
Abstract
Although it is the most voluminous plain organ, the liver is rarely a target for emergency therapeutic decisions in the critically ill. When the liver is located high, intercostal scans should be taken. Liver analysis is not exhaustive in such conditions, but this limitation has little consequence in the critically ill patient. Our 5-MHz microconvex probe is perfect for scanning the liver, especially for intercostal scans. We do not use abdominal probes. Their only use seems to be for accurate measurement of hepatic size, which is a tool of interest for the radiologist but not yet a tool for the intensivist. Unexpected uses may emerge from knowing the size of the liver, but this can be achieved using our probe.
Access provided by Autonomous University of Puebla. Download chapter PDF
Keywords
These keywords were added by machine and not by the authors. This process is experimental and the keywords may be updated as the learning algorithm improves.
Although it is the most voluminous plain organ, the liver is rarely a target for emergency therapeutic decisions in the critically ill.
When the liver is located high, intercostal scans should be taken. Liver analysis is not exhaustive in such conditions, but this limitation has little consequence in the critically ill patient.
Our 5-MHz microconvex probe is perfect for scanning the liver, especially for intercostal scans. We do not use abdominal probes. Their only use seems to be for accurate measurement of hepatic size, which is a tool of interest for the radiologist but not yet a tool for the intensivist. Unexpected uses may emerge from knowing the size of the liver, but this can be achieved using our probe.
Portal Gas
This diagnosis may be the main reason for scanning the liver in a shocked patient, since it immediately evokes the mesenteric infarction and allows immediate therapy with, in our experience, a possibility of healing. Portal gas usually requires immediate surgery [1, 2]. Portal gas is traditionally considered a pejorative sign [3], but this feeling is based on a radiographic culture. More sensitive than radiography [1], ultrasound allows the patient to from an early diagnosis. Portal gas has been described, in the adult, in volvulus, strangulation, ulcerous colitis, and intra-abdominal abscesses, which are always surgical emergencies [3].
We consider two signs of portal gas.
-
1.
Static portal gas. This term refers to punctiform hyperechoic images (without acoustic shadow), which are disseminated within the liver parenchyma and usually are peripheral. Static portal gas looks like an alveolar consolidation with air bronchograms (Fig. 7.1).
Fig. 7.1 
Mesenteric infarction and static portal gas. Numerous hyperechoic punctiform opacities, without acoustic shadow, within the liver. This patient survived (perhaps because of an early diagnosis)
-
2.
Dynamic portal gas. This term refers to the detection of mobile hyperechoic particles within the portal vein (Fig. 7.2). Showing such a flow coming from the superior mesenteric vein and not from the splenic vein clearly indicates that the gas bubbles come from the GI tract. Particles that are echoic but not hyperechoic (like gas) have a differential diagnosis (possibly cell and platelet aggregations).
Fig. 7.2 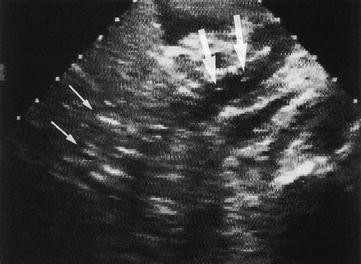
Mesenteric infarction with dynamic portal gas. A visible flow with hyperechoic particles (large arrows) is observable in the portal vein. Static portal gas can be seen (small arrows). Oblique scan of the right hypochondrium, in the axis of the portal vein (large arrows). Patient was a 70-year-old woman with septic shock


Confusion may result from aerobilia, which yields numerous air opacities. Aerobilia is a subtle diagnosis for radiologists, since the air collections are visible along the biliary vessels, which converge to the hilum, which is a more central location than in portal gas. Aerobilia can be physiologic\after biliary surgery, but rarely pathologic (ileus by impacted gallstone). Grotowski’s law elegantly solves this problem. A septic shock often requires laparotomy. Aerobilia is rare. Aerobilia without previous biliary history (simply detected by the surgical scar) is even more infrequent. In these conditions, gas in the liver is nearly always aeroportia. From the small number of patients for whom an erroneous diagnosis of aeroportia (patients who had simple aerobilia) ordered surgery, we must withdraw the patients for whom the surgery was useful, finding the real cause of sepsis. The level of morbidity following useless laparotomy is probably not zero, but certainly is low. All these factors are mutiplied by one another, resulting in a nearly negligible number of complicated laparotomies, compared with an optimal rate of well-indicated laparotomies.
Hepatic Abscess
Although a rare diagnosis, ultrasound is a quick and user-friendly method of diagnosis, since it spares the highly unpleasant pain caused by liver shaking. Yet pain can be absent in encephalopathic, shocked patients, hence the interest in a systematic fast ultrasound examination for any critically ill patient on admission.
An abscess yields a roughly round image within the regular hepatic echostructure (Fig. 7.3). It has a heterogeneous, usually hypoechoic echostructure. A characteristic sign is sometimes observed within the mass: a slow internal movement, in rhythm with respiration. This is the inertia of the pus caused by the movement, the equivalent of the plankton sign discussed in Chap. 5. In our observations, it proves the fluid nature of the collection (regardless of the presence or absence of posterior enhancement), and it indicates pathological fluid (pus, blood). Highly echoic images, if present, indicate microbial gas. Amoebic abscess yields a hypoechoic, well-limited collection.

