
Abstract
Various bioceramics or xenograft has been used to avoid autograft. However, there are large differences in the chemistry, the micro- and macrostructure, and consequently the performance in terms of resorption, absorption, and regeneration of physiological bone. The differences in such available bioceramics were reported and critical data presented. Recent developments related to CaP scaffolds including improvements in terms of engineering chemistry, surface properties, microstructure, and porosities, which lead them to be considered as being bioinstructive rather than osteoconductive scaffolds, have opened up new opportunities for bone regenerative technologies. Not only are some of these CaP bioceramics scaffolds osteoinductive in their own right, but evidence also supports the hypothesis that specific engineering bioceramics have a direct influence on the differentiation and proliferation of human mesenchymal stem cells (hMSCs). Tissue engineering, new bioactive molecules, and new surgical technologies increase the potential application of CaP bioceramics as carriers of these cells and also as scaffolds capable of guiding the behavior of these cells and the efficiency of bone regeneration. If the smart bioinstructive CaP scaffold technology led to a higher efficacy of CaP scaffolds, it would allow further surgical applications in bone tissue regeneration. The mechanical properties required for bone ingrowth and bone remodeling and mechanotransduction must be explored to allow for development of new generation scaffolds.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
- Bone substitutes
- Bone regeneration
- Calcium phosphate bioceramics
- Injectable calcium phosphate
- Scaffolds
- Tissue engineering
4.1 Introduction
Although bone tissue possesses the capacity for regenerative growth, the repair process is impaired in many clinical and pathological situations. Large bone loss caused by trauma and tumor resection and/or aging requires reconstructive surgery and/or bone regeneration. At present, bone surgeons have three different possibilities for replacing bone:
-
Autogenous bone grafts are primarily used for bone replacement, despite the pain, septic complications, and the limited amount of bone harvested from the iliac crest or other sites.
-
Allogenic bone grafts are obtained from tissue banks. These grafts have limitations because of the possible transmission of nonconventional agents or viruses and the risk of immunological incompatibility.
-
Alloplastic bone substitutes are produced in various compositions and shapes. These biomaterials can be used to fill bone cavities, serving as a scaffold for bone regeneration from the peri-implant region. Bone substitutes can also be used to supplement autogenous bone, or in combination with bone marrow aspirates. The ideal biomaterial should have a variety of forms and sizes, all with sufficient strength for use in load-bearing sites. It should also be biocompatible, biodegradable, and able to be substituted by newly formed bone.
Numerous synthetic bone graft materials are currently available as alternatives to autogenous bone for repair, substitution, or augmentation. Synthetic biomaterials include special glass ceramics described as bioactive glasses and calcium phosphates (CaPs) (e.g., calcium hydroxyapatite, HA; tricalcium phosphate, TCP; and biphasic calcium phosphate, BCP). The review of Dorozhkin [1] reported the important historical data for CaP bioceramics. In 1920, Albee [2] reported the first successful use of a calcium phosphate reagent for the repair of a bone defect in a human. More than 50 years later, the clinical use of a TCP preparation was reported in surgically created periodontal defects in animals and the use of dense HA as immediate tooth root replacements. In the early 1980s, synthetic HA and β-TCP became commercially available as bone substitute materials for dental and medical applications [3].
The term BCP describes a bioceramic that consists of a mixture of HA and β-TCP. The first studies on BCP showed that the bioactivity of these ceramics might be controlled by manipulating the HA to β-TCP ratios [4]. Subsequently, studies focused on BCP led to the significant increase in manufacture and use of commercial BCP bioceramics as bone substitute materials for dental and orthopedic applications [5].
Then, many studies were performed on CaP and especially calcium orthophosphate (Table 4.1). A large review of the chemical processing, manufacturing, biological properties, and applications of calcium orthophosphate was recently published [6]. CaP of pure HA, pure β-TCP, or BCP is achieved after sintering biological apatite or synthetic apatite obtained either by precipitation or hydrolysis. The BCP composition (HA to β-TCP ratio) obtained after sintering depends on the calcium deficiency of the unsintered biological or synthetic apatite and temperature [7]. The presence of other ions during the preparation of the unsintered calcium-deficient apatite (CDA) can also affect the HA and β-TCP or BCP sintering.
The sintering of commercial CaP reagents (labeled as “hydroxyapatite” or “calcium phosphate, tribasic” or “tricalcium phosphate”) above 900 °C was shown to result in pure HA, pure β-TCP, or BCP (Table 4.1).
Recent developments related to CaP scaffolds including improvements in terms of engineering chemistry, surface properties, microstructure, and porosities, which lead them to be considered as being bioinstructive rather than osteoconductive scaffolds, have opened up new opportunities for bone regenerative technologies [8]. Not only are some of these CaP bioceramics scaffolds osteoinductive in their own right, but evidence also supports the hypothesis that specific engineering bioceramics have a direct influence on the differentiation and proliferation of human mesenchymal stem cells (hMSCs). Tissue engineering, new bioactive molecules, and new surgical technologies increase the potential application of CaP bioceramics as carriers of these cells and also as scaffolds capable of guiding the behavior of these cells and the efficiency of bone regeneration [8].
4.2 Definitions
4.2.1 Calcium Phosphate Bioceramics
For over 30 years, HA and related CaPs have been widely used in the field of biomaterials as bone graft substitutes [3, 6, 7, 9, 10]. These materials have clinical applications in orthopedic, spinal, and maxillofacial surgery. They are currently used in various forms, but macro-/microporous bioceramics are the most advanced products [11]. Bioceramics are manufactured from well-characterized CaP powders that are mixed with pore makers and sintered at elevated temperatures (e.g., 1,000–1,300 °C). Research has primarily focused on both the formulation of appropriate bioceramic chemistry and the optimization of the physical pore structure. Mastering the chemistry of CaP bioceramics is clearly crucial for reproducible and controlled production processes but also for ensuring the adequate biological response upon implantation in bone tissue. These materials have been considered as bioactive and osteoconductive as they bond directly to bone tissue without an interstitial fibrous tissue layer. Their bioactivity is related to the solubility of CaP in physiological media. Several groups have shown that biphasic CaP bioceramics composed of HA and β-TCP represented the optimal formulation in terms of bioactivity. The TCP phase is soluble and leads to a release of calcium and phosphate ions which saturate local body fluids and precipitate a biological apatite onto the less soluble HA crystals [6, 12, 13].
4.2.2 Injectable Calcium Phosphate Bioceramics and Putties
CaP bioceramic granules associated with hydrosoluble polymers are at present extensively used [14]. Different combinations have been proposed with polymers such as gelatine, collagen, fibrin, demineralized bone matrix, hyaluronic acid or synthetic polymers such as poloxamer, and cellulose derivatives. To date, several injectable biomaterials have been developed. Some of these injectable bone substitutes are made of CaP hydraulic cements that harden in the bone defect [15–17]. Others are composed of CaP granules suspended in hydrogel, as they are the most interesting carriers used for the development of injectable bone substitute.
