
Abstract
Evidence from a growing body of preclinical and clinical studies points to the efficacy of continuously administrating anticancer chemotherapeutic drugs in low doses. This relatively new treatment strategy concept is called low-dose metronomic (LDM) chemotherapy. The therapeutic efficacy of LDM has been assessed for reducing the tumor load during the acute phase and in delaying relapse during the maintenance phase. The major benefits found in using LDM include the lack of major toxicities or complications as compared to conventional chemotherapy regimens and improved quality of life. Traditional therapeutic modalities in oncology aim toward more specific tumor targets at the tumor microenvironment, whereas LDM chemotherapy acts on a broad spectrum of mechanisms, some of which are still not clear. We will discuss in this chapter several possible LDM chemotherapy anticancer mechanisms of action. Initially, LDM was considered an antiangiogenic treatment strategy; however, in the last decade additional preclinical studies uncovered other possible mechanisms including enhancing the antitumor immune response, substantially increasing the efficacy of targeted drugs by various mechanisms, targeting a subset of chemotherapy-resistant tumor cells, and blunting host response effects found following conventional therapy. While LDM chemotherapy is currently undergoing phase III clinical evaluation, its mechanisms of action are only partially understood. Elucidating LDM’s mechanisms of action will give physicians an additional major weapon to deploy in the comprehensive management of cancer.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others

Keywords
These keywords were added by machine and not by the authors. This process is experimental and the keywords may be updated as the learning algorithm improves.
1 Introduction
Initial studies which investigated the mechanism of action of low-dose metronomic (LDM) chemotherapy demonstrated that this treatment regimen solely acts by inhibiting tumor angiogenesis. Both Browder et al. and Klement et al. – the first two back-to-back studies introducing the concept of LDM chemotherapy – showed that low-dose cyclophosphamide (CTX) or vinblastine led to significant antitumor activity in Lewis lung carcinoma and neuroblastoma, respectively [1, 2]. Browder et al. also showed that the same tumors that responded to LDM were resistant to the conventional maximum tolerated dose (MTD) chemotherapy. Klement et al. demonstrated that the addition of an antiangiogenic drug, DC101, a VEGFR2-blocking antibody, to LDM vinblastine significantly and markedly improved LDM’s therapeutic outcome in their neuroblastoma tumor model. While both studies suggested that LDM’s mechanism of action is by blocking angiogenesis, this clearly does not explain why the addition of a VEGFR2-blocking antibody to LDM vinblastine significantly improved therapy outcome, unless additional complementary mechanisms are involved [2]. These and other results were the impetus for additional preclinical and clinical studies. In this review, we will focus on several possible mechanisms to explain the antitumor activities of LDM chemotherapy and their possible implications.
2 The Antiangiogenic Effects of Low-Dose Metronomic Chemotherapy
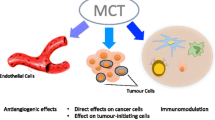
Tumor angiogenesis consists of a local division of endothelial cells from preexisting vessels, leading to neovasculature sprouting into the tumor. In addition, the systemic mobilization of bone marrow-derived proangiogenic cells, in particular endothelial progenitor cells (EPCs), incorporates into the tumor vessel wall, thus enhancing angiogenesis [3]. In the last several decades, efforts have been made to inhibit the formation of tumor blood vessels in order to halt tumor growth. Several antiangiogenic drugs have been approved by the Food and Drug Administration for the treatment of cancer. However, these therapies exhibit modest clinical benefits. In this context, LDM chemotherapy has also been identified as an antiangiogenic treatment strategy affecting various pathways of angiogenesis. LDM chemotherapy directly kills endothelial cells, induces natural inhibitors of angiogenesis, and inhibits systemic angiogenesis mediated by circulating endothelial precursor cells (CEPs). These various mechanisms of metronomic antiangiogenic effects are illustrated in Fig. 2.1 and are summarized below.

An illustration of the antiangiogenic mechanisms of metronomic chemotherapy affecting tumor growth. Metronomic chemotherapy inhibits both (1) local angiogenesis by directly killing endothelial cells and (2) systemic angiogenesis by suppressing the levels of CEPs which then cannot home to the treated tumor. In addition, (3) metronomic chemotherapy reduces the expression of proangiogenic factors, e.g., VEGF-A and FGF2, and increases the expression of antiangiogenic factors, e.g., thrombospondin-1 (TSP-1) and endostatin. The changes in these factors can inhibit both (4) local and (5) systemic angiogeneses. (6) Tumor cells exposed to metronomic chemotherapy can also increase the expression of antiangiogenic factors, and as such they may support the antiangiogenic effect of this treatment regimen
2.1 Low-Dose Metronomic Chemotherapy Directly Kills Endothelial Cells
The prolonged in vitro administration of low concentrations of cytotoxic drugs to rapidly dividing endothelial cells, such as human umbilical endothelial cells (HUVECs), induces cell apoptosis when compared to tumor cells which are more resistant to such therapy [4]. This initial study has led to further testing various chemotherapy drugs administered in low doses to assess their antiangiogenic properties on endothelial cell viability. In another study, human microvascular endothelial cells (HMVECs) were exposed to L-OHP (an active metabolite of oxaliplatin), 5FU, and SN-38 (an active metabolite of irinotecan). The cells were cultured with these drugs in low doses continuously for 144 h. The results revealed that SN-38 but not 5FU or L-OHP inhibited endothelial cell proliferation. The combination of the three drugs, however, minimally affected colorectal cancer cell proliferation [5]. Taxanes and temozolomide (TMZ) have been also shown to act as antiangiogenic agents in continuous low-dose exposure in cultures [6, 7]. Murray et al. demonstrated that sorafenib, a small-molecule antiangiogenic drug blocking the tyrosine kinase of VEGF receptors, enhances the anti-endothelial cell effect when it was combined with continuous low doses of etoposide, paclitaxel, and TMZ in culture [8]. Additionally, mouse brain endothelial cells and U87 human glioblastoma but not C6 rat glioblastoma cells were shown to be sensitive to continuous low doses of TMZ [7]. When this drug regimen was assessed in vivo, the authors demonstrated that LDM TMZ significantly reduced the antitumor activity in both C6 and U87 tumor-bearing mice, primarily due to its antiangiogenic activity as assessed by microvessel density [7]. These results further suggest that even when tumor cells are resistant to LDM TMZ in culture, they can be sensitive in the whole organism due to the drug’s antiangiogenic effects.
