
Abstract
The chapter “Conventional X-ray diagnostics” deals with the origin of X-ray radiation, the structure of the X-ray tube and the possibility of regulating the type and amount of radiation. Furthermore, the creation of the digital X-ray image as well as the processing of the images are dealt with, and special devices of conventional X-ray diagnostics are described as examples. Furthermore, you will find an overview of the basic specifications of the guidelines of the German Medical Association for conventional X-ray diagnostics.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others

The chapter “Conventional X-ray diagnostics” deals with the origin of X-ray radiation, the structure of the X-ray tube and the possibility of regulating the type and amount of radiation. Furthermore, the formation of the digital X-ray image as well as the processing of the images are dealt with, and special devices of conventional X-ray diagnostics are described as examples. Furthermore, you will find an overview of the basic specifications of the guidelines of the German Medical Association for conventional X-ray diagnostics.
1 Design and Operation of an X-ray System
An X-ray system always consists of the following components:
-
an X-ray source that generates the beams,
-
an X-ray generator, which supplies the X-ray source with high voltage,
-
an X-ray application device used for positioning the patient, and
-
an X-ray image converter (X-ray film, detector,…).
1.1 The X-ray Source
1.1.1 Structure of the X-ray Tube
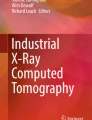
An X-ray source is a cathode source and consists of a negatively charged cathode and a positively charged anode. By heating the cathode, electrons can be released from the cathode. Due to the different charges between the cathode and the anode, these electrons are then accelerated towards the anode and finally hit the anode where, among other things, X-rays are produced (◘ Fig. 2.1).

Schematic structure of an X-ray source. (From Hartmann et al. 2014)
Since the electrons would be slowed down and deflected in normal air, the cathode and anode are located in an evacuated, i.e. airless, glass bulb. This glass bulb is located in an oil-filled radiation protection housing. The oil serves to protect against the high voltage and to dissipate heat to the outside. The protective housing also shields the parts of the X-ray radiation that do not exit through the radiation exit window. Below the radiation exit window is a legally required filter made of 1.5 mm thick aluminum. This filters out the radiation that is unable to penetrate the body due to its energy.
The Cathode
The cathode consists of one or two filaments which are heated by the so-called tube current. The heat causes the electrons to oscillate (thermal electron emission) and they can be released by the voltage triggered between the cathode and the anode. The filaments are mainly made of tungsten, since tungsten has the highest melting point of all metals (3680 K = 3406.85 °C) and the electrons can also be released relatively easily. The released electrons or the electron cloud is now accelerated towards the anode.
Since the electrons would travel undirected in the direction of the anode, they are focused by a Wehnelt cylinder. This cylinder is located in the immediate vicinity of the cathode. By applying a negative charge, the exit of the electrons can be regulated and the direction of flight focused.
The Anode
When the electrons hit the focal spot (also called focus) at the anode, various processes or even interactions occur. Only 1% of the energy is converted into X-rays, 99% of the energy is released into heat.
Because of the large amount of heat generated, the anode must be made of a particularly heat-resistant and thermally conductive material. Here, too, tungsten or a tungsten-rhenium mixture has proven to be ideal. In order to distribute the heat generated over a large volume, rotating anodes are used in X-ray diagnostics. The anode is shaped like a plate and is rotated by an electric motor (typical speed: approx. 3000 rpm). This heats not only a single point, but an entire circular path. Since the electrons always “destroy” tiny parts of the anode, this distribution also prolongs the life of the anode.
Nowadays, the entire plate is no longer made of tungsten, but consists of molybdenum and graphite to optimize heat distribution (composite anode). Only the focal spot track is still made of tungsten.
Focal Spot/Focus
Since X-rays are generated in the X-ray tube not only at one point but on a surface, the phenomenon of the penumbra occurs (◘ Fig. 2.2). On the X-ray image, the image of details becomes blurrier due to this phenomenon.

