) of 62 × 50 mm, with infiltration into the mediastinum, was diagnosed with cT4N0M0 stage IIIB disease. Irradiation with carbon ions at 72.0 GyE was performed. At 10 years after treatment, he is still alive and well without any recurrence (Fig. 21.7).
Fig. 21.7 
The planning CT showing the four-portal irradiation. The irradiation times for each port were P1:P2:P3:P4 = 4:4:5:3. The CT images taken pretreatment and 3 months and 10 years after therapy are shown

4.3 Results
Sixty-one patients were treated in this clinical trial between May 2000 and September 2011. The 61 primary tumors were treated by carbon ion beam irradiation alone using a total dose of 72.0 GyE in 16 fractions over 4 weeks. The mean age of the patients was 74.2 years (46–88), and the gender breakdown was 14 females and 47 males. By histological type (the cancer type was determined by biopsy), there were 27 adenocarcinomas, 31 squamous cell carcinomas, and three large cell carcinomas. Of the 61 patients, 39 were in stage II and 22 were in stage III, while there were 24 N1 cases, 13 N2 cases, and 24 N0 (T3-4N0M0) cases.
The statistical 3-year overall survival rate of the 61 patients was 41.2 %, with a median observation period of 22.8 months (range, 1.3–145.3 months). The 3-year cause-specific survival rate of 24 patients with chest wall infiltration (cT3,4N0M0) was 77.9 % with a median observation period of 37.1 months (range, 4.3–141.6 months) (Fig. 21.8).

The survival rate in 61 patients with locally advanced lung cancer. (a) The 3-year overall survival rate of all patients was 41.2 %. (b) The 3-year cause-specific survival rates based on the N factor
The toxicities to the skin and lungs caused by CIRT were assessed according to the NCI-CTC (early) and RTOG/EORTC (late). No adverse events greater than grade 2 were detected among the early and late reactions.
5 Normal Tissue Reaction
5.1 Pulmonary and Skin Reactions
In the previously reported phase II study, 129 patients with 131 primary lesions were treated with C-ion RT. Fifty-one primary tumors in 50 patients were treated by carbon ion beam irradiation alone using a fixed total dose of 72 GyE in 9 fractions over 3 weeks (#9802 protocol [12]). The remaining 79 patients had 80 stage I tumors (#0001 protocol [13]). A total of 127 patients were evaluated for survival, because two patients had been treated twice, one in the first protocol #9802 and one in the second protocol #0001. The IA and IB stage tumors were treated with fixed doses of 52.8 and 60.0 GyE in 4 fractions over 1 week, respectively. The mean age of the patients was 74.5 years, and the gender breakdown was 92 males and 37 females. The tumors were 72 T1 and 59 T2 tumors. The mean tumor size was 31.5 mm in diameter. By type, there were 85 adenocarcinomas, 43 squamous cell carcinomas, two large cell carcinomas, and one adenosquamous cell carcinoma. Medical inoperability had been diagnosed in 76 % of cases.
Toxicities to the skin and lungs caused by C-ion RT were assessed according to the RTOG (early) and RTOG/EOTRC (late) guidelines, as shown in Tables 21.1 and 21.2. Early skin reactions were assessed for 131 lesions and late skin reactions for 128 lesions. Of the early reaction lesions, 125 were grade 1 and six were grade 2. Among the late reaction lesions, 126 were grade 1, one was grade 2, and one was grade 3. The lung reactions were clinically assessed in 129 patients. One hundred twenty-seven had grade 0 and two had grade 2 early reactions. Late effects were followed up in 126 patients: seven patients had grade 0, 116 patients had grade 1, and three patients had grade 2 effects. No higher than a single grade 2 reaction was observed.
