
Abstract
Drug discovery is a risky and expensive business fraught with high attrition rates. The health-care benefits and financial rewards that can be realised if successful have, however, ensured the relevance and continued growth of the pharmaceutical industry. The major reasons for high attrition rates during drug discovery include lack of efficacy, toxicity, inadequate pharmacokinetics (PK), and market forces, factors which can be complexly interrelated. PK has been shown to affect the efficacy and safety of new chemical entities (NCEs). The pharmaceutical industry responded by frontloading the characterisation of the processes that determine the PK of compounds, that is, absorption, distribution, metabolism and excretion (ADME). The ADME data are being used to guide medicinal chemists in the design of molecules with favourable disease-specific PK properties. In late stages of drug discovery, the preclinical ADME data are being used to predict human PK and safety of NCEs. As African research scientists initiate drug discovery activities, integration of PK, in the traditionally medicinal chemistry- and disease pharmacology-driven efforts, is important towards ensuring increased chances of discovering good candidate drugs (CD). We have therefore set up in silico, in vitro and in vivo ADMET platforms which various African drug discovery scientists can access. Drugs for non-communicable diseases fail more from lack of efficacy than poor PK and vice versa. Drug discovery efforts in Africa are also mainly based on natural products for which little is known or can be inferred from the PK of conventional synthetic drugs. These factors point to the need of promoting the sciences and technologies of PK research at many African institutions.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
These keywords were added by machine and not by the authors. This process is experimental and the keywords may be updated as the learning algorithm improves.
7.1 Background
Prior to the 1990s, studies in pharmacokinetics (PK) were completed late in drug discovery and during drug development. The preclinical studies were mainly animal in vivo studies used for safety evaluation and human dose predictions by allometric scaling. A landmark paper by Prentis [1] reviewed the factors responsible for the failure of new chemical entities (NCEs) in British pharmaceutical companies and found that between 1964 and 1985, inadequate PK was the leading cause of failure in 39% of new chemical entities (NCEs) followed by lack of efficacy and by toxicity. PK has an intricate impact on efficacy and toxicity, emphasising the role of PK in the failure of NCEs. Further reviews corroborated Prentis’s findings [2]. Drugs for the treatment of infectious diseases failed more due to poor PK than those for non-communicable diseases, strongly suggesting the necessity for the incorporation of PK into drug discovery programmes.
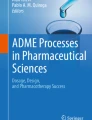
During the 1990s, industry responded by setting up many assays that enabled projects to characterise the process that determined the PK of compounds. These included in vitro methods for compound permeability, metabolism and excretion. Application of these assays was frontloaded to early phases of the drug discovery process from hit identification, lead discovery and lead optimisation through to candidate drug selection [3]. By 2000, the pharmaceutical industry had reduced the failure rate of NCEs due to PK issues from 40% to less than 10% [2]. Figure 7.1 shows the relative contribution of various factors in the attrition rates of new chemical entities [4]. It is important to note the rapid increase in the cost of goods as a cause of drug discovery and development failure followed by poor efficacy and clinical safety. Most drug discovery projects in Africa do not have access to the PK platforms which major pharmaceutical industries are using to reduce attrition rates. It is therefore likely that the failure or slow progress of some of the discovery projects in Africa could be due to lack of PK support.

Evolution of the principal reasons for drug development failure between 1991 and 2005. Adapted from [4]
7.2 Pharmacokinetic Challenges in Drug Discovery
The overall objective of drug discovery is to “find a potent and selective compound, reaching to the site of action at sufficient concentration for a sufficiently long time to elicit the desired effect with a reasonable dose that can be administered orally to humans in an acceptable form once or twice a day” (Ulf Bredberg, personal communication). In addition to this, the compound must also be safe for human use. It is in the context of achieving these objectives that pharmacokinetics can play an important role. Poor drug systemic exposure could be due to low absorption from the intestine caused by low compound permeability or low solubility. Low bioavailability can also be due to high clearance and short half-life caused by extensive liver metabolism and excretion. Absorption and metabolism therefore play a key role in determining drug exposure levels. Figure 7.2 depicts how these factors determine drug exposure levels as a measure of bioavailability.

Pharmacokinetic processes that affect drug bioavailability
With respect to safety, pharmacokinetic factors can contribute through risk for drug–drug interactions due to enzyme and/or transporter inhibition or induction. Inhibition of the metabolism of one drug (victim drug) by another (perpetrator drug) could result in overexposure of the victim drug, resulting in either exaggerated pharmacologic effects or unselective effects on other receptors. Induction, on the other hand, could result in underexposure of the victim drug associated with sub-therapeutic effects. Toxicity or idiosyncratic reactions could also arise from increased production of reactive and toxic metabolites of the new chemical entity. Toxicity can be mediated through formation of protein adducts (cytotoxicity) or nucleic acid adducts (genotoxicity).
7.3 Overview of Pharmacokinetics
Pharmacokinetics can be defined as “the study of the time course of drug and metabolite levels in different fluids, tissues, and excreta of the body, and of the mathematical relationships required to develop models to interpret such data” [5]. The key PK parameters that enable one to determine how much and how often a drug should be administered to achieve a desired therapeutic effect in a safe, efficacious and convenient manner are absorption (F a), volume of distribution (V d), clearance (CL), half-life (t 1/2) and bioavailability (F). Figure 7.3 illustrates the pharmacokinetic profiles of a drug after an intravenous (i.v) and oral (p.o) dose. The figure also shows the importance of drug concentrations with respect to effective concentration ranges and toxic ranges, parameters relevant in the safe and efficacious use of medicines. Table 7.2 shows the equations used to calculate the important pharmacokinetic parameters used in dose regimen determinations.