Penumbra as a function of focal size. (From Hartmann et al. 2014)
In order to reduce the area as much as possible, two tricks are used:
-
1.
By bevelling the edge of the plate, not only a more favorable change in the direction of the radiation is achieved, but also an optical reduction in the size of the focal spot, depending on the angle of the bevel.
-
2.
The tubes usually have two different sized cathode filaments, the large and the small focus. The small focus allows a higher spatial resolution, but is not as powerful.
1.1.2 The Depth Stop with Light Sighting
The depth diaphragm is mounted below the X-ray protection housing.
In the upper area of the depth stop, there are additional filters that can be moved into the beam path either manually or electronically. These filters have the same task as the filter located directly at the beam exit window. The low-energy radiation components that do not contribute to imaging are filtered out. This is also referred to as “hardening” of the radiation.
The depth diaphragm contains adjustable lead blades that block the X-rays. A distinction is made between the near-focus and near-object apertures. While the near-tube diaphragms shield the radiation that has not originated directly at the focus (extrafocal radiation), the near-object diaphragms serve to adjust the field size, i.e. the area to be examined.
In order for this field to be visible, a transmissive mirror is placed in the beam path of the X-rays, which is illuminated by a light bulb. The deflected light field is visible below the depth stop and corresponds exactly to the radiation field of the X-ray tube. The depth diaphragm is also rotatably attached to the protective housing in order to optimally adapt the field to the exposure.
An area dose meter is attached to the exit window of the depth aperture.
1.2 The X-ray Generator
The main component of a generator is the transformer.
With a single-phase generator, “gaps” in the applied tube voltage occur again and again due to the blocking of the negative voltage. Now one can convert this negative part by means of a rectifier. But even then the effective voltage is still full of gaps (two-phase generator). If a three-phase supply is chosen (this consists of three alternating voltages which are applied to the coil in a time-shifted manner), these gaps become smaller, but there is no constant voltage in the X-ray tube (three-phase or six-phase generator).
Since these fluctuations in the tube voltage deteriorate the quality of the resulting X-rays to the detriment of the patient, these generators are no longer approved for use in human medicine.
Nowadays, only so-called converter or high-frequency generators are used. In principle, the tube voltage is generated according to the same principle. By means of electronic circuits, however, a much more uniform tube voltage is achieved and can also be adapted to the characteristic curves of the tube in order to ensure an optimum yield of radiation.
1.2.1 Tube Voltage
The voltage applied between the cathode and anode is used to control the speed of the electrons and thus the energy with which these electrons hit the anode. Due to the effects mentioned above, the radiation becomes more energetic (beam quality).
Higher-energy radiation has a shorter wavelength than low-energy radiation. High-energy (or as it is called in radiology “harder”) radiation can penetrate dense structures more easily than lower-energy (“soft”) radiation.
These differences are used, for example, to make the ribs appear almost transparent on an X-ray of the thorax. This makes it easier to assess the lungs.
Since the radiation produced in the tube consists primarily of deceleration radiation, an increase in voltage does not only lead to an increase in energy. Due to the higher-energy electrons, more radiation is also produced at the lower energy spectrum. The voltage therefore has a disproportionate influence on the amount of radiation (◘ Fig. 2.3).

Radiant energy as a function of current intensity. (From Hartmann et al. 2014)
1.2.2 Tube Current
With the heating current applied to the cathode, the amount of radiation can be dosed.
A high current releases more electrons, which can migrate to the anode: thus one increases the amount of radiation (radiation quantity).
The amount of radiation is largely proportional to the current intensity (◘ Fig. 2.4).

Radiant energy as a function of voltage. (From Hartmann et al. 2014)
The tube current at the generator is usually controlled by adjusting the current-time product, i.e. the amount of charge.
1.2.3 Dose
The dose is always a mixture of tube current and voltage. If, for example, the voltage is increased for a forearm exposure, the resulting radiation can travel more easily through the bones. Thus, less radiation is needed for the X-ray image than if a radiation is selected, a large part of which “gets stuck in the bone”.
The higher the voltage, i.e. the harder the radiation, the less detail can be seen of the bone structures.
It is therefore necessary to choose the optimal mix between radiation quality and quantity for each body region.
1.2.4 Exposure Point System
If you want to set the voltage (kV) or the amount of charge (mAs) for an X-ray exposure on the X-ray generator, the first thing you notice is that this setting can only be made in certain stages. These individual steps are called exposure points (BP). The values of these steps depend on the X-ray tube and can differ from one X-ray system to another.
1.2.5 Automatic Exposure Control
A more precise setting of the dose can be achieved with the automatic exposure control.
1.3 Mapping Laws
As is known from natural light, the known laws also apply to X-rays:
1.3.1 Ray Theorem
The X-ray image is always a central projection with the focus as the center (◘ Fig. 2.5). The X-rays represent an object (G) on a projection surface (B) (film, detector). Here, the beam coming directly from the focus and located in the center of the irradiated field is called the central beam. The beam that strikes the irradiated surface perpendicularly is called the perpendicular beam.