We also reported the pulmonary functions and pathological findings of the patients after C-ion RT [27, 28] and demonstrated that the patients in this trial suffered from less lung damage. These less extensive and severe adverse effects for the lungs were achieved as a result of the excellent dose distribution achieved with carbon ion beams due to the formation of a Bragg peak. Furthermore, in a report regarding the radiographic changes of the lungs after C-ion RT, we described that the lung damage was observed in the parenchyma and the pleura. The severity of pulmonary reactions was correlated with dose-volume factors [29].
These findings provided valuable information for the planning of C-ion RT and for the management of patients after treatment.
5.1.1 Planning in Representative Cases
Case 1
-
A 62-year-old female with a 15 × 15 mm adenocarcinoma located in the left lower lobe (S10) was clinically diagnosed to have cT1N0M0 stage IA disease. Irradiation with a carbon ion beam at 72.0 GyE in 9 fractions over 3 weeks was performed. Ten years after treatment, she is still alive and well without any recurrence (Fig. 21.9).
Fig. 21.9 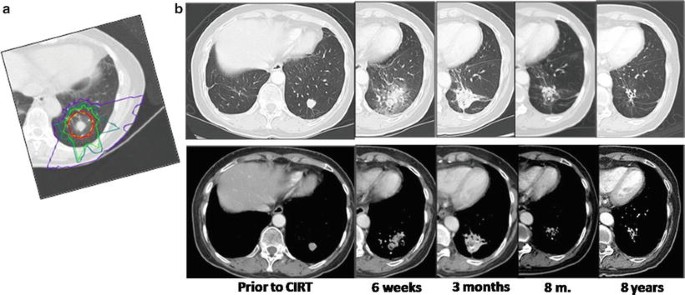
(a) The dose distribution and (b) the changes of the tumor shadow after CIRT. The early lung reaction (RTOG) and late lung reaction (RTOG/EORTC) were both grade 1

Case 2
-
A 60-year-old male patient with squamous cell carcinoma of 61 × 60 mm in size located in the right lower lobe was diagnosed with T2N0M0 disease. Carbon ion beam irradiation at 44.0 GyE in 1 day was performed. The treatment planning and skin reactions are shown in Fig. 21.10. We confirmed that the surface dose was not more than 75 % of the prescribed dose. It is important to minimize the risk of skin reactions (Fig. 21.10), and we believe this planning can help improve the outcome.
Fig. 21.10 
(A) The Dose distribution for a tumor receiving a total carbon ion dose of 44.0 GyE from four directions. (B) CT images before and after treatment. Four months after the treatment, the tumor showed a partial response (PR). (C) The body surface model of the planning dose distribution for the patient. The yellow area is 75 % of the total dose for the beams from three portals that overlapped in that area. (D) The early skin reaction was grade 2 (2 months after irradiation, left), and the late reaction (4 months after CIRT, right) was grade 1

Case 3
-
A 71-year-old female with T2N0M0 squamous cell carcinoma (46 × 38 mm in size) was treated with CIRT (40 GyE/single fraction). At 18 months after C-ion RT, the tumor shrank without severe lung fibrosis. Figure 21.11 shows the PTV of the C-ion RT and skin reactions.
Fig. 21.11 
(A) The dose distribution for a tumor receiving a total carbon ion dose of 40.0 GyE from four directions. The body surface model of the planning dose distribution for the patient. (B) CT images before and after treatment. Eighteen months after the treatment, the tumor showed a partial response. (C) The early skin reaction was grade 1 (5 weeks after irradiation, left), and the late reaction (7 months after CIRT, right) was grade 1

5.2 Chest Wall Adverse Reactions
Of 50 patients who received 72.0 GyE in nine fractions, ten patients complained of costal bone pain and tenderness around the part of the skin receiving carbon beams, which appeared at 10 ± 2.3 months on average after the start of therapy. Slight swelling of the bone and the surrounding soft tissue was observed by inspection or CT scans and disappeared within at most 1 month after. Half of the patients needed nonsteroidal anti-inflammatory medication. Costal bone fractures were observed in two patients.
