
Abstract
Primary endoscopic surgery of the frontal sinus is a technically challenging procedure that requires a thorough understanding of the three-dimensional anatomy of the frontal recess. In addition to recognizing the various types of frontal recess cells as described by Kuhn, the configuration of the uncinate process must be appreciated in order to perform a well-planned operation. The traditional approach to the frontal recess involves dissection of ethmoid cells in a posterior to anterior direction. However, other approaches are described, such as the anterior approach via the agger nasi cell. Angled instrumentation, including powered debriders, are crucial to performing a thorough dissection of frontal recess cells while preserving mucosa. These techniques combined with close postoperative surveillance have produced excellent outcomes with this procedure.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
FormalPara Core Messages-
Primary endoscopic frontal sinusotomy focuses on a thorough dissection of frontal recess cells with minimal manipulation of the frontal ostium.
-
Mucosal preservation during surgery is imperative in preventing post-operative stenosis.
-
Understanding frontal recess anatomy requires having a three-dimensional understanding of the uncinate process and the various types of frontal recess cells
-
The surgeon must formulate a stepwise plan based on careful analysis of preoperative CT images.
-
Careful postoperative debridement and long-term follow up are necessary.
Introduction
The advent of endonasal endoscopic frontal sinusotomy as the standard of care for chronic frontal sinusitis can be attributed to three major factors [1]:
-
1.
High resolution video endoscopy
-
2.
Development of specialized instrumentation
-
3.
Better understanding of frontal sinus pathophysiology
Reports on long-term patency rates have also been published in the last 20 years, showing that the success rate for endoscopic frontal sinusotomy is comparable to the open procedures that were once commonly performed. However, endoscopic frontal sinusotomy continues to be technically challenging for many surgeons due to the complex anatomy and the relatively high re-stenosis rates.
The types of endonasal frontal sinusotomy have been classified by Draf as seen in Table 19.1 [2]. The Draf Type 1 frontal sinusotomy, which can be used interchangeably with “frontal recess surgery”, consists of dissection of the frontal recess without manipulation of the frontal sinus ostium itself. This is often the initial procedure in the surgical management algorithm for frontal sinusitis. The Draf Type 2a and 2b procedures may be performed as primary surgery in cases of mucoceles or serious complications of acute sinusitis. The Draf 3, or the endoscopic modified Lothrop procedure, is typically reserved for patients who are undergoing revision surgery or endoscopic resection of anterior cranial base tumors [3].
Outcomes
The literature regarding outcomes for endoscopic frontal sinus surgery usually includes all types of frontal sinusotomy, without distinguishing whether surgery was limited to the frontal recess or not. In addition, data for primary and revision surgeries are often presented together. Follow-up time and sample size vary widely, and patency rates range from 68 % to 100 % [1, 4]. One of the first large outcomes studies was by Wigand and Hosemann in 1991, who reported that more than two-thirds of their patients had patent frontal ostia via visualization or probing after a mean follow-up of 3.5 years [5]. More recent studies have shown better long-term results. A retrospective review by Friedman et al. reported long-term results for 152 patients (255 frontal sinuses) undergoing frontal recess dissection, and found a 67.6 % and 71.1 % patency rates after initial and revision surgery, respectively, and a 78.3 % rate of significant symptom improvement at a mean follow-up of 72 months [6]. Similarly, Chan et al. reported an overall patency rate of 88 % in 161 patients (294 frontal sinuses), 42 of which were primary cases, at a mean follow-up of 45.9 months [7]. Naidoo et al. reported their results for primary Draf 2a frontal sinusotomy in 109 patients (210 frontal sinuses). Overall patency rate was 92 % with complete symptom resolution in 78 % [8].
One can conclude from this data that endoscopic frontal sinusotomy is an effective procedure with acceptable long-term results. However, it is clear that long-term follow-up in these patients is necessary, as re-stenosis and recurrence of symptoms can occur after several years.