Ray set/central projection. (From Hartmann et al. 2014)
With such a type of projection, the law of mapping applies:
In X-ray imaging, the distance g is called the focus-object distance and the distance b is called the focus-film distance (FFA). The distance B-G is called object-film distance (OFA). The variable V indicates the magnification of the image.
The greater the object-to-film distance, the larger the object is imaged, with all objects in an image plane being magnified equally.
In principle, one always wants a representation in the X-ray that is as accurate as possible in terms of size. Unfortunately, this cannot be achieved because the patient has a certain thickness. When setting the image, care is therefore taken to ensure that the region to be assessed is close to the film in order to achieve a sharp and accurate image. (Sternum in prone position, spine in supine position, …).
In some radiographs, these imaging laws are exploited. In mammography (► Chap. 3), for example, a specific region is enlarged by enlarging the OFA.
When taking a thoracic image, one would like to image the heart as accurately as possible. However, since the heart is always at a certain distance from the film, the FFA is enlarged to reduce the magnification factor (1.10 m/1.10 m − 0.20 = 1.22 → 2.0 m/2.0 m − 0.20 = 1.11).
1.3.2 Projection/Parallax
With a central projection it also happens that two objects lying on top of each other cannot be distinguished. This is particularly problematic when these objects appear in the same image size due to their size and position.
However, if the focus is now shifted in a plane, the object in the image plane also shifts (parallax shift, ◘ Fig. 2.6). In this way, objects can be “free projected” in an X-ray image, i.e. the objects that were previously displayed on top of each other are then displayed next to each other.

Projection at parallax shift. (From Hartmann et al. 2014)
1.3.3 Distortion
Since an X-ray image is a projection, it is unfortunately the case that objects are only displayed in their full extent if they are perpendicular to the central beam. If the object is not perpendicular, it will be displayed foreshortened. If it is not in the central beam, the size representation also changes (◘ Fig. 2.7).

Projection under distortion. (From Hartmann et al. 2014)
1.3.4 Law of Distance Squared
One of the most important physical laws in radiology is the distance-squared law. It states that as the distance (r) increases, the dose/intensity (I) decreases squared.
This law is of particular importance in the field of radiation protection.
1.4 Quality of the X-ray Image and Quality Improvement Measures
1.4.1 The Good X-ray Image
What makes an X-ray image a good X-ray image? Regardless of the body region to be examined and the structures to be depicted, the image should have homogeneous, sufficient exposure and good contrast.
An image is homogeneously exposed when the average blackening corresponds to a medium grey tone, i.e. when bright and dark areas in the image can be recognized evenly. Only in this way can the complete grey spectrum be used for display. It is therefore important to select the tube current, the exposure time and the quality of the radiation (tube voltage, kV) optimally.
For the representation of structures you need a sufficiently high contrast between the details.
The harder the radiation, the easier it is to penetrate dense structures, which can lead to these differences in density being displayed with similar brightness. The mnemonic “kV makes gray” describes exactly this fact: that at high kV values the image consists of relatively equal shades of gray.
Another quality feature of a good X-ray image is the sharp representation of the structures.
1.4.2 Motion Blur
Although X-ray diagnostics work with relatively short exposure times, motion blur can occur in the image. Good patient care can already improve the quality of the image by actively ensuring that the patient maintains a calm and constant posture/position during the exposure. Sometimes it is advantageous to perform an X-ray exposure lying down rather than sitting down, as the patient can be positioned more stably and unconscious movements can be avoided.
The well-known breathing command of radiology: “Breathe in, breathe no more!” serves to minimize movement. Thus, not only the optimal position of the lungs is ensured during lung inhalation, but of course also the movement of the lungs is reduced.
In some images, on the other hand, one takes advantage of the motion blur. When taking an image of the cervical spine from the front, the lower jaw would cover the vertebral bodies. By moving the lower jaw quickly (“jaw flap”), it is possible to partially prevent this overlapping by “blurring” the lower jaw on the image.
1.4.3 Scattered Beam Reduction
In an X-ray image, not only the direct radiation that passes through the body contributes to the imaging, but also the radiation scattered in the body. This scattered radiation causes the structures in the image to no longer be clearly displayed. In order to improve the image quality, this scattered radiation should therefore not hit the detector.
The amount of scattered radiation is directly dependent on the tube voltage, the patient thickness and the field size.
1.4.4 Image Noise in Digital X-ray Images
The advantage of a digital X-ray image is that almost every X-ray image results in a usable image due to the high sensitivity of the digital sensor technology. This technology is much less sensitive to deviation in the amount of radiation than the “old” X-ray film. While overexposure, i.e. too much radiation, does not harm the quality of the image, underexposure results in an image that shows much less detail. This phenomenon is also called image noise.
This noise is not always immediately visible on the preview monitors of the X-ray systems. For this purpose, the dose indicator exists in digital imaging technology, which, however, was developed by each manufacturer itself and therefore cannot be transferred from one system to another.
1.5 Setting Up a Bucky Workstation
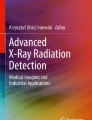
The conventional X-ray workstation is often called the Bucky workstation (◘ Fig. 2.8). Dr. Gustav Peter Bucky was, among other things, a radiologist and developed the principle of the “floating” table top and the scattered radiation grid.

