
Abstract
The search for detection of a peritoneal effusion or a pneumoperitoneum is of critical importance in the critically ill patient. The peritoneum covers the major part of the gastrointestinal (GI) tract, abdominal organs, and the abdominal wall. The abdomen is an area where, traditionally, gas collections have discouraged the operators. The static and dynamic analysis of the air will be used for prompting life-saving diagnoses anyway. The abdomen was dealt with before the lung chapters, which standardize this semiotic of air. Meanwhile, one practical suggested label for designating the abdominal gas structures is the term “G-lines” – G for gut.
Access provided by Autonomous University of Puebla. Download chapter PDF
Keywords
These keywords were added by machine and not by the authors. This process is experimental and the keywords may be updated as the learning algorithm improves.
The search for detection of a peritoneal effusion or a pneumoperitoneum is of critical importance in the critically ill patient. The peritoneum covers the major part of the gastrointestinal (GI) tract, abdominal organs, and the abdominal wall. The abdomen is an area where, traditionally, gas collections have discouraged the operators. The static and dynamic analysis of the air will be used for prompting life-saving diagnoses anyway. The abdomen was dealt with before the lung chapters, which standardize this semiotic of air. Meanwhile, one practical suggested label for designating the abdominal gas structures is the term “G-lines” – G for gut.
A 5-MHz microconvex probe is perfect for investigating the peritoneum.
Positive Diagnosis of Peritoneal Effusion
Ultrasound diagnosis of peritoneal effusion is a basic point that, for many, embodies the place of ultrasound as a tool for the emergency physician (the search for free blood). Peritoneal effusion gives characteristic patterns.
-
1.
Dark echogenicity is an accessory sign. In fact, depending on the etiology (blood, digestive fluids, pus), the liquid can be frankly echoic.
-
2.
Location. In ventilated patients in the supine position, the effusion can collect roughly everywhere. Radiologists have described five sites, which were taken again by some surgeons. In our opinion, this corresponds to a typical application of ultrasound for sonographers (i.e., 3-year post-graduates), who are required to make extremely standardized views in order to allow the radiologist to make a report. Ultrasound performed by one and read by another is not critical ultrasound. We have heard of these windows but are accustomed to simply make a liberal ultrasound scanning protocol instead of searching those windows. This being said, we will nonetheless describe usual sites (Fig. 5.1).
Fig. 5.1 
The five classical areas where peritoneal effusion are traditionally searched for: (a) right hypochondrium, (b) right flank, (c) pelvis, (d) left flank, (e) left hypochondrium. Note that we placed arrows A and E in the intercostal spaces, not under the ribs

The diaphragm must be localized in order to avoid any confusion with pleural effusion (Fig. 5.2). See Chap. 14 page 119 for basic details.

Voluminous suprahepatic effusion, longitudinal scan. The cupola (arrow) is separated from the liver (L) by the effusion, which means peritoneal location of the effusion. The anechoic pattern is suggestive of a transudate
The effusion is searched for:
-
Surrounding the liver. One can explore the last intercostal spaces, where the pattern is characteristic (Fig. 5.3). We immediately emphasize this very upper location, at the intercostal spaces.
Fig. 5.3 
Minute prehepatic peritoneal effusion (black arrows), on intercostal scan. Here anechoic effusion, whose thickness varies with the respiratory cycle (yielding a sinusoid). An exploratory puncture at this level is fully feasible. This figure also indicates the adrenal space (white arrows) for the Chap. 10
-
Surrounding the spleen, with the same comment (Fig. 5.4).
Fig. 5.4 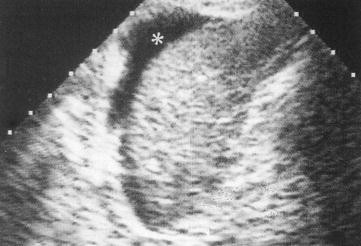
Perisplenic effusion (asterisk), clearly identified although minimal. The moon shape, between the spleen and diaphragm, is a minimal equivalent of the bat wing sign. Longitudinal scan
-
At the flanks.
-
In the pelvis (Douglas pouch) (Figs. 5.5 and 9.13 page 73).
Fig. 5.5 
This substantial pelvic effusion isolates the uterus (U) and the ligamentum teres. Transversal subpubic scan