There is little consensus on predictive factors for frontal re-stenosis, but the following have all been implicated [4, 7, 8]:
-
Frontal ostium diameter
-
Smoking
-
Asthma
-
Radiologic severity
-
Number of prior surgeries
-
Tissue eosinophilia
-
Aspirin-sensitivity
Frontal Recess Anatomy
A thorough understanding of three-dimensional frontal recess anatomy is necessary in order to perform effective endoscopic surgery in this area. A key concept is that the frontal sinus ostium opens into an inverted funnel-shaped space called the frontal recess, rather than a “nasofrontal duct “as the older literature states [9] (Fig. 19.1).

The frontal recess is a potential inverted funnel-shaped space with the most narrow portion being the internal ostium (From 1st edition)
The boundaries of the frontal recess are:
-
The skull base superiorly
-
Middle turbinate medially
-
Lamina papyracea laterally
-
Nasofrontal beak anteriorly
-
The ethmoid bulla posteriorly.
Each of these boundaries needs to be clearly identified during dissection of the frontal recess. Because the frontal recess is technically part of the anterior ethmoid cavity, it contains many variations of ethmoid septations that determine the configuration of the frontal outflow tract into the middle meatus. Despite the fact that the anatomy is so highly variable, several authors have been able to describe frontal recess anatomy in a way that is useful and practical to the surgeon.
Based on the work of Van Aylea in the 1930s and 1940s, Kuhn described the different types of frontal recess cells as shown in Table 19.2 [10, 11]. The agger nasi cell (ANC), which refers to a single ethmoid cell anterior to the frontal outflow tract, is arguably the most prevalent frontal recess cell, and has been shown to correlate with frontal sinus obstruction [12, 13]. Cells that are found above the agger nasi are referred to as frontal cells (FC) types I-III. Any cell found completely within the sinus itself is referred to as a type IV frontal cell. Posterior to the frontal outflow tract, virtually all patients will have an ethmoid bulla, which forms the posterior border of the frontal recess. However, cells above the bulla—suprabullar cell (SBC) or frontal bulla cell (FBC)—can extend into the frontal recess and cause obstruction of the frontal outflow tract. Figure 19.2 demonstrates obstruction of the frontal outflow tract by an ANC and SBC.

View of left frontal recess with 45-degree endoscope showing agger nasi cell (arrow) and suprabullar cell (asterisk). Tip of suction navigator is placed at the location of the frontal outflow tract, which is obstructed by both cells
In some instances, a supraorbital ethmoid cell (SOEC) can form from pneumatization of the orbital plate of the frontal bone. Because the opening of the SOEC is directly adjacent to the frontal ostium, it can displace or narrow the frontal sinus ostium. More often, the SOEC can serve as a useful landmark for the anterior ethmoidal artery (AEA), since the posterior margin of the SOEC opening contains the AEA in the vast majority of cases [14] (Fig. 19.3). The interfrontal sinus septal cell (IFSSC) forms from pneumatization of the frontal sinus septum, and is located medial to the frontal sinuses. Despite its central location, it typically drains unilaterally (Fig. 19.4). Both SOECs and IFSSCs can easily be mistaken for the frontal sinus ostium. While the incidence of each of these frontal recess cells varies, they all have the potential to cause outflow tract obstruction and therefore need to be recognized [15].