Schematic representation of a plot of the natural logarithm of drug plasma concentration (In[D]) with time (hours) after intravenous (i.v) and oral (p.o.) administration of a drug. Co—extrapolated initial dose, C max—maximum drug concentration achieved, T max—time to reach C max, K el—elimination rate constant, AUC—total area under the curve, a measure of drug exposure. MEC minimum effective (therapeutic) concentration, MTC minimum toxic concentration
These PK parameters (Table 7.1) can all be determined from in vivo studies in preclinical animals and in humans when the drug is administered enterally (oral, buccal or rectal) and/or parenterally (intravenous, intramuscular, peritoneal and subcutaneous). Most studies in discovery use oral and intravenous drug administration to determine the PK parameters indicated in Table 7.1.
7.4 The Drug Absorption, Distribution, Metabolism and Excretion Process
Traditionally, pharmacokinetic studies had been done either as a documentation process or as part of toxicokinetic studies in drug discovery and development. As understanding of the potential role of PK in selecting compounds with favourable PK and pharmacodynamics (PD) increased, the preclinical animal studies where used to predict human pharmacokinetics using allometric scaling. This method is based on the hypothesis that physiological parameters are proportional to body size and weight. Allometric scaling has been used to predict various PK parameters indicated in Table 7.1 with mixed success.
Important biomedical breakthroughs in the 1990s allowed scientists to develop in vitro systems to study the individual processes that constituted the PK of a compound (Table 7.2). For absorption, systems to study drug permeability and transport (e.g. Caco2, intestinal segments and transfected cell lines) enabled the prediction of the fraction of drug absorbed, F a. For metabolism, liver microsomes, hepatocytes, recombinant enzymes and cell lines enabled the humanisation of in vitro drug metabolism towards the prediction of drug clearance (CL) and drug–drug interactions [6]. These revolutions in biological systems were also accompanied by technological advancements such as LC-MS/MS and automated assays for high-throughput screening (HTS).
The deconvolution of PK to discrete processes of drug absorption, distribution, metabolism and excretion (ADME) allowed for mechanistic insights that were not possible from the holistic in vivo PK studies. They also facilitated the evolution of computational methods towards the derivation of qualitative and quantitative structure–activity relationships (SAR and QSAR) for the prediction of ADME properties. Such SAR and QSAR have resulted in very fruitful collaborations between medicinal chemists and pharmacokinetic scientists which are enabling the rapid optimisation of compounds with respect to PK and PD properties. Table 7.3 summarises the physicochemical and in vitro ADME that can now be determined and used to effect chemical modification or predict in vivo PK, thus in-calculate rational design in the drug discovery process.
There are pros and cons of using in vitro or in vivo preclinical models. The advantages of in vivo models are that you get integrated information on permeability, metabolism, secretion and transport. One can sometimes make in vitro to in vivo correlations for the animal model to support human in vitro to in vivo predictions, which can lead to the observation of the effect of unknown PK mechanisms. The major disadvantage of preclinical animal studies is that there can be great inter-species difference between the model animal and humans. This is particularly so with respect to metabolic processes. The advantages of using in vitro systems are that one can use both human and animal tissue, study the individual components of PK, derive insights into the mechanism of drug disposition and test for specific properties such as enzyme inhibition and amenability to high-throughput screening (HTS). The disadvantages of the in vitro systems are that one needs to know all mechanisms involved in a drug’s PK in order to study them individually, assays for some mechanism might not be there or are too complex to study. A major disadvantage of in vitro system is the many physiological assumptions one has to make from recombinant, sub-cellular, cellular and organ to whole animal/human systems. In general, as one progresses from simple recombinant enzymes, microsomes, to complex hepatocyte systems, success in the prediction of in vivo metabolic clearance increases, but the costs of doing the studies also increase.
7.5 In Silico ADMET
Before the development of the elaborate in vitro ADMET toolkit, efforts to predict physicochemical and pharmacokinetic parameters were solely based on the physicochemical properties of new chemical entities. The methods used properties such as lipophilicity (Log P and Log D), pKa, Mwt, melting points, binding energy, number of atoms, etc.) to predict physicochemical properties such as solubility and metabolic properties such as Michaelis–Menten constant (K m), clearance and toxicity. As the in vitro ADME assays on HTS platforms started churning out large amounts of data which were initially meant for in vitro–in vivo correlation studies, the data provided an opportunity for SAR and QSAR studies. Metabolic stability, enzyme and metabolite identification, and cytochrome P450 inhibition data using recombinant enzymes produced mechanistically clean data that were used to develop SAR and QSAR models. In addition to the in vitro data, starting with the publication of the soluble bacterial CYP crystal structures in the 1980s, homology models of CYPs were developed and docking studies used to infer ligand–enzyme active site interaction studies. This work led to the derivation of pharmacophore models for substrates and inhibitors of the major drug-metabolising enzymes, CYP1A2, 2C9 and CYP2D6. Advances in molecular biology assisted this effort by providing site-directed mutagenesis functional studies towards mapping the geometry and chemistry of proposed active sites of CYPs. After years of failed efforts to crystallise membrane-bound CYPs, success was achieved in 2000 with the crystallisation of the rabbit CYP2C5 enzyme. This work was followed by successful crystallisation of several human CYPs including CYP21A2, 2C8, 2C9, 2D6 and 3A4. Some of the enzymes were co-crystallised with substrates and/or inhibitors to give the first direct information on enzyme–ligand interactions. Advances in computational tools in quantum mechanical calculations, molecular dynamic simulations, GRID-based calculation of physicochemical properties of substrates/inhibitors and enzyme active site, and docking and scoring functions to understand orientation and affinity of enzyme–ligand interactions were successfully applied to ADMET computational modelling. This strengthened the link between Medicinal Chemistry and DMPK scientists in addressing ADMET issues at molecular level. Software such as Flex X, GOLD, GLIDE and AutoDock are being used for docking substrates/inhibitors into active sites of drug-metabolising enzymes towards studies to identify involved enzymes and predict sites of metabolism. The Volsurf software (http://www.moldiscovery.com) is being used to predict permeability, solubility and metabolic stability. Metasite (http://www.moldiscovery.com) is being used for the identification of site metabolism and when linked to mass spectrometry in metabolite identification studies. There are now many software programmes on the market, some free and others commercial. The choice of software to use is very important; they are based on different modelling techniques and different data quality and might require secondary processing for meaningful interpretation of the results. Interpretation of most of the results requires a good understanding of the biology of the ADME properties being predicted.
The initial purpose of the in vitro data of making in vitro–in vivo correlations also experienced significant advances. Notable products on the market being Simcyp (http://www.simcyp.com), Gastroplus (http://www.simulations-plus.com), WinNONlin (http://www.pharsight.com/products/prod_winnonlin_home.php) and Aureus (http://www.aureus-pharma.com), which, through various ways, try to address some of the challenges of in vitro to in vivo extrapolation (IVIVE) of ADME properties such as (a) inter-individual variability in metabolic processes, (b) interplay of drug-metabolising enzymes and drug transporters, (c) interethnic differences in PK properties and (d) estimation of concentration of test drug reaching the enzyme active site. These developments have given birth to the field of pharmacometrics where PK simulations and physiologically based pharmacokinetic modelling (PBPK) are being used to predict the likely pharmacokinetics of a candidate drug when given to humans. This is contributing to the efficient design of clinical studies and the projection of data from few patients to whole populations, something which could result in reduced costs of clinical trials which are currently the most expensive phase of the whole drug discovery and development process.
7.6 ADMET and PK Preclinical Models in Drug Discovery
Various in silico, in vitro and in vivo models are being applied in the design, characterisation and selection of new chemical entities with ADMET and PK properties predicted to result in a safe and efficacious product for clinical use in humans. Over the past 20 years, the pharmaceutical industry has developed an elaborate generic “ADMET/PK toolkit” that is used across most disease areas and is amenable to modification to address some project-specific questions. The models provide different pieces of information of varying complexity throughout the hit evaluation, lead discovery, lead optimisation and candidate drug nomination value chain (Fig. 7.4).

Schematic representation of how in silico, in vitro and in vivo preclinical platforms for ADMET characterisation are being frontloaded in the drug discovery value chain
Given the background of drug discovery activities by African research groups being driven by medicinal chemistry (mainly herbal extracts, purified natural products from herbs with reported medicinal properties and to a lesser extent conventional organic synthesis) and pharmacology (mainly screens against in vitro parasite cultures, animal disease model and to a lesser extent recombinantly expressed molecular targets), integration of DMPK was virtually absent. Before the establishment of drug discovery DMPK expertise at the African Institute of Biomedical Science and Technology (AiBST), the only PK studies done by some institutions were in vivo animal and human PK on drugs already on the market with either the aim of evaluating them for general toxicity, PK variability in African populations or PK/PD relationships in patients. The DMPK/PD-Tox Department at AiBST was therefore established with the aim of setting up an industrial DMPK platform benchmarked against the in silico, in vitro and in vivo models being used by leading pharmaceutical industry. The in silico, in vitro and in vivo models for drug discovery will therefore be described in the context of those set up at AiBST and being applied in the characterisation of anti-parasitic drugs in use and new chemical entities from various drug discovery research groups in Africa. To make the concepts relevant for the African case, drugs indicated in Fig. 7.5 will be used to demonstrate the potential benefits of integrating such tools in the discovery and development of safe and efficacious drugs in the fight against infectious diseases endemic to Africa.