Example of a Bucky workstation (table and grid wall stand)
1.5.1 Bucky Table
The table on which the patient lies during the examination is called a bucky table. The special feature of this table is that the table top can be moved in all directions.
1.5.2 Grid Wall Stand
The grid wall stand is primarily used for recording while standing or sitting. Here, the height-adjustable grid drawer is located behind a plate.
1.5.3 Tripod
The X-ray tube or, more precisely, the X-ray protection housing with depth diaphragm is often located on a so-called ceiling pendant. The ceiling pendant consists of two vertical rail systems attached to the ceiling, to which a telescopic arm is attached.
1.6 Mobile X-ray Equipment
Mobile X-ray units are used in the intensive care unit or in the operating theatre. Generator and tube are mounted on a mobile unit. Through the use of converter generators, these units have become smaller and can be operated with a normal mains voltage or even battery.
1.7 Special Radiation Protection Measures
1.7.1 Direct Radiation Protection
Shielding
When an X-ray is taken, the patient must of course be exposed to the X-rays. However, if possible, all parts of the body that are not being examined should be shielded from the radiation. Most aids for this purpose are made of lead or lead compounds (“lead rubber”). Depending on the organ being examined, the patient can be protected in various ways. In particular, the organs that are sensitive to radiation should be protected. First of all, these are the gonads, i.e. the ovaries in women and the testes in men. But also the small intestine and the hematopoietic tissue are particularly sensitive to radiation.
Since many cells in children are still growing, children are generally more sensitive to radiation than adults and therefore require special protection.
When exposing the extremities, the patient should ideally always wear a lead apron or a lead gown. Infants can also be completely wrapped in so-called radiation protection wraps.
When exposing the chest area, a half apron (gonad protection apron) or a radiation protection skirt must always be worn to protect the lower half of the body from radiation.
For exposures of the pelvis or hip, you can no longer put on a half-gun, as this would cover the bone. There are special lead covers for these exposures, depending on gender.
In male patients, the guidelines of the German Medical Association prescribe (in the case of gonadal admission) that the testicles are protected by a testicular capsule) which completely encloses the testicles.
For women, a so-called ovarian protection should be used, which can be applied either indirectly or directly. The indirect protection is attached with a splint or a magnetic holding system below the depth diaphragm and placed by means of the light visor in such a way that the ovaries are covered in the lower pelvic region. The direct ovarian shield is placed on the patient’s lower abdomen. For images while standing, this can be fixed by means of a belt.
During the X-ray exposure, all persons except the patient should leave the room. In addition, the doors of the examination room should also be closed in order to shield against possible stray radiation. If a person is required to hold the patient during the X-ray exposure, this person should always be protected with a radiation protection apron. In pediatric radiology, there are additional special radiation protection walls made of lead or lead glass for the person holding the patient during standing radiographs.
Insertion
One of the most effective methods of minimizing X-ray radiation is to fade in the radiation field.
The smaller the irradiated field, the less dose reaches the patient and the less scattered radiation is produced in the patient.
This means that the overlay not only protects the patient, but also provides a better quality X-ray image.
Additional Filters/Compensating Filters
Filters were mentioned at the beginning of this chapter. These also contribute to the radiation protection of the patient. The filters in the depth diaphragm harden the rays so that the radiation that does not contribute to image formation does not reach the patient in the first place.
Radiation Quality
The dose for the patient can also be minimized by changing the radiation quality. Whereas a few years ago, for example, the fingers were X-rayed with a voltage of 44 kV, the Medical Association now prescribes a voltage of at least 50 kV. This makes it easier for the rays to pass through the bones and the current intensity can be reduced. With the introduction of digital imaging techniques, the lower contrast resulting from the higher voltage can be increased by suitable image processing.
1.7.2 Indirect Radiation Protection
Before taking an X-ray, i.e. emitting radiation, it is important to check the preconditions for this.
It should always be checked whether an X-ray of the same region has already been taken beforehand. In this way, any unnecessary duplicate examinations can be avoided.
Viewing the preliminary images is also very important because this is the only way to select the correct imaging technique. For patients with hip prostheses, it may be necessary to select a different cassette format for the hip images in order to be able to image the complete prosthesis.
Radiation protection also includes avoiding erroneous images. The applied radiation should always result in a meaningful, diagnostic image. Therefore, careful and concentrated work is important in radiology. Thanks to digital imaging, the number of false exposures has decreased, but these are also possible here, for example, due to incorrect setting technique or too low a dose.
According to the X-ray Ordinance, the justifying indication, i.e. the reason for this examination, must be carefully examined before each examination. Particularly in the case of children, it must be considered whether an X-ray image must be taken or whether other examination methods such as an ultrasound would be sufficient to answer the question.
2 Digital Image Processing
One of the greatest advantages of digital radiography is the linear sensitivity of the imaging plate and solid-state detector. This means that there are virtually no more false exposures, as good imaging can be achieved with the digital systems even with too little or too much radiation. However, there is a small limitation in the lower dose range. If too little image information (in the form of light pulses) is available, a noisy image is produced.
Digital images also offer the possibility of processing them after they have been taken. In the following chapter, you will learn about some of these options.
2.1 Matrix
A digital image consists of many individual pixels. These are arranged in rows and columns, this arrangement is then called a pixel matrix or matrix for short (◘ Fig. 2.9). Depending on the system, an X-ray image consists of between 1024 × 1024 and 4096 × 4096 pixels. One speaks of a 1024 pixel matrix or a 4096 pixel matrix.