View of left frontal recess with 45-degree endoscope. Tip of ostium seeker is inside a supraorbital cell. The anterior ethmoidal artery (arrow) is located at the posterior margin of the SOEC opening. The frontal outflow tract is immediately anterior and medial to the SOEC

Coronal CT scan and 45-degree endoscopic view of interfrontal sinus septal cell (asterisk) that opens into the right frontal recess. Frontal sinus ostium is seen adjacent to this
Another key anatomic concept is recognizing the superior attachment of the uncinate process, which can guide dissection in the frontal recess [16]. The uncinate process will course laterally and attach to the lamina papyracea in the majority of cases [17]. In this situation, the frontal sinus will drain into the middle meatus medial to the uncinate process. The space formed by the junction of the uncinate process and the lamina papyracea is called the recessus terminalis, and can be mistaken for the frontal recess (Fig. 19.5). In remaining cases, the uncinate process will attach to the skull base or the middle turbinate, producing a drainage pathway lateral to the uncinate process. The superior attachment in these cases must be carefully handled as to prevent fracture of the lateral lamella or fovea ethmoidalis. More recently, Wormald has suggested that understanding the anatomy of the frontal recess is dependent on recognizing the close relationship between the uncinate process and the ANC. In this model, the pneumatization pattern of the ANC and FCs will determine the orientation and attachment site of the uncinate process and as a result, the location of the frontal ostium [18]. Figure 19.6 demonstrates the relationship of the ANC and the uncinate process.

Coronal CT scan showing uncinate process (arrow) attaching to lamina papyracea. Recessus terminalis is indicated by the asterisk

Cadaveric dissection of left frontal recess. (a) Anterior aspect of the agger nasi cell is removed revealing the posterior wall of the agger nasi (asterisk) which is continuous with the uncinate process. (b) Posterior wall of the agger nasi (anterior aspect of uncinate) is removed. (c) 45-degree endoscopic view of the cut edge of the uncinate process (arrows). The uncinate attaches to the lamina papyracea (LP) laterally, forming the recessus terminalis (RT). Posterior to the uncinate, the lamella of the ethmoid bulla (EB) can be seen
Instrumentation
High-resolution video endoscopy with angled endoscopes has revolutionized the management of inflammatory diseases of the frontal sinuses. While the 0-degree endoscope is effective in performing the majority of the ethmoidectomy, a 45 or 70-degree endoscope is often necessary to fully visualize the frontal recess. A variety of angled instruments are available for removal of frontal recess cells. These instruments typically have a 90-degree curvature, or a less-angled 55-degree curvature. Non-cutting giraffe forceps as well as through-cutting forceps that open in an anterior-posterior orientation, as well as a medial-lateral orientation allow for precise removal of frontal cell fragments with preservation of mucosa. Curved frontal sinus curettes, suction catheters, rongeurs, mushroom punches, and frontal ostium seekers are also used when exploring the frontal recess and removing obstructing cells [9].
Powered instrumentation also plays an important role in frontal recess surgery. A 2.9 or 3.5 mm microdebrider blade with a 90° angle is commercially available. The blade is thin and long enough to insert into the frontal sinus and is capable of removing polyps while preserving underlying mucosa. At the same time, the mouth of the debrider is smaller than the standard straight 4 mm blade and can be rotated in the position desired by the surgeon. The microdebrider can be used to remove frontal recess cells with precision and minimal damage to surrounding mucosa. In patients with extensive polypoid disease, removal of polyps in the frontal recess and within the sinus itself using forceps may prove to be time-consuming and may lead to mucosal stripping. The judicious use of an angled microdebrider is highly recommended in such cases (Video 19.1).
-
Stereotactic navigation is recommended for primary frontal sinus surgery because of the complex anatomy. Even in cases with simple anatomy, image guidance is an invaluable teaching and training tool.
Virtually all commercially available image guidance systems have angled instruments that can be used for localization.
Technique
A careful analysis of CT images should be performed prior to initiating surgery. The CT scan is ideally performed with 1 mm or less axial cuts, and high-resolution reformatted coronal and sagittal images should be available as well. It is recommended that the surgeon systematically reviews all three planes of the CT scan in order to create a three-dimensional concept of the patient’s frontal recess anatomy.
Things to look for on the CT scan:
-
Kuhn frontal recess cells
-
Relationship of the uncinate process to the frontal ostium
-
Relationship of the agger nasi cell to the frontal ostium
-
Location of the anterior ethmoidal artery
In addition, the surgeon must formulate a stepwise plan based on this anatomy. Haphazard removal of septations in the frontal recess with the hope of finding the frontal ostium is not time-efficient, may lead to complications, and is generally not advisable. When reviewing the imaging, it is helpful to keep in mind some of the common causes of failure after primary frontal sinusotomy, namely incomplete dissection of frontal recess cells and incomplete removal of the superior attachment of the uncinate process.
