
Abstract
A brief introduction is given about the diagnostic role of angiography, which, at present, is significantly reduced compared to the other noninvasive techniques such as color Doppler ultrasound, multidetector CT angiography, and magnetic resonance angiography. Then, there is a focus on technical aspects in diagnostic angiography, discussing materials and imaging parameters; subsequently, the technical aspects of interventional vascular procedures are considered. Anatomy is then reviewed as is apparent on angiographic studies.
The rest of the chapter describes angiographical appearance and interventional management of the pathologies of the kidney amenable of an endovascular approach, starting with occlusive vascular disease due to atherosclerosis, fibromuscular dysplasia, or other causes. Then, less common vascular conditions are discussed, such as renal ischemia, aneurysms, A-V fistulas, trauma, and complications of transplant surgery. Final part of the chapter concentrates on renal neoplasm, both benign and malignant, with special emphasis on the endovascular management by means of the different techniques of embolization.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others



Keywords
These keywords were added by machine and not by the authors. This process is experimental and the keywords may be updated as the learning algorithm improves.
1 Introduction
For imaging of renal pathology, a broad spectrum of radiologic diagnostic procedures is available, competing among each other, in their diagnostic performance and relevance. Nowadays, in the work-up of neoplastic lesions, ultrasound (US), computed tomography (CT), or magnetic resonance imaging (MRI) is performed predominantly, while on the other hand, the contribution of diagnostic angiography is no longer required. Digital subtraction angiography (DSA) maintains a limited role, especially in the evaluation of renal arteries, and until recently, catheter-based DSA has been considered as gold standard. However, noninvasive techniques such as CT-angiography (CTA) and MR-angiography (MRA) are evolving parallel to their quantum leap of resolutions and readiness to use. Nevertheless, shared consensus for quality assessment of these new modalities is still lacking; more comparison studies are urgently warranted. US color Doppler is a cheap and readily available technology, but it requires great experience and training for effectively assessing renal vessels, and even in that case, a substantial percentage of patients are not properly examinable. CTA is an extremely promising technique, but still has to prove itself, because its intrinsic spatial resolution could not be sufficient in pathologies like vasculitides, or in some cases, in fibromuscular dysplasia (FMD). With regard to MRI, despite the availability of ultrashort pulse sequences applying the T1 relaxation reduction effect of gadolinium-enhanced MR techniques, overestimation of renal artery stenosis still poses a substantial problem. There is also need to address that, in the past few years, nephrogenic systemic fibrosis has been recognized as a clinical entity related to the administration of gadolinium chelates to patients with renal failure. Therefore, the use of gadolinium-based contrast is under a growing concern, and it is no more considered as a harmless alternative to iodinated contrast as it has been in the past. Nevertheless, a recent study has suggested the possibility to use a lower dose of gadobenate dimeglumine to achieve signal intensity enhancement similar to that achieved with a double dose of a conventional gadolinium-based contrast agent, with excellent specificity (Soulez et al. 2008).
On the contrary, the field of renal intervention is growing, as is implied by a variety of procedures such as percutaneous transluminal angioplasty (PTA), stent placement, and embolization of both trauma and benign or malignant tumors. These methods have emerged over the last two decades, starting from an experimental setting up to a fully accepted treatment option. When renal artery angioplasty is embedded in an aggressive approach including stenting as an adjunct for more complex cases (like renal ostial lesions) and a well-organized follow-up regimen is scheduled, the therapeutic potential of organ preservation appears promisingly high. Providing an adequate perinterventional drug regimen, restenosis rates may be as low as 10%.
Endovascular interventions also include, in selected cases, capillary embolization that might be used as an alternative to nephrectomy with a similar clinical outcome. Specifically, the development of superselective small caliber embolization catheters in synergy with further refinement of embolization materials has aided to realize superselective occlusion techniques in benign vascular lesions and renal trauma.
2 Technique
2.1 Diagnostic Angiography
Angiography in the evaluation of kidney must be done by an intra-arterial approach generally using the femoral route; brachial or radial approaches are also feasible (Scheinert et al. 2001). The former is frequently used by cardiologists, performing peripheral interventions as a primary choice. However, brachial or radial approaches are the only options in cases of bilateral iliac occlusion or infrarenal aortic occlusion. It is also the most favorable in cases of extremely tortuous iliac axes or in patients with femoral surgical grafts.
The technique has been explained in the following: after the infiltration of the skin and subcutaneous tissue with a small amount of local anesthetic, a 19-gauge hollow core needle (single wall puncture needle is preferable) is inserted through the femoral (or brachial or radial) artery, and after the advancement of a short 0.035” guide wire, a 4 or 5 French (Fr) sheath is introduced. In case of femoral approach and the lack of significant stenosis or tortuosity, a standard 0.035” teflon-coated metallic guide wire can be advanced in the abdominal aorta. While in the presence of iliac axes with multiple atheromatous or calcific plaques, a 0.035” hydrophilic-coated guide wire is preferred to the standard guide wire. Sometimes, a selective diagnostic catheter (with a Cobra or multipurpose configuration) is used in association with a guide wire in order to increase the support and obtain a more easy advancement in the iliac artery.
Once reached the abdominal aorta, a 4 or 5 Fr high-flow catheter with a pig-tail or straight tip configuration is advanced over the guide wire. The tip of the catheter is positioned at the level of L1 body. After a preliminary test hand injection, which confirms the intraluminal position of the catheter, a connection to a power injector pump is established. Generally, when angiography is performed with injection from the catheter positioned in the aortic lumen, a total amount of 25–30 mL at 15–20 mL/s of iodinated nonionic contrast media are used. We prefer high concentration contrast media (320–370 mgI/mL), which may be prewarmed before injection in order to reduce the viscosity, and therefore, resistance. For selective angiography, a wide variety of catheters can be used, but the basic ones used to gain access to the renal artery are curved catheters such as the “Cobra 2” or the “Renal Double curve” or the “Simmons 1” or the “Simmons 2.” The flow rate for selective injection must be reduced to 6–8 mL at 3/4 mL/s (Figs. 7.1 and 7.2).

