
Abstract
Guidelines for vital molar therapy are presented based on best available evidence. Often the cause for vital intervention is due to caries, but seldom the depth of the carious lesion is mentioned in literature, which may hamper the evaluation of prognosis following treatment. Moreover, the lack of devices for monitoring objectively the degree of pulp inflammation makes the topic a clinical challenge where proper tooth selection is important. In this chapter, the deep and extremely deep caries lesion is defined and linked to specific treatment protocols, which include both direct pulp as well as indirect pulp capping procedures. Particularly, a classification of the pulp capping procedure is described, which relates to two specific scenarios. In Class I the need for pulp capping arises by accident, while in Class II the capping procedure is expected and the set-up for the vital pulp therapy includes the use of the operating microscope.
Access provided by CONRICYT-eBooks. Download chapter PDF
Similar content being viewed by others

Keywords
- Caries
- Indirect pulp capping
- Inflammation
- Pulp
- Pulp capping
- Pulpotomy
- Revascularization
- Stepwise excavation
Bjørndal L, Thylstrup A. A practice-based study on stepwise excavation of deep carious lesions in permanent teeth: a 1-year follow-up study. Comm Dent Oral Epidemiol. 1998;26:122–8.
This practice-based study followed teeth with deep caries, in which clinicians suspected a pulp exposure if excavated to the fullest extent. The high success rate of teeth surviving the final treatment without pulp exposure after 1 year of observation shows that it was possible for dentists in general practice to administer and manage the treatment of deep carious lesions, a process which may prolong tooth survival compared with conventional endodontic techniques.
4.1 Introduction
The management of deep caries is a daily issue in endodontic practice. For caries in the pulpal quarter of the dentin, high-level evidence data have shown that a stepwise excavation approach led to a significant decrease in the number of pulp exposures as opposed to complete excavation.
Before performing vital pulp therapy in a molar, clinicians will have to answer two questions: (A) How invasive a treatment needs to be in fulfilling the aims of preserving and maintaining the pulp tissue in a healthy clinical condition, and (B) whether the chosen modality is a permanent or temporary treatment solution. Both topics depend upon the cause and time of the injury: is the pulp exposed as a result of trauma or through caries? What is the aim of performing vital pulp therapy and when could a pulp exposure particularly in carious teeth be avoided, by changing toward an indirect pulp therapy approach?
The controversy about caries and the pulp goes back more than a century [1, 2], and represents a problem of deciding the right treatment in dentistry. G.V. Black wrote in his textbook: “…it will often be a question whether or not the pulp will be exposed when all decayed dentine overlaying the pulp is removed…and It is better to expose the pulp of a tooth than to leave it covered only with softened dentine” [1], whereas Sir John Tomes wrote decades before [2]: ……. “It is better that a layer of discolored dentine should be allowed to remain for the protection of the pulp rather than run the risk of sacrificing the tooth.”
Even today the same deep caries scenario may be interpreted and treated differently by clinicians [3–5]. The caries and pulp dilemma is partly due to the lack of a noninvasive diagnostic device for monitoring degrees of inflammation in the pulp [6], as well as a low level of scientific evidence addressing the best treatment [7–9]. Finally, the exact definition of deep caries is unclear, when outcomes of vital pulp therapy are reported. In this chapter we define radiographically deep caries as being within the inner quarter of the pulp and extremely deep if penetrating the entire thickness of the dentin (Fig. 4.1).

The radiographic presentations are shown of a deep caries lesion versus an extremely deep lesion. (a) The deep lesion involves the pulpal quarter with a radiodense zone separating the translucent zone from the pulp. (b) The extremely deep lesion defines a penetration that involves the entire primary/secondary dentin, either with no radiodense zone separating the demineralized dentin from the pulp or with a radiodense zone located within the pulp chamber indicative of tertiary dentin
A pulp exposure is defined relatively broadly being the result of a pathological change in the hard tissue of a tooth caused by caries, a mechanical factor, or trauma [10]. Here, a classification of pulp capping procedures is introduced separating two scenarios: direct pulp capping Class I (pulp exposure has been made accidently) and direct pulp capping Class II (pulp exposure is expected, as part of caries excavation and while using a microscope). This chapter aims to align updated treatment guidelines on best clinical evidence for vital pulp therapy in molars including the indirect pulp therapy approach.
4.2 The Benefit of Having a Vital Pulp
4.2.1 Apexogenesis
In injured teeth with incomplete root formation, it is essential to keep a vital pulp for the final formation and completion of the root complex, described as apexogenesis. Much focus has been given in the past to this topic [11], because the tooth has a better prognosis, if the roots are fully matured. Some of the problems associated with incomplete root formation of teeth after pulpal necrosis are briefly listed in Box 4.1 but also discussed in Chap. 7 of this book.
Box 4.1. Vital Pulp Therapy Aims at Apexogenesis for the Prevention of the Following
-
An open apex (a challenge to create a stop and establish a good seal)
-
Thin dentinal walls (more prone to fracture)
-
The incomplete apical development (in general making instrumentation and sealing more difficult)
-
Root fracture
4.2.2 Tertiary Dentinogenesis
The stimulation of tertiary dentinogenesis is a main objective of the vital pulp therapy. The classification and definition of tertiary dentin has in the past been described by many synonyms [12, 13]; here, it is presented in the context of dentinogenesis in general (Box 4.2). Tertiary dentin defines new hard tissue produced in relation to an external injury [14]. The subdivision of tertiary dentin into reactionary dentinogenesis and reparative dentinogenesis introduces a biological platform with more emphasis at the cellular origin [15, 16], as well as causes for the upregulation of the aged odontoblast secretion [17–19]. The reactionary dentin can be interpreted as the elevated growth of dentinogenesis, related to early caries lesions [20], and the odontoblast cells are stimulated by dentin matrix proteins released during caries demineralization [21, 22]. These upregulated primary odontoblast cells [18] are involved directly, but also a mixture with new beginners of secondary odontoblast-like cells can be observed in natural caries development [23]. In case of a pulp exposure, a complete new dentin formation leads to the reestablishment of a dentinal bridge formation, defined as reparative dentinogenesis (Box 4.2). Initially, it is composed by a layer of atubular mineralized matrix, described as fibrodentin [14], followed by a tubular dentin formation, presumably laid down by new secondary odontoblast-like cells.