Morrison’s pouch is a familiar area, easy to standardize, but usually redundant when liberal ultrasound scanning is performed.
-
3.
The shape is characteristic. The collection has an outside convexity and inside concavities, since they surround intraperitoneal organs such as liver, gallbladder, urinary bladder, GI tract, etc. (Fig. 5.6). For this basic sign, we suggest the label of the bat wing sign (Fig. 5.7) – distinct from the bat sign (see Chaps. 14–19). Conversely, encapsulated fluids (gallbladder, urinary bladder, renal cyst, digestive fluid, etc.) have only convex limits. A fluid image with convex limits outside cannot correspond to free peritoneal effusion. A scanning of the area shows that a peritoneal effusion is an open structure, whereas an encapsulated fluid gives a closed shape (this image appears and then disappears during scanning).
Fig. 5.6 
Substantial pelvic effusion. Illustration of the bat wing sign (see Fig. 5.7). The effusion allows a fine analysis of the bowel loops: wall, here fine and regular, without villi (ileal type); content: echoic and homogeneous
Fig. 5.7 
The bat wing sign. It is illustrated, from Fig. 5.6: each border is concave inside. When the effusion is echoic, this sign has major relevance


Special comment: In the pelvis, in a hasty transversal scan, a peritoneal effusion may simulate a half-full urinary bladder, with roughly square section (see Fig. 9.13 page 73). The fluid is collected in the Douglas pouch, which cannot generate any bat wing sign. Two keys are available to easily get out of this slight pitfall: scanning this transversal image using a large Carmen maneuver to check simply whether the top is closing (bladder) or opening (peritoneum); or remaining longitudinal to obtain the same answer (convex or concave angles at the left of the image).
-
4.
Dynamic patterns. We will see in Chap. 15 that a pleural effusion yields a sign called the sinusoid sign, due to the changes of volume of the lung. At the abdominal level, there is no lung, but the probe can exert (if not hurting) a small pressure that will result in decreasing the size of the effusion. A suggestive term for this characteristic pattern is the induced sinusoid sign (Fig. 5.8). Bowel loops swimming within the effusion are an equivalent of this sign.
Fig. 5.8 
Induced sinusoid sign. Left: suspicion of peritoneal effusion, in spite of the rather echoic pattern. Right: M mode. Slight pressures by the probe create this sinusoidal pattern, indicating that the image is not solid

Ultrasound sensitivity is high for detection of even minimal effusions [1]. A substantial effusion will fill the entire peritoneal cavity and outline the organs. Bowel loops thus become easier to analyze.
Perihepatic effusions can be distinguished from pleural effusions provided the intercostal approach is used, thus first detecting the diaphragm (Figs. 5.2 and 15.4 page 131). When the subcostal route was used, the notion that only a pleural effusion could locate behind the inferior vena cava still works (see Fig. 15.1 page 129).
Last, ultrasound easily rules out what physical examination wrongly interprets as an effusion. Ultrasound regularly allows us to avoid inserting a needle in cases of agglutination of bowel loops with fluid contents, which clinically simulates free fluid (Fig. 5.9).

A slight clinical pitfall. This patient had hydric dullness in the left iliac fossa. An ultrasound examination precluded a puncture, which would have been unproductive or even... bloody. It shows absence of peritoneal effusion and several agglomerated bowel loops (I) with fluid inside
Diagnosis of the Nature of the Effusion
In the ICU, peritoneal effusions are frequently observed (38% in our initial series). The anechoic tone usually indicates a transudate, but can be observed in exudates and hemoperitoneum. Obstacle to venous return (e.g., mechanical ventilation, right heart failure), capillary leakage, or portal hypertension are possible causes of transudate. Most of these etiologies have characteristic ultrasound patterns (right heart dilatation, cirrhosis, etc.). Multiple fluid locations (pleural, pericardial, peritoneal) usually indicate fluid overload, in principle not needing a diagnostic tap, but we have a rather safe procedure for these patients (see below).
The effusion can contain a multitude of echoes, slowly moving in suspension, as if in weightlessness, in rhythm with respiration: the plankton sign is a self-identifying label (see Fig. 15.10 page 135). This cannot be a transudate. We heard that color Doppler can create the same pattern. Hemoperitoneum, peritonitis and, also hemorrhagic ascites yield this plankton sign (Fig. 5.10). The effusion can contain multiple septations, indicating inflammatory effusion – generally, peritonitis (Fig. 5.11). Note that these septations are not visualized with CT.

