
Abstract
This study analyzes the modernization process of an Italian nursing home driven by the development and usage of software developed in-house. To clarify contradictory results regarding information technology performance in healthcare settings, this study points at the benefits gained by both the users of the software and the guests of the nursing home. This is done collecting both qualitative and descriptive quantitative data regarding the quality of life of the guests and the way operators are affected as result of the new tool adopted. Our study shows that bottom-up participatory design with autonomy, user friendliness and job simplification, and orientation toward guests, were the elements that concurrently generated a virtuous circle for the guests, the users and therefore the organization as a whole.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others

Keywords
Introduction
High-quality information management represents a focal priority in healthcare. Despite significant investments in information technology (IT) in the healthcare sector, the industry continues to struggle with poor outcomes [7]. Most research on IT-driven modernization focuses on sources of unsuccessful experiences [13], such as limited uses of technology or low perceived value [3] from the IT investment. In many cases though, information and data simply get mismanaged, neglected, or underused. This highly problematic scenario highlights the gap between what should happen in theory—as exemplified by studies that predict positive outcomes of Healthcare IT (HIT) [1] and what happens in practice.
Our study features the analysis of an experience at Fondazione Santa Clelia (FSC), an Italian nursing home that over the past decade has designed and implemented ABC, an IT tool to aid the provision and management of long-term care. The experience generated positive outcomes not only for the operators (see also Carugati et al. [5]), but also for the guests of FSC to the extent that this experience became the pilot study of a larger IT diffusion study with 100+ nursing homes using that subsequently adopted ABC. In the present study, we aim at presenting the software, its development process, and its usage in FSC. This analysis is critical to understand the elements that contribute in practice to the successful use of IT in healthcare settings.
Research Context and Methods
Research Context: Fondazione Santa Clelia
Fondazione Santa CleliaFootnote 1 (FSC) is a non-profit, Catholic, publicly accredited residential structure for the aged founded in 1982 and located in Vidiciatico, a small town near Bologna (Italy). A total of 85 guests benefit of FSC services, while 62 of them live at FSC (2009). The resident care philosophy that FSC adopts focuses more on animation and social activities, rather than on heavy use of pharmaceutical treatments. This choice is based on the belief that through social integration, guests can attain better standards of living [14]. The focus requires a high staff-to-guest ratio, which in FSC is 1 operator to 1.5 guests (ratio = 0.68). Labor costs account for 78 % of FSC’s operating expenses and making FSC among the most personnel-intensive residences for the aged of the Region Emilia-Romagna.
ABC Software
In 1999, following the input of a new general manager (GM) the first version of ABC was developed over the course of one year by a volunteer retired software engineer. Over time, the software engineer developed new functions in ABS following the emergent requests of the nursing personnel according to a modular logic. ABC’s modular structure supports daily care and offers a means to record and share behavioral and health information about the guests among all users: nurses, physiotherapists, clerks, doctors, and social animators. The system computes well-being indexes for each guest on daily basis with the aim of monitoring the quality and continuity of services and goals improvement. The data and information collected by the care personnel contain the following areas for each guest: (1) the personal data including the health and the life history; (2) the history of rehabilitation, socialization and animation; (3) the level of autonomy; (4) the information and data regarding the everyday life at FSC (meals, sleeps, falls, etc.). (5) the area of current wellbeing and health conditions; and (6) a synthesis of the objectives, measures and expected results of the different types of interventions, including the current individual plan of assistance (IPA). These areas are collected independently—not to interfere with daily work—but can be analyzed cross checking data (e.g., food with falls; gymnastic with sleep etc.)
