
Abstract
Contrast media (CM) are important in X-ray diagnostics to make certain tissues but also pathological processes, e.g. tumors, visible and to be able to assess them better. They are divided into different classes (positive/negative, water-soluble/insoluble, ionic/non-ionic, monomer/dimer) and used for different examinations. In addition to this aspect, however, the chapter also deals with the most common side effects that can be triggered by CM.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Contrast media (CM) are important in X-ray diagnostics in order to make certain tissues, but also pathological processes, e.g. tumors, visible and to be able to assess them better. They are divided into different classes (positive/negative, water-soluble/insoluble, ionic/non-ionic, monomer/dimer) and used for different examinations. In addition to this aspect, however, the chapter also deals with the most common side effects that can be triggered by CM.
1 X-ray Contrast Medium
Contrast media (CM) are used in radiology to better highlight tissue structures and thus make them assessable. Since certain organs (e.g. the abdominal organs) have a similar density, they would be difficult to distinguish in imaging without CM.
In addition, the aim of using X-ray contrast media is to achieve better imaging while at the same time being well tolerated by the patient.
Good imaging is dependent on
-
a high contrast,
-
a detailed representation,
-
a long enough contrast display depending on the examination.
Good tolerance of the contrast agent means that the CM
-
does not negatively affect any physiological processes/functions,
-
does not penetrate the blood-brain barrier or cell membranes,
-
can be quickly and completely excreted again,
-
does not result in any undesirable side effects.
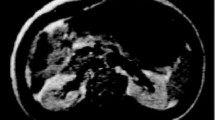
The enhancement, i.e. the accumulation of CM in the organs or tissues, is dependent on the respective organ or tissue structure and in part allows conclusions to be drawn about a specific structure in the body (e.g. in the case of the hemangioma by the so-called rosette phenomenon, ◘ Fig. 9.1).

Hemangioma of the liver with contrast enhancement
Tasks of contrast agents
-
Contrast enhancement in fabrics that otherwise differ little or not at all in density
-
Improvement of the assessability of functional processes (e.g. blood flow, excretion, etc.)
-
1.1 Classification of X-ray CMs
Contrast media can reduce the absorption of X-rays (so-called negative X-ray contrast media) in order to differentiate from the surrounding tissue, or increase it (so-called positive X-ray contrast media).
X-ray contrast media are therefore divided into two main groups:
-
1.
Substances with lower density than the environment to be imaged = negative contrast media (gases, water, methyl cellulose, sorbitol, mannitol)
-
2.
Substances with a higher density than the environment to be depicted = positive contrast media (differentiation into water-soluble, water-insoluble and oil-containing)
1.1.1 Contrast Media Negative
Negative contrast agents (◘ Fig. 9.2) used in X-ray diagnostics include gases, i.e. carbon dioxide (CO2), nitrogen dioxide (NO2), noble gas and simply: air (e.g. for imaging the stomach and intestines). But also water (or water-mannitol solutions), methyl cellulose, paraffin suspensions and sorbitol (sugar alcohol, sugar substitute) or mannitol belong to the negative CM.

Negative contrast agents. (From Hartmann et. al 2014)
Sorbitol intolerance should be clarified before using Sorbitol!
Side effects of Mannitol may include:
-
Disturbances of the fluid and electrolyte balance
-
Hypotension
-
Allergic reactions
-
Cardiac arrhythmias
-
Vertigo
Similar to methyl cellulose, carbon dioxide is used, for example, in gastrointestinal diagnostics, e.g. for double-contrast examination of the stomach and for imaging in virtual colonoscopy (◘ Fig. 9.3a, b). It is generally better absorbed in the intestine than room air and thus, as studies have shown, better tolerated by the patient.