Traumatic hemoperitoneum. In a longitudinal scan of the left hypochondrium, this mass surrounding the stomach (E) looks like a typical, normal spleen. This quietly invalidates the current practice where a sonographer makes the examination and a radiologist reads it. Any involved user will immediately notice a plankton sign within this mass. The real spleen will be recognized a little backward

Peritonitis. This effusion contains multiple septations (usually never seen on CT). Peritonitis due to pneumococcus
Our large policy of puncture in a critically ill patient, especially for anechoic effusions without a perfectly clear explanation, is allowed thanks to the excellent benefit/risk ratio authorized by using ultrasound (see Chap. 26).
Hemoperitoneum
This simple application allows fast life-saving diagnosis of bleeding in traumatized, pregnant, or other patients. Our fast system makes the unit ready after 7 s (the probe and the contact are meanwhile prepared), and we use some additional seconds to find the bleeding using liberal scanning (we do not use the traditional radiological sites). Free fluid is an extreme emergency, generating a new hierarchy of roles, as we pointed out in 1992 [2]. We see three kinds of echogenicity: anechoic collection, or a plankton sign (Fig. 5.10), or an echoic mass. The plankton sign is immediately suggestive of free blood. The echoic, heterogeneous mass, due to fast clotting may appear as a challenge if traditional approaches, which require an anechoic collection, are used. The clotted effusion can be mingled with the numerous structures of the abdomen content (bowel loops, omentum, and various types of fat) (see Fig. 9.19 page 75). Figure 29.3 page 283 proves that the blood can become echoic in a few seconds. The bat wing sign is the most efficient way to solve this outward issue. In some subtle cases, clotting appears by successive layers, and can give the illusion of bowel loops. This pitfall is usually easily bypassed, however, using intercostal scans, since in many cases of clotted hemoperitoneum, a nondependent fluid phase is detected. A fast puncture, usually done at the intercostal space, confirms the diagnosis.
A providential examination can demonstrate the site of bleeding, showing images of parenchymal rupture at the splenic or hepatic area, or even a swirl dynamic around an aortic aneurism, but this should not generate any delay. This is the time for fast laparotomy.
In the trauma context, ultrasound has long replaced the traditional diagnostic peritoneal lavage [3]. It has been proven that the use of ultrasound allows faster laparotomy of patients with suspected torso trauma [4].
We devote a simple paragraph to this life-saving application, i.e., not longer than in our 1992 edition, to save space for the multiple other life-saving applications to be dealt with in this textbook. Conversely, we are glad to see that our lines written in 1992 have inspired teams who have showed that some fields traditionally covered by sonography technicians could also be performed by managing doctors [5].
Peritonitis
Perforating peritonitis can complicate any critically ill patient. In acute abdominal disorders, physical examination is insufficient in sedated, aging patients. Additionally, plain abdominal radiographs are always hard to obtain and usually generate useless irradiation.
In patients with any acute diagnostic problems, detection of peritoneal effusion is decisive. Minimal effusions are more suspect that substantial ones (the fact of cirrhosis or overfluid therapies). A peritoneal effusion in a patient whose hydric balance is negative is suspect. Detection of pneumoperitoneum makes the diagnosis obvious (see next section).
Echoic effusions or multiple septations suggest peritonitis (Fig. 5.11). Pseudomembranes surrounding the intestinal loops yield echoic layers with apparently thickened walls. Presence of gas within the collection [6] seems a rare observation. Our policy of easy puncture regularly clarifies situations that are complex in complex patients, and surgical decisions are taken before the clinical signs become obvious, giving one precious step in advance to the patient.
Bowel analysis is rich in information (see Chap. 6). Thickened walls and abolished peristalsis are some of the basic anomalies.
Pneumoperitoneum
Ultrasound’s potential to detect pneumoperitoneum is rarely exploited. The literature describes an air barrier with acoustic shadow in the extradigestive situation, visible under the left liver, surrounding the gallbladder, in the Morrison pouch [7]. However, the multiple abdominal gas structures can discourage the operator. More standardized signs should be described.
We took point by point the semiotics of the pneumothorax (see Chap. 18), since the logics are exactly the same [8]. We therefore apply our probe in a sky-earth direction, in a supine patient. The free gas will collect at this nondependent area which is particularly accessible.
Preliminary Normal Signs to Be Described
-
1.
Gut sliding. Gut sliding is a gliding sign, a term we suggest for this dynamic of the visceral layer of the peritoneum that moves during respiration, whereas the parietal layer is motionless (Fig. 5.12).
Fig. 5.12 
Gut sliding. Sandy pattern below the peritoneal line, regular horizontal pattern above. This pattern reminds the seashore sign of lung terminology. Arrow: level of the peritoneal line
-
2.
Splanchnogram. This is a suggested term for these anatomical structures such as the liver or bowel loops (see Figs. 5.2 – 5.10). It can refer to the liver or even to the mesenteric fat, and can be called hepatogram or steatogram, for instance. This pattern clearly indicates that no free air interposition is present between the abdominal wall and the visualized organ. Note: we will not confuse spleen (the subphrenic hematopoietic organ) and splanchnos (any abdominal viscera).
-
3.
Aerogram. This term will refer to all airy structures which yield artifacts. G-lines (G for gut) are a label suggested to all these artifacts arising from the abdomen. They can be described in the same way as the thoracic artifacts. With a perfect analogy, we can describe horizontal repetitions of the peritoneal line like the lung A-lines, like the B-lines, vertical well-defined laser-like long comet-tails, and again like Z-lines, vertical comet-tail artifacts that are ill-defined, gray, and short. A, B, and Z-lines are labels devoted to the lung (see Fig. 19.319.3 page 186). In order to avoid any confusion, the abdominal artifacts will be labeled GA, GB, and GZ-lines. The simple difference is that the peritoneal line replaces the pleural line. There is no rib at the abdomen, so there is no bat sign.