Chemical structures of some anti-parasitic drugs whose ADME properties have been characterised
7.7 Compound Library Characterisation and Hit Identification and Evaluation
During the early phases of target identification and validation, the approach could involve the use of tool compounds (e.g. inhibitory analogues of the target substrate) and screening large compound libraries against a high-throughput in vitro assay for the molecular target. The compound libraries to be screened can be in-house resources or can be purchased from external sources. Before purchase of compounds and during the in vitro pharmacological screens, the compound libraries should be screened for general druggable properties. A number of such general properties have been proposed and the most widely used being the Lipinski rule of 5 for compound solubility and permeability, the major determinants of compound absorption [17]. It is important that the application of such in silico filters be done with caution since they are only guidelines which if used dogmatically, could result in the loss of novel compounds that could have unique PK and PD properties, with the possibility of intellectual property (IP) and market competitive advantages for a company. During this phase, the tractability of the biological target is evaluated with respect to PK and PD issues. PD issues involve the identification of compounds with reproducible biologic effect for the desired type of activity (e.g. agonist, antagonist or enzyme inhibition). PK issues could relate to the accessibility of the target (e.g. central nervous system), knowledge of competing endogenous ligands and intended dose formulation (e.g. i.v, p.o. or inhalation). If oral administration is the intended formulation, the following PK parameters should be predicted at this stage and be used to judge the quality of the compound library to be purchased or the hits obtained from in vitro and in silico screens: (a) Lipinski rule of 5 (Mwt, Log P, HBD, HBA), (b) PSA, (c) permeability, pKa and (d) solubility. Table 7.4 shows these predictions for some anti-parasitic drugs done using various softwares (Volsurf, MOKA, Marvin Sketch, etc.).
Given that a Lipinski score is predictive of oral absorption and that this PK parameter is a function of solubility and permeability, the predictions of permeability using Volsurf (Fig. 7.6) are supportive of the role of the physicochemical properties predicted in Table 7.4. The prediction tool in Volsurf was developed using Caco2 permeability data. Representative compounds from the various clusters for the predicted parameters are then experimentally determined for (a) water solubility, (b) lipophilicity, (c) pKa, (d) protein binding, (e) metabolic stability in human liver microsomes and microsomes from PK or PD animal model, (f) glutathione trapping of reactive metabolites in human liver microsomes, (g) inhibition of major CYPs (reversible and irreversible), (h) stability in human and PK or PD animal model plasma for drugs with moieties that could undergo hydrolysis and (i) permeability in Caco2 cells. This is done to check the predictive success of the computational tools and to generate real experimental values. The latter can be used to derive structure–activity relationship (SAR) models for the various parameters for the specific chemical series under study. At this stage, HTS approaches are used, and a ranking system is employed to make decisions on which series or cluster of compounds to proceed with and what potential ADMET and PK liabilities one needs to explore further at lead discovery stage.

Predictive projection of Caco2 permeability of novel 4-aminoquinolines in a permeability model in Volsurf
Table 7.4 shows that none of the anti-parasitic drugs violates Lipinski’s rule of 5; Mwt ≤ 500, Log P ≤ 5, HBD ≤ 5, HBA ≤ 10 and PSA ≤ 100 Å2. The compounds are therefore predicted to be permeable. The predicted solubility is, however, low, a reason why most of these drugs were made salts to enhance solubility. Due to the importance of solubility and permeability for absorption, a biopharmaceutical classification system, BCS, based on permeability and solubility, has been developed which classifies compounds into four major categories: Class 1—high permeability and high solubility, Class 2—high permeability and low solubility, Class 3—low permeability and high solubility and Class 4—low permeability and low solubility.
The compounds are predicted not to be highly protein bound except for chloroquine and amodiaquine. The prediction success can vary, e.g. artemisinin is predicted to be 50% bound and the measured value is 40%, compared to less successful, e.g. thiabendazole, predicted to be 67% bound and the measured value is 89%.
Predictions and measurements of some physicochemical and ADME properties were also researched for a novel series of 4-aminoquinolines synthesised in Prof. Kelly Chibale’s laboratory (University of Cape Town, South Africa) (Table 7.5). None of the compounds violate more than 2 of Lipinski’s rule and are therefore predicted to have good permeability. This is also supported by predictions using the software Volsurf (Fig. 7.6). In Table 7.4, it is evident that measured and predicted properties are not always in agreement which serves as a cautionary note not to be over-dependent on in silico methods in deciding the fate of NCEs. It is to be always kept in mind that predictions are only as good as the assumptions, and data quality and quantity that are used to make the predictive tools. Poor correlations on the other hand might simply mean that some unique aspects of the series one is working on are not well captured in the computational method one is using. Whether one gets good or bad predictions, the exercise demands that the drug discovery teams seek to understand the chemical basis of the ADME behaviour of new chemical entities.
7.7.1 Determination of Compound Lipophilicity
At this stage of drug discovery, Log D 7.4 is determined using a reverse phase chromatography HPLC method with the mobile phase at pH 7.4. In this method, a number of standard compounds of previously determined lipophilicity (using the shake flask, water–octanol partitioning method) are run on the reverse phase column, and their retention times are noted (k′). These are then plotted against their known Log D 7.4 values to make a standard curve. The standard compounds covering a wide span of Log D 7.4 values are used: metoprolol (0.02), propranolol (1.15), testosterone (3.19) and felodipine (5.20). The unknown compounds are then run on the same column, and their retention times are noted. These are used to read off the Log D 7.4 values of the test compounds from the standard curve. Table 7.5 shows the predicted and measured Log D 7.4 values of a series of 4-aminoquinolines with demonstrated antimalarial activity (Thelingwani et al. unpublished). Figure 7.7 shows the retention times of standard compounds and the standard curve (plot of literature Log D 7.4 against measured capacity factor of standard compounds) from which the capacity factors of unknown compounds are used to read off their predicted Log D 7.4.