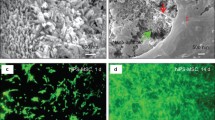
MBCP Gel is a non-self-hardening injectable biomaterial. It is composed of BCP granules associated with a hydrosoluble polymer. These materials have been shown to be perfectly biocompatible and potentially resorbable, and thanks to their initial plasticity, they assume the shape of bone defects very easily, eliminating the need to shape the material to adjust it to the implantation site [14, 18]. MBCP Gel does not have the mechanical properties of hydraulic bone cements. However, bone cells are able to invade the spaces created by the disappearance of the polymer carrier. Bone ingrowth takes place all around the granules at the expense of the resorption of the BCP granules (Fig. 4.1). In time, the mechanical properties are increased due to the presence of the newly formed bone. Numerous reports both in vitro and in vivo have confirmed the efficacy and performance of this concept for an injectable bone substitute used in bone reconstruction [14, 18–20].

MBCP Gel (In’Oss™). Human bone regeneration after revision surgery of nonintegrated dental implant, 8 months. SEM showing in grey the newly formed bone and in light grey the residual bioceramics particles integrated in the regenerated bone
IBS2 [21, 22] is a self-hardening composite. The BCP granules are associated with silanized HPMC-Si hydrogel. The guiding principles of silanized HPMC-Si hydrogel are its hydrophilic and liquid properties (it is viscous before being mixed with the CaP load and injection) and its pH-controlled reticulation process [23, 24]. The silanized hydrogel/CaP composite presents self-reticulation properties, due to the change in pH as a catalyst and without an exothermic effect. Once in the implantation site, in contact with the biological buffer liquids, a chemical reaction without additive and without any catalyst allows bridging and reticulation between the various macromolecular chains.
Prior to cross-linking, the composite is an injectable viscous liquid that hardens in the bone defect forming a gel loaded with BCP ceramic particles. IBS2 can entirely fill and remain in the bone defects. The BCP particles provide bioactivity supporting the bone healing process by osteoconduction. The cross-linked HPMC-Si hydrogel provides intergranular spaces for bone ingrowth. However, the jellification before blood diffusion delays osteoconduction of the BCP particles, and cells and tissue colonization at the expense of the composite.
Jellification is an important property of this material. It prevents the material from being washed out from the bleeding transplant site, after implantation. For an injectable bone substitute to maintain the bioceramic granules in unclosed cavities, the reticulation must increase the density of the material, reduce the dissolution or degradation of the polymer, and delay diffusion of the biological fluid and cell colonization [24].
The advantage of ready-to-use mixtures is their easiness of use and the reproducibility of the final material. Their kinetics for osseous reconstruction can be fast because of the many intergranular paths. These materials have relatively few intrinsic primary mechanical properties, even if the vehicles used harden by reticulation. Achieving mechanical properties is secondary to rapid physiological bone ingrowth.
BCP/fibrin glue: The association of bioceramics (TricOs®) and fibrin sealants may be interesting for the clinical applications of composite bone substitutes [25, 26]. Indeed, CaP granules are not easy to handle, are limited to filling bone cavities, and are not available for bone apposition. In addition, adding bioactive factors can improve the performance of bioceramics. In this regard, the adjunction of a binding agent, such as fibrin glue, improves the stability of the granules at the site of implantation and provides the scaffold effect of bioceramics with the additional osteogenic property. Fibrin-CaP composite could be obtained by mixing Baxter’s fibrinogen, the thrombin components of fibrin sealant (Tisseel® Baxter BioSciences BioSurgery), and TricOs® granules [27]. Macroporous Biphasic Calcium Phosphate TricOs® is a mixture of HA/β-TCP in a 60:40 ratio. Granules of 1–2 mm in diameter presenting both macroporosity (50–55 %) and microporosity (30–35 %) are used. To enhance the working time, a low thrombin concentration (4 U) is used. The Tisseel/TricOs volume ratio is 1 to 2. Numerous preclinical studies have been performed in rabbits and goats, both for biocompatibility and biofunctionality, using, for example, sinus lift augmentation and bone filling in long bone. Histology, histomorphometry, and X-ray microtomography have demonstrated the osteogenic properties of the composite [27].
Calcium phosphate cements: The need for a material for minimally invasive surgery (MIS) prompted the development of a concept for self-setting injectable CaP cement (CPC) as bone substitute. Currently, several CPCs are commercially available and more are being investigated. LeGeros et al. first introduced the concept in 1982 [15], and the first patent was obtained by Brown and Chow in 1986 [16]. All current CPCs are reported to have good mechanical properties and reasonable setting times. However, after setting, these materials remain dense and do not provide rapid bone substitution because of the lack of macroporosity. Numerous studies have reported the applications of currently available commercial CPCs [1, 17]. New BCP-based CPCs have recently been developed [28]. The MCPC consists of multiphasic CaP phases, including BCP. In vivo, the components of the cement resorb at different rates, allowing the formation of interconnecting macroporosity, thus facilitating bone ingrowth and substitution of the cement with the newly forming bone [28].
The powder component is essentially made of a settable and resorbable matrix (which includes α-TCP, stabilized amorphous CaP (s-ACP), and monocalcium phosphate monohydrate (MCPM)). A sieved fraction of macroporous BCP granules ranging between 80 and 200 μm in diameter are incorporated into the matrix. The cement liquid is an aqueous solution of Na2HPO4.
After setting MCPC in distilled water at 20 °C, the mechanical properties in compression of such materials were 10 ± 2 MPa at 24 h and 15 ± 2 MPa after 48 h. The cohesion time for injectability was reached after 20 min. Animal models of critical size defects in rabbit epiphyses or goat vertebral bodies demonstrated the performance and efficacy of CPC. MBCP granules act as a scaffold for bone osteoconduction, and resorption of the ACP content of the cement allowed macroporosity and bone ingrowth between and at the surface of the BCP granules, extending to the core of the implanted site. The cement matrix dissolved as expected, forming an open structure for cell colonization and bone ingrowth at the expense of the self-setting bone void filler [7, 28].
4.2.3 Fundamental Physicochemical Properties
4.2.3.1 Resorption
CaP bioceramic resorption [29] is the process by which resorption cells such as macrophages and osteoclasts break down the biomaterials and release the ions, resulting in a transfer of calcium and phosphate from the bioceramic to the blood [30]. This active process undertaken by the cells is equivalent to bone remodeling. The process is largely associated with the degradation of the bioceramic [6, 31] by biological fluids, the mechanical stress of the implantation site, releasing smaller particles. In the inflammation process, the size of the particles has a strong influence on dissolution [32], leading to the conclusion that resorption is dependent on the dissolution.