Box 4.2. Classification of Dentinogenesis
-
Primary dentinogenesis: dentin produced before the tooth erupts
-
Secondary dentinogenesis: dentin physiologically produced after the tooth has erupted, eventually reducing the size of the pulp cavity
-
Tertiary dentinogenesis, dentin produced as a response to external stimuli and can be further divided into:
-
Reactionary dentin (new tubular dentin):
-
(a)
Produced by upregulated odontoblasts or a mixture of these odontoblast cells and new secondary odontoblast-like cells
-
(a)
-
Reparative dentin (two layers of hard tissue = dentinal bridge):
-
(a)
Initially a layer of atubular dentin = fibrodentin (nonodontoblast origin)
-
(b)
Followed by a layer of tubular dentin produced by new secondary odontoblast-like cells
-
(a)
-
A significant portion of the dental literature has been dealing with the study of a newly formed hard tissue barrier and the status of the pulp after vital pulp therapy. A simple parameter for examining new pulp-protective agents has been to confirm whether or not tertiary dentin is present following pulp therapy. A recent systematic review has argued [24] that these microscopic analyses of histological sections on newly formed hard tissue may be considered a surrogate endpoint, which is difficult to interpret in the clinic. Future hard tissue studies following vital pulp therapy should analyze in more detail how well newly formed tertiary dentin reacts as a barrier, in order to avoid late invasion of microorganisms, and what is the structural integrity of newly formed hard tissue.
The formation of reparative dentin might be beneficial in terms of blocking potential bacteria from invading the pulp due to the atubular interface, as opposed to the structure of the primary tubular dentin. However, it should be remembered that the reparative dentin might contain more organic material and be less mineralized than primary dentin. The more organic material the dentin comprises, the more permeable it will be, and therefore the reparative dentin represents an inferior type of dentin as compared to primary dentin [12]. Also it is important to note that reparative dentin with or without so-called tunnel defects, cannot keep away the bacterial invasion from untreated progressing caries and/or a leaking coronal restoration. The optimal endpoint for evaluating vital pulp therapy would be to determine the long-term clinical outcome of the pulp, i.e., function, healthy state, and capacity of preventing a secondary infection [24].
4.2.3 Inflammation and Tertiary Dentin
Most experimental studies on pulp capping and protective agents have been carried out in healthy teeth, which in reality makes it difficult to transform information into the clinical situation, where the exposed pulp most often is expected to be associated with various grades of inflammation. Severity of pulp inflammation may influence tertiary dentin. At the extreme, inflammation will lead to pulp necrosis, hence stop or even absence of any tertiary dentinogenesis. In contrast, milder degrees of pulp inflammation may seem beneficial for tertiary dentinogenesis [25]. Taken together, some treatment principles can be aligned for the vital pulp therapy promoting apexogenesis and tertiary dentinogenesis (Box 4.3).
Box 4.3. General Principles for Vital Pulp Therapy
-
Removal of (i) bacterial infected dentin and (ii) clinically judged inflamed pulp tissue
-
The application of a pulp protective agent stimulating reparative dentinogenesis
-
To secure apexogenesis by the vital radicular pulp tissue
-
Performance of a coronal seal for preventing secondary infection of the reparative dentin and hence the development of infected pulp necrosis associated with apical periodontitis
4.3 Clinical Evaluation of Inflammation
Before the principles of vital pulp therapy are laid out, it is important to recall that a precise clinical diagnosis of the degree of inflammation in the pulp is not possible [3]. Little or no correlation exits between the histological findings of pulp pathosis and clinical symptoms [26–28]. Moreover, in a clinical setting a diagnostic device is not yet available for objectively measuring a threshold of reversible pulp inflammation being beneficial or not for tertiary dentinogenesis. The diagnoses are based on interpretation of data from the pretreatment examination, the clinical examination, as well as the radiographic examination [29], rather than histopathological findings. Clinical data are shown for case selection that divide the condition of the pulp into so-called reversible pulpitis and irreversible pulpitis (Box 4.4).
Box 4.4. Reversible and Irreversible Pulpitis
-
Reversible pulpitis:
-
A clinical diagnosis – based of the evaluation of subjective, clinical, and radiographic findings.
-
Suggest that if the external stimuli are removed the pulp will return asymptomatic and vital after long term evaluation.
-
Thermal changes (air, liquid) may produce a sharp transient pain.
-
In case of pulp exposure hemostasis can be obtained.
-
The diagnosis does not indicate the precise histological status of the pulp.
-
-
Irreversible pulpitis:
-
It is a clinical diagnosis associated with subjective and objective findings indicating presence of pain (spontaneous and or prolonged unbearable pain/disturbed night sleep).
-
Temperature changes may produce lingering pain.
-
In case of pulp exposure hemostasis cannot be obtained.
-
The diagnosis does not indicate the precise histological status of the pulp.
-
Figure 4.2 shows a clinical example of an extremely deep caries lesion with direct exposure of the pulp prior to excavation. The patient arrived to the dental office with prolonged pain and disturbed night sleep. The clinical diagnosis “irreversible pulpitis” is further confirmed by the color of the blood being dark red. In this case also pus is apparent associated with a frank cavitation, and hemostasis is not possible to achieve, and root canal treatment is initiated.

(a) Preoperative periapical radiograph showing extremely deep caries lesion in the mandibular second molar with apical periodontitis. (b) Tooth shown before treatment. Clinically the tooth is vital and the combined diagnosis is “irreversible pulpitis” and apical periodontitis. (c) Following excavation an exposure of the pulp is present with pus. (d) During further access to the pulp cavity focal areas of pus are noted within the bleeding inflamed pulp. (e) Complete excavation performed before placement of “endodontic working” restoration and preparation of an aseptic working field. (f) Root canal treatment is initiated and determination of working length is about to be accomplished
4.4 Indications and Treatment Concepts for Vital Pulp Therapy
The principal indications for performing vital pulp therapy are carious lesions, mechanical iatrogenic injury, and trauma. In the context of molar endodontics, the most frequent cause for endodontic treatment including vital pulp therapy has, in the general practice environment, been caries [30]. Therefore, the aligned treatment guidelines are described within the “scenario” of a carious pulp exposure. From the literature, it is often unclear whether the clinicians are creating a pulp exposure by accident or whether it is the intention to do a pulp exposure; moreover the depth of the carious pulp exposures are seldom defined in clinical studies [31]. The following vital pulp therapy guidelines will include these aspects.