The antiangiogenic activity of LDM chemotherapy has also been documented in vivo in several preclinical models. LDM doxifluridine suppresses tumor growth via its antiangiogenic activity, as assessed by an in vivo imaging technique. In this study, the addition of TNP-470, an antiangiogenic agent, to the LDM doxifluridine regimen resulted in a significant reduction of the growth of uterine carcinosarcoma in bearing mice compared to mice treated with each of the drugs and to the drug regimen alone [9]. This study also discusses additional results from various trials demonstrating the additional or even synergistic antitumor effects of LDM chemotherapy when combined with antiangiogenic drugs. For example, LDM topotecan in combination with pazopanib, a small-molecule inhibitor of angiogenesis, resulted in a significant increase in antitumor activity, due in part to reduced tumor microvessel density. The antiangiogenic effects seen in this study were related to the inhibition of systemic angiogenesis rather than inhibiting local antiangiogenic activity in treated tumors. However, no experiments were performed to test whether LDM topotecan may directly kill endothelial cells in culture [10]. Taken together, the aforementioned in vitro and in vivo preclinical studies suggest that continuous exposure of chemotherapy in low doses in the absence or presence of direct antiangiogenic agents markedly induces endothelial cell apoptosis in vitro and as a result increases their antitumor efficacy in vivo. Thus, one of the mechanisms of LDM chemotherapy is in inducing endothelial cell apoptosis, since in many cases these cells are more sensitive to the drug regimen than the tumor cells.
2.2 Low-Dose Metronomic Chemotherapy Alters the Expression of Angiogenesis-Related Factors
A balance between proangiogenic and antiangiogenic factors exists in tissues in order to maintain angiogenic homeostasis. In tumors this balance is violated as tumor cells secrete proangiogenic factors leading to increased endothelial cell sprouting and tumor angiogenesis [11]. Several studies investigated the antiangiogenic effects of LDM chemotherapy focusing on changes in the balance between angiogenic stimuli and natural inhibitors of angiogenesis. LDM CTX upregulates the expression of thrombostpondin-1 (TSP-1), a natural inhibitor of angiogenesis [12], in the serum of Lewis lung carcinoma-bearing mice. While tumor-bearing mice treated with LDM CTX express high levels of TSP-1 and subsequently exhibit enhanced treatment outcome, mice lacking the expression of TSP-1 (TSP1−/− mice) bearing Lewis lung carcinoma treated with the same therapy did not show any antitumor activity of such therapy [13]. In support of this study, it was shown that TSP-1 expression is upregulated in tumor cells and perivascular cells following LDM CTX, indicating again the antiangiogenic effects of LDM CTX not related to direct endothelial cell killing [14].
In contrast, a combination of LDM CTX with high-dose doxorubicin exhibited a dramatic decrease in the expression of TSP-1 in the plasma of rats bearing prostate tumors, suggesting that the antiangiogenic effects mediated by the upregulation of endogenous inhibitors of angiogenesis can be negated when such treatment is combined with a bolus administration of other chemotherapy drugs [15]. Apart from TSP-1, other pro- and antiangiogenic factors are altered in response to LDM chemotherapy. It was recently demonstrated that LDM etoposide alters the angiogenic switch in tumors by inhibiting VEGF-A and FGF2 secreted from tumor cells and by increasing plasma levels of endostatin, a natural endogenous angiogenesis inhibitor [16]. Clinical studies showed decreased levels of angiogenic factors such as VEGF and PDGF-BB in cancer patients treated with LDM capecitabine or LDM CTX, methotrexate, and thalidomide [17, 18]. In addition, TSP-1 serum levels were upregulated in cancer patients treated with LDM CTX. However, the elevated levels of TSP-1 did not correlate with clinical benefits [19]. In patients with non-small lung cancer, levels of VEGF, VEGFR1, and TSP-1 were tested in the serum following either MTD or LDM cisplatinum and docetaxel chemotherapies. While MTD combined therapy induced a significant change in VEGFR1 and TSP-1 serum levels, the impact of LDM chemotherapy (using weekly docetaxel and cisplatinum regimen) did not alter these factors in the serum of treated patients. Surprisingly, MTD chemotherapy induced a significant long-lasting increase in TSP-1 levels and a decrease in VEGFR1 levels as opposed to LDM chemotherapy. The authors concluded that continued administration of LDM chemotherapy does not necessarily act as an antiangiogenic chemotherapy regimen when compared to MTD regimen [20].