Approaches to the frontal recess include the following:
-
Posterior to anterior ethmoidectomy
-
Anterior approach via agger nasi cell with or without “axillary flap”
-
“Bulla intact” frontal sinusotomy
Because of the nature of mucosal inflammation in chronic rhinosinusitis, frontal sinus disease is usually found in conjunction with inflammation of the other paranasal sinuses. In our practice, endoscopic sinus surgery proceeds first with an ethmoidectomy in an anterior to posterior direction to the level of the sphenoid sinus. With the skull base defined by the level of the sphenoid roof, ethmoid cells along the skull base are then removed in a posterior to anterior direction, ending with dissection of the frontal recess. Therefore, frontal sinusotomy is typically performed last. Although the nuances of surgery of the ethmoid, maxillary, and sphenoid sinuses are beyond the scope of this chapter, having an understanding of the anterior ethmoidectomy is crucial to the success of frontal sinusotomy.
The anterior ethmoidectomy begins with careful medialization of the middle turbinate. Any compromise of turbinate mucosa during this step can produce synechiae in the region of the axilla of the middle turbinate, which can in turn scar the frontal recess. While the middle turbinate may need to be resected in some cases, care must be taken to prevent the cut end of the turbinate from lateralizing and scarring to the lamina papyracea. If a concha bullosa exists, the entire lateral aspect needs to be removed since the middle turbinate will serve as the medial limit of dissection in the frontal recess. Next, a thorough removal of the uncinate process up to its superior attachment must be performed. If the uncinate is not completely visualized with the 0-degree endoscope, it is important to re-address this area later in the procedure. Inferiorly, the natural os of the maxillary sinus is then identified, and a maxillary antrostomy may or may not be performed. The medial wall of the orbit, or the lamina papyracea, must then be visualized or palpated. The lamina papyracea needs to be skeletonized during the anterior ethmoidectomy in order to serve as the lateral extent of dissection in the frontal recess.
After the skull base is defined, ethmoidectomy proceeds in a posterior to anterior direction along the skull base. As the surgeon approaches the frontal recess, angled endoscopes are usually necessary for adequate visualization. The anterior ethmoidal artery (AEA), which is found in between the second and third lamellae, courses the skull base in an anteromedial direction as it exits the lamina papyracea. It is often found hanging below the level of the skull base, and is dehiscent in up to 66 % of cases [19]. Knowledge of its anatomy is important in preventing troublesome bleeding and in performing a thorough dissection of frontal recess cells. Because of its vulnerable yet variable location, several studies have attempted to define its endoscopic anatomy. As mentioned previously, a useful landmark for the AEA is the SOEC. Because the AEA can be coursing within the posterior opening of the SOEC, aggressive removal of the septation extending from the posterior margin of the supraorbital cell is not advised. Once the AEA is identified, the remaining septations of the ethmoid bulla, SBC, FBC, and anterior margin of the SOEC opening can be removed along the skull base posterior to the frontal ostium, keeping in mind that the ethmoid roof begins to curve superiorly as one approaches the ostium.
In the frontal recess anterior to the ostium, the uncinate process must first be removed up to its superior attachment site. The frontal recess cells, particularly the ANC must be addressed using angled instrumentation. The walls of these cells are removed without disturbing the surrounding mucosa, in a process described by Stammberger as “uncapping an egg” [20]. As these cells are removed, the frontal ostium will become more visible. It is important to note that the while the ANC and the FCs are typically anterior to the ostium, they can be either medial or lateral to the ostium. In addition, the dense bone of the nasofrontal beak can be gently palpated in order to confirm the location of the ostium and ensure that all frontal cells are removed (Video 19.2). If an IFSSC exists, the laterality of its drainage pathway should be identified preoperatively on imaging. Removal of the septation separating the frontal sinus from the IFSSC will open the drainage pathway for both. With the Draf type I frontal sinusotomy, it should be noted that the frontal ostium itself is untouched, and circumferential mucosal preservation of the ostium should be achieved. Stenting of the frontal ostium may be considered in cases where mucosa is inadvertently injured or the frontal ostium is unusually narrow.