A reaction of the chest wall is an adverse effect that, depending on the severity, can significantly impair the patient’s quality of life. We have been making an effort to minimize the risk of severe chest wall toxicity, and for rib sparing, by cutting off the PTV margin on the bone.
5.2.1 Case Study
A 69-year-old male patient with lung cancer (adenocarcinoma cT2N0M0; 37 × 25 mm) located in the left upper lobe (S5) was treated with carbon ion beam radiotherapy (72.0 GyE/9 fr/3 weeks). Nine months after treatment, he complained of pain around the skin that had received the carbon beams, and the pain resolved in a month. At 4 years after treatment, he was well without any recurrence (Fig. 21.12).

The upper panel shows the CT images before and after the treatment. The costal bone fracture appeared 30 months after CIRT
References
Asamura H, Goya T, Koshiishi Y, et al. A Japanese Lung Cancer Registry study: prognosis of 13,010 resected lung cancers. J Thorac Oncol. 2008;3:46–52.
Smythe WR, American College of Chest Physicians. Treatment of stage I non-small cell lung carcinoma. Chest. 2003;123:181S–7.
Jeremic B, Classen J, Bamberg M. Radiotherapy alone in technically operable, medically inoperable, early-stage (I/II) non-small-cell lung cancer. Int J Radiat Oncol Biol Phys. 2002;54:119–30.
Zimmermann FB, Bamberg M, Molls M, et al. Radiation therapy alone in early stage non-small cell lung cancer. Semin Surg Oncol. 2003;21:91–7.
Nagata Y, Hiraoka M, Mizowaki T, et al. Survey of stereotactic body radiation therapy in Japan by the Japan 3-D Conformal External Beam Radiotherapy Group. Int J Radiat Oncol Biol Phys. 2009;75:343–7.
Zimmermann FB, Geinitz H, Schill S, et al. Stereotactic hypofractionated radiation therapy for stage I non-small cell lung cancer. Lung Cancer. 2005;48:107–14.
Onishi H, Araki T, Shirato H, et al. Stereotactic hypofractionated high-dose irradiation for stage I nonsmall cell lung carcinoma: clinical outcomes in 245 subjects in a Japanese multiinstitutional study. Cancer. 2004;101:1623–31.
Senan S, Lagerwaard F. Stereotactic radiotherapy for stage I lung cancer: current results and new developments. Cancer Radiother. 2010;14:115–8.
Onishi H, Shirato H, Nagata Y, et al. Hypofractionated stereotactic radiotherapy (HypoFXSRT) for stage I non-small cell lung cancer: updated results of 257 patients in a Japanese multi-institutional study. J Thorac Oncol. 2007;2 Suppl 3:S94–100.
Nagata Y, Takayama K, Matsuo Y, et al. Clinical outcomes of a phase I/II study of 48 Gy of stereotactic body radiotherapy in 4 fractions for primary lung cancer using a stereotactic body frame. Int J Radiat Oncol Biol Phys. 2005;63:1427–31.
Miyamoto T, Yamamoto N, Nishimura H, et al. Carbon ion radiotherapy for stage I non-small cell lung cancer. Radiother Oncol. 2003;66:127–40.
Miyamoto T, Baba M, Yamamoto N, et al. Curative treatment of stage I non-small-cell lung cancer with carbon ion beams using a hypo-fractionated regimen. Int J Radiat Oncol Biol Phys. 2007;67:750–8.
Miyamoto T, Baba M, Sugane T, et al. Carbon ion radiotherapy for stage I non-small cell lung cancer using a regimen of four fractions during 1 week. J Thorac Oncol. 2007;2:916–26.
Sugane T, Baba M, Imai R, et al. Carbon ion radiotherapy for elderly patients 80 years and older with stage I non-small cell lung cancer. Lung Cancer. 2009;64:45–50.