4.2.3.2 Dissolution
The solubility of CaP phases is mainly related to their chemical composition and crystal properties [3, 6, 29, 33, 34]. Different solubility product constants (K sp) have been reported for synthetic or biological CaP compounds, as shown in Table 4.1 [6]. The solubility is affected by cationic or anionic substitutions in the apatite lattice. For instance, carbonated or CDA are more soluble than fluoroapatite (FAP). Comparative dissolution in acetate buffer provided the following order of solubility: bone >> enamel >> β-TCP > HA. β-TCP has been found to dissolve faster in physiological solutions, as well as exhibiting a greater rate of dissolution or degradation than HA, when implanted in heterotopic or ectopic sites. Depending on the HA to β-TCP weight ratios, the solubility of BCP ceramics will be more similar to that of β-TCP or HA. The dissolution of CaP ceramics is also affected by its porosity and particle size. Increasing the porosity greatly enhances the surface area in contact with fluids and, thus, leads to a faster dissolution rate. As shown in Fig. 4.2, CaP ceramics exhibit macropores with diameter sizes ranging from 200 to 600 μm. While macropores are well interconnected, they permit the percolation of fluids, cells, and tissues within their structure. As illustrated in Fig. 4.2b, some ceramics may also exhibit a microporous surface. Spherical CaP grains appear bounded by necks leaving tiny pores approximately 0.1–1 μm in size. This remaining microporosity results from incomplete sintering of ceramics, especially when poorly crystalline precursor CaP powders and low sintering temperature and time (e.g., 1,000–1,200 °C for 1–10 h) are used. The lower temperature of sintering has a significant role in the formation in lattice defect. The lattice defect is particularly involved in the process of dissolution [32] explaining the large difference in the solubility of different HA scaffolds. According to the crystal size, lattice defect, and active cell resorption, the entire CaP can be resorbable. Only the kinetics differs according to time. A small-sized HA crystal with lattice defect is more resorbable than large, high crystalline TCP for example.

(a) MBCP+, Micro- and Macroporous Biphasic Calcium Phosphate, macropores. (b) MBCP+, Micro- and Macroporous Biphasic Calcium Phosphate, micropores
4.2.3.3 Absorption
The degradation and dissolution processes release high levels of calcium and phosphate ions into the extracellular fluid as the osteoclasts tunnel into the mineralized bone. Contrarily to degradation and elimination of some biomaterials, CaP ceramics elements released are absorbed during the physiopathological processes during bone regeneration. The released Ca and PO4 ions are precipitated at the surface of the residual crystals, and secondary nucleation and hetero epitaxic growing processes have been reported [11, 13]. This process has also been observed in Bioglass by Larry Hench [33], and the basis of bioactivity has been well documented by Kokubo using simulated body fluid incubation [34].
4.2.4 Fundamental Biological Properties
4.2.4.1 Osteointegration and Osteocoalescence
All CaP ceramics have been found to be biocompatible. HA ceramics are considered as non-resorbable, while β-TCP is resorbable based on the amount of implant left as a function of time. It is now generally accepted that CaP ceramics are bioactive and osteoconductive. Bioactivity is a property of the ceramic surface that induces biological integration of soft and hard living tissues. The core mechanism of bioactivity is the partial dissolution and release of ionic products in vivo, elevating local concentrations of calcium and phosphate and precipitating a biological apatite on the surface of the ceramics. This process of dissolution/precipitation has been studied in detail using transmission electron microscopy (TEM) of ceramics implanted in ectopic or heterotopic sites. The BCP grains partly dissolve in body fluids leading to the precipitation of tiny apatite crystals on their surface or between the grains. TEM studies have shown that these apatite crystals were similar to bone apatite in size, shape, and electron diffraction patterns [11]. The abundance of the apatite microcrystals associated with large grains of ceramics appeared to be directly related to the HA to β-TCP ratio of BCP ceramic implants. A higher amount of β-TCP gave a greater amount of precipitated apatite crystals. These microcrystals were identified as carbonate-containing apatites that are associated with an organic matrix similar to bone.
This surface precipitation may incorporate various proteins and growth factors present in the microenvironment, which may subsequently promote cell attachment and function. The bioactive ceramics are assumed to have a surface phase biologically equivalent to bone mineral. It suggests that osteoblasts are attracted to this layer and produce bone extracellular matrix leading to bone apposition (osteoconduction), rather than fibrous tissue encapsulation of ceramics. This “bone bonding” has also been called osseocoalescence [35], a better definition to explain the chemical bonding between CaP bioceramics and bony crystals.
4.2.4.2 Osteoconduction
In 1991, Damien described osteoconduction as the ability of a substitute (graft or material) to promote development of vascular and osteoprogenitor cells from the recipient site [36]. In 1998, Davies described osteoconduction as the process by which the bone is directed into the material structure, pore channels, from the surface of materials by an invasion of differentiated oestogenic cells [37]. This specific integration of the surface of a substitute in direct contact with the bone, without the interposition of fibrous tissue, is called osteogenesis link [37]. In 1999, Cornell defined osteoconduction as the passive ability of a material to promote bone growth, and which supports continuity or cellular and vascular invasion [38]. In 2001, Albrektsson described osteoconduction as bone growth on a surface. An osteoconductive surface allows bone ingrowth into the pore channels and on its surface [39].
4.2.4.3 Osteogenicity and Osteoinduction
Osteoinductivity is the ability of a material to induce osteogenesis and is demonstrated by bone formation in non-osseous (heterotopic) sites. Osteoinductive factors have previously been associated only with bone morphogenetic proteins (BMPs) present in bone matrix. However, many studies have reported osteoinductive properties associated with biomaterials. Several factors that contribute to the osteoinductive property of a material include the animal model, implantation sites, and biomaterial properties [40–44]. Biomaterial properties include composition, surface roughness, and geometry (concavities, porosities). To improve the biological properties of biomaterials and bone substitute in order to optimize the healing of bone critical size defects, it is necessary to evaluate their ability to induce osteogenesis in ectopic sites and to have a complete physicochemical characterization. For example, the specific surface area of the bioceramics crystals is generally not evaluated or reported in the articles in relation with CaP scaffolds associated with MSCs, as reported by Gibson [8]. The lack of information, the controversial studies, and the semantic aspect of osteogenicity or osteoinduction hamper the correct evaluation of intrinsic osteoinductive properties of CaP bioceramics.
In 1889, Senn reported that the implantation of decalcified dog bone promoted healing of large-bone defects [45], but the work was difficult to reproduce [46]. In 1931, Huggins observed an ectopic ossification after implantation of soft tissue (bladder wall) in the superficial muscle of the abdomen (rectus abdominis) of adult dogs [47]. He found an osteoid tissue 16 days after implantation, but did not find a mineralized bone tissue. From day 18 to 26 post implantation, he observed a characteristic bone tissue (tissue and cell components), formed by intramembranous ossification. This type of structure is generally present in the bones of the skull, shoulder blades, and the ilium [48]. During the past 30 years, Levander found ossification in muscle tissue after injection of extract of pure alcohol [49, 50]. In 1958, Bridges observed formation of bone and cartilage in nonskeletal tissue (kidney capsule, subcutaneous) after implantation of devitalized tissue or tissue extracts (epiphyseal cartilage, bone fragments) [51]. Urist and McLean in 1952, training in ectopic anterior chamber of the eye, described ectopic bone formation [52]. Urist described induced bone formation in ectopic sites using decalcified bone matrix in several species [53].