4.4.1 Direct Pulp Capping Class I (Accidental Pulp Exposure)
No additional enlargement is made of the exposed pulp. Typically, the exposure has just occurred following a trauma or an accidental perforation during a preparation procedure (Fig. 4.3). It is a prerequisite that the pulp is healthy. Clinically, this means that the pulp is vital and the patient is without subjective pain prior to treatment, and hemostasis can be expected. The exposure of the pulp is less than 1 mm in diameter and should be located in the coronal third, but preferable in relation to a pulp horn. The pulp protective agent can be placed directly at the pulp exposure and the cavity can be sealed efficiently. It may also take place during excavation of caries, but in an area not directly related to the carious dentin, because the pulp exposure has been made by accident.

(Left) Direct pulp capping Class I: an accidental pulp exposure has occurred during preparation. No additional enlargement is carried out. (Middle) The cavity is irrigated with saline. (Right) Calcium hydroxide capping material is placed prior to permanent restoration
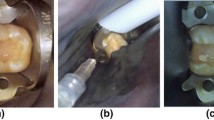
4.4.2 Direct Pulp Capping Class II (Intentional Pulp Exposure)
This modality includes the mandatory use of an operating microscope during caries excavation [32]. The potential implementation of carious dentin into the pulp during excavation can better be limited by the use of magnification. If hemostasis can be achieved it should be seen as the clinical interpretation of an acceptable and treatable pulp, but the exact extent of pulp inflammation is currently impossible to predict objectively in the clinical setting. No global consensus is available for this approach, and it may be argued that a pulp exposure shall be avoided by an indirect pulp therapy where less invasive excavation procedures are introduced (see below).
It has been shown in cases with deep or extremely deep caries that if the bacterial invasion zone penetrates the pulp close to reparative dentin, the subjacent pulp is severely inflamed [33], making both vital and indirect pulp therapy unpredictable treatment options. When irreversible inflammation in the pulp is present, hemostasis is typically not possible to obtain; therefore pulp capping is contraindicated in deep or extremely deep caries. However, when hemostasis can be controlled, such lesion depths may be successfully treated (Fig. 4.4). The result of apexogenesis following treatment of a deep carious lesion is shown in (Fig. 4.5).

(Left) Preoperative radiograph of a 12-year-old child showing first mandibular molar with extremely deep caries. (Middle) After excavation and carious exposure and MTA application. (Right): Postoperative 1-year follow-up. Tooth vitality present and well-defined lamina dura in the apical region. Note the formation of tertiary dentin (Courtesy of Dr. G. Bogen)

(a) Preoperative radiograph of a 7-year old child, showing first mandibular molar with deep caries. (b) After excavation and carious exposure and MTA application. (c) Postoperative 3-year follow-up. Tooth vitality present and completed root formation (Courtesy of Dr. G. Bogen)
4.4.3 “Partial” Pulpotomy
As opposed to direct pulp capping, an additional removal of suspected inflamed pulp tissue is performed, and for providing a better seal of the pulp protecting agent, which may be a problem with complicated crown fractures [34]. The definition between a direct pulp cap procedure Class II and the partial pulpotomy appears to overlap in carious pulp exposures. In particular where the treatment is carried out under the conditions of “reversible pulpitis” [35–37], the argumentation of avoiding pulp exposure in the first place is in principle the same as indicated for direct pulp capping Class II. In contrast, a “several-day-trauma” tooth with exposed pulp represents the classical indication for this treatment modality, where the tissue is expected to be superficially and inflamed. In this situation, a superficial removal of pulp tissue is highly beneficial [34]. The completion of an incomplete root complex is shown following a partial pulpotomy (Fig. 4.6).

(a) Preoperative periapical radiograph showing deep carious lesion in the mandibular first molar. (b) Postoperative radiograph taken immediately after treatment with partial pulpotomy and MTA. (c) Tooth: 16 months after treatment. Notice dentine bridge formation in the mesial side of the tooth (arrow). (d) Tooth: 26 months after treatment. Notice the well-formed dentinal bridge (arrow) and the physiological continuation of root formation (Reprinted from Barrieshi-Nusair and Qudeimat [37]; with permission)
4.4.4 “Full” Pulpotomy
In single rooted teeth, the definition includes the surgical amputation of the coronal portion of an exposed pulp, whereas in molar it covers the removal of the entire pulp tissue in the pulp chamber down to the orifices (1–2 mm into in the root canals). The rationale is to completely remove the inflamed pulp tissue. As the prognosis of the vital pulpectomy is very high (see Chap. 8) why then attempt a “full” pulpotomy?
In children it seems advisable to try a conservative pulp-preserving procedure, even in deeply carious permanent teeth with signs of “irreversible pulpitis,” whereby ideal conditions can be established, as already discussed the loss of the vital pulp function is so devastating in teeth with immature apices (Box 4.1). If failure then occurs, apexification or regenerative techniques can still be options. It has been speculated that a full pulpotomy could be a more permanent treatment option in cases of “irreversible pulpitis,” but with established hemostasis, but only case series and case report are available [38, 39].
4.4.5 “Emergency” Pulpotomy
Often “emergency” treatments are closely associated with the practical aspect of lacking time, as the patient arrives unexpected to the dental office and being in acute pain. Thus, a simple treatment is urgently needed to reduce the level of pain in the first place and then a treatment session can be scheduled for completing the final pulpectomy, when proper time is available. An “emergency” pulpotomy has shown to be able to reduce pain in relation to acute “irreversible pulpitis” and without the need of additional medicaments [40]. It is a temporary treatment, but with the surgical pulp approach being the same as the “full” pulpotomy, except for the temporary seal.