In contrast to the traditional posterior to anterior approach to the frontal recess, other approaches have been described. In cases of isolated frontal sinus disease, frontal sinusotomy alone can be performed without a complete anterior ethmoidectomy. After the middle turbinate is medialized, the superior portion of the uncinate process is removed up to its attachment. The agger nasi cell and frontal cells are then removed, leaving the ethmoid bulla intact. In most cases, this is sufficient to allow identification of the frontal ostium and restoration of the outflow tract. The “intact bulla sinusotomy”, first described by Louri in 1993, essentially leaves the ethmoid bulla to be used as the posterior boundary of the frontal recess, thereby preventing injury to the anterior ethmoidal artery and minimizing trauma to healthy sinus cavities [21, 22].
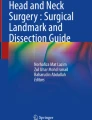
In an approach described by Schaefer and Close in 1990, endoscopic frontal sinusotomy begins with removal of the anterior wall of the agger nasi cell at the axilla of the middle turbinate [23]. The posterior wall of the agger nasi and any existing Kuhn frontal cells are subsequently removed with up-biting forceps. A variation of this technique has been described as the agger nasi “punch-out procedure” [24]. The technique was elaborated by Wormald, who described the use of a posteriorly based mucosal flap to cover the bone along the cut edge of the middle turbinate axilla. The flap is raised and set aside initially, and the anterior wall of the agger nasi cell is entered with a Hajek sphenoid punch. This provides excellent exposure to the frontal recess with a 0-degree endoscope, facilitating removal of other frontal cells with straight instruments. Wormald reported a high rate of frontal ostium patency at a mean follow-up of 15.4 months [25] (Fig. 19.7).

Left frontal recess dissection with 45-degree endoscope. (a) 90-degree frontal sinus curette placed immediately posterior to a partition containing the anterior wall of the suprabullar cell and the posterior wall of the agger nasi cell. (b) This partition is gently fractured in an anterior direction (c) frontal sinus ostium visualized after removal of the agger nasi (*See Video 19.2 for corresponding video of Fig. 19.7)
Because lateralization of the middle turbinate has been cited as a common cause of failure after frontal sinusotomy, it must be ensured that the middle turbinate remains in the medialized position during the healing period. Although non-absorbable nasal packing is rarely used in our practice, finger cots are generally better tolerated than petroleum jelly impregnated gauze. We prefer absorbable hemostatic materials, which help to stent open the middle meatus. Also available are absorbable medicated stents, which can be placed in the ethmoid cavity. Finally, surgical techniques for maintaining middle turbinate medialization include creation of controlled adhesions with the septum and a trans-septal middle turbinate suture [26, 27].
Techniques to maintain medialization of the middle turbinate:
-
Use of spacer or stent
-
Controlled adhesion with septum
-
Trans-septal suture
In difficult cases, an image guidance system is helpful in confirming entry into the frontal sinus. Some have reported the utility of trans illumination as a method for confirming patency of the frontal outflow tract [28]. Other techniques include intraoperative use of a balloon dilatation device with an illuminated guide wire. For cases in which excessive bleeding prevents adequate visualization, angled suction instruments are an option. However, most bleeding subsides with tamponade using oxymetazoline or epinephrine-soaked pledgets, in addition to optimization of the patient’s blood pressure. In rare cases when bleeding and poor visualization persist, it is recommended that the procedure is staged.
Postoperatively, patients are prescribed oral antibiotics, nasal steroid spray, and high-pressure nasal saline irrigations.
-
In our practice, patients with severe polyposis or history of sinus tissue eosinophilia are also given budesonide irrigations and a month-long prednisone taper if not contraindicated.