In 1968, Friedenstein defined osteoinduction as the “induction of undifferentiated inducible osteoprogenitor cells that are not yet committed to the osteogenic lineage to form osteoprogenitor cells” [54]. In 1987, Wilson-Hench described osteoinduction as the process by which osteogenesis is induced [55]. In 2001, Albrektsson described the term “osteoinduction” by undifferentiated pluripotent primary cells that are stimulated in one way or another to grow in an osteoprogenitor lineage [39].
4.3 Smart Scaffolds
4.3.1 Scaffolds and Cells Combination
CaP in bone mineral is not a pure HA but a carbonate-substituted apatite with other minor constituents. Current commercial CaP-based biomaterials consist of HA, β-TCP, biphasic CaP, BCP (an intimate mixture of HA and β-TCP), and polymer/CaP composites. Physical forms include granules, blocks, scaffolds, cements, and coatings on orthopedic and dental implants. Numerous CaP scaffolds have received the CE mark, or FDA approval. Given that the physicochemical characteristics impact directly or indirectly on the bioactive properties of biomaterials, it is essential to correlate them with their effect in vivo. A panel of biomaterials available on the market (based on HA and β-TCP) have been studied in terms of surface area, hydrophilicity, porosity, zeta potential, crystalline phases, and density. We have performed total chemical and structural characterization of 12 commercial products (granules). The characterization was assessed by:
-
Scanning electron microscopy (SEM) to characterize the surface morphology and check the homogeneity and the presence of both micropores and macropores
-
Specific surface area (SSA) (by BET method) to evaluate the available surface for protein
-
Mercury porosimetry to measure the porosity
-
X-ray diffraction (XRD) in order to check the nature and the proportion of the crystalline phases as mentioned by the manufacturer
-
Permeability qualitatively evaluated by methylene blue absorption
The results (Tables 4.2, 4.3, and 4.4) highlight the differences in the properties of commercial CaPs and demonstrate how the quality criteria required for such bone substitutes are based on biomimicry. Pores distribution may be a more relevant quality criterion and it is often not discussed in the literature, even at times concerning incorrect HA to TCP ratio. Only 4 products of the 12 tested are constituted with both essential macropores and micropores: MBCP, MBCP+, Calciresorb 35, and BCP Bicalphos. These chemical differences in micro- and macrostructure provided controversial results in terms of resorption/absorption, osteogenic/osteoinductive properties, and finally performance in bone regeneration [56].
Osteoinductivity in CaP biomaterials can be introduced in one of two ways:
-
First, by designing the CaPs with appropriate geometry and topography (combined macroporosity, microporosity, and concavities) that will entrap and concentrate the circulating growth factors (e.g., BMPs)
-
Second, by combining the CaP biomaterials with growth factors (BMPs, mesenchymal cells) and bioactive proteins (collagen, OPs, peptides based on osteonectin) or by seeding chondrocytes
The exact geometrical factors and the way to reproducibly obtain them are still unknown. The appropriate dosage of growth factors, mode of incorporation, and timed release remain to be determined.
The concept of introducing osteoinductive CaP biomaterials is an exciting one. Such materials will eventually replace the use of autografts and allografts with their attendant shortcomings. Numerous pieces of evidence indicate that the intrinsic MSC capacity to activate endogenous regenerative mechanisms and to recruit host cells in an ectopic bone formation model is critically dependent on MSC technology but also the physicochemical and structural properties of the scaffolds [57]. Nonetheless, for the success of the MSC transplant, the nature and the structure of scaffolds onto which cells are seeded are very critical. In addition to being a three-dimensional carrier for the cells, and a matrix with the correct shape for new tissue to form within, scaffolds are crucial in determining the optimal microenvironment for the cells to fully express their regenerative potential. A large collaborative project of the seventh framework program (topic HEALTH-2009-1.4.2 on Regenerative Bone defects using New biomedical Engineering approaches, REBORNE) [58] explores these scientific and clinical fields. The main objective is to develop smart scaffolds that stimulate bone tissue formation in combination with adult stem cells for regenerating bone defects in orthopedic and maxillofacial surgery.
We have optimized the new scaffolds based on a micro-/macroporous concept of MBCP, with a microstructure highly suitable for tissue engineering techniques and showing improved osteogenic properties. In different animal models, a mixture of MBCP granules and total bone marrow appeared to be the most efficient, amongst all the materials tested for bone substitution in difficult circumstances like irradiated areas and radionecrosis [59, 60].
The development of CaP ceramics for use in bone grafts involves a better control of the process of biomaterials resorption and bone substitution. Bone graft biomaterials are largely represented by CaP HA, TCP, and biphasic CaP, MBCP. The concept based on biphasic CaP ceramics is achieved by an optimum balance of the more stable phase of HA and more soluble TCP. The material is soluble and gradually dissolves in the body, leading to the formation of new bone as it releases calcium and phosphate ions into the biological medium [5]. These bioceramics are largely used for bone reconstruction and will be optimized for combination marrow during surgery or for bone tissue engineering using stem cells. We have optimized matrices in terms of their physicochemical and crystal properties, in order to improve cell colonization and to increase the kinetics of bone ingrowth. The fast cell colonization and resorption of the material are associated with the interconnected macropore structure, which enhances the bone resorption substitution process. The micropore content involves diffusion of biological fluids and suitable absorption surfaces for circulating growth factors. A difference of only 10 % of the amount of micropores into the CaP bioceramics improves the permeability and adsorption of proteins of more than 40 %.
Our work developing smart scaffolds for tissue engineering [12, 41] was based on the concept of MBCP technology. Interconnected Micro- and Macroporous Biphasic CaP ceramic (MBCP+, CE mark, and FDA 510k, Biomatlante SA France) was an improvement in the microporous and macroporous CaP bioceramic developed 20 years ago [5]. Briefly, CDA was associated to a mixture of selected particles of porogen. After isostatic compaction, the block was sintered according to a specific process of sublimation/calcination at low temperature. The low sintering temperature has the advantage of preserving the high micropore content and smaller crystal size, in addition to a higher sintering temperature. The bioceramics were then characterized using X-rays, FTIR, X-ray microtomography, permeability, Hg porosimetry, BET specific surface area, mechanical testing, and SEM. The crystal structure at the nanoscale was observed and analyzed using high-resolution transmission electron microscopy (hrTEM) and electronic diffraction (ED). The granules of MBCP+ have been tested in several preclinical studies in goats, rabbits, and rats, with or without cell addition (total bone marrow, MSCs), in critical size defects of femoral epiphysis and non-bony sites to test osteogenicity/osteoinductive properties.