Intervention Description
Before the introduction of ABC, the information existed in paper documents but it was almost impossible to analyze and use. Only administrative staff had access to computers. This is the reason why staff involvement was considered pivotal during the entire development phase. Moreover, the programmer was asked by the GM not to be pro-active, rather he was invited to rely on the input of the most available, enthusiastic or interested operators of FSC. The first prototype was developed with a group of nurses. The development approach was to computerize existing paper documents so that users could feel comfortable with the new electronic form. The second step was that of either eliminating useless information, or adding additional information, or both. As the software evolved, it became evident that the main advantage of ABC was the ability to provide access to all the information when it occurred. This continuous development approach was used in the course of the last 13 years to develop modules to support all the remaining protocols, processes and procedures with the involvement of all the professional profiles working in FSC. The system is still (in 2012) under development, albeit at a slower pace, and the users still play the main role in the development. Personnel, managers, and guests interviewed in multiple occasions declare the implementation to be a success with 100 % rate of adoption at FSC.
Data Collection
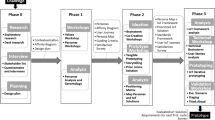
The qualitative data were collected during two field trips, in October 2008 and September 2009 for the purpose of involving all stakeholders multiple times in our data collection [2]. During the first round of data collection, we conducted semi-structured interviews with five people: the general manager, the software developer, an administrative assistant, and two nurses. These interviews lasted 60–150 min and helped us understand how the new IT tool had been developed.
The focus of the second visit was the usage of the tool. We interviewed ten employees (approximately 60 min each) about their daily use of ABC, including a nurse coordinator, five nurses, two social animators, a physiotherapist, and the administrative clerk responsible for the interface between users and the developer. Furthermore, we interviewed two guests who had moved to FSC before the development of ABC. Moreover, we undertook a field observation of the entire working day of a nurse. Finally we carried out two interviews with the GM and the software developer.
We collected the descriptive quantitative data regarding the operators and the guests for 1999 and 2009 (Table 1). To measure changes in guests’ mobility and autonomy, we used three internationally recognized parameters (Table 2). The Barthel index measures people’s ability to perform normal daily activities, such as eating or walking on a flat floor from 0 (severe, no self-sufficiency) to 100 (complete self-sufficiency) [12]. The Global Evaluation Functional index similarly attempts to define self-sufficiency, partial dependency, and total dependency. Its score varies from 0 (self-sufficiency) to 1,000 (maximum dependency) [8]. Finally, the Mini Mental State Examination measures disturbances to intellectual efficiency and the potential presence of deterioration [10] with a score between 0 (max impairment) and 30 (no impairment).
Data Analysis
The data analysis involved the comparison and cross checking, over time, of qualitative and descriptive quantitative data. All interviews were tape recorded, transcribed and translated from Italian into English by a person different from the authors of this manuscript. Interview protocols are available from the authors upon request and all interviewees provided verbal consent to use their data. The content of the interviews and field notes was analyzed using Nvivo software to aid the qualitative analysis [11]. To ensure that the system development activities and the development of the organization were grounded in the data, we coded for interconnected evidence of positive and negative experiences with ABC, acceptance or resistance of the system, and evidences of organizational impacts (either positive or negative) [9] with special focus on guests related activities and performances about well being and quality of life. The qualitative data reported by interviewees were then triangulated with the quantitative data extracted from the ABC system. The data analysis involved three cycles of coding according to Charmaz’s method [6]. Finally, we cross-checked our coding among authors to control for internal reliability of the analysis. Disagreements among coders were handled by double-checking with the interviewees, procedure that also helped with the external validity of subsets of the analysis, along with cross checking our results with the GM of FSC and through his agreement on the content of this paper.
Results: The benefits for Operators and Guests
Evidences from the Qualitative Analysis
Our qualitative investigation of the development (data collection—phase 1) and use (data collection—phase 2) of the ABC software reveals two main outcomes: (1) The software gradually responded to all the informational and operational needs of the organization, and (2) its use had tangible results for guests’ perceptions of their quality of life, managerial decision-making processes, and external perceptions of the quality of care. In brief, the software is widely used, and our interviewees perceive that this use leads to positive results. According to the GM, “through the use of ABC we were able to retain our employees longer, to have more money for social interventions rather than pharmacological treatments, and above all we have prolonged and improved the lives our guests.”