2.3 Low-Dose Metronomic Chemotherapy Blocks Systemic Angiogenesis
While the effect of local angiogenesis is well established in cancer, the contribution of systemic angiogenesis (also called vasculogenesis) is greatly debated [21, 22]. Recent studies have shown that following acute therapy, systemic cells significantly contribute to the regeneration of neo-angiogenesis in treated tumors, thereby promoting tumor regrowth [23]. LDM chemotherapy was shown to substantially suppress the number of circulating bone marrow-derived proangiogenic cells (BMDCs) such as CEPs. The initial study in this direction tested levels of CEPs in lymphoma-bearing mice that underwent LDM or MTD CTX. While the MTD regimen induced a substantial increase in the number of CEPs in the blood, the LDM regimen significantly and continuously suppressed it. Once the LDM CTX therapy was terminated, the number of CEPs subsequently rose in peripheral blood followed by tumor regrowth [24]. These results further suggest that LDM CTX can suppress systemic angiogenesis mediated by CEPs. Based on this study, antiangiogenic drugs or treatment strategies thought to inhibit systemic angiogenesis have been further tested. Mice treated with antiangiogenic drugs or with LDM chemotherapy using CTX, vinblastine, cisplatinum, or vinorelbine revealed that the maximal suppression in CEP levels in mice undergoing such therapy correlated with the maximum antiangiogenic activity [25, 26]. Therefore, the CEP suppression level could serve as a biomarker for the optimal angiogenic activity of both antiangiogenic drugs and LDM chemotherapy [25, 26]. More recent studies focused on CEP level measurements in mice treated with drug combinations involving an LDM chemotherapy regimen. For example, the administration of LDM taxanes such as docetaxel alone or in combination with AEE788, a dual EGFR and VEGFR inhibitor, resulted in a marked decrease in CEP levels in mice bearing ovarian cancers which led to a significant reduction in tumor growth and prolonged survival [6]. In another study, oral topotecan in LDM regimen in combination with pazopanib resulted in a marked reduction in viable CEPs as well as circulating endothelial cells (CECs) and reduced tumor microvessel density in several pediatric solid tumors [10]. Importantly, suppressed levels of CEPs were also documented in a drug combination in which acute therapy can sometimes induce rapid mobilization of CEPs. For example, studies conducted on mice treated with vascular disrupting agents (VDAs) revealed a marked and rapid elevation in CEP levels in the peripheral blood of treated mice [27]. The same effects have also been demonstrated in cancer patients enrolled in a phase I clinical study testing the anti-vascular agent AVE8062 [28]. Consequently, Daenen et al. reasoned that the combination of LDM CTX with VDAs may block the rapid mobilization of CEPs found following VDA therapy. They tested this by using mice bearing metastatic breast carcinoma or melanoma xenografts which were treated with OXi-4503, LDM CTX, or the combination of the two drugs. They found that levels of CEPs which were rapidly elevated following VDA therapy were significantly inhibited when such therapy was combined with LDM CTX. These anti-vasculogenic effects resulted in less colonization of BMDCs at the treated tumor, which is often seen following VDA therapy. The authors concluded that the combination of VDA and LDM CTX resulted in prolonged tumor control, in part due to the anti-vasculogenic activity of the metronomic chemotherapy [29].
Clinically, CEC and CEP levels were evaluated in cancer patients undergoing LDM chemotherapy to assess their prognostic or predictive value following antiangiogenic therapy. Mancuso et al. analyzed the kinetics and viability of CECs in advanced breast cancer patients treated with methotrexate, thalidomide, and LDM CTX. They found that increased levels of apoptotic CECs correlated with therapy outcome, suggesting that CECs may predict clinical response to metronomic/antiangiogenic therapy [30]. In another study, long-term interferon-α, thalidomide, and celecoxib treatment combination was tested in patients with slow-growing solid tumors. The levels of CEPs were analyzed during the course of the therapy, and the results suggest that low baseline levels of CEPs predict subsequent clinical benefits [31]. Another recent study strongly supports these findings. Investigators demonstrated that high CEP levels in hepatocellular cancer patients treated with sorafenib and LDM tegafur and uracil were associated with poor survival [32]. CEC levels, on the other hand, were evaluated in breast cancer patients treated with LDM CTX, capecitabine, and bevacizumab (an anti-VEGF-A neutralizing antibody). As opposed to CEPs, high baseline levels of CECs predicted prolonged clinical benefits. It was suggested that active vascular turnover in tumors may result in high baseline levels of CECs which then can effectively be blocked by an antiangiogenic drug or treatment regimen [33].
Not all chemotherapy drugs administered in an LDM regimen may affect systemic angiogenesis. A recent study by Francia et al. has demonstrated that oral gemcitabine administered daily inhibits tumor growth and angiogenesis, but does not significantly suppress the levels of CEPs. Therefore, this drug regimen has antitumor and antiangiogenic activity without inhibiting the systemic angiogenesis as seen with other LDM chemotherapies [34]. Overall, these studies highlight the impact that most chemotherapy drugs administered in an LDM chemotherapy regimen have on BMDC levels, particularly on CEPs and CECs. However, LDM’s effects on other BMDCs known to contribute to systemic angiogenesis, e.g., hemangiocytes [35] and myeloid-derived suppressor cells [36], still need further investigation.
3 Additional Antitumor Activity Mechanisms of Low-Dose Metronomic Chemotherapy
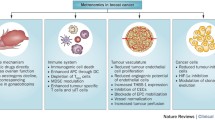
In the last decade, new mechanisms of antitumor activity of LDM chemotherapy besides those related to antiangiogenic activity have been proposed and investigated. It has been shown that LDM chemotherapy can enhance the immune response against tumor cells thereby promoting tumor growth control in an “immunotherapy-like” strategy. This mechanism will extensively be covered in another chapter in this book. Additionally, limited evidence exists regarding the potential of LDM chemotherapy in targeting cancer stem cells (CSCs), a subpopulation of tumor cells with stem cell characteristics that are normally resistant to conventional therapy. Lastly, LDM chemotherapy blocks host effects promoting tumor regrowth commonly found following acute therapy [37]. Table 2.1 presents a summary of several proposed mechanisms of action for the antitumor activity of LDM chemotherapy. These proposed mechanisms are discussed in more detail below.