4.5 Brief Comments on Capping Agents
For decades the capping agent to promote healing and maintaining viability of the remaining pulp tissue has been a calcium hydroxide-containing material applied either as a base or as a liner. Within the last 20 years, calcium silicate-containing materials have gained more and more focus. In particularly, MTA (mineral trioxide aggregate, Dentsply Tulsa Dental, OK, USA) has been investigated and used intensively. More recently other bioceramic cements have been introduced such as Biodentine (Septodont, Saint Maur des Fosses, France) or iRoot BP (Innovative BioCeramix, Vancouver, BC, Canada). Only limited clinical information is actually available to show potential clinical differences. The reason for selecting the silicate containing materials is therefore based mainly on laboratory studies, where it is shown that these materials may create a better quality of the hard tissue laid down, without so-called tunnel defects. Interestingly, a recent randomized clinical trial [41] showed no differences between the two classic pulp agents, i.e., the calcium hydroxide containing liner Dycal (DeTrey Dentsply, Skarpnäck, Sweden) and MTA. This may also underline that other variables such as patient age and irreversible pulp inflammation may determine the prognosis accounting for problems leading to failure or not. Finally, larger studies may be needed to show actual differences, when it comes to the choice of the very best pulp agent.
4.6 Treatment Guidelines for Vital Pulp Therapy in Molars
4.6.1 Direct Pulp Capping Class I
4.6.1.1 Pretreatment Data
-
Patient information: subjective evaluation of the region having the present symptom by questioning the patient on the area in focus, intensity, duration, stimulus, relief, and spontaneity. Absence of any signs of “irreversible pulpitis” is mandatory to permit direct pulp capping (Box 4.4).
-
Objective extraoral examination as well as examination of the intraoral soft and hard tissues.
-
Clinical examination showing a tooth that is vital with no lingering or persistent prolonged pain following thermal testing. Other tests such as palpation, percussion, and mobility should have negative findings.
-
Radiographic examination: radiographs showing the involved tooth, furcation, periapical area, and the surrounding bone. No apical pathosis is present.
4.6.1.2 Diagnosis
-
Reversible pulpitis
4.6.1.3 Treatment Protocol
-
The tooth is isolated with rubber dam (mandatory for all types of vital pulp therapy).
-
The cavity and the pulp exposure area are gently flushed with saline in order to remove detritus and to establish a clean nonbleeding pulp wound.
-
Direct flush at the exposure should be avoided.
-
Firm pressure with a cotton pellet should be avoided as the removal tends to reactivate bleeding.
-
Hemostasis should be reached within 5 min.
-
The site of the perforation should be noted in the file of the patient for the future plan of restoration.
-
Pulp capping agent is applied at the exposure site and in contact with the tissue (e.g., calcium hydroxide containing base material or mineral-trioxide aggregate (MTA)) followed by a layer of glass-ionomer (Ketac Molar; 3 M ESPE, Glostrup, Demark))
-
A permanent restoration is placed immediately or within a few days in order to prevent secondary bacterial infection.
-
After 6 months, the tooth is checked with respect to subjective symptoms and tooth vitality; in case of absence of any response, a radiographic examination is performed to diagnose potential apical pathosis.
4.6.1.4 Contraindications
-
If hemostasis is not achieved, direct pulp capping is not done and pulpectomy is indicated (see Chap. 6)
-
Direct pulp capping (Class I) should not be carried out in deep or extremely deep caries in adults (Fig. 4.1).
4.6.2 Direct Pulp Capping “Class II” and “Partial Pulpotomy”
4.6.2.1 Pretreatment Data
-
Patient information: Absence of any signs of “irreversible pulpitis” is mandatory (Box 4.4)
-
Objective extraoral examination as well as examination of the intraoral soft and hard tissues
-
The tooth is vital (e.g., bleeding is observed from the exposure site), no lingering or persistent prolonged pain is found following thermal testing (this may, however, be difficult to ascertain in children)
-
Radiographic examination; radiographs showing the involved tooth, furcation, periapical area, and the surrounding bone. No apical or furcal pathosis are present.
4.6.2.2 Diagnosis
-
Reversible pulpitis
4.6.2.3 Treatment Protocol
All the steps are followed as described for adults. However, note additional details are mandatory for vital pulp therapy for the extremely deep caries lesion [32]:
-
Excavation is carried out under the operating microscope and aided by the use of caries detector solution.
-
Hemostasis is established within 5 min. following the use of 5.25 % sodium hypochlorite.
-
No specific rules about the size of the perforation which means that it is not a matter of choosing a “direct pulp capping,” “partial,” or even “full” pulpotomy; it is related to the fact whether or not hemostasis can be obtained.
-
In case hemostasis is not occurring, the “partial” pulpotomy procedure is applied, which means that a 1.5–2 mm deep preparation is made with a sterile diamond bur in a high speed hand piece under water spray.
-
When hemostasis is obtained, MTA is applied in a thickness of 4–5 mm (mixed according to the manufacture’s prescriptions; however, as dry as possible).
-
Place moist cotton pellet over MTA followed by a solid interim restoration (composite or glass-ionomer cement, e.g., Ketac Molar; (3 M ESPE, Glostrup, Demark)).
-
-
After 1 week (or at least 2 days) the temporary restoration and the cotton pellet is removed for controlling a proper hardening of the capping agent, followed by a permanent restoration.
-
Notably, the treatments have primarily been examined in children and even though the caries has been extremely deep the clinical diagnosis has been “reversible pulpitis” [32].
4.6.2.4 Contraindications
-
If hemostasis cannot be achieved, direct pulp capping is omitted and pulpectomy is indicated (see Chap. 6).
-
Without the use of the operating microscope it is not a so-called Class II modality.
4.6.3 “Full” Pulpotomy for Children and Adolescents
4.6.3.1 Pretreatment Data
-
Patient information: No signs of “irreversible pulpitis” is first choice; however in case of incomplete root formation, signs of “irreversible pulpitis” should be a candidate for a “full” pulpotomy procedure.
-
Objective extraoral examination as well as examination of the intraoral soft and hard tissues.
-
Clinical examination: The tooth is vital (bleeding point from pulp exposure/fracture line), no lingering or persistent prolonged pain following thermal testing. This may be very difficult to do in children. In case of signs of “irreversible pulpitis,” the aspect of whether or not hemostasis can be obtained need to be confirmed clinically.
-
Radiographic examination; radiographs showing the involved tooth, furcation, periapical area, and the surrounding bone. No apical or furcal pathosis is present.
4.6.3.2 Diagnosis
-
Reversible pulpitis
OR
-
Irreversible pulpitis and based on careful case selection
4.6.3.3 Treatment Protocol
-
All pulp tissue is removed from the pulp chamber.