(a) Catheter tip (arrow) seems correctly positioned, but renal artery opacification is faint for the prevalent opacification of celiac trunk and superior mesenteric artery, which overlays right renal artery. (b) Selective renal angiography, a stenosis is present (arrow), as well as a postenotic dilatation (dashed arrow). (c) Renal arteries, correct visualization with a 20° LAO projection, a stenosis of the proximal left renal artery is evident (arrow)

(a) Selective renal angiography: an unstable catheter for shape and position can become dislodged (arrow) for the high flow during power injection. (b) If the catheter is positioned too distal in the main renal artery, the first part of the lumen is not visualized, an ostial stenosis could, therefore, go unnoticed
For acceptable diagnostic results, the equipment must be of high quality with x-ray tube and generator able to give good results in terms of spatial and contrast resolution also in large patients. Modern DSA systems are based on digital fluoroscopy/ fluorography systems and are equipped with special software and display facilities. The mask and the serial images are obtained from the television camera in analog form or from the charge-coupled device (CCD) television camera in digital form. Using a conventional TV camera with the image intensifier will require that the images are digitized in an analog-to-digital converter, which converts the TV line image (525/625 or 1,023/1,249 lines) to an image matrix, commonly with 512 × 512, 1,024 × 1,024, or 2,048 × 2,048 pixels. From a CCD camera, the images are digitized already in the electronics close to the light-sensitive CCD chip.
The last evolution of digital angiography systems is the introduction of flat-panel technology. This allows direct digital imaging without the intermediate step of analog-to-digital conversion with significant improvement of efficiency of the system. The dominating method is based on an indirect X-ray conversion process, using cesium iodide scintillators. It offers considerable advantages in radiography, angiography, and fluoroscopy. The other method employs a direct converter such as selenium, which is particularly suitable for mammography. Both flat detector technologies are based on amorphous silicon active pixel matrices. Flat detectors facilitate the clinical workflow in radiographic rooms, with improved image quality, and provide the potential to reduce dose. This added value is based on their large dynamic range, their high sensitivity to X-rays, and the instant availability of the image. Advanced image processing is instrumental in these improvements and expand the range of conventional diagnostic methods. In angiography and fluoroscopy, the transition from image intensifiers to flat detectors is facilitated by ample advantages they offer, such as distortion-free images, excellent coarse contrast, large dynamic range, and high X-ray sensitivity. Furthermore, another major advantage of flat-panel technology is that, although the tube is essentially unchanged, the image intensifier is eliminated. The image-receiving component of the unit, the flat panel itself, is smaller and more compact, allowing easier access to the patient during interventional procedures.
Another important facility in DSA systems is postprocessing of images. The radiologist can use many processing options such as windowing, filtering, and quantitative measurements of distance and density. Sometimes, the anatomical structures move after the mask has been acquired, and for perfect subtraction, the mask has to be moved a few pixels or perhaps just a fraction of a pixel (pixel shift). Such functions are available in most DSA systems. The frame rate of acquisition must be quite high (at least 3 frames/s) in the first 3–5 s (arterial phase), then it can be decreased at 2 frames/s (parenchymal phase). In cases of prolonged acquisitions, when also a venous phase is acquired, the frame rate can be further reduced to 1 frame/s. Generally, when the diagnostic problem is focused on the arterial bed, only arterial and parenchymal phases are performed.
Concerning the position of the tip of the catheter, it should not be placed too cranial in order to avoid the filling of the celiac trunk and the superior mesenteric artery with contrast media, and therefore, cause problems of overmatching of these arteries on the renal arteries (Fig. 7.1).
Considering the correct projections, it must be underlined that it is crucial to visualize the ostium of renal arteries, since it is the most frequent site of atheromatous lesions; their detection depends not only on their position, but also on the size of the aorta, which once filled with contrast media can hide the origin of the renal arteries. In the second half of the nineties, some papers were published on the contribution of CT elucidating this topic, based on the fact that CT is very effective in a precise evaluation of the position of the renal artery origin and their relationship with the aorta (Verschuyl et al. 1997a, b). These papers have shown that left renal artery can be well depicted in the antero-posterior view because in 80% of cases its origin is between 90 and 120° in respect to aorta axes, but it is useful to add a left anterior oblique (LAO) projection of 20°. Right renal artery shows a variable degree of origin and in 85% of cases it is between −85 and −45°. For this side, the projection that better shows the right renal ostium is always the LAO at 20°, but sometimes a LAO at 40° is useful. In Verschujl et al.’s experience (Verschuyl et al. 1997b), the routine use of AP and LAO projections at 20 and 40° gave a correct evaluation of 92% of 400 renal arteries considered. In detail, the first projection to be done is the LAO at 20°, and if this one is not sufficient, the AP projection can be performed followed by the LAO at 40° in selected cases. Other authors suggest to do only a LAO at 15° (Harrington et al. 1983).
Another alternative solution for renal artery evaluation is to proceed at selective angiography: this modality has the advantage to better define the distal branches of the main trunk; however, often it is unable to correctly evaluate the ostium because the tip of the catheter is placed distally with respect to the ostium Fig. 7.2).
It must be underlined that this type of maneuver is not totally risk-free, particularly in the case of atheromatous stenosis of the ostium for the risk of colesterinic embolization (Morita et al. 1989).
Another problematic issue is the detection of accessory or polar renal arteries, which are not an unusual event due to an incidence of 32% in the monolateral form and 12% in the bilateral form and may represent a cause of clinical problems and also technical problems (Verschuyl et al. 1997a). In some cases these accessory arteries may originate on the same plane of the main trunk, and for this reason, reduce the detection of this vessel (Fig. 7.3). In these cases, oblique cranio-caudal or caudo-cranial projections are useful to distinguish overlapping vessels or proceed to selective catheterization (Fig. 7.3b).

(a) In the AP projection the origin of the two accessory renal arteries (arrow) is on the same plane, main trunk is more cranial (dashed arrow). (b) After cranio-caudal projection, the origins of the two accessory renal arteries (arrows) are better defined
3 Interventional Renal Vascular Procedures
3.1 Vascular Interventions
Since its introduction in 1978, percutaneous transluminal renal angioplasty (PTRA) has emerged as a highly effective technique for the correction of renal artery stenoses. Renal angioplasty has notable physiologic, psychological, and economic advantages over other treatment modalities, and it should now be considered the therapy of choice for renovascular hypertension.
The indications of renal angioplasty are still evolving. The common indications are as follows (Kidney and Deutsch 1996):
-
Sudden onset of hypertension.
-
Hypertension in a patient without a positive family history.
-
Hypertension in a patient without a medical history of factors known to cause hypertension.
-
Malignant hypertension.
-
Hypertension refractory to pharmacotherapy.
-
Patient noncompliance with medications.
-
Hypertension in a patient with abdominal bruit suggestive of renal artery narrowing.
-
Hypertension in a patient who develops renal failure while taking captopril.
-
Sudden onset of hypertension in a young woman not taking oral contraceptives (for patients in this group, the likelihood of FMD is increased).
From a technical point of view, different modalities to perform endovascular treatment of renal artery stenosis are available as follows:
-
Simple balloon transluminal renal angioplasty, with selective stenting in case of suboptimal result at PTA.
-
Primary renal artery stenting.
-
Renal artery stenting with distal protection device.
Regarding evolution of material employed in this type of intervention, the “trend” is to use materials derived from coronary intervention experience, and significant improvements have been introduced for diagnostic catheters, guidewires, PTA catheters, and stents.
Diagnostic catheters: in the past, 4 or 5 French preshaped diagnostic catheters (Cobra, Renal Double Curve, Simmons, etc.) were used to catheterize a stenotic renal artery, and in association with hydrophilic guide wires, the stenosis was negotiated (Fig. 7.4a). Frequently, catheters were advanced beyond the stenosis and hydrophilic guidewires were changed with stiff Teflon-coated stainless steel wires (such as 0.035”Rosen Heavy Duty), and standard profile PTA balloon catheters and premounted stent were advanced over this wire. In the last years, many centers have adopted the use of guiding catheters specifically designed for renal interventions. These guiding catheters, derived from coronary intervention experience, are larger in caliber (6–8 Fr) and have a large lumen. Usually they give a superior support compared to conventional diagnostic catheters and are advanced close to the ostium of the renal artery. At this point, the stenosis is negotiated with a 0.014” or 0.018” guidewire avoiding fragmentation of the atheromatous plaque. Then low-profile balloon catheter or premounted stent are advanced (Fig. 7.4b). This technique has been also defined “Do not touch technique” because it avoids, as much as possible, passages of materials and devices at the level of the atheromatous plaque.