3.1 Low-Dose Metronomic Chemotherapy Enhances the Antitumor Activity of Oncolytic Virotherapy
Oncolytic virotherapy is one of the recent novel investigated routes of cancer therapy which has entered clinical testing. The efficacy of oncolytic virotherapy combines the ability of the virus to directly destroy cancer cells on one hand and to increase the immune system’s response against cancer cells on the other [38]. The current oncolytic viruses are still under thorough investigation both preclinically and clinically. Although they are considered nonpathogenic to humans, they were found to selectively replicate in human cancer cells, thereby promoting cancer regression [39]. One of the complications of oncolytic virotherapy is the immune system’s reaction against the viral infection. Therefore, the use of LDM chemotherapy which can suppress or deplete several immune cell types that normally act against the injected virus is considered a therapeutic advantage when combined with oncolytic virotherapy [40]. This treatment combination was found to be efficacious in several preclinical tumor models, such as B16 melanoma [40], ovarian carcinoma [41], glioblastoma [42], and pancreatic cancer [43] among others. In addition to the impact of LDM chemotherapy on the immune system, other effects may exist. For example, LDM paclitaxel in combination with an oncolytic virus in relapsed ovarian cancer resulted in substantial treatment benefits. The reason was that paclitaxel therapy promoted a morphological change in replicating tumor cells, which in turn induced an immune response against the tumor cells leading to an induction of the immune system against the tumor cells, especially those which were already infected with the oncolytic virus [41]. Clinically, patients with advanced solid tumors who progressed after conventional therapies were treated with a combination of LDM CTX and oncolytic adenovirus therapy. While the purpose of LDM CTX was to eliminate the T-regulatory cell activity, the intra-tumoral injection of the oncolytic virus increased cytotoxic T cells and induced Th1-type immunity in those patients, leading to a decrease in tumor burden. These results further suggest that LDM chemotherapy promotes immunological effects which can enhance the oncolytic virotherapy in several ways [44]. CTX in low doses is not the only drug that can act synergistically with oncolytic virotherapy; LDM TMZ can also enhance the antitumor activity of oncolytic virotherapy in patients with refractory tumors. This treatment regimen inhibits regulatory T-cell activity, which in combination with oncolytic adenovirus therapy results in tumor responses in two thirds of the patients. The authors suggest that LDM chemotherapy promotes tumor cell autophagy and elicits antitumor immune responses which results in improved oncolytic virus therapy efficacy [45]. It should be noted that oncolytic virotherapy has been tested also with MTD chemotherapy and found to be superior in terms of treatment efficacy compared to conventional MTD monotherapy [46]. In addition, tumor regrowth observed following MTD chemotherapy can be significantly delayed with treatment involving oncolytic virotherapy [47]. However, most of these studies are still under thorough clinical evaluation in early phase studies, and the mechanisms of action of these treatment combinations are not fully understood. Overall, the combination of LDM chemotherapy with oncolytic virotherapy enhances the activity of the virus against the tumor cells by altering the immune system against the virus and/or by improving the sensitivity of the tumor cells to the virotherapy.
3.2 Low-Dose Metronomic Chemotherapy Prevents Host Effects Seen in Response to Acute Therapy
Rebound angiogenesis has often been seen following treatment with MTD chemotherapy, in part due to a rapid mobilization and tumor homing of systemic angiogenic cells, e.g., CEPs to the treated tumor site, leading to tumor regrowth [3]. As opposed to MTD, LDM chemotherapy induces its antiangiogenic effects in part by suppressing the levels of CEPs in the blood [25]. Importantly, it has been suggested that the changes in the levels of CEPs in response to acute therapy are not associated with the tumor type or tumor stage but rather almost entirely related to the response of the host which generates such effects, especially since some of the experiments were performed on non-tumor-bearing mice [3, 27, 48].
We have recently shown that following MTD therapy, a rapid and significant upregulation of host G-CSF and SDF-1 was observed in the plasma of treated mice and cancer patients [3]. These factors are known to accelerate BMDC mobilization and homing into tumors; therefore, they could explain the regrowth of tumors following acute therapy [3, 49]. Additionally, the host effect in response to acute therapy is not limited to boosting tumor angiogenesis, but it may also accelerate metastasis spread [50]. These pro-tumorigenic and pro-metastatic effects found following MTD chemotherapy were also reported after other therapies including small-molecule antiangiogenic drugs [51] and VDAs [49]. There is some evidence that LDM chemotherapy can negate these host proangiogenic and pro-tumorigenic effects. The administration of LDM regimen following an acute dose of chemotherapy markedly improved the treatment outcome of pancreatic, breast, and prostate cancers as well as erythroleukemia [52, 53]. Vives et al. recently demonstrated that LDM CTX or gemcitabine administered following acute MTD therapy of the same drug was superior in terms of antitumor activity associated with decreased angiogenesis and reduced metastasis for the treatment of ovarian and pancreatic adenocarcinoma models when compared to any of the treatments involving monotherapy regimen. In fact, peritoneal metastases were documented only in the control and MTD treatment groups, but were absent in the group consisting of MTD and LDM chemotherapy drug combination [54]. Hanahan and colleagues termed this combined regimen as a “chemo-switch” in which MTD chemotherapy (either alone or in combination with targeted agents) is followed by LDM maintenance therapy [52]. In the clinic, the combination of MTD and LDM therapy was recently tested in a multi-targeted chemo-switch regimen using sorafenib, gemcitabine, and LDM capecitabine for the treatment of metastatic renal cell cancer. The authors reported that the response rates of the combined therapy were greater than what was documented for gemcitabine and capecitabine or sorafenib monotherapy. These initial findings suggest a synergistic activity of the chemo-switch concept that needs further clinical evaluation [55].
Although LDM on its own leads to antiangiogenic effects, a remarkable synergistic antitumor effect was observed when an LDM chemotherapy regimen was combined with an antiangiogenic drug or with a VDA (for review see [56, 57]). As mentioned above, the combination of a VDA with continuous administration of LDM CTX resulted in decreased tumor regrowth compared with VDA monotherapy, due in part to the inhibition of acute CEP mobilization found following VDA monotherapy [29]. In addition, LDM topotecan administered in combination with pazopanib [58] showed significant improvement in overall survival of mice bearing metastatic ovarian cancer [59, 60]. The superior effects of the maintenance LDM chemotherapy which was administered after acute therapy could be explained by the fact that LDM regimen reduces the systemic involvement of BMDCs that are rapidly mobilized following some acute therapies as demonstrated by Daenen et al. [29]. In addition, LDM regimen reduces the expression levels of several circulating proangiogenic factors induced in response to the targeted therapy [54, 59, 60]. Therefore, blocking the pro-tumorigenic activities generated by the host in response to acute therapy explains the treatment superiority of combining a targeted therapy with LDM chemotherapy, even when the same drug is used in both regimens.