The employees of FSC were reticent to try a new technology, but through incremental development, they managed to gain considerable IT skills and now consider it an integral part of their work, rather than a mandated burden: “If I think how scared I was at the beginning … and now I could not live without it [ABC software]” (physiotherapist).This seemingly abnormal but positive use of HIT by the health professionals reflects the contribution of three factors that emerged from our analysis, which led to continuous, pervasive, value-adding use of ABC: (1) bottom-up design with autonomy, (2) user friendliness and job simplification, and (3) orientation toward guests.
Bottom–Up Design with Autonomy
The idea of having a software tool integrated into FSC’s daily activities came from the GM. However, the interviews confirm that the software was developed by the volunteer programmer by never including anything in the program that had not been demanded by staff. Furthermore, the GM enforced a positive cycle that always provided sufficient slack resources to include enough personnel in the development process: Take the physiotherapists for example… never before existed the concept of knowing over years how much bike a guest does, who does more often or in which days it is done. I wouldn’t know what is important so all these requests and the input tables came from the operators. Then of course we had to standardize to make data entry similar for all modules. This was my suggestion to their request to make the software simple to use (software developer).
In this respect, neither the GM, nor the software developer forced any top-down solution onto users. Users in turn took full advantage of the chance to define their own work tool with respect to their duties, processes, and organizational structure. The “showcase” module in ABC provides a good example, as summarized in the following comment: The doctors entered the system from home and wrote the prescriptions without looking at the guests diaries. So we asked the programmer to create a rule that the doctors have to pass through the diary of a guest before accessing the prescription page (head nurse). Over time, the bottom-up approach grew to feel so natural for the organization that initiatives to change or add new modules came only from users. Twelve years after the first test, ABC is an integral part of the activities engaged in by anyone who works at FSC; even training is done internally, such that “everybody is good at using the software perhaps because they come here and the group helps them. We do the training ourselves, on the job” (head nurse).
User Friendliness and Job Simplification
A key characteristic of ABC is that its complexity grew together with the IT skills and capabilities of the healthcare operators. Many operators (e.g., nurses, health assistants) had been IT illiterate before the introduction of ABC. However since the tool grew with them, they quickly realized its accessibility. The initiative achieved such a warm welcome that the operators even tried to enhance their capability on their own. As the GM recounted, “some of them at the beginning asked help from their sons and daughters; others went to the local computer store for help. Today training is no longer necessary but we sponsor it if they ask. I even had a cook taking an Access course.” Furthermore, ABC simplifies and accelerates certain functions by fully reflecting the job of healthcare operators, which require both standard outcomes and immediate local responses. That is, it supports very complex analyses but also provides quick overviews and includes tools to help users react quickly to known problems: If a guest has an urgent problem which requires going to the hospital, it is necessary to print an accompanying module. This is a complex document … people normally panic … especially at night. Here you see … it is sufficient to click here to print the complete document with all the information (software developer).
Orientation Toward Patients/Guests
Finally, largely as a consequence of the previous factors, the data collected in ABC generates a positive cycle of additional value and use for analysis and planning. For example, before ABC, even the individual assistance plans were based mostly on hunches. The ABC software instead provides visual warnings related to daily issues for each guest (e.g., diet, evacuation, mobility, sleep). These warnings are organized temporally, which enables operators and managers to take proper actions according to the current situation or trends. Consider an example of how the warnings in ABC were used in a specific, actual situation to solve one of the major problems for elderly people worldwide, namely, falls [4]: For example, who falls more than others? Mr. White has fallen 28 times this year [2009]. With ABC I can see falls per year, let’s s22 2008: 82 falls in 2008… I am interested in place: 19 falls have taken place in his room. The falls happening in rooms are due to get up phase … he will never accept bedrails. Here you see it: Slipped off bed, found near the bed…. So you see, by crossing data on falls over time and personal data we are able to reflect … being more accurate with our response, grants him, and his family, a better life. Result: we put a gym mat near his bed just in case, to soften the falls: it is non-intrusive, he is happy, and it costs nothing (general manager).