Postoperative debridements are performed twice during the first month using angled rigid endoscopes and instruments. Because of the long-term risk of frontal stenosis, these patients are routinely monitored for several years or more.
Conclusion
Primary endoscopic frontal sinusotomy focuses on the removal of obstructing frontal recess cells with mucosal preservation and minimal manipulation of the frontal sinus ostium. This requires technical skill as well as a sound understanding of the three-dimensional anatomy of the frontal recess. Familiarizing oneself with the different types of frontal recess cells as described by Kuhn is most useful. In addition, knowing the variations of the superior attachment of the uncinate process, as well as the pneumatization patterns of the ANC and FCs, is crucial to successful frontal recess dissection. New instrumentation along with advances in the knowledge of sinonasal anatomy and physiology have allowed excellent long-term outcomes with this approach.
References
Weber R, Draf W, Kratzsch B, Hoseman W, Schaefer SD. Modern concepts of frontal sinus surgery. Laryngoscope. 2001;111:137–46.
Draf W. Endonasal micro-endoscopic frontal sinus surgery, the Fulda concept. Oper Tech Otolaryngol Head Neck Surg. 1991;2:234–40.
Draf W. Endonasal frontal sinus drainage type I-III according to Draf. In: Kountakis SE, Senior BE, Draf W, editors. The frontal sinus. Berlin: Springer; 2005. p. 219–32.
Chandra RK, Palmer JN, Tangsujarittham T, Kennedy DW. Factors associated with failure of frontal sinusotomy in the early follow-up period. Otolaryngol Head Neck Surg. 2004;131(4):514–8.
Wigand ME, Hosemann WG. Endoscopic surgery for frontal sinusitis and its complications. Am J Rhinol. 1991;5(3):85–9.
Friedman M, Bliznikas D, Vidyasagar R, Joseph NJ, Landsberg R. Long-term results after endoscopic sinus surgery involving frontal recess dissection. Laryngoscope. 2006;116(4):573–9.
Chan Y, Melroy CT, Kuhn CA, Kuhn FL, Daniel WT, Kuhn FA. Long-term frontal sinus patency after endoscopic frontal sinusotomy. Laryngoscope. 2009;119(6):1229–32.
Naidoo Y, Wen D, Bassiouni A, Keen M, Wormald PJ. Long-term results after primary frontal sinus surgery. Int Forum Allergy Rhinol. 2012;2(3):185–90.
Karanfilov BI, Kuhn FA. The endoscopic frontal recess approach. In: Kountakis SE, Senior BE, Draf W, editors. The frontal sinus. Berlin: Springer; 2005. p. 219–32.
Van Alyea OE. Ethmoid labyrinth: anatomic study with clinical significance of its structural characteristics. Arch Otolaryngol. 1939;29:881–901.
Kuhn FA. Chronic frontal sinusitis: the endoscopic frontal recess approach. Oper Tech Otolaryngol Head Neck Surg. 1996;7:222–9.
Bradley DT, Kountakis SE. The role of agger nasi air cells in patients requiring revision endoscopic frontal sinus surgery. Otolaryngol Head Neck Surg. 2004;131(4):525–7.
Brunner E, Jacobs JB, Shpizner BA, Lebowitz RA, Holliday RA. Role of the agger nasi cell in chronic frontal sinusitis. Ann Otol Rhinol Laryngol. 1996;105(9):694–700.
Jang DW, Lachanas VA, White LC, Kountakis SE. Supraorbital ethmoid cell: a constant landmark for endoscopic identification of the anterior ethmoidal artery. Submitted for publication. Otolaryngol Head Neck Surg. 2014;151(6):1073–7.
Lien CF, Weng HH, Chang YC, Lin YC, Wang WH. Computed tomographic analysis of frontal recess anatomy and its effect on the development of frontal sinusitis. Laryngoscope. 2010;120(12):2521–7.