3.3 Low-Dose Metronomic Chemotherapy May Disrupt the Cancer Stem Cell’s Niche
A subpopulation of cells in the tumor mass has recently been characterized as tumor “stem cells” since these cells can initiate tumor growth and metastasis. Such cells are termed cancer stem cells (CSCs) or tumor-initiating cells (TICs) [61]. The properties of CSCs are quite similar to those of normal stem cells. CSCs have the ability to initiate tumor growth, drive tumor cell proliferation, and differentiate into multi-lineage cells and to contain a self-renewal capacity [61]. Recent studies showed that CSCs possess a strong DNA repair system, which distinguishes them from other “more differentiated” tumor cells [62]. Like stem cells, CSCs resist many conventional therapies including chemotherapy and radiation. As such, they are probably the sole viable subpopulation of tumor cells left after therapy. Ongoing research into new treatment modalities which can kill CSCs are currently being undertaken [63]. In terms of angiogenesis, a growing body of evidence suggests that CSCs require angiogenic factors and blood vessels to maintain their characteristics. CSCs were found to reside in close proximity to tumor vasculature [64, 65]. Disrupting the VEGF-neuropilin axis was found to decrease the number of CSCs, suggesting that CSCs are angiogenic or VEGF dependent [65, 66]. CSCs of C6 rat gliomas secrete both VEGF and SDF-1 used to promote systemic and local angiogenesis thereby contributing to tumor growth [67]. Therefore, antiangiogenic therapy, in particular anti-VEGF therapy, was predicted to possibly eradicate CSCs. Indeed, in several preclinical studies it was demonstrated that anti-VEGF therapy reduces the number of CSCs in treated tumors thereby explaining the increased treatment efficacy of chemotherapy in combination with antiangiogenic therapy [65, 66]. For other antiangiogenic treatment strategies, such as LDM chemotherapy, only limited literature exists. Treatment of C6 rat glioma-bearing mice with LDM CTX alone or in combination with an antiangiogenic drug (DC101) led to a reduced number of sphere-forming tumor cells that are usually enriched with CSCs [23]. In a hepatocellular carcinoma model, the combination of LDM CTX with an antiangiogenic drug led to tumor dormancy as long as the LDM chemotherapy regimen was maintained. However, once the mice were removed from the maintenance treatment protocol, tumor regrowth was subsequently observed. Although the authors focused on tumor dormancy, others suggested that dormant tumor cells could serve as CSCs since they can initiate tumor growth [68]. Interestingly, in another study in which MTD chemotherapy was followed by maintenance LDM therapy, the authors documented that the combination of chemo-switch therapy resulted in a decreased number of CSCs in both pancreatic and ovarian cancers using CD133, CD44, and CD24 as markers, which are selectively expressed on CSCs of such tumor types [54]. Overall, while limited evidence suggests that LDM chemotherapy may affect the viability and number of CSCs, more research is required to elucidate the mechanism by which LDM chemotherapy acts against CSCs.
4 Summary
Efforts to uncover the mechanisms of action of LDM chemotherapy are still ongoing. Several mechanisms have been presented which can explain the antitumor activity of this treatment modality. However, LDM’s mechanisms of action are only partially understood, and we are far from comprehending the complete picture. Some of the benefits of using LDM chemotherapy in the clinic are the following: the usually low costs of such drugs, improved quality of life of treated patients, and the lack of major toxicities and clinical complications [69]. As such, LDM chemotherapy can be offered as an alternative treatment for conventional therapy. It can be given during the acute phase to reduce tumors and in times of remission as a maintenance therapy to delay relapse and as a palliative treatment for advanced incurable metastatic diseases [37, 56]. Recent clinical and preclinical studies demonstrate (mostly empirically) that LDM chemotherapy substantially improves the antitumor activity of other anticancer drugs such as antiangiogenic small-molecule drugs [70]. While the combination of small-molecule drugs along with MTD chemotherapy regimen usually resulted in major toxicities and complications, LDM chemotherapy as a replacement has been shown preclinically to work well. It should be noted that the results of several phase III clinical studies utilizing LDM chemotherapy regimen in combination with other targeted drugs will soon be announced. This may lead to a paradigm shift in the way we treat cancer [37, 56]. Meanwhile, the lack of a thorough understanding on how LDM chemotherapy acts against tumor cells and the empirical nature of its evaluation in the clinic probably moderate the enthusiasm among clinicians in extensively using this treatment modality for cancer [37, 69]. Further experimentation toward elucidating LDM chemotherapy’s mechanisms of action will pave the way for the intelligent use of this treatment regimen benefiting cancer patients worldwide.
References
Browder T, Butterfield CE, Kraling BM, Marshall B, O’Reilly MS, Folkman J (2000) Antiangiogenic scheduling of chemotherapy improves efficacy against experimental drug-resistant cancer. Cancer Res 60:1878–1886
Klement G, Baruchel S, Rak J, Man S, Clark K, Hicklin D, Bohlen P, Kerbel RS (2000) Continuous low-dose therapy with vinblastine and VEGF receptor-2 antibody induces sustained tumor regression without overt toxicity. J Clin Invest 105:R15–R24