Typical results outputs/presentation of various physicochemical and ADME determinations available at AiBST
7.7.2 Determination of Compound Solubility
Solubility in water is determined using a turbidimetric assay. In this assay, test compounds dissolved in DMSO are diluted in water, and the different solutions are evaluated for precipitation spectrophotometrically at a wavelength of 595 nm. In this method, a highly water-soluble compound, paracetamol, and a poorly soluble compound, niclosamide, are used as controls. In the absence of a precipitate, the absorbance remains below 0.05 units and will increase as precipitate is formed. Compounds are then classified as soluble (>100 μM), intermediate (<50 μM), partial (<20 μM) and insoluble (<10 μM). Solubility is very important in the design of in vitro experiments as it informs one on the maximum concentrations one can reliably work with in aqueous solutions. Figure 7.7 shows typical solubility/precipitation results of paracetamol, niclosamide and a test 4-aminoquinoline.
7.7.3 Determination of Compound Permeability
The Caco2 cell line derived from the human colon carcinoma has proved a very good predictive model for the fraction of drug absorbed, F a. This is because it has many of the morphological and physiological attributes of the small intestine, such as microvilli, and various mechanisms of permeability (transcellular, paracellular and active transport based). The cells are plated in a cell culture inset device in which the cells grow to confluence on a porous filter. Compounds are loaded on the apical side of the cell culture insert device, and samples are collected over time on the basolateral side. These data are then used to calculate the apparent permeability, P app, as cm/s. Compounds with P app < 1 × 10−6 cm/s being classified as low permeability, <20 × 10−6 cm/s—moderate permeability and >20 × 10−6 cm/s—high permeability. To investigate the potential role of efflux transport, the test compound can also be put in the basolateral side, and samples can be collected and measured on the apical side. If the ratio of A to B/B to A is greater than 2, this points to the possible existence of active transport of the compound.
7.7.4 Determination of Compound Metabolic Stability
Metabolic stability, a measure of a compound’s extent of biotransformation, is determined in liver microsomes (for oxidative metabolism) and plasma (for compounds likely to undergo hydrolysis). Microsomes are the most commonly used in vitro system due to the fact that most drugs are mainly metabolised by cytochrome P450s which have the highest concentration in liver microsomes. The study involves incubating 1.0 μM of test compound in 0.5 mg/ml liver microsomes for 0, 5, 10, 15, 20 and 30 min. The elimination rate constant, K el, is estimated from the plot of the natural logarithm of remaining drug concentration versus incubation time. The K el is then used to calculate the elimination half-life, which in turn, is used to calculate the intrinsic metabolic clearance (ml/min), CLint = (0.693 × volume)/t 1/2. Figure 7.7 shows a typical metabolic stability result for low, high and intermediate clearance compounds. Such studies are done with liver microsomes and cytosols from preclinical animal models and humans. To control the assays, a set of standard compounds is run with each batch of test compounds. Table 7.5 shows the metabolic stability of a novel series of 4-aminoquinolines with demonstrated antimalarial activity.
7.7.5 Determination of Cytochrome P450 Inhibition
The modern clinical setup is characterised by the practice of poly-pharmacy where patients are taking many drugs at the same time, either to treat multiple co-ailments or due to the need of combination therapy for increased efficacy. The latter is very common in the treatment of infectious disease in order to reduce the risk for drug resistance. At hit identification and characterisation, the test compounds are evaluated for inhibitory effects on recombinant CYPs, 1A2, 2C9, 2C19, 2D6 and 3A4. These are among the most important CYPs responsible for the metabolism of most drugs on the market and are associated with a risk for drug–drug interactions if inhibited. High-throughput assays using substrates which are metabolised to fluorescent metabolites can be used. In the assay, each test compound is tested for inhibitory effects on each rCYP at different concentrations. The inhibitor concentration resulting in 50% reduction in enzyme activity (IC50) is determined by plotting the remaining enzyme activity as a measure of fluorescence against the varying concentrations of the test compound. For each rCYP, a positive control inhibitor is used, napthaflavone for CYP1A2, sulfaphenazole for CYP2C9, ticlopidine for CYP2C19, quinidine for CYP2D6 and ketoconazole for CYP3A4. Figure 7.7 shows typical inhibitory effects of some 4-aminoquinolines on CYP1A2. Table 7.5 shows the inhibitory effects of 4-aminoquinolines on the major drug-metabolising enzyme, CYP3A4.
While most inhibitory effects of compounds are of a reversible mode (competitive or non-competitive), some compounds demonstrate time-dependent inhibition (TDI). TDI is usually associated with the bioactivation of a test compound to a reactive metabolite which in turn forms a covalent bond with the CYP, resulting in irreversible (referred to as mechanism-based inhibition—MBI) or quasi-irreversible (referred to as metabolite intermediate complex inhibition—MIC) inhibition. Mechanism-based inhibition can, in addition, result in idiosyncratic reactions due to immunogenic reactions caused by proteins covalently modified by the reactive metabolites. The assay for the determination of TDI involves pre-incubation of the test compound with the enzyme (that would result in the inactivation of enzyme molecules) followed by a second incubation in which the enzyme substrate is added (to measure the remaining enzyme activity). Control reactions with pre-incubation without the test compounds or without NADPH, the cofactor required for CYP activity, are also run in parallel. The final result is given as a ratio, which if below 0.7 is indicative of TDI effects and if >0.9 is indicative of no TDI effects. Control TDI compounds for each of the enzymes are used, furafylline for CYP1A2, tielinic acid for CYP2C9, ticlopidine for CYP2C19, paroxetine for CYP2D6 and troleandomycin for CYP3A4.
The in silico and in vitro studies at this compound library and hit identification and characterisation stage help projects in identifying potentially important trends that can affect the feasibility of pursuing certain compound classes to the lead discovery phase. For example, in the presence of alternatives, strong correlations between Log P, potency, metabolic stability and CYP inhibition could be a “show stopper” as they point to a very difficult chemical space to separate and optimise for these important PK/PD/safety variables. A series exhibiting very strong TDI can also be a serious liability as the possibility of idiosyncratic reactions that could be caused by such compounds is difficult to predict clinically. High Log P values at hit identification stage are also not favourable since medicinal chemists generally increase lipophilicity to increase potency during lead optimisation. It is therefore important to invest in highly competent teams to exploit the large amounts of data generated in a manner that extracts information and translates it to innovative project strategies for successful hit identification.
7.8 Lead Discovery
During lead discovery (LD), clusters identified in hit identification stage are worked on to select two to three series which meet the lead compound criteria set for the project. The main purpose of this phase is to identify key liabilities associated with the selected series and to suggest ways they could be addressed during the subsequent lead optimisation (LO) stage. Series carrying severe DMPK problems associated with the pharmacophore, e.g. an overlap of the pharmacophore for pharmacologic effects and that of a DMPK liability such as metabolic instability or CYP inhibition, are usually discontinued. The LD phase is a learning phase where the selected scaffolds from LI are expanded to identify any structure activity relationship in physicochemical and ADMET properties. Assays performed during LI continue to be performed to keep track of any changes in physicochemical and ADME properties as the exploration of the chemical space of the selected series is conducted.
Additional assays are also conducted at this stage. These include metabolite identification (to understand the possible basis of metabolic instability and/or mechanism of reactivity), enzyme identification and in vivo PK in preclinical PK and PD animal models. These data are used to understand the relationship between structural and DMPK properties (QSPR—quantitative structure property relationship). At this stage, one also investigates in vitro–in vivo correlation for DMPK properties such as absorption and clearance. In vitro and in vivo DMPK and PD data are also modelled at this stage to derive PK/PD models. Such models at this early stage are important as they can rescue a chemical series with seemingly poor DMPK or PD properties. There are many successful drugs on the market which would not have made it based on their DMPK or their PD properties alone. Addressing each of these properties separately is therefore risky in drug discovery and development. The ideal situation in the selection of lead series is where one can optimise the DMPK issues without compromising pharmacological properties. The difficult situation and usually a show stopper is when these key properties covariate and cannot be optimised independently.
7.8.1 Metabolite Identification
The major determinant of drug clearance is metabolism. To understand and possibly address metabolic instability or chemical reactivity, identification of metabolites formed is important. There are many software programmes which have been developed for the prediction of metabolites. In our laboratory, we use the software called Metasite (Molecular Discovery Ltd) and various docking software (Auto Dock, Flex X, or GOLD). Metasite works by using GRID (Molecular Discovery Ltd) derived chemical interaction energy maps of the test compound and that of the CYP’s active site. The maps of the compounds are overlayed on the maps of the CYP’s active sites, and a similarity index is used to identify compound-CYP matches. To suggest the site of metabolism, the distance of the nearest hydrogen to the CYP reactive centre is measured and used to rank all hydrogen in the compound. Distances (3–5 Å) associated with the possibility of hydrogen abstraction (the major mechanism of compound oxidation by CYPs) are used to identify and rank metabolic hot spots. The prediction engine can also take into account reactivity factors (i.e. in addition to the optimal distance, it will also identify functional groups associated with increased easy of oxidation). The result is therefore a ranking of sites for possible metabolism and hence the likely metabolites formed. Figure 7.8 shows the successful use of Metasite in the prediction of sites of metabolism of thiabendazole. We also use various docking algorithms to deduce possible metabolites. Figure 7.8 also shows the application of the docking programme, GOLD, in the prediction of the enzyme and site of metabolism in the biotransformation of amodiaquine.

In vitro, metabolite identification is done from incubations of test compound with human and preclinical PK and PD animal model liver microsomes or hepatocytes or human recombinant enzymes. Metabolite identification is then done by LC-MSMS. The MSMS product ion is interpreted by biotransformation scientists. It can also be done through assistance by software such as MetaboLynx (http://www.waters.com/waters), LighSight (http://info.appliedbiosystems.com/metaboliteID) and Mass-Metasite (http://www.moldiscovery.com). Most CYP-mediated reactions are aromatic hydroxylations, aliphatic hydroxylations, N-dealkylation and O-dealkylation and epoxidations. Metabolite structure can be interpreted in terms of these common reactions such as +16 for hydroxylation or N-oxidation, +32 for dihydroxylation and −14 for demethylation. Some metabolites cannot be easily elucidated by MSMS and might require NMR. In this case, the microsomal incubation is scaled up in order to generate 10–50 μg of metabolite. The 1H-NMR spectrum of the metabolite is obtained, and the changes of resonance are used to determine the site of metabolism, hence the structure of the metabolite.
Knowledge of the metabolite can be used for several purposes in drug discovery. These include guidance in blocking of metabolic hot spots to stabilise the compounds and synthesising the metabolites and testing them for pharmacological and toxicological effects. Figures 7.9 and 7.10 show the metabolite identification in the metabolism of amodiaquine.