Hepatic abscess. Huge round hypoechoic mass, which in real-time has a slow internal motion, characteristic from a fluid nature. Percutaneous ultrasound-guided drainage (see Fig. 26.3 page 263) has withdrawn 1,150 cc of frank pus (Streptococcus milleri)
Hydatidosis should be classically evoked before any puncture of fluid hepatic mass. This does not cause a problem when the cyst is well defined and anechoic, since there is no emergency, but it may in the suppurative forms, when the cyst becomes echoic and heterogeneous (Fig. 7.4).

Hydatid cyst of the liver. The heterogeneous pattern (arrowheads) indicates a complication, here suppuration, which was confirmed at the laparotomy of this 45-year-old man in septic shock. Longitudinal scan of the liver. L, liver
Isolated Hepatomegaly
Some operators may evaluate the weight of each lobe. Others find that a subjective view is sufficient [4]. Measuring the liver makes ultrasound an expert discipline. The cause of an enlargement usually appears on the screen: acute right heart failure yields a homogeneous pattern with dilated hepatic veins, inferior vena cava, and right heart chambers (Fig. 7.5). Abscesses and tumors will be usually detected without problem. We will describe the steatosic liver here, but interested readers can find a portion of fatty liver in Fig. 6.7 page 45.

Cardiac liver in right heart failure. Dilatation of the three hepatic veins, which open into an inferior vena cava (V), also dilated. Note that this scan is far from the ideal site where the IVC caliper should be measured (see Figs. 4.2 and 23.4). Epigastric subtransverse scan
The cirrhotic liver yields a coarse or nodular pattern, atrophy or hypertrophy of one lobe with resulting global dysmorphia, absence of suppleness of the parenchyma, signs of portal hypertension with dilatation of the portal vein, ascites, reopening of the umbilical vein, splenomegaly (see Fig. 10.6 page 78) and others. Please call a radiologist who knows these signs and can sharply measure a liver. See Fig. 6.12 page 47 for an illustration of esophageal varices.
Diffuse Infectious Disorders
Tuberculous hepatic miliary can be missed by ultrasound (Fig. 7.6). When there is strong clinical suspicion, a prompt liver biopsy should provide bacteriological confirmation.

Diffuse tuberculous miliary. In this longitudinal scan of the liver and the kidney (K), it is hard to detect frank anomalies. Real-time showed that the liver parenchyma pattern was homogeneously granular, but one can consider it as a subtle sign– requiring experience
Cholestasis
Cholestasis often occurs in ventilated patients. Ultrasound is a quick way to check for the bile ducts. Yet in our observations, the cause of cholestasis is always medical: for example, sepsis, impairment of venous return, drug interactions. We are still awaiting a surgical cause of cholestasis in a patient initially admitted in the ICU for a medical reason. We therefore advise the non-radiologist to invest energy in priority targets (lung, etc.) and call the radiologist in this setting in order not to lose time.
The intrahepatic duct is anterior to the portal bifurcation (Fig. 7.7) and the main duct anterior to the portal vein (Fig. 7.8). The maximal normal caliper of the main bile duct is said to be 7 mm for some (up to 12 mm in the case of an old cholecystectomy), but 4 mm for others authors [5]. A dilated common bile duct acquires a tortuous route and cannot be visualized in a single view. The sensitivity of ultrasound is limited for detection of common bile duct calculi, which rarely produce posterior shadows, even if massive [6].

Dilatation of intrahepatic bile ducts. Biliary vessels (X) are visible anterior to portal bifurcation (V), producing a double-channel pattern

Dilatation of the common bile duct. Anterior to the portal vein (V), the common bile duct (arrow) is dilated (9-mm caliper). Oblique scan of epigastric area. G, gallbladder
Hepatic Veins
Ultrasound is a noninvasive method for examining hepatic veins [7]. They are easy to analyze when anechoic and surrounded by echoic hepatic tissue (Fig. 7.5). They can often be compressed using probe pressure (look out for painful sensitivity in those patients being seen for abdominal pain). In critically ill patients, frequent right heart failure or liberal fluid therapy makes hepatic veins appear more easily. In hepatic vein thrombosis (Budd-Chiari syndrome), the veins are filled with echoic material. They can therefore appear filiform or even isoechoic to the liver. The inclusion of other signs would deviate too far from our aim (critical ultrasound, a simple discipline).
The Budd-Chiari syndrome is a rare cause of acute abdominal pain, at least in our institutions. The frequent causes will be usually detected using simple ultrasound. The detection of nonanechoic veins in a patient who is really suspect for hepatic vein thrombosis makes ultrasound extremely contributive. The decision of providing a unit with Doppler for this sole indication would condemn the user to very rarely exploit this potential. If the suspicion is high, then and only then may DIAFORA logistics (referral to an outside Doppler examination) be envisaged.
In critically ill patients, mobile gas is sometimes observed in the median and left hepatic veins, which are the nondependent veins (Fig. 7.9). Maybe air accidentally coming from perfusions (in the arms, for instance) is trapped in these veins. A tricuspid regurgitation, frequent in the mechanically ventilated patient, may be the cause.