In practice, visualization of conserved peak gut sliding or splanchnogram allow pneumoperitoneum to be discounted, at the bedside.
Signs of Pneumoperitoneum (Fig. 5.13)
Like for pneumothorax, they can be organized into a decision tree.

Decision tree for the diagnosis of pneumoperitoneum
-
1.
Abolition of gut sliding (Fig. 5.14) This sign is observed in most cases of free pneumoperitoneum. Patients with abdominal history (surgical adherences) or with (quasi) absence of diaphragmatic motion can display absent gut sliding. Abolished gut sliding is therefore observed in 8% of patients with absence of pneumoperitoneum proven on CT.
-
2.
Aerogram – i.e., absence of splanchnogram Instead of anatomic patterns, only artifacts are visible from the peritoneal line. This sign is always present at the location of the pneumoperitoneum. It is also an usual finding in a meteorized patient – requiring more subtle signs. A splanchnogram is of precious help to rule out pneumoperitoneum in the cases where gut sliding is abolished.
-
3.
Absence of GB-lines In none of our observations of pneumoperitoneum were GB-lines visible. GA-lines (or GZ-lines, which have the same meaning) are exclusively observed, making a sensitive sign of pneumoperitoneum. The principle of the A-line sign is detailed in Chap. 18.
-
4.
The gut point This sign is an exact equivalent of the lung point, dealt with in Chap. 18. It has a 50% sensitivity and is a specific sign.
-
5.
Other signs Countless additional signs could be described. Postural change-induced signs may be used, but we do not like to turn these fragile, shocked patients. In addition, the fewer the number of signs, the simpler the use of ultrasound.