X-ray diffraction identified the HA and β-TCP content despite the molecular mixture in the single crystal (MBCP technology used the mechanical combination HA and TCP crystals separately). The HA to TCP ratio was 20:80 (Fig. 4.3a, b). No trace of other sources of CaP or foreign species could be observed by FTIR. Using hrTEM of a single crystal of HA/TCP, we were unable to observe separate crystals of HA or TCP. The single crystal observed was a molecular mixture (nano-crystallographic domains) consisting of the biphasic compound (Fig. 4.4). Convergent Beam Electron Diffraction had insufficient resolution to characterize the precise HA or β-TCP domains, but the two crystallographic parts were intimately associated into single crystals.

MBCP+, Micro- and Macroporous Biphasic Calcium Phosphate. (a) XRD, (b) FTIR. FTIR confirms high purity of HA and TCP without any carbonate

hrTEM showing lattice place plane of HA/TCP. Numerous grain boundaries are observed between BCP crystals (arrow)
The combination of chemistry and microstructure has also been studied by Yuan [44]. The study confirmed the essential role of the microstructure, that the smaller crystals displayed high microporosity, and that there was greater bone formation when combined with MSCs. The data were obtained with TCP and BCP; the best results related to the higher content of TCP. In this study, the pure TCP contained 5–10 % HA, corresponding to a BCP with a low HA ratio.
The smart scaffold we developed for tissue engineering (MBCP+ ™) has the following characteristics: the crystal size is 0.5 μm and the SSA (specific surface area) 6 m2/g for MBCP+. The SSA difference in bioceramics (sintered CaP) (Table 4.2) showed a large range, from less 1 to 6 m2/g. This involved high difference in the adsorption capacity of non-collagenic proteins, growth factors, adhesion molecules, etc. For example, with SSA of 6 m2/g, the adsorption capacity was six times higher than SSA of 1 m2/g, or >1,000 % comparing to SSA <0.5 m2/g.
The compression test result is 4 MPa. The porosity consists of 19.6 ± 2.4 % macropores (>100 μm), 39.8 ± 3.1 % mesopores (5–100 μm), and 40.6 ± 3.2 % micropores <5 μm, for a total porosity of 73 %.
Numerous concavities on the granules increased the developed surface for cell colonization and seem to support higher osteogenic cell differentiation and spreading. The larger amount of newly formed bone appearing in the concavities was demonstrated by human alveolar pocket filling after 4 months of implantation (Fig. 4.5).

Light microscopy, sinus lift after 4 months of implantation showing newly formed bone (large arrow, pink) formed at the expense of the MBCP+ granules (*) particularly into the concavity of them (light arrow)
The advantage of a smart scaffold includes faster bone ingrowth into the macropores and the concavities, as observed in short-term implantation of MBCP+, relative to classical MBCP. However, after 12 weeks of implant in rabbit preclinical models, no statistical difference was observed between the two implant types. The rate of resorption was higher for MBCP+, 17 % versus 12 % at 6 weeks and 19 % versus 17 % after 12 weeks (no significant difference). These properties can be advantageous for tissue engineering scaffold technologies.
This higher permeability and absorption ability were mainly due to the distribution of pore size, particularly mesopores, with the high micropore content representing around 40 % of the total porosity. After implantation, bone ingrowth was observed at the expense of the bioceramic, and newly formed bone progressively replaced the bioactive material, followed by Haversian bone remodeling [5]. In vitro 3D MSCs/BCP constructs were formed after a few days of culturing the BCP particles and MSCs. In the proliferative medium, we measured higher BSP and BMP-2 expression than the cells on TCP plates alone, demonstrating the importance of the 3D scaffold for osteogenic expression [39].
The in vivo experiments indicated that the high cell colonization by osteogenic cells is due to the interconnected and microporous structure associated with higher solubility and 3D environment [61]. Moreover, a previous study comparing the equivalent macro- and microstructures of different calcium phosphate bioceramics (HA, TCP, or BCP 60/40 and BCP 20/80) showed that the best scaffold for tissue engineering was a 20:80, thanks to the combination of stem cells cultivation and expansion, followed by implantation in a non-bony site [62]. Osteogenic or osteoinductive properties of CaP ceramics with an optimal micro- and macroporosity have also been demonstrated without cell combination, after implantation in a non-bony site (muscular area) [40, 41, 43]. Ripamonti has also postulated that the geometry of the material (concavity) is a critical parameter in bone induction [42, 63]. The events and the origin of these important osteoinductive properties are the dissolution of the most soluble phase and the release of calcium and phosphate ions, followed by the precipitation of biological apatite leading to concentration of local growth factors [41]. The osteoprogenitor cells may in turn recognize the bone-like apatite layer formed in vivo by dissolution-reprecipitation on the material, leading to production of mineralized bone.
The kinetics of bone ingrowth by osteogenic cell differentiation needs to develop inside the macropores. Without macropores and mesopores, these processes are unable to occur within the implants. The association of dissolution at the crystal level, the diffusion of the biological fluid into the micropores, and the resorption by macrophages and osteoclastic cells of the materials at the surface and inside the macropores involve a progressive bone substitution of the materials by physiological well-vascularized bone. This is the common process of resorption-absorption/bone substitution of the Micro- and Macroporous Biphasic Calcium Phosphate ceramics. The intimate mixture of the process developed for smart scaffold MBCP+ gave a unique and original property, contrarily to some others BCP described in the literature using a mechanical mixture of HA on one side and β-TCP on the other [6].
4.3.2 Scaffold for Drug Delivery
CaP bioceramics have frequently been proposed for the adsorption of bioactive factors and for drug delivery systems. A recent study by Smucker et al. [64] was the first to demonstrate enhanced posterolateral spinal fusion rates in rabbits, using a synthetic peptide (B2A2-K-NS) coated on to microporous granules of BCP, with a 60:40 HA to TCP ratio. Different concentrations of the peptide (a synthetic receptor-targeted peptide that appears to amplify the biological response to rhBMP-2) were tested. This study provided more evidence of mature/immature bone ingrowth across the inter-transverse process spaces than the controls did. Microporous and macroporous biphasic CaP granule bioceramics for peptide adsorption and local delivery seem to be a good compromise for future associations of osteoconductive/osteogenic properties for such bioceramics and for the osteoinductive properties of peptides and growth factors.
Antibiotics may also be candidates to be delivered by this technology. It is common practice for surgeons to mix antibiotics with bone grafts when treating infected bone defects or for preventing infection after surgery [65]. Local delivery of antibiotics is both pharmacologically more effective and safer. If properly formulated, bioactive cements have been shown to be an ideal carrier for local delivery of antibiotics [66, 67]. New CPC has been specifically engineered to have microporosity, macroporosity, and resorbability for optimal cell adhesion, cell migration, and bone formation. Recently, the MCPC® reported in this paper was associated with delivery of gentamicin [68].