Hyperechoic structure, highly dynamic in real-time, is visible at the median hepatic vein (arrows). Trapped air in the hepatic venous system. Subtransverse epigastric scan acquired with an Ausonics 2000 unit (a 39-cm width, 14-kg machine – although of limited resolution)
Hepatic Tumors
Metastases are sometimes a fortuitous discovery. This recognition may be useful in some cases. Multiple disseminated images with random distribution, isoechoic, hyperechoic with a fine hypoechoic stripe, or again hypoechoic images are possible (Fig. 7.10). Other tumors do not need particular management during the stay in the ICU. A round, regular, anechoic image is generally a biliary cyst, sometimes an uncomplicated hydatid cyst. An echoic heterogeneous mass within a cirrhotic parenchyma will be suggestive of hepatocarcinoma. These tumors and others (adenoma, focal nodular hyperplasia, angioma, primitive malignant tumors, heterogeneous steatosis, etc.) are extensively described in excellent textbooks [4, 8, 9]. We should here refer the patient to imaging specialists.

Hepatic metastases. Hypoechoic masses, disseminated in the liver, surrounded by peritoneal effusion (asterisk)
Trauma
Direct signs of liver contusion can be detected in favorable cases (see Fig. 28.4 page 275).
Interventional Ultrasound
We successfully aspirate from time to time hepatic abscesses with the material described in Chap. 26. Too deep locations or locations near the dome may cause technical problems.
Percutaneous or Transjugular Liver Biopsy
Liver biopsies are not performed in the ICU. Using our simple equipment, it is possible to monitor this procedure at the bedside. Some indications can be imagined in the ICU: documenting fulminans hepatitis or suspected diffuse tuberculosis, having a definitive proof of malignancy if this can alter management. Usually, hemostasis disorders require a transjugular approach, which means transportation of a critically ill patient to a specialized center. Yet transjugular hepatic biopsy could be performed at the bedside under sonographic guidance, with a triple impact: immediate catheterization of the internal jugular vein (see Chap. 12); ultrasound guidance toward the target; and accurate guidance to an hepatic vein. Ultrasound works in the three dimensions and thereby is better than radioscopy, which gives a nice overview but works in only two dimensions, with occasional hemorrhagic accidents.
References
Lee CS, Kuo YC, Peng SM et al (1993) Sonographic detection of hepatic portal venous gas associated with suppurative cholangitis. J Clin Ultrasound 21:331–334
Traverso LW (1981) Is hepatic portal venous gas an indication for exploratory laparotomy? Arch Surg 116:936–938
Liebman PR, Patten MT, Manny J (1978) Hepatic portal venous gas in adults. Ann Surg 187:281–287
Menu Y (1986) Hépatomégalies. In: Nahum H, Menu Y (eds) Imagerie du foie et des voies biliaires. Flammarion, Paris, pp 86–96
Berk RN, Cooperberg PL, Gold RP, Rohrmann CA Jr, Ferrucci JT Jr (1982) Radiography of the bile ducts. A symposium on the use of new modalities for diagnosis and treatment. Radiology 145:1–9
Weill F (1985) L’ultrasonographie en pathologie digestive. Vigot, Paris
Menu Y, Alison D, Lorphelin JM, Valla D, Belghiti J, Nahum H (1985) Budd-Chiari syndrome, ultrasonic evaluation. Radiology 157:761–764
Taboury J (1989) Echographie abdominale. Masson, Paris
Weill F (1985) L’ultrasonographie en pathologie digestive. Vigot, Paris, pp 455–456
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
Copyright information
© 2010 Springer-Verlag Berlin Heidelberg
About this chapter
Cite this chapter
Lichtenstein, D.A. (2010). Liver. In: Whole Body Ultrasonography in the Critically Ill. Springer, Berlin, Heidelberg. https://doi.org/10.1007/978-3-642-05328-3_7
Download citation
DOI: https://doi.org/10.1007/978-3-642-05328-3_7
Published:
Publisher Name: Springer, Berlin, Heidelberg
Print ISBN: 978-3-642-05327-6
Online ISBN: 978-3-642-05328-3
eBook Packages: MedicineMedicine (R0)