Metabolite identification in the metabolism of (a) amodiaquine 1 and its metabolites formed after incubations for 30 min with rCYP1A1. Extracted ion chromatograms of m/z 356 (1), m/z 328 (2), m/z 317 (10), m/z 315 (9), m/z 301 (8) and m/z 299 (3) and (b) MS/MS spectra of 3 [9]

It shows the metabolic scheme in the biotransformation of amodiaquine [9]. 1—amodiaquine, 2—desethylamodiaquine, 3—amodiaquine aldehyde metabolite and 4—amodiaquine aldehyde quinoniemine metabolite
7.8.2 Trapping of Reactive Metabolites
Some metabolites are very reactive and difficult to isolate and conduct structural studies on since they react with biological components in the incubation. Studies on reactive metabolites are done in two stages: the first is to screen compounds for the generation of reactive metabolites. This is done by screening for the formation of glutathione conjugates in human liver microsomes. If iminium ions are likely to be formed, trapping experiments are done using cyanide. Other reactive metabolites are better trapped with methyloxamine or cysteine. For series containing carboxylic acid functions, the stability of acyl glucuronides should also be assessed. The isolation and subsequent structural elucidation of such reactive metabolites is a challenge since they usually covalently react with the biological matrix. To overcome this, non-biological systems can be used. The use of electrochemical oxidation is being successfully used to generate most CYP medicated metabolites. Figures 7.10 and 7.11 show how this approach has been used to characterise reactive metabolites of amodiaquine. Both electrochemical oxidation and microsomal incubations where used to characterise the bioactivation of amodiaquine to amodiaquine quinoneimine and the aldehyde metabolite. Trapping experiments with cysteine resulted in four cysteinyl conjugates, and those with glutathione gave four glutathionyl conjugates. MSMS and 1NMR were used to characterise the structures of these metabolites [10]. The generation of the aldehyde metabolite was done by electrochemical oxidation and structural studies done by MSMS and 1NMR. Trapping of the aldehyde metabolite was done with methoxylamine. Trapping experiments with N-acetyl cysteine revealed that the aldehyde was further oxidised to an aldehyde quinoneimine species, both in the rCYP incubations and in the electrochemical system (Fig. 7.11).

The bioactivation and trapping studies for amodiaquine to amodiaquine quinoneimine and the aldehyde metabolite. The amodiaquine quinoneimine gave 4 cysteinyl conjugates, 7–10. The aldehyde metabolite and its quinoneimine metabolite formed conjugates with methoxyamine (AM) and N-acetyl cysteine (NAC) [9, 10]
7.8.3 Enzyme Identification
Towards understanding the basis of metabolic stability and/or bioactivation of new chemical entities, there is a need to identify the enzymes involved in the generation of identified metabolites. This knowledge will be helpful in molecular design towards disrupting the physicochemical determinates of the compound’s specific interactions with the enzyme involved. For example, if one shows that a compound is metabolised by CYP2D6, there are well-known qualitative and quantitative structure activity relationships (SAR) associated with substrates of this enzyme that can enable medicinal chemists to reduce metabolic rates by either blocking metabolic hot spots or disrupting the CYP2D6 substrate pharmacophore. This strategy can be used to either solve instability issues or block the generation of reactive metabolites. Enzyme identification is also important towards understanding inter-individual variability in the pharmacokinetics of a drug. If one finds that a drug is solely metabolised by say CYP2D6, then the known genetic and environmental variation of this enzyme in human populations will be expected to reflect the pharmacokinetic variation of the new chemical entity.
Enzyme identification is also used towards predicting likely drug–drug interactions in situations where the test compound is co-administered with a drug that inhibits or induces the enzyme that is mainly responsible for the elimination of the test compound. There are several commonly used methods for enzyme identification (Fig. 7.12a, b, c). It is generally encouraged to use at least two of these methods to arrive at a relatively accurate conclusion on the qualitative and quantitative contributions of various enzymes in the metabolism of a test compound. First, the compound is incubated with sub-cellular fractions known to be involved in the metabolism of drugs. Since most drugs undergo oxidative metabolism by CYPs, identification for these enzymes will be discussed in detail. Data from work on the metabolism of amodiaquine will be used to illustrate the methodology (Fig. 7.12). Data on the identification of CYPs responsible for the metabolism of anti-parasitic drugs will be used to demonstrate the likely general and specific implications of such information in the safe and efficacious use of these drugs in African populations.

Some methods used in reaction phenotyping as applied to the characterisation of the metabolism of amodiaquine (ADQ) and the formation of desethylamodiaquine. The top panel shows the disappearance of amodiaquine in incubations across a panel of rCYPs and the formation of desethylamodiaquine by the same panel of rCYPs. The lower panel, left, shows the correlation of amodiaquine disappearance and desethylamodiaquine formation in a panel of human liver microsomes characterised for CYP2C8 activity. The lower panel, right, shows the inhibitory effect of CYP selective diagnostic inhibitors on the disappearance of amodiaquine in incubations with human liver microsomes
-
(a)
Screening of Compound Metabolism Across a Panel of Recombinant Enzymes
In this experimental setup, the compound is incubated with each of a panel of recombinant CYPs such as CYP1A1, 1B1, 2A6, 2B6, 2C8, 2C9, 2C19, 2D6 and 3A4. The incubation in which the test compound is depleted by over 20% is highlighted as a possible contributor to the compound’s metabolism. The relative contribution of the highlighted enzymes in the metabolism of the test compound is then determined using the relative activity factor. This involves determining the metabolic clearance of enzyme-specific substrate (e.g. midazolam for CYP3A) in human liver microsomes and also with the recombinant enzyme. The ratio of activity in human liver microsomes/activity in recombinant enzyme would be an expression of nanomoles of recombinant enzyme/mg of liver microsomes. This is referred to as the relative activity factor (RAF) as it estimates the relative amount of CYP3A in the liver microsomes in activity terms. The clearance of the test compound is then determined with recombinant enzyme, the value which will be multiplied by the RAF to give the metabolic activity in the clearance of the test compound due to the specific enzyme. To estimate the relative contribution of various CYPs, the test compound is then incubated with the liver microsomes, which gives the total clearance from the contribution of many other CYPs in the microsomes. For the relative contribution of the specific enzyme(s), the activity obtained from multiplying the RAF with the activity of the specific rCYP is then divided by the compound clearance in the liver microsomes. The fraction of the compound metabolised (f m) by the specific CYP will then be expressed as a percentage. Table 7.6 shows the application of the above approach in the metabolism of anti-parasitic drugs by CYPs. This knowledge of which CYPs are responsible for the metabolism of these anti-parasitic drugs enables one to infer pharmacokinetic variability and risk for drug–drug interactions in the clinical use of these drugs.
-
(b)
Correlation Analysis
In this approach, a set of individual human liver microsomes, n = 5–7, is chosen which shows a wide spectrum of activities of each of the major human CYPs. This is done using CYP-specific marker substrate reactions such as CYP1A2 (phenacetin to paracetamol), CYP2A6 (coumarin to 7-OH coumarin), CYP2B6 (efavirenz to 8-OH efavirenz), CYP2C9 (diclofenac to 4-OH diclofenac), CYP2C19 (S-mephenytoin to 4-OH mephenytoin), CYP2D6 (bufuralol to 1-OH bufuralol) and CYP3A4 (midazolam to 1-OH midazolam). In addition to the wide range of activity, the activities of each of the CYPs for the various CYPs should not cross-correlate as this will make it difficult to differentiate the roles of such CYPs. The test compound is then incubated with each of these liver microsomes, and the activities are cross-correlated with the activities of the various CYPs. Cross-correlations of >0.7 are indicative of a significant contribution of that enzyme. Figure 7.12 shows such cross-correlations in the identification of the enzymes responsible for the metabolism of amodiaquine.
-
(c)
Use of Potent and Selective Diagnostic Chemical Inhibitors
This approach exploits the knowledge that there are some compounds which demonstrate potent and selective inhibition of some human CYPs. The test compound is therefore incubated with human liver microsomes in the presence and absence of such inhibitors. The extent of inhibition of the test compound’s clearance is therefore an estimate of the relative contribution of the inhibited enzyme. The most commonly used potent and relatively selective inhibitors are furafylline and α-naphthoflavone (CYP1A2), sulfaphenazole (CYP2C9), ticlopidine (CYP2C19), quinidine (CYP2D6), quercetin (CYP2C8) and ketoconazole (CYP3A). Figure 7.12 shows how this has been used in estimating the relative contribution of CYPs in the metabolism of amodiaquine. These data conclusively identify CYP2C8 as the major enzyme responsible for the metabolism of amodiaquine to its major metabolite, desethylamodiaquine.
7.8.4 In Vivo Pharmacokinetics
Whereas the in silico and in vitro ADMET studies mainly offer mechanistic understanding of pharmacokinetics which is useful in the design of molecules with predicted good PK, in vivo pharmacokinetics are needed to provide a whole system profile of the test compounds. At preclinical stage, various animal models including mice, rat, guinea pig, rabbit, dog and monkey are used to provide pharmacokinetic data on bioavailability, absorption, volume of distribution, half-life and clearance. While these animal models give an integrated outcome of all the PK processes of absorption, distribution and elimination, their major limitation is that of species differences in such processes between them and humans. This is particularly so for metabolic processes where, for most drugs, there are major inter-species differences. This poses a challenge in making allometric scaling predictions of animal PK to human PK. Other parameters such as volume of distributions and protein binding, however, tend to scale relatively well between species. For drugs which undergo rapid metabolism hence have their clearance limited by blood flow instead of metabolism, they also tend to scale better between species.
Against these limitations, the in vivo preclinical PK is, however, still useful in establishing in vitro–in vivo correlations. This is done against the debateable logic that, if in vitro ADME parameters using sub-cellular fractions from a preclinical animal model can be successfully scaled to the in vivo PK data in that animal, then in vitro ADME parameters derived from human sub-cellular fractions will also be predictive of human PK. A lack of correlation would also be interpreted in a similar way. Most importantly, in vivo PK studies are used to establish plasma concentration–effects relationships in disease animal models. This preclinical proof-of-concept data give projects confidence to take compounds through to human studies.
In routine in vivo PK profiling of compounds the test compound is given to 3 animals i.v and another three animals p.o. Samples are collected over a 24-h period, and PK parameters (Table 7.1) are calculated from the plot of drug concentration versus time using PK software such as Winnonlin (http://www.pharsight.com/products/prod_winnonlin_home.php). If in vitro data show that a test compound inhibits a human CYP whose orthologue can be found in preclinical animal models such as CYP1A2, one can conduct preclinical in vivo drug–drug interaction studies. Figure 7.13 demonstrates such an application of in vivo PK studies in the evaluation of the inhibitory effects of medicinal plant extracts that had been shown to be potent inhibitors of human CYP1A2 in vitro. Using caffeine as a marker for CYP1A2 activity, the effects of each herbal extract were evaluated on its pharmacokinetics in rats. Data from such studies could be used to support recommendations of product label revisions with respect to risk for drug–herb interactions.