Virtual colonoscopy in 3D a and 2D b reconstruction. A pedunculated polyp was seen (arrow). (From Mang et al. 2008)
CO2 can also be used in intra-arterial angiography of the kidneys, the lower extremity and in the diagnosis of dialysis shunts as a contrast medium with very few side effects. Patients with an intolerance to iodine-containing contrast media and patients with renal insufficiency are of particular benefit. However, CO2 must not be used in angiography of the thorax, upper extremities or supraaortally, as this can trigger serious neurological complications, in the worst case accompanied by strokes.
Double Contrast—What Does that Mean?
Double contrast means performing fluoroscopy with a positive CM (usually barium, section water-insoluble contrast media) and a negative CM (e.g. cellulose, water, CO2). The negative CM provides better distension (widening, expansion) of the bowel and distribution of the positive CM, resulting in better contrast of the bowel folds. This technique (the best known method is the enteroclysma, i.e. the contrast enema according to Sellink) is no longer frequently performed, as other imaging methods (especially magnetic resonance imaging) are now preferred for the desired visualization.
Room air is used (partly supplementary) for imaging the gastrointestinal tract (e.g. colon double contrast examination) and for arthrographies (contrast medium-supported radiological joint examination).
1.1.2 Contrast Media Positive
1.1.2.1 Water-Soluble Contrast Media Containing Iodine (◘ Fig. 9.4)
Iodine-containing, water-soluble contrast media are used for the imaging of
-
Vessels (angiography, phlebography),
-
Renal pelvic calices and urinary tract (e.g. MCU, cystography),
-
Gastrointestinal tract (oral),
-
Bile ducts (e.g. ERCP, PTCD).

Positive, water-soluble contrast agents. (From Hartmann et. al 2014)
Especially in computed tomography (specifically: CT angiography, CT coronary angiography) they are often used. They are also used in myelography.
Why Iodine?
Iodine-containing CMMs are used because iodine as a chemical element has a high contrast density as well as a relatively low toxicity and forms a strong bond with the other chemical structures of the contrast agent complex.
Triiodobenzoic Acid (Renal)
These are contrast media that are largely excreted through the kidney by glomerular filtration (therefore renal = nephrotop). A small part is also excreted via the liver-biliary system and the intestine.
Triiodobenzenes produce a well-contrasted representation and are classified into ionic and non-ionic CMs, whereby ionic CMs are no longer used in practice because they have a higher side-effect potential (◘ Table 9.1).
If the limit is exceeded or if liver function is impaired, the CM is excreted via the kidneys (renal insufficiency)!
In the case of a pathological restriction of liver metabolism, special attention should be paid to a particularly gentle slow infusion.
Contrast Media Ionic
Ionic contrast agents carry a salt group in their chemical structure, which gives them an ionic charge. They have a high osmolality (number of osmotically active particles in a solution) and a higher plasma protein binding. This also makes them less well tolerated, in contrast to non-ionic CM (◘ Table 9.1). The BfArM (Federal Institute for Drugs and Medical Devices) declared in 2000 on the i.v. application of certain ionic contrast media:
Ionic high-osmolar contrast media exhibit a higher chemotoxicity and a higher osmotoxicity than the low-osmolar non-ionic contrast media preferred today. Chemotoxicity and osmotoxicity cause a variety of undesirable effects on different organs and organ systems, respectively. The intravascular application of ionic contrast media is associated with a significantly higher risk of triggering a contrast medium side effect in all patient groups compared to the application of non-ionic monomeric contrast media.
Ionic CMMs are hardly ever used in X-ray diagnostics, especially as i.v. CMs (◘ Fig. 9.5)—their use should be well weighed up with regard to possible risks and pre-existing underlying diseases (morbidities) of the patients.

More strongly contrasted colon (right) after rectal filling with diluted contrast medium, orally given CM (loops of small intestine) is more diluted due to fluid retention in the intestine in case of bridenileus in the right lower abdomen
Contrast Media Non-Ionic
As the name suggests, non-ionic CMs have no ionizing group, but a hydrophilic (i.e. water-loving) group that ensures solubility. Since they have a lower osmolality than ionic CM (but still twice as high as that of plasma), they are also referred to as low-osmolar CM (◘ Table 9.1). Because of this property, they are also associated with side effects much less frequently.
Intravenous iodine-containing contrast media are eliminated renally. Only a small proportion is excreted hepatically via the bile. This proportion may cause you to see contrast of the gallbladder one or two days after intravenous contrast administration (◘ Fig. 9.6).