(a) Selective renal angiography with a 5 French diagnostic catheter, a stenotic plaque (arrow) is present at the ostium. (b) Same patient, but angiography is now performed through the guiding catheter (arrow), during stent placement (dashed arrow). The advantage of guiding catheter is that it enables to check every moment of the different steps of the procedure
Guide wires: while negotiation of renal stenosis was done with 0.035” guide wire in the past, several cath lab adopt the rule to negotiate stenosis with 0.014” or 0.018” guidewires in the last years, in order to decrease trauma to arterial plaques, and therefore, reduce distal embolization. Both stainless steel and nitinol guide wires are used, generally with a short soft tip, and still able to give a support to the advancement of low-profile PTA balloon catheters or stents.
Balloon catheters: for many years, standard balloon catheters were employed for dilatation of renal artery stenosis. These catheters have the following characteristics:
-
Shaft corresponding to a 5 F catheter.
-
“Over the wire” construction: this means that the entire catheter runs on the guide wire.
-
Short tip (shorter then 5 mm): this can be useful in the case of distal stenosis near the proximal division of the main trunk.
-
Balloon can be noncompliant or with low-compliance structure: in the first case, once reached the nominal pressure of the balloon (i.e., 8 atm), further increment of pressure will not lead to further increase in the diameter of the balloon. In the second case, once reached the nominal pressure of the balloon, further increment of pressure will cause further smooth increase in the nominal diameter of the balloon till 10% of the nominal diameter. The choice of the type of balloon is operator-dependent and well-defined guidelines do not exist.
In the last years, many centers have adopted the use of low-profile PTA balloon catheters derived from coronary interventions. These differ significantly from standard PTA catheters for the following reasons:
-
Very low-profile tip: the tip has a diameter of 2.6 F (0.66 mm) or lower compared to 1.65 mm of standard PTA balloon, and for this reason, an atraumatic advancement of the catheter through the stenosis is warranted.
-
Generally, this catheter is provided of a hydrophilic coating on the surface of the balloon and on the distal part of the shaft, which enables advancement.
-
Monorail or rapid exchange construction: this term defines a particular way of construction of the catheter for which only the last 30–40 cm of the catheters run over the wire. This gives the significant advantage to the following:
-
Avoid changes of guidewires.
-
Avoid the use of long guidewires.
-
Reduces procedural times.
-
Stents: also in the field of stent, significant evolutions have been introduced moving from balloon expandable stent to be crimped over standard PTA balloon catheter to premounted balloon expandable stent on standard PTA catheter to the very last generation of low-profile premounted stent over rapid exchange or monorail balloon catheter. This last type of material as microguidewires and low-profile balloon catheters reduce the risk of traumatism to the atheromatous plaques responsible for distal embolization. Although in the past some authors treated renal artery stenosis with self-expandable stent (Raynaud et al. 1994), there is a general agreement that balloon expandable stents are much more preferable because their deployment is more precise and these stents have superior radial force. Until few years ago, only stainless steel stents were available, while in the recent years new materials such as chromo-cobalt alloy has been introduced. This alloy has similar strength of stainless steel, but inferior weight and superior long-term results are expected, even if not proven currently. Few data are available on the use of drug-eluting stents in the treatment of renal artery stenosis. One recent multicenter trial in which a Sirolimus-eluting stent was compared to a bare-metal stent shows that the angiographic outcome at 6 months did not reveal any significant difference between the two stents. Renal artery stenting with both stents significantly improved blood pressure. The paper concludes that only further studies with larger patient population and longer angiographic follow-up will be able to determine if there is a significant benefit of drug-eluting stents in treating ostial renal artery stenosis (Zahringer et al. 2007). Stents are mounted over no-compliant or low-compliant balloon catheters. In the first case, manufacturers offer stents with intermediate diameters such as 4.5, 5.5, 6.5 mm. While in the case of stents premounted on low-compliant balloon, no intermediate measures are available due to the possibility of overdilatation of these types of balloons. Generally, the length of the stents are 10, 12, 15, 18 until 24 mm. In addition, stents with a “flaring effect” are also available. This option allows the possibility to oversize the proximal diameter of the stent at the level of the ostium.
Postprocedural imaging has been used for follow up and, to assess the effectiveness of percutaneous revascularization, clinical criteria, and laboratory findings together. Serial Doppler ultrasound (US) is a ready available technique and able to diagnose residual stenosis or restenosis (Akan et al. 2003). Anyway, Doppler US is known to be challenging; even for the evaluation of native RAs owing to patient-related factors, its diagnostic performance in patients with implanted stents is additionally hampered by metal-induced waveform distortion (Sharafuddin et al. 2001; Parenti et al. 2008; Rocha-Singh et al. 2008). Magnetic resonance angiography after stent placement is limited by the ferromagnetic artifacts caused by most stents (Tello et al. 1998). More recently, technical advances with multidector CT have pointed out with prospective studies (Steinwender et al. 2009) how CT angiography can provide excellent noninvasive technique to detect and evaluate intra-stent restenosis, in comparison with invasive DSA.
Distal embolic protection devices: this device was firstly designed for carotid endovascular interventions as carotid artery stenting. It is a sort of microguidewire which mounts on the distal part a conic shaped filter made of a membranous material as polyurethane or nylon or a windsock-like nitinol basket, 2–3 cm distal to a floppy tip (Fig. 7.5). Distal protection devices work by interrupting or filtering blood flow in the internal carotid artery. Its use in renal interventions is still under investigation. Some centers have evaluated this tool on significant number of cases (Henry et al. 2003). The most important characteristics are the ability to cross stenotic lesions and the “capture capability.” Generally, they are able to entrap embolic debris from medium to large size, generally particles more than 100 µm in long diameter. The aim of distal filter is to reduce embolization during the different phases of the maneuver. Some limitations in this filter exist due to the fact that they are not specifically designed for renal arteries, but for carotid arteries. The main limitation is that the “landing zone” of the filter may end distally to the main division of the main renal trunk and so only part of the kidney parenchyma is protected by the risk of debris embolization.