The pharmacokinetics of caffeine, a marker substrate for CYP1A2, in rats, by itself and after co-administration with various plant extracts with reported in vivo antimalarial effects that had been found to inhibit human CYP1A2 in vitro (Moyo et al. unpublished)
7.8.5 In Vitro to In Vivo Correlation
Most preclinical in silico and in vitro data give information that is generally used in a qualitative manner for SAR and sometimes quantitative manner in QSAR modelling to guide the design of molecules. To gain confidence in the lead compounds selected, efforts are then made to make quantitative in vitro ADME to in vivo PK correlations. This is probably the most difficult part in drug discovery pharmacokinetics since many of the in silico and in vitro animal model systems are fraught with many mechanistic and physiological limitations. The ambitious effort of putting together many pieces of ADME information to predict the in vivo outcome has received enormous attention since its success is the key measure of the usefulness of preclinical DMPK.
7.8.5.1 Absorption (F a)
The absorption rate constant, K a, is determined from in vivo animal PK studies by the method of residuals. It is a difficult parameter to predict since it depends on the formulation used. The average K a from several preclinical animal models is used for humans. K a has a maximum value of 0.1 min−1. K a is useful in the estimation of C max, a value important in the predictions of drug–drug interactions and design of toxicological studies. The software, Gastroplus, which takes into account dissolution properties, can be used to give some estimates of this value.
The fraction absorbed, F a, can be predicted from allometric scaling where rat to human correlations are better than dog to human, with the latter usually over-predicting F a. For many drugs, the in vitro Caco2 permeability measures, P app, show a positive correlation with F a. This is particularly so for drugs whose main mechanism of permeability is passive transcellular. The plot of P app versus F a is, however, very steep in the P app value range of 0.2 and 0.8 × 10−6. This is why the predictions are generally simplified to P app > 1.0 × 10−6 being associated with F a of over 80%. Compounds which undergo active transport or are extensively metabolised in the gut are more difficult to predict from permeability studies using Caco2 cells. Better predictions can be made using pieces of intestinal tissues in an Ussing chamber permeability/absorption system.
The software, Gastroplus, can be used to predict F a where solubility and dissolution rates versus GI transit time are also taken into account. Using this software, more complex modelling that takes into account compound stability in gastrointestinal juice, chemical stability at low pH, efflux, uptake and metabolism in the gut wall can be considered.
The equation used in the prediction of the concentration of drug absorbed is
where C abs—concentration of drug absorbed, C max—maximal plasma concentration, K a—absorption constant, F a—fraction absorbed and Q H—liver blood flow.
7.8.5.2 Volume of Distribution (V d)
Volume of distribution (V d) can be estimated using the simplified Oie–Tozer equation:
where V is volume of distribution, V p is plasma volume, f u is unbound fraction in plasma, V t is volume of tissue and f u,t is the unbound fraction in tissue.
The f u,t, V p and V t for each species can be obtained from the standard data tables found in the literature. The average f u,t in animals is assumed to be equal to f u,t in humans and is used in Eq. (7.2). The plasma protein binding, f u, is measured in vitro using human plasma.
Allometric scaling can then be used to predict V d in humans from animal V d by plotting the total volume in preclinical species (in units of litres per animal) versus animal body weight (kg) on a log–log scale:
The free volume of distribution, V u, can be normalised by taking into account differences in protein binding between species. This normalised value can then be used in the allometric scaling discussed above. Such normalised values tend to give better predictions of V d in humans with a twofold order of magnitude of the real value:
7.8.5.3 Hepatic Clearance (CLH)
Clearance is one of the most important PK parameters because it affects both how much and how often a drug should be administered. When combined with volume of distribution, it gives the half-life, t 1/2 = 0.693 V d/CL, and when combined with fraction absorbed, F a, it gives the bioavailability (F). The relationship with bioavailability is based on the following relationships: CL = Dose i.v/AUC i.v, and F = (AUC p.o/Dose p.o)/(AUC i.v/Dose i.v). Substitutions with CL will then give F = (AUC p.o/Dose p.o) × CL. Successful prediction of drug clearance from preclinical data is therefore of high priority in drug discovery [11].
Against a background where allometric scaling of animal clearance to humans has not been successful, the development of in vitro metabolism models based on human tissues, microsomes and hepatocytes has resulted in improved in vitro–in vivo correlations. The in vitro–in vivo correlation starts by scaling up the intrinsic in vitro clearance, CLint (μl/min/mg liver microsomes or μl/min/million hepatocytes), from the test tube experiment to hepatic clearance per kg (ml/kg) animal model or human body weight. This is done using scaling factors for the various species used in drug discovery (Table 7.7).
The scaling equation for in vivo clearance ( ml/min/kg body weight) is
To estimate hepatic clearance from this intrinsic metabolic clearance, physiological scaling factors such as liver blood flow (Q H), plasma protein binding (PPB) and blood plasma partitioning (B/P) are required. These factors are then input into one of several models for the prediction of hepatic clearance (CLH), the well-stirred model, the dispersion model or the parallel tube model.
In the “well-stirred” or the “venous equilibrium” model, the liver is assumed to be a single “well-stirred” compartment, and the unbound concentration in the venous blood leaving the organ is in equilibrium with and equal to the intracellular unbound concentration in the hepatocytes.
The hepatic clearance, CLH, is expressed as
where CLint is the intrinsic clearance [from Eq. (7.5)], reflecting the actual metabolic capacity of the enzyme system when there is free access to substrate, f uB is the free fraction in whole blood and Q H is the total liver blood flow.
In the parallel tube model, the liver is assumed to be composed of a number of parallel tubes, with enzymes uniformly distributed along the tubes. The unbound blood concentration at any point along the tube is assumed to be in equilibrium with the intracellular unbound concentration:
The dispersion model is even more physiologically “correct” than the other two models in that it also incorporates axial dispersion of blood caused by the branching and connections of the sinusoids. The degree of dispersion is expressed by the dispersion number, Dn. The model assumes that the diffusion of drug along the sinusoids is much more rapid than the blood transit through the liver. At its two extremes, the dispersion model collapses to either the parallel tube model (\( {\hbox{Dn}} \to 0 \)) or the well-stirred model (\( {\hbox{Dn}} \to \infty \)). The elimination capacity is expressed by the efficiency number Rn:
The mathematical expression is more complex than for the other two models:
where a = (1 + 4RnDn)1/2.
The difference between these three liver models is in their description of the concentration profile across the liver. This has most effect for high clearance compounds, which results in the highest difference in concentration across the liver. A comparison of the predictive value of the three models was studied for 28 compounds, and none of the models gave consistently better results than the other models. Since the well-stirred model is the simplest in nature, it has become the one most commonly used.