-
The amputation area should be at the orifice (1.5–2 mm into the root canal) and eventually made with a sterile diamond bur in a high speed hand piece under water spray.
-
Radicular pulp tissue is examined for hemostasis.
-
A pulp capping material is placed, typically calcium hydroxide (DeTrey Dentsply, Skarpnäck, Sweden) or MTA.
-
The blunt end of a paper point may be used to ensure that the capping material is proper placed. Seal the preparation including the entire pulp chamber in a thickness of 4–5 mm MTA.
-
After 1 week (or at least 2 days), the temporary restoration and the cotton pellet are removed for controlling a proper hardening of the capping agent, followed by a permanent restoration.
-
A practical approach has been to place a permanent restoration at once.
-
If the patient presents with signs of “irreversible pulpitis,” but hemostasis can be successfully accomplished, an MTA pulpotomy procedure may be considered as an alternative treatment [39, 40]. In such cases it is recommended that the patient receive a relatively short follow-up visit within the following 2 days to assess subjective symptoms. Concomitantly, an assessment of MTA setting may be performed followed by a permanent restoration.
4.6.3.4 Contraindications
-
If hemostasis is not achieved, pulpectomy is indicated (Chap. 6).
4.6.4 Indications for Indirect Pulp Therapy
In relation to deep caries the decision to treat the pulp indirectly may be considered. An indirect pulp therapy addresses the excavation of deep dentin aiming to avoid pulp exposure. The therapy may be performed either in one or two treatment sessions.
Much research during the past decades has modified the original concept of a pulp close excavation during the indirect pulp therapy [42]. For example, Kerkhove et al. [43] described it as leaving only residual caries, meaning that if a further limited excavation was carried out, a pulp exposure would be present. Other studies have introduced less invasive and partial excavation procedures leaving more carious dentin behind permanently and with an apparent good prognosis, primarily in children [44–46]; therefore the original invasive concept of indirect pulp therapy appears outdated.
4.6.5 Stepwise Exaction (2-Step Approach)
The concept of performing two treatment sessions is also described as a stepwise excavation. The focus of the first treatment/excavation appointment is not to reach residual caries close to the pulp, as the risk of exposure of the pulp increases the closer the excavation is performed [47, 48]. In contrast, the aim of the first treatment is to change the active cariogenic environment. The consequence of leaving carious dentin temporarily subjacent to a so-called treatment restoration is that the clinical features of carious dentin will change to that of slowly progressing or arrested caries [49, 50]. The active deep carious environment can clinically be recognized as a soft discolored and wet tissue, which may change towards a darker harder and drier appearance of the carious dentin. Clinically, a second and final excavation of arrested carious dentin will be easier to accomplish without risking a pulp exposure.
High-level evidence data have shown that a stepwise excavation approach led to a significant decrease in the number of pulp exposures as opposed to complete excavation [51, 52]. This approach may be carried out within a practice-based environment even with the concept of two visits [53]. Within communities where it would be difficult to receive the patient for an additional appointment, a one-step partial caries removal approach might be the treatment of choice; however the evidence behind is lower [47].
4.6.6 Detailed Treatment Guidelines for Indirect Pulp Therapy
4.6.6.1 Stepwise Excavation and Partial Excavation
The present two protocols refer to methods supported by high level of evidence. The first protocol takes adults into account, aiming to prevent exposure of the pulp using stepwise excavation: The last procedure is the partial excavation in one step aiming to prevent over-excavation in children (<18 years). Note the restrictions in both protocols:
4.6.6.1.1 Pretreatment Data (Stepwise Excavation)
-
Patient information; subjective evaluation of the region having the present symptom by questioning the patient on the area in focus, intensity, duration, stimulus, relief, and spontaneity. No signs of “irreversible pulpitis” is mandatory for stepwise excavation (no unbearable pain causing disturbed night sleep).
-
Objective extraoral examination as well as examination of the intraoral soft and hard tissues.
-
Clinical examination: The tooth is vital with no lingering or persistent prolonged pain following thermal testing. Other tests such as palpation, percussion, and mobility should have negative outputs.
-
Radiographic examination; radiographs showing the involved tooth, furcation, periapical area, and the surrounding bone. No apical pathosis is present. The depth of the caries lesion is in the pulpal quarter, and there is a well-defined radiopaque zone between the pulp and caries lesion defined here as a deep lesion (Fig. 4.1).
4.6.6.1.2 Treatment Protocol (Stepwise Excavation) [49]
-
Remove as much of the superficial necrotic and demineralized dentin, so that a temporary restoration can be placed in the cavity.
-
No excavation close to the pulp.
-
Calcium hydroxide-based material and glass-ionomer are placed.
-
Treatment interval 3–9 months.
-
Final excavation is carried out using hand excavators.
-
Calcium hydroxide based material and final permanent restoration is placed (Fig. 4.7).
Fig. 4.7 
Principle demonstration of the stepwise excavation approach of a molar. (a) Radiographic feature of a secondary molar with deep caries. (b) Cariogenic surface plaque and undermined enamel removed visualizing the exposed carious dentin. (c) A sketch of the temporization of the retained active carious dentin after 1-step. (d) After the treatment interval retained carious dentin will become darker, harder, and drier. (e) The retained carious dentin shown after removal of the temporary restoration. (f) Complete excavation is carried out to optimize the cavity for final restoration, and has been facilitated due to decrease of caries activity. (g) A sketch of the permanent restoration is in place. (h) A 4–year follow-up with no apical pathology. However, complete arrest of caries activity has not been achieved; a new proximal lesion has progressed in the third molar

4.6.6.1.3 Pretreatment Data (Partial Excavation)
-
Patient information: identical to stepwise.
-
Objective extraoral examination as well as examination of the intraoral soft and hard tissues.
-
Clinical examination: identical to stepwise.
-
Radiographic examination: radiographs showing the involved tooth, furcation, periapical area, and the surrounding bone. No apical pathosis is present. The depth of the caries lesion is in pulpal quarter, and starting from half the dentin thickness and into the pulp.
4.6.6.1.4 Treatment Protocol (Partial Excavation) [44]
-
Remove as much of the superficial necrotic and demineralized dentin, so the permanent restoration can be placed.
-
Final excavation is carried out using hand excavators.