The gentamicin release profiles from the cement samples with different setting times were quite similar. Both cement groups showed an initial burst of gentamicin release in the first 24 h. After the initial burst, the release rate slowed significantly and stayed relatively constant between day 7 and day 28 (the endpoint). The amount and rate of the initial burst release were affected by the cement setting time. The release of gentamicin from the cement allowed to set for 1 h showed greater variation than the cement allowed to set for 24 h. Within the first 24 h, approximately 72 % of the gentamicin was released from the cement with 1 h, compared to the slower release of the gentamicin from the cement with a 24-h set time (approximately 51 %). By 28 days, around 87 and 76 % of the gentamicin had been released from the cements that had set for either 1 h or 24 h, respectively. The gentamicin release rates from both the 1-h and 24-h set-time samples were almost constant after day 7, averaging 59 μg/day for the cement with a 1-h set time and 87 μg/day for the 24-h set time. Therefore, in our release system, these constructs are capable of releasing gentamicin concentrations of 12 and 17 μg/ml on a daily basis for the 1-h and 24-h set-time cement samples, respectively. This is more than one order of magnitude greater than the minimum inhibitory concentration (MIC) for reference strains of S. aureus, which is in the range of 0.12–0.25 μg/ml [69].
It was interesting to note that the cement without gentamicin showed a decrease in ultimate compressive strength during setting, from 24 to 48 h in phosphate-buffered saline at 37 °C. The ultimate compressive strength dropped from 5.5 to 3.87 MPa indicating that the cement had dissolved. When the gentamicin was present, the cement showed an increase in both the strength and modulus, when the set time was extended from 24 to 48 h. It appeared that the addition of gentamicin might have delayed the dissolution of the cement, while allowing it to continue to set and thus further increase its mechanical strength.
Due to its unique preparation method and bioresorbability, the bioactive cement employed in this study may be effective as both a bone graft substitute and a carrier for the local delivery of antibiotics to prevent or treat infections. Ideal bioactive cement will initially release a clinically effective amount of antibiotics, maintain a steady release of a safe dose over an extended period, and retain no residual amount of antibiotics at the end of the desired treatment time. As demonstrated in this study, the MCPC™ bioactive cement released over 50 % of the loaded gentamicin per cylinder, that is, 7.5 mg in the first 24 h. A steady release of a therapeutically significant amount of 60–90 μg of gentamicin per day was maintained up to 28 days. As the MCPC™ is engineered to bioresorb and quickly develops a macroporous structure, the remaining amount of 2–4 mg of gentamicin per set-time sample is expected to discharge completely as the bioactive cement resorbs. The MCPC™ resorbable bone substitute has demonstrated its potential to be used as a carrier for the local delivery of gentamicin. Future studies will expand the investigation to evaluate the release profile and mechanical properties of this bioactive cement when loaded with other antibiotics, such as tobramycin and vancomycin.
4.4 Conclusions and Future Prospects for Calcium Phosphate Materials as Bone Substitutes
Advanced technologies for developing smart osteogenic scaffold bioceramics for tissue engineering involve focusing on improving the efficacy of such matrices for further relevant surgical technologies, such as the combination with bone marrow for surgery or expanded stem cell in vitro for bone tissue engineering.
It has recently been shown that some porous CaP bioceramics induce ectopic bone formation after implantation into the muscles of large animals. These biomaterials have demonstrated the ability to induce bone formation after 6–12 weeks in muscular sites, without the addition of osteogenic cells or bone growth factors prior to implantation. Ectopic bone formation with Haversian structures was observed in close contact with the MBCP granules. Well-mineralized bone with mature osteocytes had formed on or between the granules. The ectopic bone showed trabeculae bridging the granules, restoring the bone architecture.
Although many groups have described induction of ectopic bone by biomaterials, it remains a subject of controversy because the mechanisms are poorly understood. In vivo studies have shown that materials should exhibit two features in order to induce ectopic bone: (1) a microporous surface and (2) a macroporous structure. Osteoinduction does not seem to be related to the chemistry of the material, as various types of bioceramic compositions have demonstrated ectopic bone formation. Osteoinduction by biomaterials also seems to be animal dependent and has so far only been observed in the muscles of large animals such as dogs, baboons, sheep, and goats. Several explanations have been proposed. First, CaP ceramics may concentrate bone growth factors from body fluids, which then trigger stem cells to form bone tissue. Second, the geometry of the material is a critical parameter in bone induction, and third, osteoprogenitor cells might in turn recognize the bone-like apatite layer formed in vivo by dissolution-reprecipitation on the material and produce mineralized bone. Other studies have proposed that low oxygen tension in the central region of the implants might provoke a dedifferentiation of pericytes from blood microvessels into osteoblasts. Microparticles released from low sintered ceramics might provoke a specific inflammatory reaction leading to osteogenesis, or the circulating progenitor cells might differentiate into osteoblasts following stimulation by the inflammatory cytokines released by macrophages. The process might be similar to the healing of bone fractures, where debris and fragments of bone are present. Nevertheless, the cascade of biological events leading to material osteogenesis remains unclear.
In the future, this intriguing property will benefit synthetic bone substitutes. Advanced CaP bioceramics with superior bone healing properties might replace biological bone grafting from materials such as autologous or demineralized bone. Much of the interest in the development and modification of the smart CaP bioceramics is based on improving the osteoconduction or the initial mechanical properties of bone substitutes. There is evidence to suggest that small-sized particles that are released into the microenvironment after implantation and degradation are then recognized as debris and promote an inflammatory reaction that recruits phagocytic macrophages and induces potential bone breakdown, a phenomena that can boost osteogenic cell differentiation [31]. Ongoing work is required to explore the modulation of inflammation, the optimization of the initial mechanical property for easy-to-use bioceramics, and expression of mechanotransduction, in order to develop more clinically relevant applications for synthetic bone graft.
If the smart bioinstructive CaP scaffold technology led to a higher efficacy of CaP scaffolds, it would allow further surgical applications in bone tissue regeneration. The mechanical properties required for bone ingrowth and bone remodeling and mechanotransduction must be explored to allow for development of new generation scaffolds [70].