Stammberger H, Kopp W, Dekornfeld TJ, et al. Special endoscopic anatomy. In: Stammberger H, Hawke M, editors. Functional endoscopic sinus surgery: the Messerklinger technique. Philadelphia: BC Decker Publishers; 1991. p. 61–90.
Landsberg R, Friedman M. A computer-assisted anatomical study of the nasofrontal region. Laryngoscope. 2001;111(12):2125–30.
Wormald PJ. The agger nasi cell: the key to understanding the anatomy of the frontal recess. Otolaryngol Head Neck Surg. 2003;129(5):497–507.
Araujo Filho BC, Weber R, Pinheiro Neto CD, Lessa MM, Voegels RL, Butugan O. Endoscopic anatomy of the anterior ethmoidal artery: a cadaveric dissection study. Braz J Otorhinolaryngol. 2006;72(3):303–8.
Stammberger H. FESS “Uncapping the Egg” the endoscopic approach to frontal recess and sinuses. A surgical technique of the Graz University Medical School. Tuttlingen: Endo-Press; 2000.
Louri MC. Endoscopic frontal recess and frontal sinus ostium dissection. Laryngoscope. 1993;103:455–8.
Landsberg R, Segev Y, Friedman M, Fliss DM, Derowe A. A targeted endoscopic approach to chronic isolated frontal sinusitis. Otolaryngol Head Neck Surg. 2006;134(1):28–32.
Schaefer SD, Close LG. Endoscopic management of frontal sinus disease. Laryngoscope. 1990;100:155–60.
Pletcher SD, Sindwani R, Metson R. The agger nasi punch-out procedure (POP): maximizing exposure of the frontal recess. Laryngoscope. 2006;116:1710–2.
Wormald PJ. The axillary flap approach to the frontal recess. Laryngoscope. 2002;112:494–9.
Thornton RS. Middle turbinate stabilization technique in endoscopic sinus surgery. Arch Otolaryngol Head Neck Surg. 1996;122(8):869–72.
Bolger WE, Kuhn FA, Kennedy DW. Middle turbinate stabilization after functional endoscopic sinus surgery: the controlled synechiae technique. Laryngoscope. 1999;109(11):1852–3.
Friedman M, Landsberg R, Tanyeri H. Intraoperative and postoperative assessment of frontal sinus patency by transillumination. Laryngoscope. 2000;110(4):683–4.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Electronic Supplementary Material
Below is the link to the electronic supplementary material.
Video 19.1
Removal of polyps from left frontal recess in a patient with allergic fungal sinusitis. 45-degree endoscope and 90-degree 3.5 mm rotatable microdebrider is used in the frontal recess and within the frontal sinus. Bone fragments are removed with 90-degree giraffe forceps. Note that mucosal preservation is possible with careful use of powered instrumentation. (MP4 13536 kb)
Video 19.2
Frontal recess dissection in a patient with frontal sinus obstruction secondary to a large agger nasi cell and suprabullar cell. (See Figs. 19.1 and 19.7) 45-degree endoscope and 90-degree frontal sinus curette are used to fracture the agger nasi cell anteriorly and inferiorly. Fragments of the cell are removed with 90-degree giraffe instruments and a 90-degree 3.5 mm microdebrider. (MP4 18029 kb)
Rights and permissions
Copyright information
© 2016 Springer-Verlag Berlin Heidelberg
About this chapter
Cite this chapter
Jang, D.W., Kountakis, S.E. (2016). Primary Endoscopic Surgery. In: Kountakis, S., Senior, B., Draf, W. (eds) The Frontal Sinus. Springer, Berlin, Heidelberg. https://doi.org/10.1007/978-3-662-48523-1_19
Download citation
DOI: https://doi.org/10.1007/978-3-662-48523-1_19
Published:
Publisher Name: Springer, Berlin, Heidelberg
Print ISBN: 978-3-662-48521-7
Online ISBN: 978-3-662-48523-1
eBook Packages: MedicineMedicine (R0)