a–d Examples of different image matrices. (From Hartmann et al. 2014)
The larger this matrix is for the same image size, the more accurate the image representation.
2.2 Color Depth
A specific color is stored for each pixel. This color information depends on the so-called color depth of the image. If only the information 1 (white) or 0 (black) is stored for each pixel of an image, the color depth is said to be one bit (◘ Fig. 2.10). However, since the X-ray image does not only consist of black or white, but of different shades of gray, each pixel is described with a certain value, which describes the gray value between black and white.

Examples of the different color depths. (From Hartmann et al. 2014)
With a color depth of 1 bit, only two color values, black and white, can be displayed (21 = 2 colors), with a color depth of 2 bits, four colors can be stored (22 = 4), and so on. The image that is created at the detector has a color depth of 14 bits, i.e. it contains 16,384 gray values.
2.3 Error Correction
As soon as you take a digital X-ray image, it is processed by the acquisition system itself in the first step. The so-called raw image is analyzed directly by the acquisition system. First, image errors are corrected, i.e. pixels that do not “fit” the environment due to detector errors or measurement errors are replaced by the average value of the surrounding pixels. Such mismatched pixels can be those that are permanently interpreted as black or white, but also pixels that do not respond to radiation as efficiently as those surrounding them. These errors can be detected during the calibration of the system. The result of this calculation is called a “pre-processed image”.
The next processing step is a so-called histogram analysis. Here, the brightness distribution of the complete image is analyzed. The software used is precisely adapted to the type of detector used and cannot simply be exchanged. The histogram analysis makes it possible to detect direct radiation and scattered radiation and to use this information to improve the contrast of the image accordingly.
Practice Questions
-
1.
Name the main technical components of an X-ray system.
-
2.
What is meant by “image noise”?
-
3.
What is the law of mapping?
-
4.
Which measures count as direct radiation protection?
-
5.
What is a matrix?
Solutions ► Chap. 27
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2023 Springer-Verlag GmbH Germany, part of Springer Nature
About this chapter

Cite this chapter
Vockelmann, C. (2023). Conventional X-ray Diagnostics. In: Kahl-Scholz, M., Vockelmann, C. (eds) Basic Knowledge Radiology. Springer, Berlin, Heidelberg. https://doi.org/10.1007/978-3-662-66351-6_2
Download citation
DOI: https://doi.org/10.1007/978-3-662-66351-6_2
Published:
Publisher Name: Springer, Berlin, Heidelberg
Print ISBN: 978-3-662-66350-9
Online ISBN: 978-3-662-66351-6
eBook Packages: MedicineMedicine (R0)