(a) 3D MIP CT-angio shows a high-grade short stenosis of the proximal right renal artery (arrow). (b) Preprocedural selective angiography confirms the lesion. (c) Postprocedural, a stent (arrow) has been placed and normal caliber has been restored. Note the embolic protection device in the distal segment of the main trunk (dashed arrow)
3.2 Other Endovascular Interventions
Arterial embolization: renal conditions eligible to be occluded by means of an embolization procedure of a renal artery consist mainly of kidney tumors (both benign as angiomyolipomas (AML) or malignant as advanced renal cell carcinomas), the other common setting of embolic therapy is renal trauma.
From a technical point of view, this procedure needs confidence with the use of embolic materials such as:
-
Coils: these are mechanical devices with a helical shape variable in diameter and length. Frequently, nylon filaments are added on their surface. Coils can be pushable or detachable: the first ones, once released from the catheter cannot be retrieved, while the detachable coils, if the final position is not correct, can be reintroduced in the catheter and changed with another coil. A recent evolution of coils are the so called “vascular plugs.” They are mechanical devices made of nitinol mesh with different shapes, self-expandable and able to achieve rapid occlusion of the target vessel. Once released in the vessel, if the deployment is not correct, the device can be recaptured and repositioned. When the plug is in the right position, it can be easily detached. Compared with the coils, it has the significant advantage that occlusion of the target vessel is obtained with a single device instead of several coils.
-
Particulate agents: most of them are based on polyvinyl alcohol (PVA) particles of different size from 50 to 1,200 µm. Usually, embolization with PVA particles causes a permanent occlusion of vessels of the size of the particles used. Recent evolution consists in new types of microspheres consisting of a biocompatible, acrylamido PVA macromer, which shows deformable capability, lower tendency to aggregate inside the catheter during injection with lower body reactions. An alternative are gelatine or fibrine sponge. These materials are manually reduced to small fragments by operator and then mixed with contrast media and slowly injected under fluoroscopic control. They are quite easy to use, but the main limitation is that the effect of this type of embolization is limited to a short period, and after 10–20 days, many of the vessels may be reopened.
-
Liquid embolic agents: N-butyl-cyanoacrylate (NBCA) was the first liquid embolic agent applied in the clinical practice. It is a monomer acrylic glue which rapidly polymerizes when in contact with ionic media such as blood and causes a permanent occlusion. To avoid adherence to the tissue of the thin catheters required for the superselective embolization, NBCA has to be injected through a catheter washed with a 5% dextrose solution and the catheter has to be withdrawn promptly after injection. The technique requires considerable expertise; there is also the risk of undesired embolizations. Moreover, NBCA polymerizes with an exothermic reaction, causing pain to the patient. Its use was mainly diffused in neuroradiologic embolization procedures, but in the last years, this product was abandoned also because it does not have the regular mark approval for an endovascular use (CE Mark). Glubran 2 is an acrylic glue bearing a CE mark authorized for surgical and endovascular use in neuroradiology and interventional radiology. The comonomer of Glubran 2 comprises a monomer of NBCA and a monomer of Metacryloxysulpholane (MS) (owned by GEM Srl). MS allows the monomer of NBCA to polymerize with a lower exothermic reaction (45°C) and a slightly longer polymerization time (Leonardi et al. 2002). Compared to the monomer NBCA, the Glubran 2 causes less pain to the patient and is associated with a lower risk of adherence of the catheter to the tissue, hence showing a greater ease of use. Differently, acrylic glues, once deposited into the nidus, determine its permanent occlusion and prevent its replenishment through feeding branches.
3.3 Renal Phlebography
From the diagnostic point, the only role left for renal phlebography is the sampling of the blood from the renal veins in patient with renal hypertension to clarify which kidney is responsible for an increased production of the hormone renin. In these cases no particular imaging documentation of veins is required, unless anatomic significant variants are found. It is, however, important to obtain blood samples from each renal vein and from the inferior vena cava above and below the renal veins. Samples need not be simultaneous; however, it is better if they are closely spaced temporally. Renin levels from one kidney, which are >1.5 times of the contralateral kidney, are indicative of renovascular hypertension. An increased renin value in the suprarenal inferior vena cava compared to the infrarenal vena cava is also suggestive of renovascular hypertension.
4 Anatomy and Variants
4.1 Arteries
In the majority of patients, main renal arteries originate between the upper margin of L1 and the lower margin of L2 vertebrae and frequently the origin of the right renal artery is higher than left renal artery. The ostium of both renal arteries is located laterally; however, the ostium of the right renal artery tends to be located on the ventral aspect of the abdominal aorta, and as previously said and well shown on CT studies (Verschuyl et al. 1997a), there is a significant variation in its position.
The ostium of the left renal artery more frequently originates on the lateral aspect of the abdominal aorta; however, in a significant number of cases, it tends to be located on the dorsal wall of the aorta. The right renal artery in the first 1–2 cm has an anterior course and then turns posteriorly with a cranio-caudal obliquity. The left renal artery has a more linear and horizontal course. The caliber of the artery in the proximal part generally is 6 mm. The main renal artery divides into segmental arteries near the renal hilum (Kadir and Brothers 1991). The first division is typically the posterior branch, which arises just before the renal hilum and passes posterior to the renal pelvis to supply a large portion of the blood flow to the posterior portion of the kidney. The main renal artery then continues before dividing into four anterior branches at the renal hilum: the apical, upper, middle, and lower anterior segmental arteries. The apical and lower anterior segmental arteries supply the anterior and posterior surfaces of the upper and lower renal poles, respectively; the upper and middle segmental arteries supply the remainder of the anterior surface. The segmental arteries then course through the renal sinus and branch into the lobar arteries. Further divisions include the interlobar, arcuate, and interlobular arteries (Fig. 7.6).