References
Dorozhkin S (2013) A detailed history of calcium orthophosphates from 1770s till 1950. Mater Sci Eng C33:3085–3110
Albee FH, Morrison HF (1920) Studies in bone growth. Triple calcium phosphate as a stimulus to osteogenesis. Ann Surg 71:32–39
De Groot K (1983) Bioceramics of calcium phosphate. CRC Press Inc., Boca Raton
Legeros R, Guy D, John L (2009) Bioactive bioceramics, orthopaedic biology and medicine. In: Pietrzak WS (ed) Musculoskeletal regeneration, biological materials and methods. Humana Press, Totowa, pp 153–181
Guy D, Franck J, Pierre L (2009) The micro macroporous biphasic calcium phosphate concept for bone reconstruction and tissue engineering. In: Bikramjit B, Dhirendra SK, Ashok K (eds) Advanced biomaterials: fundamentals, processing, and applications. Wiley, Hoboken, pp 101–141
Dorozhkin S (2012) Calcium orthophosphates: applications in nature, biology, and medicine. Pan Stanford Publishing Pte Ltd., Singapore, pp 1–853
LeGeros RZ (1991) Calcium phosphates in oral biology and medicine, vol 15, Monographs in oral science. Karger, Basel
Gibson IR (2012) Calcium phosphate as scaffolds for mesenchymal stem cell. In: Ramalingam M, Ramakrishna S, Best S (eds) Biomaterials and stem cells in regenerative medicine. CRC Press, Boca Raton, pp 219–237
Bohner M (2000) Calcium orthophosphates in medicine: from ceramics to calcium phosphate cements. Injury 31:37–47
Hench LL, Thompson I (2010) Twenty first century challenges for biomaterials. J R Soc Interface 7(4):S379–S391
Daculsi G, Laboux O, Malard O, Weiss P (2003) Current state of the art of biphasic calcium phosphate bioceramics. J Mater Sci Mater Med 14(3):195–200
Daculsi G, LeGeros R, Nery E, Lynch K, Kerebel B (1989) Transformation of biphasic calcium phosphate ceramics in vivo. Ultrastructural and physicochemical characterization. J Biomed Mater Res 23:883–894
Daculsi G, LeGeros RZ, Heughebaert M, Barbieux I (1990) Formation of carbonate apatite crystals after implantation of calcium phosphate ceramics. Calcif Tissue Int 46:20–27
Daculsi G, Weiss P, Bouler JM, Gauthier O, Aguado E (1999) Biphasic calcium phosphate hydrosoluble polymer composites: a new concept for bone and dental substitution biomaterials. Bone 25:59–61
LeGeros RZ, Chohayeb A, Shulman A (1982) Apatitic calcium phosphates: possible restorative materials. J Dent Res 61:343
Brown WE, Chow LC (1987) A new calcium phosphate water-setting cement. In: Brown PW (ed) Cement research progress. American Ceramic Society, Westerville, pp 352–379
Niwa S, LeGeros RZ (2002) Injectable calcium phosphate cements for repair of bone defects. In: Lewandrowski K-U, Wise DL, Trantolo DJ, Gresser JD (eds) Tissue engineering and biodegradable equivalents. Scientific and clinical applications. Marcel Dekker, New York, pp 385–400
Daculsi G (2006) Biphasic calcium phosphate Granules concept for Injectable and Mouldable Bone Substitute. In: Vincenzini P, Giardino R (eds) Advances in science and technology, vol 49. Trans Tech Publications, Faenza, Italy, pp 9–13
Weiss P, Layrolle P, Clergeau LP, Enckel B, Pilet P, Amouriq Y, Daculsi G, Giumelli B (2007) The safety and efficacy of an injectable bone substitute in dental sockets demonstrated in a human clinical trial. Biomaterials 28:3295–3305
Daculsi G, Durand M, Fabre T, Vogt F, Uzel AP, Rouvillain JL (2012) Development and clinical cases of injectable bone void filler used in orthopaedic (Développement et cas cliniques d’un substitut osseux injectable en orthopédie). IRBM 33:253–261
Lapkowski M, Weiss P, Daculsi G, Dupraz A (1997) Composition pour biomatériau, procédé de préparation II Date de dépôt. CNRS Patent WO 97/059
Fellah BH, Weiss P, Gauthier O, Rouillon T, Pilet P, Daculsi G, Layrolle P (2006) Bone repair using a new injectable self-crosslinkable bone substitute. J Orthop Res 24(4):628–635
Fatimi A, Tassin JF, Quillard S, Axelo MAV, Weiss P (2008) The rheological properties of silated hydroxypropylmethylcellulose tissue engineering matrices. Biomaterials 29:533–543
Turczyn R, Weiss P, Lapkowski M, Daculsi G (2000) In situ self hardening bioactive composite for bone and dental surgery. J Biomater Sci Polym Ed 11(2):217–223
Le Guehennec L, Layrolle P, Daculsi G (2004) A review of bioceramics and fibrin sealant. Eur Cell Mater 13(8):1–11
Le Nihouannen D, Saffarzadeh A, Aguado E, Goyenvalle E, Gauthier O, Moreau F, Pilet P, Spaethe R, Daculsi G, Layrolle P (2007) Osteogenic properties of calcium phosphate ceramics and fibrin glue based composites. J Mater Sci Mater Med 18(2):225–235
Khairoun I, LeGeros RZ, Daculsi G, Bouler JM, Guicheux J, Gauthier O (2004) Macroporous, resorbable and injectable calcium phosphate-based cements (MCPC) for bone repair, augmentation, regeneration and osteoporosis treatment. Provisional patent 11/054 623
Daculsi G, Durand M, Hauger O, Seris E, Borget P, LeGeros R, LeHuec JC (2012) Self hardening macroporous biphasic calcium phosphate bone void filler for bone reconstruction. Animal study and human data. Key Eng Mater 493–494:703–713
Goyenvalle E, Aguado E, Legeros R, Daculsi G (2007) Effect of sintering process on microporosity, and bone growth on biphasic calcium phosphate ceramics. Key Eng Mater 333–334 (in press). Trans Tech Publication, Switzerland
Fellah BH, Delorme B, Sohier J, Magne D, Hardouin P, Layrolle P (2010) Macrophage and osteoblast responses to biphasic calcium phosphate microparticles. J Biomed Mater Res A 93(4):1588–1595
Basle MF, Chappard D, Grizon F, Filmon R, Delecrin J, Daculsi G, Rebel A (1993) Osteoclastic resorption of CaP biomaterials implanted in rabbit bone. Calcif Tissue Int 53:348–356
Daculsi G, Legeros RZ, Legeros J, Mitre D (1991) Lattice defects in calcium phosphate ceramics: high resolution TEM ultrastructural study. J Biomed Mater Res Appl Biomater 2:147–152
Hench LL (1994) Bioceramics: from concept to clinic. J Am Ceram Soc 74:1487–1510
Kokubo T, Takadama H (2006) How useful is SBF in predicting in vivo bone bioactivity? Biomaterials 27(15):2907–2915
Daculsi G, Passuti N (1990) Bioactive ceramics, fundamental properties and clinical applications the osteocoalescence process. In: Oonishi H, Heimcke G (eds) Ceramics in medicine, pp 3–10
Damien CJ, Parsons JR (1991) Bone graft and bone graft substitutes: a review of current technology and applications. J Appl Biomater 2(3):187–208