The perception of care is confirmed by the two guests whom we interviewed about their experiences with regard to the effects of ABC. For example, one guest noted: “At first I did not understand how the nurse from the day shift could know that I had a difficult night. They care a lot about me” (guest).
Evidences from the Descriptive Quantitative Data
During the first 10 years of usage, the average age of FSC guests increased from 80.5 to 83.1 years. A 3 year increase in average age entails greater complexity and costs for care and clinical services. However, even as the FSC guests grew older, mortality rates decreased significantly, from 24 deaths in 1999 to 15 in 2009, a reduction of 37.5 %. This trend emerged even though FSC moderately increased its bed capacity (+2, an increase of 3.3 %) (Table 1).
As the scores in Table 2 reveal, on all three parameters, the guests have attained improved quality of life since the ABC implementation. In this sense, FSC demonstrates its strong orientation toward rehabilitating guests’ residual physical and mental autonomy. It is important to clarify that these positive differences do not refer to the same population of guests given the turnover of guests over 10 years. The ABC software played a significant role in improving FSC capability of personalizing the services through a strong orientation for recovering or maintaining the residual levels of autonomy. This resulted in a higher attractiveness for a population of guests with higher cognitive and functional autonomies. This means that FSC, also thanks to the use of the ABC software, is now more capable of attracting guests who although need to be treated for different typical illness of the aged prefer to live in a nursing home where the residual levels of cognitive and physical autonomy are stimulated.
From a HRM perspective, the adoption of ABC generated better outcomes in terms of personnel loyalty, tenure, and participation. As in many Western healthcare organizations, staff tenure has been a serious problem at FSC. In the past decade though, the extent of this problem was nearly halved, with notable positive effects for the quality and continuity of health services provided. Furthermore, average sick days taken by staff members decreased by 16 % (Table 1).
Discussion
FSC developed a system that fit its needs as they emerged. More advanced needs, such as cross-analyses of trends, medication lists, and hospital documentation, entered the system only later and in stepwise fashion. Each function was developed only on when users asked for them. Furthermore the development reflected the evolving needs of the guests. As the types of guests changed (i.e., older, requiring more complex treatment), the software evolved to fit these needs. The quantitative data, whose trends became visible thanks to the software, also played a pivotal role in establishing and maintaining a virtuous cycle both for guests and operators. In particular, they provided tangible, objective proof that the work was benefiting guests. These positive trends fed users’ enthusiasm and thus constituted key factors for these projects: The constant decrease of the use of drugs replaced by stronger rehabilitation and social measures, the improvement of the mobility conditions of guests, [and] the fall in the number of deaths from 24 to 15 with (in the last year) 8 people who were over 95 could not happen without the IT modernization process of the organization driven by the new software (general manager). While not all improvements are strictly due to ABC, the organizational practices in use today are supported largely by the tool (we could not leave without it!) making ABC an important contributor to the organizational performances.
Study Limitations and Future Research
This is a promising exploratory study for a wider investigation involving part of (or all) the more than 100 other organizations that have adopted the same tool. However, we need to take into account few limitations. The first limitation refers to the absence of a control group. No solution could be provided because the presence of an internal control group subjected to a lower quality level of long-term care, due to the absence of the software use, would be unequal and discriminant and potentially cause legal problems. Second, we are aware of the fact that rather than providing the evolution of those parameters for the same population, we presented only the comparison (but also the amelioration) of two fixed situations in different times and with almost totally different populations. To overcome these limitations, future research should focus on the comparison of two or more nursing homes having similar type of population, with some using ABC while others used as external control groups.