Shaked Y, Henke E, Roodhart JM, Mancuso P, Langenberg MH, Colleoni M, Daenen LG, Man S, Xu P, Emmenegger U et al (2008) Rapid chemotherapy-induced acute endothelial progenitor cell mobilization: implications for antiangiogenic drugs as chemosensitizing agents. Cancer Cell 14:263–273
Bocci G, Nicolaou KC, Kerbel R (2002) Protracted low-dose effects on human endothelial cell proliferation and survival in vitro reveal a selective antiangiogenic window for various chemotherapeutic drugs. Cancer Res 62:6938–6943
Fontana A, Galli L, Fioravanti A, Orlandi P, Galli C, Landi L, Bursi S, Allegrini G, Fontana E, Di Marsico R et al (2009) Clinical and pharmacodynamic evaluation of metronomic cyclophosphamide, celecoxib, and dexamethasone in advanced hormone-refractory prostate cancer. Clin Cancer Res 15:4954–4962
Kamat AA, Kim TJ, Landen CN Jr, Lu C, Han LY, Lin YG, Merritt WM, Thaker PH, Gershenson DM, Bischoff FZ et al (2007) Metronomic chemotherapy enhances the efficacy of antivascular therapy in ovarian cancer. Cancer Res 67:281–288
Kim JT, Kim JS, Ko KW, Kong DS, Kang CM, Kim MH, Son MJ, Song HS, Shin HJ, Lee DS et al (2006) Metronomic treatment of temozolomide inhibits tumor cell growth through reduction of angiogenesis and augmentation of apoptosis in orthotopic models of gliomas. Oncol Rep 16:33–39
Murray A, Little SJ, Stanley P, Maraveyas A, Cawkwell L (2010) Sorafenib enhances the in vitro anti-endothelial effects of low dose (metronomic) chemotherapy. Oncol Rep 24:1049–1058
Naganuma Y, Choijamts B, Shirota K, Nakajima K, Ogata S, Miyamoto S, Kawarabayashi T, Emoto M (2011) Metronomic doxifluridine chemotherapy combined with the anti-angiogenic agent TNP-470 inhibits the growth of human uterine carcinosarcoma xenografts. Cancer Sci 102:1545–1552
Kumar S, Mokhtari RB, Sheikh R, Wu B, Zhang L, Xu P, Man S, Oliveira ID, Yeger H, Kerbel RS et al (2011) Metronomic oral topotecan with pazopanib is an active antiangiogenic regimen in mouse models of aggressive pediatric solid tumor. Clin Cancer Res 17:5656–5667
Folkman J (1996) Tumor angiogenesis and tissue factor. Nat Med 2:167–168
Bouck N, Polverini PJ, Tolsma SS, Frazier WA, Good D (1991) Tumor suppressor gene control of angiogenesis. J Cell Biochem Suppl 15F:216 (Abstr)
Bocci G, Francia G, Man S, Lawler J, Kerbel RS (2003) Thrombospondin-1, a mediator of the antiangiogenic effects of low-dose metronomic chemotherapy. Proc Natl Acad Sci U S A 100:12917–12922
Hamano Y, Sugimoto H, Soubasakos MA, Kieran M, Olsen BR, Lawler J, Sudhakar A, Kalluri R (2004) Thrombospondin-1 associated with tumor microenvironment contributes to low-dose cyclophosphamide-mediated endothelial cell apoptosis and tumor growth suppression. Cancer Res 64:1570–1574
Damber JE, Vallbo C, Albertsson P, Lennernas B, Norrby K (2006) The anti-tumour effect of low-dose continuous chemotherapy may partly be mediated by thrombospondin. Cancer Chemother Pharmacol 58:354–360
Panigrahy D, Kaipainen A, Butterfield CE, Chaponis DM, Laforme AM, Folkman J, Kieran MW (2010) Inhibition of tumor angiogenesis by oral etoposide. Exp Ther Med 1:739–746
Loven D, Be’ery E, Yerushalmi R, Koren C, Sulkes A, Lavi I, Shaked Y, Fenig E (2008) Daily low-dose/continuous capecitabine combined with neo-adjuvant irradiation reduces VEGF and PDGF-BB levels in rectal carcinoma patients. Acta Oncol 47:104–109
Colleoni M, Orlando L, Sanna G, Rocca A, Maisonneuve P, Peruzzotti G, Ghisini R, Sandri MT, Zorzino L, Nole F et al (2006) Metronomic low-dose oral cyclophosphamide and methotrexate plus or minus thalidomide in metastatic breast cancer: antitumor activity and biological effects. Ann Oncol 17:232–238
Lansiaux A, Salingue S, Dewitte A, Clisant S, Penel N (2012) Circulating thrombospondin 1 level as a surrogate marker in patients receiving cyclophosphamide-based metronomic chemotherapy. Invest New Drugs 30:403–404
Tas F, Duranyildiz D, Soydinc HO, Cicin I, Selam M, Uygun K, Disci R, Yasasever V, Topuz E (2008) Effect of maximum-tolerated doses and low-dose metronomic chemotherapy on serum vascular endothelial growth factor and thrombospondin-1 levels in patients with advanced nonsmall cell lung cancer. Cancer Chemother Pharmacol 61:721–725
Wickersheim A, Kerber M, de Miguel LS, Plate KH, Machein MR (2009) Endothelial progenitor cells do not contribute to tumor endothelium in primary and metastatic tumors. Int J Cancer 125:1771–1777
Bertolini F, Shaked Y, Mancuso P, Kerbel RS (2006) The multifaceted circulating endothelial cell in cancer: from promiscuity to surrogate marker and target identification. Nat Rev Cancer 6:835–845
Folkins C, Man S, Xu P, Shaked Y, Hicklin DJ, Kerbel RS (2007) Anticancer therapies combining antiangiogenic and tumor cell cytotoxic effects reduce the tumor stem-like cell fraction in glioma xenograft tumors. Cancer Res 67:3560–3564
Bertolini F, Paul S, Mancuso P, Monestiroli S, Gobbi A, Shaked Y, Kerbel RS (2003) Maximum tolerable dose and low-dose metronomic chemotherapy have opposite effects on the mobilization and viability of circulating endothelial progenitor cells. Cancer Res 63:4342–4346
Shaked Y, Emmengger U, Man S, Cervi D, Bertolini F, Ben-David Y, Kerbel RS (2005) The optimal biological dose of metronomic chemotherapy regimens is associated with maximum antiangiogenic activity. Blood 106:3058–3061
Shaked Y, Bertolini F, Man S, Rogers MS, Cervi D, Foutz T, Rawn K, Voskas D, Dumont DJ, Ben-David Y et al (2005) Genetic heterogeneity of the vasculogenic phenotype parallels angiogenesis: implications for cellular surrogate marker analysis of antiangiogenesis. Cancer Cell 7:101–111