Davies JE (1998) Mechanisms of endosseous integration. Int J Prosthodont 11(5):391–401
Cornell CN (1999) Osteoconductive materials and their role as substitutes for autogenous bone grafts. Orthop Clin N Am 30:591–598
Albrektsson T, Johansson C (2001) Osteoinduction, osteoconduction and osseointegration. Eur Spine J 10(Suppl 2):S96–S101
Barradas Ana MC, Yuan H, van Blitterswijk CA, Habibovic P (2011) Osteoinductive biomaterials: current knowledge of properties, experimental models and biological mechanisms. Eur Cell Mater 21:407–429
Le Nihouannen D, Daculsi G, Saffarzadeh A, Gauthier O, Delplace S, Pilet P et al (2005) Ectopic bone formation by microporous calcium phosphate ceramic particles in sheep muscles. Bone 36(6):1086–1093
Ripamonti U, Crooks J, Kirbride A (1999) Sintered porous hydroxyapatites with intrinsic osteoinductive activity: geometric induction of bone formation. S Afr J Sci 95:335–343
Yuan H, Yang Z, De Bruijn JD, De Groot K, Zhang X (2001) Material-dependent bone induction by calcium phosphate ceramics: a 2.5-year study in dog. Biomaterials 22:2617–2623
Yuan H, Fernandes H, Habibovick P, de Boer J, Barrads AMC, de Ruiter A, Walsh WR, van Blitterswijk CA, de Bruijn JD (2010) Osteoinductive ceramics as a synthetic alternative to autologous bone grafting. Proc Natl Acad Sci 107:13614–13619
Senn NS (1889) On the healing of aseptic bone cavities by implantation of antiseptic decalcified bone. Am J Med Sci 98(3):219–243
Rengachary SS (2002) Bone morphogenetic proteins: basic concepts. Neurosurg Focus 13(6):e2
Huggins CB (1931) The phosphatase activity of transplants of the epithelium of the urinary bladder to the abdominal wall producing heterotopic ossification. Biochem J 25(3):728–732
Bronner ME, LeDouarin NM (2012) Development and evolution of the neural crest: an overview. Dev Biol 366(1):2–9
Levander G (1934) On the formation of new bone in bone transplantation. Acta Chir Scand 74:425–426
Levander G (1938) A study of bone regeneration. Surg Gynecol Obstet 67:705–714
Bridges JB, Pritchard JJ (1958) Bone and cartilage induction in the rabbit. J Anat 92(1):28–38
Urist MR, McLEAN FC (1952) Osteogenetic potency and new-bone formation by induction in transplants to the anterior chamber of the eye. J Bone Joint Surg Am 34-A(2):443–476
Urist MR (1965) Bone formation by autoinduction. J Sci 150(3698):893–899
Friedenstein AY (1968) Induction of bone tissue by transitional epithelium. Clin Orthop 59:21–37
Wilson-Hench J (1987) Osteoinduction. In: Williams D (ed) Progress in biomedical engineering. Elsevier, Amsterdam, p 29
Daculsi G, Fellah BH, Miramond T, Durand M (2013) Osteoconduction, Osteogenicity, Osteoinduction, what are the fundamental properties for a smart bone substitutes. IRBM 34(4):346–348
Ramalingam M, Ramakrishna S, Best S (eds) (2012) Biomaterials and stem cells in regenerative medicine. CRC Press/Taylor & Francis Group, Boca Raton, pp 1–546
Regenerative bone defects using new biomedical engineering approaches, REBORNE 2010–2014, 7th PCRD EC program. www.reborne.org
Espitalier F, Vinatier C, Lerouxel E, Guicheux J, Pilet P, Moreau F, Daculsi G, Weiss P, Malard O (2009) A comparison between bone reconstruction following the use of mesenchymal stem cells and total bone marrow in association with calcium phosphate scaffold in irradiated bone. Biomaterials 30(5):763–769
Lerouxel E, Moreau A, Bouler JM, Giumelli B, Daculsi G, Weiss P, Malard O (2009) Effects of high doses of ionising radiation on bone in rats: a new model for evaluation of bone engineering. Br J Oral Maxillofac Surg 47(8):602–607
Cordonnier T, Layrolle P, Gaillard J, Langonné A, Sensebé L, Rosset P, Sohier J (2010) 3D environment on human mesenchymal stem cells differentiation for bone tissue engineering. J Mater Sci Mater Med 21(3):981–987
Arinzeh TL, Tran T, McAlary J, Daculsi G (2005) A comparative study of biphasic calcium phosphate ceramics for human mesenchymal stem-cell-induced bone formation. Biomaterials 26(17):3631–3638
Ripamonti U (1996) Osteoinduction in porous hydroxyapatite implanted in heterotopic sites of different animal models. Biomaterials 17:31–35
Smucker JD, Aggarwal D, Zamora PO, Atkinson BL, Bobst JA, Nepola JV, Fredericks DC (2007) Assessment of B2A2-K-NS peptide coated on an osteoconductive granule in a rabbit postrolateral fusion model. In: Proceedings AAOS, San Diego, 12–14 Feb 2007
Hanssen AD (2005) Local antibiotic delivery vehicles in the treatment of musculoskeletal infection. Clin Orthop Relat Res 437:91–96
Sasaki T, Ishibashi T, Katano H, Nagumo A, Toh S (2005) In vitro elution of vancomycin from calcium phosphate cement. J Arthroplasty 20:1055–1059
Frutos P, Torrado S, Perez-Lorenzo ME, Frutos G (2000) A validated quantitative colorimetric assay for gentamicin. J Pharm Biomed Anal 21:1149–1159
McNally A, Sly K, Lin S, Bourges X, Daculsi G (2007) Release of antibiotics from macroporous injectable calcium phosphate cement. Key Eng Mater 333–334 (in press). Trans Tech Publication, Switzerland
Andrews JM (2001) Determination of minimum inhibitory concentrations. J Antimicrob Chemother 48(Suppl 1):5–16
Liedert A, Kaspar D, Blakytny R, Claes L, Ignatius A (2006) Signal transduction pathways involved in mechano transduction in bone cells. Biochem Biophys Res Commun 349:1–5
Acknowledgments
We would like to thank the 7th framework program HEALTH-2009-1.4.2 of the European Commission on Regenerative Bone defects using New biomedical Engineering approaches (REBORNE project).
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2014 Springer-Verlag Berlin Heidelberg
About this chapter
Cite this chapter
Daculsi, G., Fellah, B.H., Miramond, T. (2014). The Essential Role of Calcium Phosphate Bioceramics in Bone Regeneration. In: Ben-Nissan, B. (eds) Advances in Calcium Phosphate Biomaterials. Springer Series in Biomaterials Science and Engineering, vol 2. Springer, Berlin, Heidelberg. https://doi.org/10.1007/978-3-642-53980-0_4
Download citation
DOI: https://doi.org/10.1007/978-3-642-53980-0_4
Published:
Publisher Name: Springer, Berlin, Heidelberg
Print ISBN: 978-3-642-53979-4
Online ISBN: 978-3-642-53980-0
eBook Packages: Chemistry and Materials ScienceChemistry and Material Science (R0)