-
Calcium hydroxide based material and final permanent restoration is placed (Fig. 4.8).
Fig. 4.8 
Clinical photographs and radiographs depicting a 1-visit indirect pulp therapy of permanent mandibular left first molar. (a) Tooth with a deep carious lesion with large accumulations of cariogenic biomasses. (b) Clinical photograph showing the cavity preparation (caries was not completely removed at areas close to the pulp), prior to the final restoration. (c) Clinical view after 1-year follow-up. (d) The pretreatment radiograph shows no apical pathosis, but a deep carious lesion. (e) After 1 year, the radiograph shows no apical radiolucency with successful treatment (Reprinted from Orhan et al. [51]; with permission)
-
The partial excavation approach has not been systematically examined in adults.

4.7 Factors Controlling Prognosis
Some factors controlling prognosis have been discussed for vital [9] and indirect pulp therapy [47, 52] in relation to caries. The prognosis is connected to methodological problems related to comparing data, which were not prospectively obtained so the following findings should be interpreted with caution.
Based on so-called pooled data, the success rates were reported to be 72.9 % for direct pulp capping (no distinction was made between Class I and II) with a recall period more than 3 years (patients: 6–10 years of age; n = 231), and 99.4 % for partial pulpotomy (patients, 6–27 years of age; n = 23) and 99.3 % (patients, 6–70 years of age; n = 37) for full pulpotomy [9]. Taken together these data indicate that the vital pulp therapy is effective with an acceptable outcome, and proper case selection should indicate the specific treatment needed.
A more recent retrospective observational study [54] suggested a 2-year survival rate of 56.2 % (patients, mean age 41 years, n = 51) for pulp capping. The relatively low survival rate confirms previous observational data suggesting that the prognosis of pulp capping may be related to age [9, 55]. Within a recent randomized clinical multicenter trial examining pulp capping versus partial pulpotomy in cariously exposed pulps in adults [52], the results showed an even worse outcome following both direct pulp capping (Class I) and partial pulpotomy, with a pooled pulp survival rate of only 33.2 % after 1½ year. The results showed that a caries lesion, located in the inner ¼ of the dentin in adults, may represent the threshold for success full pulp capping in adults, and without the use of magnification (Class I). In short, age of the patient and caries lesion depths are important prognostic variables.
In Box 4.5 variables are listed that influence prognosis.
Box 4.5. Potential Factors Increasing Success of Vital Pulp Therapy
-
Aseptic working field with rubber dam isolation – mandatory
-
Younger age – better prognosis
-
Immediate placement of the definitive restoration – to secure and prevent secondary infection
-
Mechanical/accidental exposure vs. an attempted carious exposure – If Class I or Class II protocols are chosen acceptable prognosis can be expected even in cariously exposed pulps but proper case selection is mandatory.
-
Size of exposure? If hemostasis can be obtained not an issue – important to reach direct contact and without a blood clot in between the agent and the pulp tissue.
-
Pulp protective agent – no high evidence data to select one particular material from another but MTA and calcium hydroxide have been the two most often used, with the former being the most often chosen material recently.
-
Pulpal inflammation that is judged reversible (see below).
Pulp status must be evaluated before treatment:
-
Patients’ symptoms and history is not enough.
-
Radiographic interpretation is not enough.
-
Use objective pulpal tests and arrive to complete pulpal and periapical diagnoses.
-
Hemostasis
4.8 The Indications for Vital Pulp Therapy May Change Over Time
Undoubtedly the vital pulp therapies have been established and developed in their own context of time and tradition. The focus of full pulpotomy has been to maintain a vital radicular pulp in order to secure the completion of the root complex in immature teeth (apexogenesis), and particularly to avoid the necrotic and bacterial infected incomplete root complex.
About 50 years ago the prevalence of caries worldwide as well as the speed of caries progression was higher than today [56]. If a “deep” or an “extremely deep” lesion is present even before the root complex is fully completed, the speed of caries progression has been obviously very high. Accordingly, it can be speculated that the degree of inflammation in “pulps with carious exposures in the 1960s” was often in a more severe and irreversible stage than what can be observed today. In other words, the rationale and the magnitude of using “full” pulpotomy may have changed today, as the speed of the caries progression has reduced.
However, as a paradox the “full” pulpotomy treatment has started to be reevaluated [57], and it may be an alternative to the vital pulpectomy, as the research area of pulp regeneration has developed rapidly. In this chapter, “full” pulpotomy has been presented with respect to (I) securing apexogenesis, and (II) being the emergency treatment approach for the acute “irreversible pulpitis” in molars.
However, pulpotomy is a highly integrated treatment approach for the future revascularization procedure, and perhaps particularly in necrotic teeth with an incomplete root complex [58, 59]. A revascularization protocol has been suggested, but currently being modified and tested [60, 61]. At this point in time, only limited evidence from case reports illustrates the potential for regenerative therapy in molars as opposed to single-rooted teeth (Box 4.6).
Box 4.6. Revascularization Protocol
-
Patient/parent compliance with the necessary multiple appointment treatment plan may be significant for case selection.
-
Disinfect canal but no mechanical instrumentation is performed.
-
Irrigate with sodium hypochlorite.
-
Dry root canal.
-
Triple antibiotic paste – (metronidazole, ciprofloxacin, minocycline) be aware of staining of the tooth with the use of minocycline.
-
Recently suggested that a classic calcium hydroxide dressing might be as beneficial as the triple paste but not tested in a randomized design.
-
Perform temporary restoration.
Two to three weeks later:
-
Remove medicament with sodium hypochlorite irrigation.
-
Induce bleeding from apical tissue (use of an anesthetic without a vasoconstrictor when trying to induce bleeding).
-
Control intracanal hemorrhage to below the CEJ with pressure.
-
Place MTA over blood clot to level of CEJ (a collagen matrix is useful for the controlled placement of MTA to a desired and optimal level).
-
Perform permanent restoration.
4.9 Summary
-
Carious pulp exposures are the most frequent cause for vital pulp therapy in molars.
-
Case selection should be performed with attention toward age of the patient and depth of the caries lesion.
-
Vital and indirect pulp therapies should be seen as permanent treatments.
-
Direct capping Class I should be avoided in the pulpal inner one-fourth.
-
Direct pulp Class II is designed for deep and extremely deep caries with the mandatory use of magnification.