Shaked Y, Ciarrocchi A, Franco M, Lee CR, Man S, Cheung AM, Hicklin DJ, Chaplin D, Foster FS, Benezra R et al (2006) Therapy-induced acute recruitment of circulating endothelial progenitor cells to tumors. Science 313:1785–1787
Farace F, Massard C, Borghi E, Bidart JM, Soria JC (2007) Vascular disrupting therapy-induced mobilization of circulating endothelial progenitor cells. Ann Oncol 18:1421–1422
Daenen LG, Shaked Y, Man S, Xu P, Voest EE, Hoffman RM, Chaplin DJ, Kerbel RS (2009) Low-dose metronomic cyclophosphamide combined with vascular disrupting therapy induces potent antitumor activity in preclinical human tumor xenograft models. Mol Cancer Ther 8:2872–2881
Mancuso P, Colleoni M, Calleri A, Orlando L, Maisonneuve P, Pruneri G, Agliano A, Goldhirsch A, Shaked Y, Kerbel RS et al (2006) Circulating endothelial cell kinetics and viability predict survival in breast cancer patients receiving metronomic chemotherapy. Blood 108:452–459
Noberasco C, Spitaleri G, Mancuso P, Zorzino L, Radice D, Milani A, Rocca A, Bertolini F, Sandri MT, Curigliano G et al (2009) Safety, tolerability and biological effects of long-term metronomic administration of non-cytotoxic anti-angiogenic agents. Oncology 77:358–365
Shao YY, Lin ZZ, Chen TJ, Hsu C, Shen YC, Hsu CH, Cheng AL (2011) High circulating endothelial progenitor levels associated with poor survival of advanced hepatocellular carcinoma patients receiving sorafenib combined with metronomic chemotherapy. Oncology 81:98–103
Calleri A, Bono A, Bagnardi V, Quarna J, Mancuso P, Rabascio C, Dellapasqua S, Campagnoli E, Shaked Y, Goldhirsch A et al (2009) Predictive potential of angiogenic growth factors and circulating endothelial cells in breast cancer patients receiving metronomic chemotherapy plus bevacizumab. Clin Cancer Res 15:7652–7657
Francia G, Shaked Y, Hashimoto K, Sun J, Yin M, Cesta C, Xu P, Man S, Hackl C, Stewart J et al (2012) Low-dose metronomic oral dosing of a prodrug of gemcitabine (LY2334737) causes antitumor effects in the absence of inhibition of systemic vasculogenesis. Mol Cancer Ther 11:680–689
Jin DK, Shido K, Kopp HG, Petit I, Shmelkov SV, Young LM, Hooper AT, Amano H, Avecilla ST, Heissig B et al (2006) Cytokine-mediated deployment of SDF-1 induces revascularization through recruitment of CXCR4+ hemangiocytes. Nat Med 12:557–567
Shojaei F, Wu X, Malik AK, Zhong C, Baldwin ME, Schanz S, Fuh G, Gerber HP, Ferrara N (2007) Tumor refractoriness to anti-VEGF treatment is mediated by CD11b(+)Gr1(+) myeloid cells. Nat Biotechnol 25:911–920
Loven D, Hasnis E, Bertolini F, Shaked Y (2012) Low-dose metronomic chemotherapy: from past experience to new paradigms in the treatment of cancer. Drug Discov Today 18(3–4):193–201
Kelly E, Russell SJ (2007) History of oncolytic viruses: genesis to genetic engineering. Mol Ther 15:651–659
Chan WM, Rahman MM, McFadden G (2013) Oncolytic myxoma virus: the path to clinic. Vaccine 31(39):4252–4258
Qiao J, Wang H, Kottke T, White C, Twigger K, Diaz RM, Thompson J, Selby P, de Bono J, Melcher A et al (2008) Cyclophosphamide facilitates antitumor efficacy against subcutaneous tumors following intravenous delivery of reovirus. Clin Cancer Res 14:259–269
Ingemarsdotter CK, Baird SK, Connell CM, Oberg D, Hallden G, McNeish IA (2010) Low-dose paclitaxel synergizes with oncolytic adenoviruses via mitotic slippage and apoptosis in ovarian cancer. Oncogene 29:6051–6063
Cheema TA, Kanai R, Kim GW, Wakimoto H, Passer B, Rabkin SD, Martuza RL (2011) Enhanced antitumor efficacy of low-dose Etoposide with oncolytic herpes simplex virus in human glioblastoma stem cell xenografts. Clin Cancer Res 17:7383–7393
Onimaru M, Ohuchida K, Nagai E, Mizumoto K, Egami T, Cui L, Sato N, Uchino J, Takayama K, Hashizume M et al (2010) Combination with low-dose gemcitabine and hTERT-promoter-dependent conditionally replicative adenovirus enhances cytotoxicity through their crosstalk mechanisms in pancreatic cancer. Cancer Lett 294:178–186
Cerullo V, Diaconu I, Kangasniemi L, Rajecki M, Escutenaire S, Koski A, Romano V, Rouvinen N, Tuuminen T, Laasonen L et al (2011) Immunological effects of low-dose cyclophosphamide in cancer patients treated with oncolytic adenovirus. Mol Ther 19:1737–1746
Liikanen I, Ahtiainen L, Hirvinen ML, Bramante S, Cerullo V, Nokisalmi P, Hemminki O, Diaconu I, Pesonen S, Koski A et al (2013) Oncolytic adenovirus with temozolomide induces autophagy and antitumor immune responses in cancer patients. Mol Ther 21:1212–1223
Opyrchal M, Aderca I, Galanis E (2009) Phase I clinical trial of locoregional administration of the oncolytic adenovirus ONYX-015 in combination with mitomycin-C, doxorubicin, and cisplatin chemotherapy in patients with advanced sarcomas. Methods Mol Biol 542:705–717
Black AJ, Morris DG (2012) Clinical trials involving the oncolytic virus, reovirus: ready for prime time? Expert Rev Clin Pharmacol 5:517–520
Shaked Y, Kerbel RS (2007) Antiangiogenic strategies on defense: on the possibility of blocking rebounds by the tumor vasculature after chemotherapy. Cancer Res 67:7055–7058
Shaked Y, Tang T, Woloszynek J, Daenen LG, Man S, Xu P, Cai SR, Arbeit JM, Voest EE, Chaplin DJ et al (2009) Contribution of granulocyte colony-stimulating factor to the acute mobilization of endothelial precursor cells by vascular disrupting agents. Cancer Res 69:7524–7528