Conclusions
We have presented an IT-driven modernization process for a nursing home that, through careful management and patience, managed to design an HIT system based completely on the needs of users and guests. Proper implementation and productive utilization of a new IT tool appears more likely if the system provides tangible results, obtained from (1) a design focused on the needs of patients, (2) a system that it is easy to learn and use, and (3) a bottom-up approach that considers tips and warnings provided by users. The results provide internal validity that helps maintain motivation, and external validity that supports the organization in its market. Such outcomes require more thinking and energy than money, in contrast with a complex, top-down, universal, cost-cutting IT tools traditionally implemented in health-care organization. These greater efforts realized through the three main results of our research have activated a continuous virtuous circle that brought benefits for guests and operators.
Notes
- 1.
Acknowledgments: we thank the personnel and guests of FSC for their support.
References
Adler-Milstein, J., & Bates, D. W. (2010). Paperless healthcare: Progress and challenges of an IT-enabled healthcare system. Business Horizons, 53(2), 119–130.
Alberg, A. C. (2008). Care recipients’ Perceptions of activity-related Life space and life satisfaction during and after geriatric rehabilitation. QLR, 17, 509–520.
Bath, P. A. (2008). Health informatics: Current issues and challenges. JIS, 34(4), 501–518.
Bowen, M. E., Craighead, J., Wingrave, C. A., & Kearns, W. D. (2010). Real time locating systems (RTLS) to improve fall detection. Gerontechnology, 9(4), 464–471.
Carugati, A., Giangreco, A., & Sebastiano, A. (2011). Moving the implementation line: A nursing home’s path to success with IT. SIM, 16(4), 73–101.
Charmaz, K. (2006). Constructing grounded theory: A practical guide through qualitative analysis. Thousand Oaks: Sage.
Charney, P. (2007). Computer technology and the nutrition support professional: Make it work for you! Nutrition in Clinical Practice, 22, 421–427.
Cucinotta. D., Angelin, A.& Godoli, G., et al. (1989). Proposta e Validazione di un Semplice Indice per la Valutazione Funzionale Globale dell’Anziano: il GEFI. Giornale di Gerontologia 38, 31–36.
Eisenhardt, K. M. (1989). Building theories from case study research. AMR, 14(4), 532–550.
Folstein, M. F., Folstein, S. E., & McHugh, P. R. (1975). Mini-mental state. A practical method for grading the cognitive state of patients for the clinician. Journal of Psychiatric Research, 12(3), 189–198.
Hutchison, A. J., Johnston, L. H., & Breckon, J. D. (2010). Using QSR-NVivo to facilitate the development of a grounded theory project: An account of a worked example. International Journal of Social Research Methodology, 13(4), 283–302.
Mahoney, F. I., & Barthel, D. (1965). Functional evaluation: The barthel index. Maryland State Medical Journal, 14, 56–61.
Mantzana, V., Themistocleous, M., Irani, Z., & Morabito, V. (2007). Identifying healthcare actors involved in the adoption of information systems. EJIS, 16(1), 91–102.
Meyer, D., Marx, T., & Ball-Seiter, V. (2011). Social isolation and telecommunication in the nursing home: A pilot study. Gerontechnology, 10(1), 51–58.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2013 Springer-Verlag Berlin Heidelberg
About this chapter
Cite this chapter
Sebastiano, A., Carugati, A., Giangreco, A. (2013). The Pursuit of Happiness: The Virtuous Circle of an IT Tool for its Users and Beneficiaries. In: Spagnoletti, P. (eds) Organizational Change and Information Systems. Lecture Notes in Information Systems and Organisation, vol 2. Springer, Berlin, Heidelberg. https://doi.org/10.1007/978-3-642-37228-5_6
Download citation
DOI: https://doi.org/10.1007/978-3-642-37228-5_6
Published:
Publisher Name: Springer, Berlin, Heidelberg
Print ISBN: 978-3-642-37227-8
Online ISBN: 978-3-642-37228-5
eBook Packages: Business and EconomicsBusiness and Management (R0)