Intravenous pyelogram (IVP) 12 min after CM administration
Monomers and Dimers
Both ionic and nonionic contrast agents have monomeric and dimeric variants. The difference lies in the chemical structure: the number of benzene rings in dimeric nonionic CMMs is two, in monomeric nonionic CMMs only one—due to the more complex structure, dimeric nonionic CMMs are also more viscous, i.e. more viscous, and must therefore be warmed up before application, as the viscosity decreases with increasing temperature.
CM are before their use in a heat cabinet to reduce the viscosity. Due to the viscosity, the CM can only be injected with increased force. Therefore, errors can occur with CM pumps when they are cold. Therefore, care must be taken to ensure that a heat sleeve is used.
Dimeric ionic contrast agents, on the other hand, have two acid groups, for example.
1.1.2.2 Water-Insoluble Contrast Media
Barium Sulphate
Barium sulphate (BaSO4) is used in the diagnosis of the gastrointestinal tract as an orally administered CM (◘ Fig. 9.7). However, today it is only used in very rare cases.

Coronary reconstruction with elongated foreign body in the terminal ileum (arrow); in the selected bone window, the foreign body stands out better from the diluted barium sulfate in the other intestinal loops due to its higher density. (From Fabel 2006)
Since barium sulfate is hypotonic to blood plasma, it can cause dehydration in the intestine.
It must not be used in cases of suspected ileus (intestinal obstruction), perforation or suture insufficiency, dysphagia (risk of aspiration!) or other serious illnesses.
1.1.2.3 Contrast Media Containing Oil
Oils
Oils that have been iodized are used in lymphography. However, they are difficult to degrade in the body and produce by-products, and are therefore associated with many disadvantages and side effects. Since water-soluble contrast media would diffuse too quickly in the lymphatic system, and thus no good imaging of the lymphatic vessels is possible, there is no alternative. In the past, iodinated oils were also used in myelography (◘ Fig. 9.8), but due to the severe side effects, this is now only performed with water-soluble non-ionic contrast media.

Myeolography with oily CM. (From Hartmann et al. 2014)
The amount of CM to be administered depends on the examination, the weight of the patient and the iodine concentration of the CM. In CT, concentrations of 400 mg iodine/ml are often administered. Thus, if a patient is injected with 100 mL of CM, he or she will receive 40 g of iodine! The daily requirement of an adult is 180–200 μg per day.
2 MR Contrast Medium
The functioning of MRI is related to relaxation times as already shown. The signal strength of the tissue is significantly influenced by the T1 and T2 relaxation time. The use of contrast agents increases the signal difference between the tissues and thus the image contrast.
To achieve this, substances with a large magnetic moment (many unpaired electrons on the outermost shell) are used, which accelerates the ambient relaxation (decay of magnetizations) in the environment. Gadolinum complexes are commonly used MR contrast agents in this context.
The amount of relaxation time reduction is called relaxivity. It is a measure of the effectiveness of an MR contrast agent.
Since the effect is stronger in T1 measurements, CM are mainly used in such sequences.
MR-CM can be used as positive (“whiteners”) and negative (“blackers”) depending on the measurement in which they are used. Since they shorten the relaxation times in both T1 and T2 time, they can lead to different image effects.
-
The shortening of the T1 time leads to a faster reconstruction of the longitudinal magnetization and thus to a signal amplification (white).
-
The shortening of the T2 time leads to a faster decay of the transverse magnetization and thus to a signal drop (black) (◘ Fig. 9.9).

Magnetic resonance cholangiopancreaticography (MRCP) with negative contrast of the stomach with 100 mL of pineapple juice immediately before the examination. Note the signal-elevated distal loops of small bowel and the pineapple juice signal-extinguished stomach. The contrast is due to the high manganese and iron content of the pineapple juice
2.1 Gadolinum
Gadolinum is the “all-rounder” among the MR contrast agents, has seven unpaired electrons and greatly reduces the relaxation time (in T1-weighted sequences with signal enhancement). However, the free paramagnetic ions are very toxic. Therefore, the MR contrast agents used are derivatives of gadolinum (◘ Fig. 9.10). These include:

Imaging of a neuroectodermal tumor in a 5-year-old girl using gadolinum MR. (From Choi 2005)
Non-Specific Gadolinum Complexes
-
Are excreted via the kidney,
-
distribute only in the extracellular space (no penetration of the blood-brain barrier),
-
have an HWZ of 90 min,
-
are not metabolized or bound to proteins,
-
have a high stability.
The accumulation of gadolinium in a tissue depends on the general condition of the patient (fever), the waiting time after the injection and the dose (“much helps much”). The contrast medium may “behave differently” in a patient with fever than in patients without fever. This may play a role in the findings.
MR contrast media are generally well tolerated. Side effects occur in only 1–2% of examinations, mainly affecting the kidney. In a few cases, allergic reactions have also been reported.
The edema signal in STIR or TIRM sequences is masked by CM administration, so these sequences must be performed before contrast administration.
3 Sonographic Contrast Agent
Contrast agents used in sonography perform their function by increasing the reflection of ultrasound waves—this results in a stronger signal response, which can be read on the ultrasound screen as higher contrast.
The imaging of contrast microbubbles in diagnostic sonography is based on excitation of the microbubbles in the sound field, whereby the microbubbles start to oscillate.
The higher the intensity of the irradiated ultrasonic waves, the stronger the reaction of the microbubbles (up to bubble destruction).
4 Contraindications
The most important contraindications are given in the following overview:
Contraindications for CM Application
Absolute Contraindications
-
Severe kidney dysfunction not previously requiring dialysis
-
Manifest hyperthyroidism
-
Anaphylactoid reaction to the iodine-containing CM to be used
-
Certain thyroid carcinomas
Relative Contraindications
-
Heart failure
-
Severe hepatic dysfunction
-
Hematological diseases (Waldenström’s disease)
After CM injection, thyroid scintigraphy is not informative!
5 Side Effects
Adverse reactions caused by CM may be dose-dependent or dose-independent (◘ Table 9.2).
Among other things, vasodilatation may occur, which causes a drop in blood pressure (hypotension). Histamines released from mast cells are responsible for an immediate allergic reaction and in turn lead to vasodilation of the small peripheral vessels. This is the cause of a possible circulatory shock. Furthermore, an involvement of the coagulation system and the CNS is discussed.
Many patients assume that a CM reaction is accompanied by an iodine allergy—but an iodine allergy would not be compatible with life, since we need iodine as an indispensable component of our human metabolism.
An adverse CM reaction is not based on an iodine allergy, but is due to an intolerance of the CM complex.
Locally, especially with iodine-containing contrast media, pain, damage to the vessel walls, vasodilatation (→ drop in blood pressure) may occur.
Low osmolar CMs are generally better tolerated than high osmolar ones, non-ionic ones better than ionic ones.
Special caution and close scrutiny of the use of CM is required in patients with:
-
Status after severe CM reaction
-
Allergies
-
Bronchial asthma
-
Kidney disease
-
Thyroid disorders
6 Pregnancy and Breastfeeding
Pregnancy is a relative contraindication for an X-ray examination. The radiation exposure is relatively high for the unprotected child, depending on the planned examination. In certain emergency situations, it is nevertheless unavoidable to perform an examination on a pregnant patient. There are no precise data on the extent to which CM is transferred to the fetus and exposes it in this case.
About 1% CM is found in the mother’s milk. That this amount has a harmful effect on the infant has not yet been proven. The current recommendation does not call for any special measures. Nevertheless, a 24-hour breastfeeding break can be considered.
Practice Questions
-
1.
Which negative and positive contrast media are used in radiology?
-
2.
What factors influence the accumulation of gadolinum in tissues?
-
3.
What is meant by “double contrast”?
-
4.
What are absolute, what are relative contraindications for the administration of CM?
-
5.
What should be considered during breastfeeding with regard to the administration of CM?
Solutions ► Chap. 27
Author information
Authors and Affiliations
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2023 Springer-Verlag GmbH Germany, part of Springer Nature
About this chapter

Cite this chapter
Kahl-Scholz, M. (2023). Contrast Agent. In: Kahl-Scholz, M., Vockelmann, C. (eds) Basic Knowledge Radiology. Springer, Berlin, Heidelberg. https://doi.org/10.1007/978-3-662-66351-6_9
Download citation
DOI: https://doi.org/10.1007/978-3-662-66351-6_9
Published:
Publisher Name: Springer, Berlin, Heidelberg
Print ISBN: 978-3-662-66350-9
Online ISBN: 978-3-662-66351-6
eBook Packages: MedicineMedicine (R0)