Gingis-Velitski S, Loven D, Benayoun L, Munster M, Bril R, Voloshin T, Alishekevitz D, Bertolini F, Shaked Y (2011) Host response to short-term, single-agent chemotherapy induces matrix metalloproteinase-9 expression and accelerates metastasis in mice. Cancer Res 71:6986–6996
Ebos JM, Lee CR, Christensen JG, Mutsaers AJ, Kerbel RS (2007) Multiple circulating proangiogenic factors induced by sunitinib malate are tumor-independent and correlate with antitumor efficacy. Proc Natl Acad Sci U S A 104:17069–17074
Pietras K, Hanahan D (2005) A multitargeted, metronomic, and maximum-tolerated dose “chemo-switch” regimen is antiangiogenic, producing objective responses and survival benefit in a mouse model of cancer. J Clin Oncol 23:939–952
Shaked Y, Emmenegger U, Francia G, Chen L, Lee CR, Man S, Paraghamian A, Ben David Y, Kerbel RS (2005) Low-dose metronomic combined with intermittent bolus-dose cyclophosphamide is an effective long-term chemotherapy treatment strategy. Cancer Res 65:7045–7051
Vives M, Ginesta MM, Gracova K, Graupera M, Casanovas O, Capella G, Serrano T, Laquente B, Vinals F (2013) Metronomic chemotherapy following the maximum tolerated dose is an effective anti-tumour therapy affecting angiogenesis, tumour dissemination and cancer stem cells. Int J Cancer 133(10):2464–2472
Bellmunt J, Trigo JM, Calvo E, Carles J, Perez-Gracia JL, Rubio J, Virizuela JA, Lopez R, Lazaro M, Albanell J (2010) Activity of a multitargeted chemo-switch regimen (sorafenib, gemcitabine, and metronomic capecitabine) in metastatic renal-cell carcinoma: a phase 2 study (SOGUG-02-06). Lancet Oncol 11:350–357
Pasquier E, Kavallaris M, Andre N (2010) Metronomic chemotherapy: new rationale for new directions. Nat Rev Clin Oncol 7:455–465
Kerbel RS, Kamen BA (2004) Antiangiogenic basis of low-dose metronomic chemotherapy. Nature Rev Cancer 4:423–436
Hutson TE, Figlin RA (2007) Evolving role of novel targeted agents in renal cell carcinoma. Oncology (Williston Park) 21:1175–1180
Merritt WM, Nick AM, Carroll AR, Lu C, Matsuo K, Dumble M, Jennings N, Zhang S, Lin YG, Spannuth WA et al (2010) Bridging the gap between cytotoxic and biologic therapy with metronomic topotecan and pazopanib in ovarian cancer. Mol Cancer Ther 9:985–995
Hashimoto K, Man S, Xu P, Cruz-Munoz W, Tang T, Kumar R, Kerbel RS (2010) Potent preclinical impact of metronomic low-dose oral topotecan combined with the antiangiogenic drug pazopanib for the treatment of ovarian cancer. Mol Cancer Ther 9:996–1006
Reya T, Morrison SJ, Clarke MF, Weissman IL (2001) Stem cells, cancer, and cancer stem cells. Nature 414:105–111
Viale A, De Franco F, Orleth A, Cambiaghi V, Giuliani V, Bossi D, Ronchini C, Ronzoni S, Muradore I, Monestiroli S et al (2009) Cell-cycle restriction limits DNA damage and maintains self-renewal of leukaemia stem cells. Nature 457:51–56
Zhou BB, Zhang H, Damelin M, Geles KG, Grindley JC, Dirks PB (2009) Tumour-initiating cells: challenges and opportunities for anticancer drug discovery. Nat Rev Drug Discov 8:806–823
Calabrese C, Poppleton H, Kocak M, Hogg TL, Fuller C, Hamner B, Oh EY, Gaber MW, Finklestein D, Allen M et al (2007) A perivascular niche for brain tumor stem cells. Cancer Cell 11:69–82
Benayoun L, Gingis-Velitski S, Voloshin T, Segal E, Segev R, Munster M, Bril R, Satchi-Fainaro R, Scherer SJ, Shaked Y (2012) Tumor-initiating cells of various tumor types exhibit differential angiogenic properties and react differently to antiangiogenic drugs. Stem Cells 30:1831–1841
Beck B, Driessens G, Goossens S, Youssef KK, Kuchnio A, Caauwe A, Sotiropoulou PA, Loges S, Lapouge G, Candi A et al (2011) A vascular niche and a VEGF-Nrp1 loop regulate the initiation and stemness of skin tumours. Nature 478:399–403
Folkins C, Shaked Y, Man S, Tang T, Lee CR, Zhu Z, Hoffman RM, Kerbel RS (2009) Glioma tumor stem-like cells promote tumor angiogenesis and vasculogenesis via vascular endothelial growth factor and stromal-derived factor 1. Cancer Res 69:7243–7251
Martin-Padura I, Marighetti P, Agliano A, Colombo F, Larzabal L, Redrado M, Bleau AM, Prior C, Bertolini F, Calvo A (2012) Residual dormant cancer stem-cell foci are responsible for tumor relapse after antiangiogenic metronomic therapy in hepatocellular carcinoma xenografts. Lab Invest 92(7):952–966
Kerbel RS (2007) Improving conventional or low dose metronomic chemotherapy with targeted antiangiogenic drugs. Cancer Res Treat 39:150–159
Pasquier E, Kieran MW, Sterba J, Shaked Y, Baruchel S, Oberlin O, Kivivuori MS, Peyrl A, Diawarra M, Casanova M et al (2011) Moving forward with metronomic chemotherapy: meeting report of the 2nd International Workshop on Metronomic and Anti-Angiogenic Chemotherapy in Paediatric Oncology. Transl Oncol 4:203–211
Acknowledgments
This study was supported in part by the European Research Council (under FP-7 program) and Israel Cancer Research Fund to YS. The authors would like to thank Prof. Giulio Francia for the critical reading of this chapter. The authors disclose no conflict of interest.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2014 Springer-Verlag Berlin Heidelberg
About this chapter
Cite this chapter
Fremder, E., Shaked, Y. (2014). Mechanisms of Action of Low-Dose Metronomic Chemotherapy. In: Bocci, G., Francia, G. (eds) Metronomic Chemotherapy. Springer, Berlin, Heidelberg. https://doi.org/10.1007/978-3-662-43604-2_2
Download citation
DOI: https://doi.org/10.1007/978-3-662-43604-2_2
Published:
Publisher Name: Springer, Berlin, Heidelberg
Print ISBN: 978-3-662-43603-5
Online ISBN: 978-3-662-43604-2
eBook Packages: Biomedical and Life SciencesBiomedical and Life Sciences (R0)