Schematic anatomy of the renal arteries and branching. 1 main trunk, 2 adrenal artery, 3 gonadal artery, 4 segmentary artery, 5 lobar artery, 6 arcuate artery
Renal artery variations are divided into two groups: early division and extrarenal arteries. Branching of the main renal arteries into segmental branches more proximally than the renal hilus level is defined early division (Fig. 7.7), while with the term of “extrarenal artery” two groups are defined: hilar (accessory) and polar (aberrant) arteries. Hilar arteries enter kidneys from the hilus with the main renal artery, whereas polar arteries enter kidneys directly from the capsule outside the hilus. The origin of these extra renal arteries is quite variable and majority of them arise from the abdominal aorta over or below the main trunk. Infrequently, they may arise from the common iliac arteries. Renal artery origins arising above the superior mesenteric artery are extremely rare. Congenital anomalies of renal position and conformation are often associated with aberrant location of renal artery origins and supernumerary vessels. In particular, horseshoe kidney has a 100% incidence of multiple renal arteries (Fig. 7.8). The renal pelvis and proximal ureters are supplied by small branches of the interlobular, arcuate, and distal main renal arteries. The middle portion of the ureters is supplied by the gonadal arteries (Fig. 7.6). The distal ureters are supplied by terminal branches of the internal iliac arteries, most notably the cystic artery.

(a) CT-angio shows an early division (arrow) from the main renal trunk, with an eccentric stenosis of the superior artery. (b) Same patient, selective angiography confirms the finding. (c) Angiography poststent deployment

(a) CT-angio shows a horseshoe kidney in a patient with an abdominal aortic aneurysm involving both iliac arteries. Note the two polar arteries, the first (arrow) arising from the abdominal aorta and supplying the right inferior renal pole, and the second (dashed arrow) arising from the proximal tract of the right common iliac artery and supplying the left lower renal pole. (b) Diagnostic aortography failed to show the polar arteries, only the second (dashed arrow) is barely visible. (c) The first polar artery is later shown after selective catheterism

Shows RAS cascade. Critical stenosis at the main renal artery reduces flow and pressure distal to it. Kidney releases renin (not shown) that converts angiotensinogen to angiotensin-I (AT-I), then metabolized into the lungs to angiotensin-II, the effect is constricting arterioles and rising the aldosterone level. The final outcome is rise in systemic blood pressure
In several anatomic and angiographic studies, it was stated that the rate of bilateral extrarenal arteries is to be 10–15% (Kadir and Brothers 1991; Talovic et al. 2004), that the rate of early division in the general population is 15%, that aberrant renal arteries are observed twice as often as accessory renal arteries and the frequency rate of extrarenal arteries is the same on the right and left sides, and that in 12% of the general population extrarenal arteries are bilateral. In a recent series (Ozkan et al. 2006), the frequency rate of early division and bilateral extrarenal arteries was 8 and 5%, respectively, which is low when compared to other major series. In this series, no statistically significant differences were detected between the frequency rates of ERA on the right and left sides, and this finding was compatible with other studies.
The renal arteries are end arteries. In contrast to other districts (i.e., the colonic and hepatic), the intrarenal collateral pathways are poorly developed. In the presence of slowly progressive proximal renal artery stenosis, renal capsular, ureteral, adrenal, and other retroperitoneal arteries may enlarge sufficiently to provide a collateral blood supply to keep kidney perfusion, but with a compromised function. Acute proximal occlusion of a previously normal renal artery results in profound ischemia due to insufficient preexisting collateral supply.
4.2 Veins
The renal cortex is drained sequentially by the arcuate veins and interlobar veins. The lobar veins join to form the main renal vein. The renal vein usually lies anterior to the renal artery at the renal hilum. The left renal vein is almost three times longer than the right renal vein. The left renal vein averages 6–10 cm in length and normally courses anteriorly between the superior mesenteric artery and the aorta before emptying into the medial aspect of the inferior vena cava. The right renal vein averages 2–4 cm in length and joins the lateral aspect of the inferior vena cava. Unlike the right renal vein, the left renal vein receives several tributaries before joining the inferior vena cava. It receives the left adrenal vein superiorly, the left gonadal vein inferiorly, and a lumbar vein posteriorly.
While anatomic variants of the renal veins are commonly visible in CT, their demonstration during renal phlebography is not so obvious and easy. Multiple renal veins constitute the most common venous variant and are seen in approximately 15–30% of patients (Kadir and Brothers 1991). Multiple right renal veins occur in up to 30% of individuals, and sometimes a single vein may divide before joining the inferior vena cava (Beckmann and Abrams 1980).
The most common anomaly of the left renal venous system is the circumaortic renal vein, seen in up to 17% of patients (Kahn 1973; Ferris 1969). In this anomaly, the left renal vein bifurcates into ventral and dorsal limbs that encircle the abdominal aorta. The posterior limb is usually the smaller of the two, although this is certainly variable. There are two common variants of the circumaortic vein: in the most frequent (approximately 75% of cases), one renal vein at the renal hilum subsequently divides before entering the inferior vena cava; in the less common variant, two distinct veins originate from the renal hilum (Beckmann and Abrams 1979, 1980). In the presence of a circumaortic renal vein, the gonadal vein will typically join the retroaortic limb and the adrenal vein will join the preaortic limb (Kadir and Brothers 1991). A less common venous anomaly is the completely retroaortic renal vein, seen in 3% of patients. Here, the single left renal vein courses posterior to the aorta and drains into the lower lumbar portion of the inferior vena cava. Alternatively, the retroaortic renal vein can drain into the iliac vein (Satyapal et al. 1999).