-
High evidence data indicate that the two-step indirect approach should be the treatment of choice in carious lesions extending into the pulpal one-fourth of the dentin in adults.
-
No difference can be found between direct pulp capping and partial pulpotomy in adults.
-
Pulpotomy might be the future technical approach for even case with irreversible signs of pulpitis – but hemostasis is mandatory.
-
No systematic clinical evidence is yet available for molars and pulp regeneration. Moreover, the main focus addresses the necrotic root canal.
References
Black GV. A work on operative dentistry in two volumes. Vol. II the technical procedures in filling teeth. 2nd ed. Chigaco: Medico-Dental Publishing; 1908.
Tomes J. A system of dental surgery. London: John Churchill; 1859. p. 336.
Dumsha T, Hovland E. Considerations and treatment of direct and indirect pulp-capping. Dent Clin North Am. 1985;29:251–9.
Seale NS. Indirect pulp therapy: an alternative to pulpotomy in primary teeth. Tex Dent J. 2010;127:1175–83.
Seal NS, Glickman GN. Contemporary perspective on vital pulp therapy: views from the endodontists and pediatric dentists. J Endod. 2008;34:S57–61.
Mejáre IA, Axelsson S, Davidson T, Frisk F, Hakeberg M, Kvist T, Norlund A, Petersson A, Portenier I, Sandberg H, Tranæus S, Bergenholtz G. Diagnosis of the condition of the dental pulpa: a systematic review. Int Endod J. 2012;45:597–613.
Nadin G, Goel BR, Yeung CA, Glenny AM. Pulp treatment for extensive decay in primary teeth. Cochrane Database Syst Rev. 2003;(1):CD003220. doi: 10.1002/14651858. CD003220.
Miyashita H, Worthington HV, Qualtrough A. Plasschaert A. Pulp management for caries in adults: maintaining pulp vitality. Cochrane Database Syst Rev. 2007;(2):CD004484. doi: 10.1002/14651858.CD004484.pub2.
Aguilar P, Linsuwanont P. Vital pulp therapy in vital permanent teeth with cariously exposed pulp: a systematic review. J Endod. 2011;37:581–7.
MESH definition. Accessed 11 Feb 2016 from http://www.ncbi.nlm.nih.gov/mesh/?term=pulp+exposure.
Webber RT. Apexogenesis versus apexification. Dent Clin North Am. 1984;28:669–97.
Mjör IA. Human coronal dentine: structure and reactions. Oral Surg. 1972;33:810–23.
Trowbridge HO. Pathogenesis of pulpitis resulting from dental caries. J Endod. 1981;7:52–60.
Baume LJ. The biology of pulp and dentine. A historic, terminologic-taxonomic, histologic-biochemical, embryonic and clinical survey. Monogr Oral Sci. 1980;8:1–220.
Lesot H, Béque-Kirn C, Kubler MD, Meyer JM, Smith AJ, Cassidy N, Ruch JV. Experimental induction of odontoblast differentiation and stimulation during reparative processes. Cells Mat. 1993;33:201–17.
Smith AJ, Tobias RS, Plant CG, Browne RM, Lesot H. Odontoblast stimulation in ferrets by dentine matrix components. Arch Oral Biol. 1994;39:13–22.
Simon S, Smith AJ, Berdal A, Lumley PJ, Cooper PR. The MAP kinase pathway is involved in odontoblast stimulation via p38 phosphorylation. J Endod. 2010;36:256–9.
Simon SRJ, Berdal A, Cooper PR, Lumley PJ, Tomson PL, Smith AJ. Dentin-pulp complex regeneration: from lab to clinic. Adv Dent Res. 2011;23:340–5.
Couve E, Osorio R, Schmachtenberg O. The amazing odontoblast: activity, autophagy, and aging. J Dent Res. 2013;92(9):765–72.
Bjørndal L, Darvann T, Thylstrup A. A quantitative light microscopic study of the odontoblastic and subodontoblastic reactions to active and arrested enamel caries without cavitation. Caries Res. 1998;32:59–69.
Magloire H, Bouvier M, Joffre A. Odontoblast response under carious lesions. Proc Finn Dent Soc. 1992;88:257–74.
Smith AJ, Scheven BA, Takahashi Y, Ferracane JL, Shelton RM, Cooper PR. Dentine as a bioactive extracellular matrix. Arch Oral Biol. 2012;57:109–21.
Bjørndal L, Darvann T. A light microscopic study of odontoblastic and non-odonotoblastic cells involved in the tertiary dentinogenesis in well-defined cavitated carious lesions. Caries Res. 1999;33:50–60.
Olsson H, Petersson K, Rohlin M. Formation of a hard tissue barrier after pulp capping in humans. A systematic review. Int Endod J. 2006;39:429–42.
Cooper PR, Takahashi Y, Graham LW, Simon S, Imazato S, Smith AJ. Inflammation-regeneration interplay in the dentine-pulp complex. J Dent. 2010;38:687–97.
Seltzer S, Bender IB, Ziontz M. The dynamics of pulp inflammation: correlations between diagnostic data and actual histologic findings in the pulp. Oral Surg Oral Med Oral Pathol. 1963;16:846–71.
Seltzer S, Bender IB, Ziontz M. The dynamics of pulp inflammation: correlations between diagnostic data and actual histologic findings in the pulp. Oral Surg Oral Med Oral Pathol. 1963;16:969–77.
Dummer PM, Hicks R, Huws D. Clinical signs and symptoms in pulp disease. Int Endod J. 1980;13:27–35.
Reit C. Värdering av information. Tandläkertidningen. 1995;87:67–77.
Bjørndal L, Reit C. The annual frequency of root fillings, tooth extractions and pulp-related procedures in Danish adults during 1977–2003. Int Endod J. 2004;37:782–8.
Bjørndal L, Demant S, Dabelsteen S. Depth and activity of carious lesions as indicators for the regenerative potential of dental pulp after intervention. J Endod. 2014;40:S76–81.
Bogen G, Kim JS, Bakland LK. Direct pulp capping with mineral trioxide aggregate: an observational study. J Am Dent Assoc. 2008;139:305–15.
Reeves R, Stanley HR. The relationship of bacteria penetration and pulpal pathosis in carious teeth. Oral Surg Oral Med Oral Pat. 1966;22:59–65.