Pneumoperitoneum. Left (real-time): massive air barrier with horizontal repetition artifact (“A-like line,” arrow). Right (time-motion): this mode objectifies the complete absence of gut sliding
Previsible Pitfalls
Gut sliding can be more or less ample. A patient with peritonitis may have diminished gut sliding, partly explained by antalgic hypopnea.
A distended stomach will come against the anterior wall, making gut sliding hard to detect and able to generate GA lines. Consequently, analysis of gut sliding will contribute more if the stomach was previously localized in one way or another.
Very incipiens pneumoperitoneum with only some bubbles visible on CT should theoretically provide difficulties using ultrasound, but we wait for our first case to conclude.
Advantage of Ultrasound
In acute abdominal disorders, ultrasound was able to replace during decades the traditional radiograph showing cupolas or the positional radiographs, which was delicate to perform in tired, shocked, or ventilated patients. Many patients died from delay in diagnosis. Now, ultrasound must face CT. It will simply be able to avoid the drawbacks of CT (see Chap. 19).
Interventional Ultrasound
When dealing with peritoneal effusion, we practice ultrasound-assisted puncture at the slightest doubt. Free of complications when done properly, it has an excellent risk to benefit ratio. This is especially true in the critically ill patient with complex clinical presentation. We find this attitude paradoxically safer than the risky attitude of inferring the type of effusion from its echostructure. In our routine, basic diagnoses are regularly made, in spite of misleading clinical presentations.
We almost always use a 21-gauge green needle. Ultrasound has the major advantage to allow the puncture far from the traditional landmarks. A tap in the right iliac fossa, classically forbidden, is for us very commonplace: ultrasound shows that a fluid collection is interposed before the caecum. Ultrasound even makes it possible to puncture near to the forbidden area of the epigastric vessels, since they can be clearly identified (Fig. 5.15). Puncturing peritoneal effusions using intercostal route is routine in our current practice.

The epigastric vessels. Transverse paraumbilical scan with Carmen maneuver easily showing these two tubular parietal structures (arrows). Note the peritoneal effusion deeper
The procedure is simple: one almost always performs the tap just after ultrasound location (see Chap. 26).
We have exceptionally noticed difficult attempts for very localized effusions in the right iliac fossa, or pelvis of elderly patients. One hypothesis is a loose parietal layer which is driven back by the slow needle, without piercing it. In this case, persisting in inserting the needle to the end could result in piercing remote structures (bowel loops, iliac vessels, etc.). Ultrasound guidance is required but, even here, some procedures remain delicate.
References
Ferrucci JT, Vansonnenberg E (1981) Intra-abdominal abscess. JAMA 246:2728–2733
Lichtenstein D (1992) General ultrasound in the critically ill, 1st edn. Springer, Paris, pp 27–28
Rose JS, Levitt MA, Porter J et al (2001) Does the presence of ultrasound really affect computed tomographic scan use? A prospective randomized trial of ultrasound in trauma. J Trauma 51:545–550
Melniker LA, Leibner E, McKenney MG, Lopez P, Briggs WM, Mancuso CA (2006) Randomized controlled clinical trial of point-of-care, limited ultrasonography for trauma in the emergency department: the first sonography outcomes assessment program trial. Ann Emerg Med 48:227–235
Rozycki GS, Ochsner MG, Feliciano DV, Thomas B, Boulanger BR, Davis FE, Falcone RE, Schmidt JA (1998) Early detection of hemoperitoneum by ultrasound examination of the right upper quadrant: a multicenter study. J Trauma 45(5):878–83
Taboury J (1989) Echographie abdominale. Masson, Paris, pp 246–249
Gombergh R (1985) Atlas illustré des indications classiques et nouvelles de l’échographie. Polaroïd, Paris
Lichtenstein D, Mezière G, Courret JP (2002) Le glissement péritonéal, un signe échographique de pneumopéritoine. Réanimation 11(Suppl 3):165
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
Copyright information
© 2010 Springer-Verlag Berlin Heidelberg
About this chapter
Cite this chapter
Lichtenstein, D.A. (2010). Peritoneum. In: Whole Body Ultrasonography in the Critically Ill. Springer, Berlin, Heidelberg. https://doi.org/10.1007/978-3-642-05328-3_5
Download citation
DOI: https://doi.org/10.1007/978-3-642-05328-3_5
Published:
Publisher Name: Springer, Berlin, Heidelberg
Print ISBN: 978-3-642-05327-6
Online ISBN: 978-3-642-05328-3
eBook Packages: MedicineMedicine (R0)