5 Occlusive Disease
The majority of renal occlusive disease (>90%) is due to atherosclerosis and FMD. These pathologies can be present as clinical asymptomatic or with symptoms and signs, consisting of arterial hypertension or renal failure. Less common causes of stenosis of the renal artery are dissection, vasculitis, neurofibromatosis (NF), compression from mass effect (i.e., neoplasia, haematoma), and developmental.
The majority of hypertensive patients (95%) are affected from what is defined as primary hypertension; in other terms, there is no structural abnormality that can be isolated as cause of the condition. In only 1–5% of the hypertensive population, the condition can be attributed to the stenosis of renal arteries, in that case it is then defined as secondary.
The mechanisms of arterial hypertension due to stenotic disease of the renal artery are based on the activation of the renin-angiotensin-aldosterone system (RAAS) (Fig. 7.9).
In the human physiology the most important mechanism to control circulatory volume on the long term is the renal-body fluid feedback system. If the arterial pressure is too high, the kidney excretes increased quantities of sodium and water, and on the other hand, when arterial pressure falls, the kidney reduces the rate of sodium and water excretion until pressure returns to normal levels. This mechanism acts over the period of several days.
The kidneys control pressure through the renin-angiotensin system (RAS). When the arterial pressure falls too low, the kidney releases a small protein (renin) that activates the RAS. This helps to raise arterial pressure in several ways, and by doing so, corrects the initial fall of pressure. Angiotensin-II (AT-II) is the end product of this chain and acts constricting arterioles and veins throughout the body, raising total peripheral resistances and decreasing vascular capacity (Guyton and Hall 2006).
This consideration explains how stenosis of renal arteries causes hypertension. This behavior has been described in the “Two-kidney one clip” hypertension model by Goldblatt (Goldblatt 1934; Glodny and Glodny 2006). In this experiment a constrictor is placed on a renal artery of an animal, thus the reduced blood flow to the kidney induces production of large amounts of renin from the cells of the juxtaglomerular apparatus. During several days, there is a steady increase in blood pressure until arterial pressure rises to a level that allows return to normal renal perfusion. Same happens in clinical renovascular hypertension.
About clinical presentation, there are some signs that are characteristics of renovascular hypertension compared to the primary form. Generally, renovascular hypertension is hard to control with drug therapy; moreover, the onset and the increase in blood pressure are usually sudden, in addition, at physical examination, a high-pitched epigastric bruit can be present. As previously stated, patients are poorly responsive to drug therapy; moreover, if treated with ACE-inhibitors or AT-II blockers, acute renal failure may appear, with consequent rise in serum creatinine.
Further manifestations of renal hypertension are left ventricular dysfunction and renal dysfunction. The first is due to left ventricular hypertrophy as a consequence of myocardial fibrosis and leads to diastolic and later systolic dysfunction with significant morbidity and mortality. The second one, renal dysfunction, may be caused by severe bilateral renal artery stenosis or functional single kidney. An important role may have been the contemporary presence of diabetes mellitus causing nephrosclerosis.
Duplex Doppler ultrasonography is a good screening test in many patients, but it has limitations in larger persons and can overlook small accessory arteries. For patients with normal renal function but a high clinical index of suspicion for renovascular disease, contrast-enhanced magnetic resonance angiography and computed tomographic angiography are the most accurate imaging tests (Hartman and Kawashima 2009) (Table 7.1).
5.1 Atherosclerotic Renal Artery
Most of the patients with a positive imaging for renal artery stenosis are asymptomatic. At angiography, atherosclerotic plaques are usually localized within 1 cm to the ostium, most often consisting of stenosis at the origin, since less than 10% of the stenosis are distal than 1 cm. On that basis, lesions can be classified as ostial stenosis or proximal stenosism, and on the other hand, intrarenal branches are affected on a variable degree. Frequently, plaque formation begins in the aorta wall with progression into the renal artery lumen, inducing the typical appearance of the ostial, usually eccentric location of the atherosclerotic renal artery stenosis.
Epidemiology of atherosclerotic plaques is focused on male rather than female gender, affecting especially individuals older than 60 years. In a large autopsy series, stenosis producing more than >50% of reduction in caliber was found in 18% of those between 65 and 74 years and in 42% of those older than 75 years (Fauci and Harrison 2009). The quantification of a renal stenosis on angiography is based on the degree of luminal narrowing: some authors consider significant a narrowing superior or equal to 50%, while other authors tend to set a 70% degree of stenosis as threshold (Olin et al. 1995) (Fig. 7.10). During angiography, sometimes anterior or posterior plaques may be underestimated or even undetected on AP and oblique views (Cam et al. 2010). Other indirect signs suggesting a stenosis of the renal artery are the poststenotic dilatation (Fig. 7.11), the slow flow distal to the lesion, the presence of collateral circulation, and the reduced size of the renal parenchyma. Sometimes angiography may detect irregularities such as dissections or ulcerations (Fig. 7.12) of the surface of the plaque responsible for the stenosis. Calcifications of the plaque are underestimated in DSA due to automatic subtraction of calcium; however, they can be visualized as linear artifacts at the site of the plaque (Fig. 7.13). A useful sign of the severity for a renal artery stenosis is a systolic pressure gradient >10 mmHg between the aorta and the renal artery distal to the lesion. However, it must be underlined that sometimes a catheter placed through a moderate lesion to measure pressure may further decrease the cross-sectional area of the lumen and then overestimate the gradient (Kaufman 2003).