Cvek M. A clinical report on partial pulpotomy and capping with calcium hydroxide in permanent incisors with complicated crown fracture. J Endod. 1978;4:232–7.
Mejáre I, Cvek M. Partial pulpotomy in young permanent teeth with deep carious lesions. Endod Dent Traumatol. 1993;9:238–42.
Mass E, Zilberman U. Clinical and radiographic evaluation of partial pulpotomy in carious exposure of permanent molars. Pediatr Dent. 1993;15:257–9.
Barrieshi-Nusair KM, Qudeimat MA. A prospective clinical study of mineral trioxide aggregate for partial pulpotomy in cariously exposed permanent teeth. J Endod. 2006;32:731–5.
Witherspoon DE, Small JC, Haris GZ. Mineral trioxide aggregate pulpotomies: a case series outcome assessment. J Am Dent Assoc. 2006;137:610–8.
Eghbal MJ, Asgary S, Baglue RA, Parirokh M, Ghoddusi J. MTA pulpotomy of human permanent molars with irreversible pulpitis. Aust Endod J. 2009;35:4–8.
Hasselgren G, Reit C. Emergency pulpotomy: pain relieving effect with and without the use of sedative dressings. J Endod. 1989;15:254–6.
Chailertvanitkul P, Paphangkorakit J, Sooksantisakoonchai N, Pumas N, Pairojamornyoot W, Leela-Apiradee N, Abbott PV. Randomized control trial comparing calcium hydroxide and mineral trioxide aggregate for partial pulpotomies in cariously exposed pulps of permanent molars. Int Endod J. 2014;47:835–42.
Bjørndal L, Mjör IA. Dental caries: characteristics of lesions and pulpal reactions. In: Mjör IA, editor. Pulp-dentin biology in restorative dentistry. Chicago: Quintessence; 2002. p. 55–75.
Kerkhove Jr BC, Herman SC, Klein AI, McDonald RE. A clinical and television densitometric evaluation of the indirect pulp capping technique. J Dent Child. 1967;34:192–201.
Maltz M, de Oliveira EF, Fontanella V, Bianchi R. A clinical microbiological, and radiographic study of deep caries lesions after incomplete caries removal. Quint Int. 2002;33:151–9.
Gruythuysen R, van Strijp G, Wu M-K. Long-term survival of indirect pulp treatment performed in primary and permanent teeth with clinically diagnosed deep carious lesions. J Endod. 2010;36:1490–3.
Maltz M, Garcia R, Jardim JJ, et al. Randomized trial of partial vs. stepwise caries removal: 3-year follow-up. J Dent Res. 2012;91:1026–31.
Ricketts D, Lamont T, Innes NP, Kidd E, Clarkson JE. Operative caries management in adults and children. Cochrane Database Syst Rev. 2013;(3):CD003808. doi: 10.1002/14651858. CD003808.pub3. Review.
Schwendicke F, Meyer-Lueckel H, Dörfer C, Paris S. Failure of incompletely excavated teeth – a systematic review. J Dent. 2013;41:569–80.
Bjørndal L, Larsen T, Thylstrup A. A clinical and microbiological study of deep carious lesions during stepwise excavation using long treatment intervals. Caries Res. 1997;31:411–7.
Orhan AI, Oz FT, Ozcelik B, Orhan K. A clinical and microbial comparative study of deep carious lesion treatment in deciduous and young permanent molars. Clin Oral Invest. 2008;12:369–78.
Orhan AI, Firdevs TO, Orhan K. Pulp exposure occurrence and outcomes after 1- or 2-visit indirect pulp therapy vs complete caries removal in primary and permanent molars. Pediatric Dent. 2010;32:347–55.
Bjørndal L, Reit C, Bruun G, et al. Treatment of deep caries lesions in adults: randomized clinical trials comparing stepwise vs. direct complete excavation, and direct pulp capping vs. partial pulpotomy. Eur J Oral Sci. 2010;118:290–7.
Bjørndal L, Thylstrup A. A practice-based study on stepwise excavation of deep carious lesions in permanent teeth: a 1-year follow-up study. Community Dent Oral Epidemiol. 1998;26:122–8.
Miles JP, Gluskin AH, Chambers D, Peters OA. Pulp capping with mineral trioxide aggregate (MTA): a retrospective analysis of carious pulp exposures treated by undergraduate dental students. Oper Dent. 2010;35:20–8.
Hørsted P, Søndergaard B, Thylstrup A, EL Attar K, Fejerskov O. A retrospective study of direct pulp capping with calcium hydroxide compounds. Endod Dent Traumatol. 1985;1:29–34.
Marthaler TM. Changes in dental caries 1953–2003. Caries Res. 2004;38:173–81.
Simon S, Perard M, Zanini M, Smith AJ, Charpinter E, Djole SX, Lumley PJ. Should pulp champer pulpotomy be seen as a permanent treatment? Some preliminary thoughts. Int Endod J. 2013;46:79–87.
Banchs F, Trope M. Revascularization of immature permanent teeth with apical periodontitis: new treatment protocol? J Endod. 2004;30:196–200.
Lovelace TW, Henry MA, Hargreaves KM, Diogenes A. Evaluation of the delivery of mesenchymal stem cells into the root canal space of necrotic immature teeth after clinical regenerative endodontic procedure. J Endod. 2011;37:133–8.
Petrino JA, Boda KK, Shambarger S, Bowles WR, McClanahan SB. Challenges in regenerative endodontics: a case series. J Endod. 2010;36:536–41.
Torabinejad M, Turman M. Revitalization of tooth with necrotic pulp and open apex by using platelet-rich plasma: a case report. J Endod. 2011;37:265–8.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2017 Springer-Verlag Berlin Heidelberg
About this chapter
Cite this chapter
Bjørndal, L. (2017). Vital Pulp Therapy for Permanent Molars. In: Peters, O. (eds) The Guidebook to Molar Endodontics. Springer, Berlin, Heidelberg. https://doi.org/10.1007/978-3-662-52901-0_4
Download citation
DOI: https://doi.org/10.1007/978-3-662-52901-0_4
Published:
Publisher Name: Springer, Berlin, Heidelberg
Print ISBN: 978-3-662-52899-0
Online ISBN: 978-3-662-52901-0
eBook Packages: MedicineMedicine (R0)