In general practice in pharmacokinetic studies, we measure plasma clearance and make the assumption that the B/P is 1.0. This might not be true for some drugs such as chloroquine and some 4-aminoquinolines which tend to partition into red blood cells. For these drugs, plasma clearance is not equal to blood clearance. In general, we also assume that binding to microsomes or cellular components is not important, but for some drugs, clearance predictions are improved by taking into account binding to in vitro biological components. Correction of microsomal binding significantly improves the prediction of clearance of acidic compounds. The ideal equation for the prediction of clearance is therefore
Using this equation, it is clear that the clearance of a drug cannot be greater than the blood flow through that organ. For compounds with very high intrinsic clearance, the equation reduces to CLb = Q H, and for low instrinsic clerance drugs, the equation reduces to CLb = CLint. Compounds are then ranked as low clearance (<25% Q H) or high clearance (>75% Q H).
7.8.5.4 Bioavailability (F)
Bioavailability is determined by both absorption and hepatic clearance:
where CLH/Q H = extraction ratio.
In a scenario where there is complete absorption and no gut metabolism, bioavailability will be equal to 1−extraction ratio (E). For cases where this is not so, one needs to calculate the concentration of the drug that is absorbed, C abs, using Eq. (7.1):
At the preclinical stages, K a can be calculated from animal model PK studies and assumed to be the same in humans; F a, fraction absorbed, can be estimated from Caco2 permeability studies. Estimation of human bioavailability from preclinical animal by allometric scaling is generally not good but is reasonable with data from monkey studies.
7.8.5.5 Half-Life (t 1/2)
The half-life along with the therapeutic index and the PK–PD relationship dictates the dosing frequency. It is also used in attempts to estimate human C max, hence important for safety and CYP inhibition studies. Combining CL and V d at steady state (V ss) gives the effective half-life: t 1/2 = 0.693 V d/CL. Allometric prediction of half-life from preclinical animals generally under-predict this parameter, with human half-lives being >5-fold higher than those in rats and threefold higher than in dogs and monkeys. Use of in vitro data for CL from human cellular and sub-cellular systems and in vivo V ss from preclinical animal models gives improved results for half-life in humans.
7.9 Drug–Drug Interactions
Metabolism-based drug–drug interaction (DDI) is responsible for clinically important safety and efficacy issues in the use of medicines. Inhibition is generally associated with increased plasma concentration of the victim drug which might result in increased incidences and severities of adverse drug reactions (ADRs). On the other hand, induction generally results in reduced plasma levels of the victim drugs which might result in sub-therapeutic concentration which can promote the emergence of drug resistance in the treatment of infectious diseases. Prediction of the effects of induction is still qualitative while that for inhibition can now be done quantitatively. In this chapter, we will present the approaches used in the prediction of inhibition based drug–drug interactions.
With the data generated from in vitro experiments on the IC50, inhibition constant (K i), mechanism of inhibition and estimated pharmacologically effective concentration, EC50, one can make predictions of the likelihood of enzyme inhibition based drug–drug interactions in the early phases of drug discovery. The Food and Drug Administration, FDA, has already come up with comprehensive guidelines on the determination of the risk for DDIs (http://www.fda.gov/cder/guidance/index.htm). For general evaluations of DDIs, one can use the assumption that effective plasma concentrations will be around 1.0 μM for the selective and potent new chemical entities. This assumption should be used with caution and re-evaluate compounds for DDI risk as PK/PD studies generate a more accurate estimation of likely plasma concentrations.
The simple prediction equation is therefore [I]/K i, where [I] is the concentration of inhibitory test compound. The value to use for this concentration is a highly debated point as it can be total C max, C ss, unbound C max, C ss, total or unbound I max (the concentration entering the liver from the portal vein). FDA guidelines are based on total plasma concentrations, C max, but most researchers are increasingly using the unbound concentration entering the liver. FDA has ranked the risk for inhibition based on the above assumption as follows:
K i | I/K i | In vivo interaction |
|---|---|---|
Reversible mechanism | ||
<1 μM | >1 | Highly likely |
1–50 μM | 0.1–1 | Possible |
>50 μM | <0.1 | Remote |
A more accurate way of quantifying DDI is to determine the extent of inhibition as the reduction in clearance or increase in AUC. This can be achieved using the following equations:
With the assumption that in vivo, drug concentrations (S) will be much lower than K m, the fractional inhibition reduces to [I]/([I] + K i). The decrease in clearance or increase in AUC can then be estimated by the equation:
Since most drugs are eliminated by many routes, the equation needs to take into account the fraction of the drug’s clearance, f m, which is by the inhibited enzymes. The fraction of the metabolic route (f m) inhibited is very important in estimating the risk for DDI. f m > 0.8 is associated with high risk for DDI since the metabolism of the affected drug significantly depends on the affected enzyme. AUC increases of >2-fold are associated with high risk for DDI.
In the early phases of drug discovery, when IC50 only are determined, one can estimate the K i for competitive inhibition as the worst case scenarios where K i = IC50/2. For non-competitive inhibition, K i = IC50.
For the estimation of inlet concentration, the following equation is used:
Assuming C max to be the effective concentration interacting with the drug-metabolising enzymes, we have estimated the likelihood of DDI in the use of anti-parasitic drugs. Using the simple model of C max, we have estimated the likelihood of DDI in the use of anti-parasitic drugs (Table 7.8). In vivo studies on the inhibitory effects of thiabendazole and artemisinin on CYP1A2-mediated metabolism confirmed these in vitro data. Thiabendazole and artemisinin inhibited the formation of paraxanthine from caffeine by 92% and 66%, respectively [12].
7.10 Lead Optimisation
The lead optimisation stage utilises all in silico, in vitro and in vivo tools to build knowledge that can guide the medicinal chemists in addressing ADME issues in the selected series and enable PK scientists to make first dose in man predictions of new chemical entities. Before the onset of lead optimisation (LO), the candidate drug target profile (CDTP) must be formulated with respect to oral bioavailability, clearance, effective half-life, therapeutic dose, drug–drug interactions caused by the CD and risk for the generation of reactive metabolites. These can differ significantly depending on the intended use of the drug, e.g. if the drug is aimed at long duration of action, then the design must aim for a drug with a larger half-life (t 1/2) and a smaller elimination rate constant (K el). If on the other hand a drug is too toxic or is required for a short duration of action, the design should aim for a smaller half-life and larger elimination rate constant. For a typical once-daily oral drug, the CDTP has generally a bioavailability of >25% to reduce the risk of large variability and a dose size of <300 mg to ensure that it fits in average-size tablet. Other CDTP goals are a low risk for reactive metabolites, minimal or reduced enzyme or transporter inhibition or induction to avoid drug–drug interactions.
During lead optimisation, iterations of DMPK and pharmacological evaluations, design of molecules and synthesis of molecules define a high point in the creative process of drug discovery (Fig. 7.14). The depicted movement of compounds and information shows an integrated paradigm that has come to characterise most drug discovery approaches used by leading pharmaceutical companies. This approach requires multidisciplinary teams that are tightly coupled to each other for rapid data turn-around times, design and implementation strategies.