(a) Typical proximal stenosis of the left renal artery, diameter analysis. (b) Short high-grade stenosis of the right renal artery (selective catheterism)

(a) Vessel ectasia (arrow) after a moderate stenosis. (b) postenotic dilatation (arrow) after a high-grade stenosis (dashed arrow)

(a) Stenosis with dissected appearance of the plaque (arrow). (b) Ulcerated plaque (arrow) in a young boy with fibromuscular dysplasia (FMD)

(a) Calcified plaques are commonly underestimated at angiography, but can often be diagnosed as subtraction artifacts (arrow). (b) Different patient, a calcified plaque is dislocated at margin of the lumen (arrows) after stent deployment
Atherosclerotic renal artery stenosis is a progressive disease, even in initially unaffected arteries with up to 18% occlusion rate over 5 years (Tollefson and Ernst 1991; Schreiber et al. 1984).
In time, a stenosis can progress into renal insufficiency, especially if it is bilateral. As a matter of fact, 10% of all the patients requiring haemodialysis are related to an evolution of a bilateral renal artery stenosis. Restenosis, due to intimal hyperplasia after stenting, develops in a subset of patients and repeat intervention may be required. The incidence of restenosis after angioplasty and stenting using color Doppler has been recently assessed with result that restenosis occurs in a substantial number of patients treated. Preoperative statin medication use and increased preoperative diastolic blood pressure are associated with reduced risk of restenosis (Corriere et al. 2009).
However, no general agreement on the efficacy of endovascular treatment of renal artery stenosis by angioplasty or stenting compared to medical therapy is available. The last largest trial (ASTRAL trial) conducted mainly in United Kingdom and completed in the beginnings of 2008 in which 806 renal failure patients (serum creatinine approximately 2 mg/dL) with atherosclerotic renal artery stenosis were randomized to receive either catheter-based intervention and medical therapy or medical therapy alone failed to show an advantage of endovascular treatment over medical therapy alone. On an average, the percentage of stenosis in the renal artery was 75% and no significant difference in the baseline characteristics between the intervention group and the medical therapy group were observed. The procedure was successful in 88% of patients with a residual renal artery stenosis <50%. At 1 year, there was no difference in the change in serum creatinine between the two groups (serum creatinine increased by 0.2 mg/dL in both groups).
At 1-year follow-up, there was no statistically significant difference in the rates of myocardial infarction, cerebrovascular events, or hospitalization due to angina, heart failure, the need for percutaneous coronary intervention, or bypass surgery between the intervention and medical therapy groups (66% vs. 59%, HR 0.9 (0.66–1.15), p = 0.3). Risk-adjusted mortality was also the same in the two treatment arms (HR 0.92 (0.68–1.26), p = 0.6). The investigators concluded that there is “currently no evidence of benefit from catheter-based revascularisation on renal function in the ARVD patients entered into the ASTRAL study” (The Astral Investigators 2009).
Some observations to these not very encouraging results have been recently reported (Weinberg 2010). The first is the absence of a quantitative angiography which could grade the stenosis. The second observation regards the inclusion criteria and the end point: the study was finalized to evaluate improvement in renal function in patients which underwent renal artery stenting or medical therapy. However many patients had unilateral disease and 41% had a stenosis less than 70%. It has been argued that these are patients whose condition would not be expected to worsen with medical therapy nor to improve with stenting. The third limitation concerns the long period of recruitment started in 2000 and lasted at the end of 2008 and the high number of centers enrolled with a very low number of patients for some centers (two patient/year) with a superior rate of adverse events in comparison to other trials. Furthermore in this “long” period of recruitment significant advances in materials were introduced and many of the procedures were performed without “state of art” materials.
5.1.1 Endovascular Treatment of Atherosclerotic Renal Artery Stenosis
The preliminary experiences at the beginning of the 1990s obtained with conventional balloon angioplasty for the treatment of renal artery stenosis proved to be effective in atherosclerotic stenosis of the main renal trunk and in FMD with procedural success rate of 82–100% and restenosis rate of about 10% (Safian and Textor 2001; Canzanello et al. 1989; Plouin et al. 1998). However, the simple balloon angioplasty of ostial atherosclerotic lesions showed a low beneficial effect due to inferior technical success and higher restenosis rate of up to 47% over the long term and explained with the elastic recoil and rigidity of the lesion and potential dissection (Blum et al. 1997; Van de Ven et al. 1995). The introduction of stenting has revolutionized endovascular renal revascularization and two randomized trials proved the superiority of stenting over conventional balloon angioplasty, particularly in the treatment of atherosclerotic ostial lesions. With the new low-profile premounted stents, the success rate of treatment is obtained in about 100% of cases with restenosis rates ranging from 0 to 23% (Dorros et al. 1998; Zeller 2005; Jokhi et al. 2009). The procedure, however, is not always successful and deterioration of renal function following stenting has been reported (Safian and Textor 2001; Zeller et al. 2003). Main causes are embolism and contrast-induced nephropathy. The first may be reduced by an accurate technique of manipulation of different devices and by cleaning the tip of the guiding catheter from debris collected during the engagement of the renal artery by aspiration of blood through the catheter. The use of distal protection device may be useful; however, as previously mentioned, it is limited by the anatomy of the renal artery.
5.2 Fibromuscular Dysplasia (FMD)
FMD consists of a heterogeneous group of lesions affecting the arterial wall, characterized by nonatherosclerotic intimal, medial, or adventitial thickening (periarterial fibromuscular dysplasia). It accounts for less than 10% of cases of renal artery stenosis, and 90% of the cases involve the media.
As previously stated, FMD, most of the time, consists of medial fibrodysplasia, in this conditions web-like tissue reduces the lumen of the vessel (Kumar 2009). More forms of FMD exist especially in young patients, where the distinction between neurofibromatosis and arteritis is challenging or not possible at all.
Imaging features of FMD on angiography are the typical beaded, aneurismal appearance of the middle to distal main renal artery. This pattern is valid for medial FMD, other angiographical patterns appear for less common entities (Olin 2007).
5.2.1 FMD, Variants, and Appearance on Angiography
-
Medial FMD: string of beads. Most common. The beading is larger than the normal caliber. Localized medial-distal renal artery and its branches. Seventy-five to eighty percent of the total. Some areas of thinning may develop aneurysm in a minority of patients (Fig. 7.14a, b). Infrequently, FMD may affect other districts as carotid arteries or iliac arteries as well (Fig. 7.14c, d).
Fig. 7.14 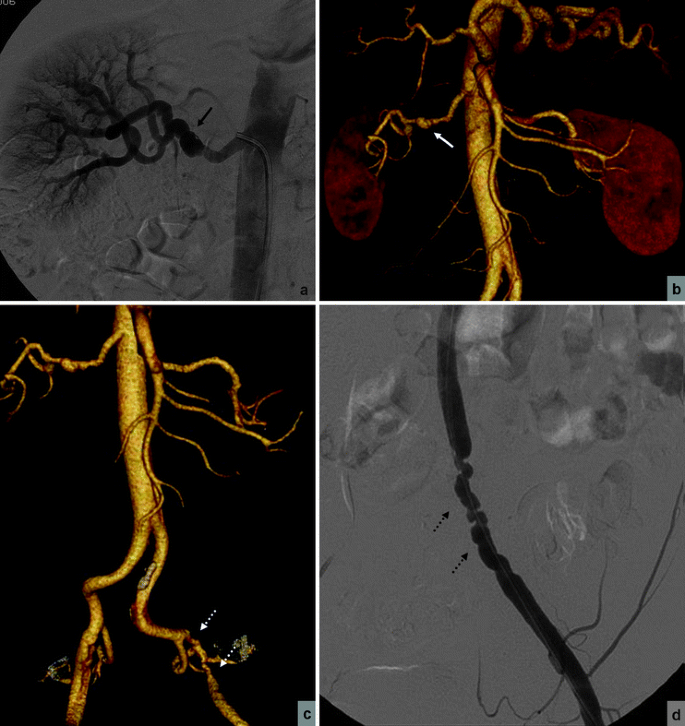
(a) Selective angiography of the right renal artery, classical appearance of the “string of beads” pattern (arrow) in medial fibromuscular dysplasia. (b) CT-angio shows the same finding: proximal tract of the main renal trunk is unaffected. (c) same patient, complete CT-angio shows left iliac artery is affected as well, stenosed with a beaded pattern (dashed arrows). (d) Selective angiography of the left iliac artery (dashed arrows), confirms
-
Perimedial: it occurs in young girls 5–15 years old; fewer beads of smaller diameter; collateral arteries often form around area of stenosis. It accounts for 10%.
-
Medial hyperplasia: it appears as a concentric focal band; it resemble intimal fibroplasia.
-
Intimal FMD: a focal, concentrical stenosis; a long smooth narrowing (that could be confused for Takayasu arteritis or giant cell arteritis) or a focal band-like narrowing. Around 10% of the cases (Fig. 7.15).
Fig. 7.15 
(a) Aortography in a young boy with intimal fibromuscular dysplasia shows a band-like stenosis of the left renal artery (arrow). (b) Treated with angioplasty (arrow), with partial results. (c) Later, for recurrence of hypertension after few months, a stent (arrow) has been placed
-
Adventitial: a perimedial collar of focal stenosis: occasionally multiple, robust collateral network, lesser number of beads than in medial FMD. Rare.


Multidetector CT seems to be a promising technique for imaging of FMD, still some complex case could require the superior spatial resolution of catheter-based angiography for a definitive assessment (Blondin et al. 2009).
The location of FMD is typically in the distal portion of the renal artery (Fig. 7.14), but sometimes extends to the distal branches (Cluzel et al. 1994). In more or less half of the patients, the condition is bilateral. However, the degree of involvement is extremely variable also in the same kidney in the case of multiple arteries (Fig. 7.16).