Kanai T, Endo M, Minohara S, et al. Biophysical characteristics of HIMAC clinical irradiation system for heavy-ion radiation therapy. Int J Radiat Oncol Biol Phys. 1999;44:201–10.
Nishimura H, Miyamoto T, Yamamoto N, et al. Radiographic pulmonary and pleural changes after carbon ion irradiation. Int J Radiat Oncol Biol Phys. 2003;55:861–6.
Yamamoto N, Miyamoto T, Nishimura H, et al. Preoperative carbon ion radiotherapy for non-small cell lung cancer with chest wall invasion-pathological findings concerning tumor response and radiation induced lung injury in the resected organs. Lung Cancer. 2003;42:87–95.
Yasukawa T, Yamaguchi Y, Aoyagi H, et al. Diagnosis of hilar and mediastinal lymph node metastasis of lung cancer by positron emission tomography using 11C-methionine. Jpn J Lung Cancer. 1996;36:919–26.
Sobin LH, Wittekint C, editors. TNM classification of malignant tumors. International Union Against Cancer (UICC). 6th ed. NewYork: Wiley-Liss; 2002.
Minohara S, Kanai T, Endo M, et al. Respiratory gated irradiation system for heavy-ion radiotherapy. Int J Radiat Oncol Biol Phys. 2000;47:1097–103.
Kanai T, Furusawa Y, Fukutsu K, et al. Irradiation of mixed beam and design of spread-out Bragg peak for heavy-ion radiotherapy. Radiat Res. 1997;147:78–85.
Endo M, Koyama-Ito H, Minohara S, et al. HIPLAN-a heavy ion treatment planning system at HIMAC. J Jpn Soc Ther Radiol Oncol. 1996;8:231–8.
Koto M, Miyamoto T, Yamamoto N, et al. Local control and recurrence of stage I non-small cell lung cancer after carbon ion radiotherapy. Radiother Oncol. 2004;71:147–56.
Nagata Y, Takayama K, Matuo Y, et al. Clinical outcomes of a phase I/II study of 48Gy of stereotactic body radiotherapy in 4 fractions for primary lung cancer using a stereotactic body frame. Int J Radiat Oncol Biol Phys. 2005;63:1427–31.
Onishi H, Araki T, Shirato H, et al. Stereotactic hypofractionated high-dose irradiation for stage I nonsmall cell lung carcinoma. Cancer. 2004;101:1623–31.
Timmerman R, MacGarry R, Yiannoutsos C, et al. Excessive toxicity when treating central tumors in a phase II study of stereotactic body rdiation therapy for medically inoperable early-stage lung cancer. J Clin oncol. 2006;24:4833–9.
Kadono K, Homma T, Kamahara K, et al. Ekkect of heavy – ion radiotherapy on pulmonary function in stage I Non-small cell lung cancer patients. Chest. 2002;122:1925–32.
Yamamoto N, Miyamoto T, Nishimura H, et al. Preoperative carbon ion radiotherapy for non-small cell lung cancer with chest wall invasion pathological findings concerning tumor response and radiation induced lung injury in the resected organs. Lung Cancer. 2003;42:87–95.
Nishimura H, Miyamoto T, Yamamoto N, et al. Radiographic pulmonary and pleural change after carbon ion irradiation. Int J Radiat Oncol Biol Phys. 2003;55:861–6.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2014 Springer Japan
About this chapter
Cite this chapter
Yamamoto, N., Nakajima, M. (2014). Lung Cancer. In: Tsujii, H., Kamada, T., Shirai, T., Noda, K., Tsuji, H., Karasawa, K. (eds) Carbon-Ion Radiotherapy. Springer, Tokyo. https://doi.org/10.1007/978-4-431-54457-9_21
Download citation
DOI: https://doi.org/10.1007/978-4-431-54457-9_21
Published:
Publisher Name: Springer, Tokyo
Print ISBN: 978-4-431-54456-2
Online ISBN: 978-4-431-54457-9
eBook Packages: MedicineMedicine (R0)