The integrated drug discovery paradigm that is driven by a tight interplay of DMPK, medicinal chemistry and pharmacology [14]
The variables described in this chapter clearly indicate that the ADME process is dependent on a host of chemical properties. It is also evident that lipophilicity (the tendency of a compound to partition into a non-polar lipid matrix versus an aqueous matrix) has a major impact on all the ADME processes, making it one of the most important parameters determining both drug pharmacokinetics and pharmacodynamics. It has been shown to correlate with compound solubility, permeability, metabolism, protein binding, distribution and pharmacologic potency. This property has resulted in the so-called physicochemical dilemma where it positively correlates with parameters which require opposite optimisation directions. For example, high lipophilicity is predictive of poor solubility but predictive of good permeability, yet one needs both good solubility and permeability for good oral absorption. High lipophilicity positively correlates with metabolic instability, high enzyme inhibitory effects and high drug target potency, making it difficult to independently optimise for these parameters. These are some of challenges lead optimisation scientists will have to solve towards the nomination of a candidate drug with predicted good PK/PD properties for the first time in human studies. The preclinical ADME and PK parameters culminate in dose in man estimation (Fig. 7.15).

Equation for dose estimation showing the importance of clearance and bioavailability
7.11 Conclusions
The ADME and PK studies discussed in this chapter are now an integral part of the drug discovery efforts in Africa where they guide medicinal chemistry and pharmacology in the design and eventual selection of candidate drugs predicted to be safe and efficacious in humans. Figure 7.14 shows the new paradigm of drug discovery where ADME and PK have evolved from descriptive sciences to predictive sciences that are contributing to the reduction of attrition rates of new chemical entities. For the pharmaceutical industry, integration of DMPK in drug discovery and development has successfully addressed this parameter as a hurdle in this complex and expensive process. It has left issues of therapeutic efficacy and toxicity as outstanding causes of high attrition rates of new chemical entities. Continued ADMET/PK research is needed to tease out its contribution to the continuing challenge of poor efficacy and idiosyncratic reactions associated with some new chemical entities.
For Africa, there is need to have more laboratories and institutions with knowledge and technical capacity to provide ADME/PK support to drug discovery projects. The successful effort at AiBST can be used as a template for the promotion of ADMET/PK on the continent. Drug discovery activities in Africa are projected to increase in the framework of the African Network for Drug and Diagnostic Innovation (ANDI) which was recently initiated (http://www.andi-africa.org). AiBST will contribute to ANDI projects through support of medicinal chemistry- and pharmacology-driven projects with ADME/PK input and services. New applications of ADME/PK towards the safe and efficacious use of herbal medicines are also under development at AiBST. Preliminary studies have resulted in the setup of in vitro and in vivo platforms for the evaluation of herbal medicines for drug–herb metabolic interactions [15]. In yet another innovative approach, we have initiated collaborations with medicinal chemists in implementing ADMET-guided drug discovery from natural products and through rescuing of old drugs by addressing their ADMET liabilities [16]. Our work on amodiaquine aims at addressing the toxicity issues associated with the antimalarial whilst our work on praziquantel aims at addressing the issue of low oral bioavailability associated with this antischistosomicide. With respect to pharmacogenetics of drug metabolism, our work is showing that for some drugs such as efavirenz, the genetic polymorphism of CYP2B6, the enzyme responsible for the drug’s metabolism and elimination, could be a clinically relevant biomarker in personalising the treatment of HIV/AIDS patients. These developments are further expanding the utility of ADMET/PK in drug discovery, development and rational clinical use of medicines.
Abbreviations
- ADMET:
-
Absorption, distribution, metabolism, excretion and toxicity
- AiBST:
-
African Institute of Biomedical Science and Technology
- AUC:
-
Area under the curve
- CL:
-
Clearance
- C max :
-
Maximum plasma concentration
- DME:
-
Drug-metabolising enzymes
- DMPK:
-
Drug metabolism and pharmacokinetics
- F a :
-
Fraction absorbed
- f u :
-
Fraction unbound
- HPGL:
-
Hepatocytes per gram of liver
- HTS:
-
High-throughput screening
- IVIVE:
-
In Vitro to in vivo extrapolation
- K el :
-
Elimination rate constant
- LD:
-
Lead discovery
- LO:
-
Lead optimisation
- MPPG:
-
Microsomal protein per gram
- NCEs:
-
New chemical entities
- PD:
-
Pharmacodynamics
- PK:
-
Pharmacokinetics
- PSA:
-
Polar surface area
- QSAR:
-
Quantitative structure activity relationship
- SAR:
-
Structure activity relationship
- t 1/2 :
-
Half-life
- TDI:
-
Time-dependent inhibition
- T max :
-
Time to reach maximum plasma concentration
- V d :
-
Volume of distribution
References
Prentis RA, Lis Y, Walker SR (1988) Pharmaceutical innovation by the seven UK-owned pharmaceutical companies (1964–1985). Br J Clin Pharmacol 25:387–396
Kola I, Landis J (2004) Can the pharmaceutical industry reduce attrition rates? Nat Rev Drug Discov 3:711–716
Kerns EH, Di L (2008) Drug-like properties: concepts, structure design and methods. From ADME to toxicity optimisation. Elsevier, Amsterdam
Ana Ruiz-Garcia A, Bermejo M, Moss A et al (2008) Pharmacokinetics in drug discovery. J Pharm Sci 97:654–690
Gilbaldi M (1975) Biopharmaceutics and clinical pharmacokinetics. Lea & Febiger, Philadelphia
Masimirembwa CM, Otter C, Berg M et al (1999) Heterologous expression and kinetic characterization of human cytochromes P-450: validation of a pharmaceutical tool for drug metabolism research. Drug Metab Dispos 27:1117–1122
Li XQ, Björkman A, Andersson TB et al (2003) Identification of human cytochrome P(450)s that metabolise anti-parasitic drugs and predictions of in vivo drug hepatic clearance from in vitro data. Eur J Clin Pharmacol 59:429–442
Thelingwani RS, Zvada SP, Hugues D et al (2009) In vitro and in silico identification and characterisation of thiabendazole as a mechanism-based inhibitor of CYP1A2 and simulation of possible pharmacokinetic drug-drug interactions. Drug Metab Dispos 37:1286–1294
Johansson T, Jurva U, Grönberg G et al (2009) Novel metabolites of amodiaquine formed by CYP1A1 and CYP1B1: structure elucidation using electrochemistry, mass spectrometry, and NMR. Drug Metab Dispos 37:571–579
Jurva U, Holmén A, Grönberg G et al (2008) Electrochemical generation of electrophilic drug metabolites: characterization of amodiaquine quinoneimine and cysteinyl conjugates by MS, IR, and NMR. Chem Res Toxicol 21:928–935
Masimirembwa CM, Bredberg U, Andersson TB (2003) Metabolic stability for drug discovery and development: pharmacokinetic and biochemical challenges. Clin Pharmacokinet 42:515–528
Bapiro TE, Sayi J, Hasler JA et al (2005) Artemisinin and thiabendazole are potent inhibitors of cytochrome P450 1A2 (CYP1A2) activity in humans. Eur J Clin Pharmacol 61:755–761
Bapiro TE, Egnell AC, Hasler JA et al (2001) Application of higher throughput screening (HTS) inhibition assays to evaluate the interaction of antiparasitic drugs with cytochrome P450s. Drug Metab Dispos 29:30–35
Masimirembwa CM, Thompson R, Andersson TB (2001) In vitro high throughput screening of compounds for favorable metabolic properties in drug discovery. Comb Chem High Throughput Screen 4:245–263
Gwaza L, Wolfe AR, Benet LZ et al (2009) In vitro inhibitory effects of Hypoxis obtusa and Dicoma anomala on cyp450 enzymes and pglycoprotein. Afr J Pharm Pharmacol 3:539–546
Chibale K, Guantai E, Masimirembwa C (2011) Extracting molecular information from African natural products to facilitate unique African-led drug-discovery efforts. Future Med Chem 3:257–261
Lipinski C, Lombardo F, Dominy BW et al (1997) Experimental and computational approaches to estimate solubility and permeability in drug discovery and development settings. Adv Drug Deliv Rev 23:3–25
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2012 Springer Berlin Heidelberg
About this chapter
Cite this chapter
Masimirembwa, C., Thelingwani, R. (2012). Application of In Silico, In Vitro and In Vivo ADMET/PK Platforms in Drug Discovery. In: Chibale, K., Davies-Coleman, M., Masimirembwa, C. (eds) Drug Discovery in Africa. Springer, Berlin, Heidelberg. https://doi.org/10.1007/978-3-642-28175-4_7
Download citation
DOI: https://doi.org/10.1007/978-3-642-28175-4_7
Published:
Publisher Name: Springer, Berlin, Heidelberg
Print ISBN: 978-3-642-28174-7
Online ISBN: 978-3-642-28175-4
eBook Packages: Chemistry and Materials ScienceChemistry and Material Science (R0)