(a) Selective catheterism, a polar artery (arrow) is affected by a mild form of fibromuscolar dysplasia. (b) The lesion is treated with angioplasty. (c) Same patient, selective catheterism of the main renal trunk delineates the vessel as unremarkable
FMD can rarely produce secondary acute dissections with signs on CT scans such as a hypodense wedge (infarcts), iperdense mass (hemorrhage), and clinically with hematuria and flank pain. Intimal and periarterial fibromuscular dysplasia is more commonly associated with progressive dissection and thrombosis: anyway, macroaneurysms and dissections are complications of FMD and do not represent distinct histopathological changes (Slovut and Olin 2004).
In contrast with atherosclerotic renal artery stenosis, FMD typically affects relatively young patients: close to 30 year-old and is more common in the female sex (girls and women between 15 and 50 years of age) (Safian and Textor 2001).
Contrary to atherosclerotic stenosis, FMD rarely leads to renal artery occlusion, and at the same time, also renal failure secondary from FMD is very rare.
The cause of fibromuscular dysplasya in unknown, even if many theories have been proposed, such as smoking, genetic predisposition, or hormonal factors.
Sometimes it could be difficult to differentiate FMD from vasculitis; anyway, the former is by a noninflammatory process, and therefore by definition, it is not associated with inflammatory acute phase reactants, anemia, or thrombocytopenia.
5.2.2 Endovascular Treatment of FMD
Before the advent of endovascular treatment, surgical revascularization was the primary alternative for patients with refractory hypertension. Technical rate of success was variable from 89 to 97% with hypertension cured in 33–66% of patients; a long-standing hypertension, high-grade atheromasic lesions, or the need for complex branch-vessel repair have lowered the change of success.
Compared to surgery, percutaneous revascularization by angioplasty technique (Fig. 7.16) is less costly, less invasive, associated with a lower morbidity, and could be proposed as an outpatient procedure; moreover, if it fails, the surgical option is still feasible.
Placement of a stent, which is a common procedure for atherosclerotic stenosis, is not advised in FMD and has been reserved for cases with complications with suboptimal results on angioplasty or especially when renal artery dissection or restenosis or persistent hypertension occurs (Fig. 7.15).
The success of angioplasty results in the reduction of blood pressure in few weeks, which represents the reduced excretion of plasma renin: technical success ranges from 85 to 100%, depending on the cases series examined. The rate of restenosis ranges from 7 to 27% over follow-up period of 6 month to 2 years.
After the intervention, there is imaging to assess the technical result of the procedure; moreover, the patients are candidates for yearly follow-up with color Doppler ultrasonography to assess the progression of disease, restenosis, or reduction in kidney volume.
As a final note, even if it lies beyond the aims of this book, we ought to remind that FMD is often a multifocal disease, affecting the extracranial cerebrovascular circulation (carotid or vertebral arteries), in association with the presence of intracranial aneurysm. More rarely, other arterial beds could be affected, such as popliteal, iliac, splanchnic, or coronary.
5.3 Other Causes
These causes are much less common and include compressive lesions on the lumen of the renal artery or other conditions that alter the wall of the vessel. It can be due to extension of an aortic dissection or iatrogenic events such as unintentional ostium coverage by aortic stent-graft or by a vasculitis. Compressions are most commonly caused by a subcapsular hematoma (from a tumor or trauma).
6 Acute Renal Ischemia
Thrombosis of the main renal artery and their branches, especially in the elder population, is a significant cause of reduction in glomerular filtration rate (GFR), and therefore, renal function.
When acute renal occlusion in otherwise normal renal artery presents, infarct of the entire organ is prone to happen within 1 h since the collateral blood supply, mostly from capsular arteries, is unable to provide enough flow. In the setting of a chronic renal artery stenosis, a complete occlusion can result in an incomplete infarct of the kidney, since the gradual development of collaterals can provide some perfusion.
Acute ischemia is secondary due to a number of conditions, from intrinsic pathology of the renal vessels (posttraumatic, atherosclerotic, inflammatory), as a complication of an aortic dissection (Fig. 7.17), or resulting from distant emboli: fat emboli, emboli from the left heart (mural thrombi, bacterial endocarditis), or paradoxical emboli (in the presence of patent foramen ovale or atrial-septal defect).

(a) CT-angio shows aortic dissection (dashed arrow): left kidney is vascularized while right kidney is under perfused (arrow). (b) The dissection flap enters in the right renal artery (arrow). (c) Same patient, aortography confirms the right kidney (arrow) is underperfused. (d) The right renal artery is patent after placement of three sequential stents (arrows)
Short-warm ischemia time means that only a limited amount of cases are amenable of treatment with endovascular therapy or surgical revascularization.
Clinical presentation is variable and linked to the speed of onset: if sudden, symptoms such as flank pain, fever, hematuria, and nausea may be present. More gradual occlusions (i.e., with a renal stenosis already in place) can go undetected.
6.1 Renal Vein Thrombosis
The thrombosis of one or both renal veins has a number of different predisposing conditions, like trauma, extrinsic compression, invasion by renal tumors, pregnancy, oral contraceptives, dehydratation, nephrotic syndrome, etc.
As in arterial occlusion, clinical symptoms are dependent from the onset; if the thrombosis is fast or abrupt, significant pain is expected, while in gradual thrombosis the only symptoms may consist in recurrent pulmonary emboli.
7 Renal Artery Aneurysms
It can be atheromatous or manifestation of fybromuscular dysplasia. Their incidence is quite low, about 0.3–0.7 of autopsies and up to 1% of renal arteriographic procedures (Tham et al. 1983). Most of renal artery aneurysms are localized at the first or second order branches of the renal arteries and have a saccular and noncalcified appearance. Frequently, they are observed in patient with FMD, and for this reason, a female predilection is observed. On the other hand, when secondary to some sort of vasculitis, they are often distributed to the distal, intraparenchimal, branches. Mycotic or traumatic pseudoaneurysms are a differential diagnosis, but could require similar treatment.
Renal artery aneurysms are frequently clinically silent; however, association with hypertension is reported in significant percentage (Canzanello et al. 1989). Hypotheses regarding the causes of hypertension are the contemporary presence of a renal artery stenosis, microembolization from the aneurysm sac, compression or kinking of the renal artery or of its branches, and turbulent flow.
The risk of rupture is very low and decisions regarding management should be based on patient age and gender, severity of hypertension, anticipated pregnancy, and anatomic features of the aneurysm. Although size greater than 2 cm is considered a threshold for surgical treatment, rupture of aneurysms less than 2 cm has been reported (English et al. 2004). Clinical picture during this phase includes flank pain, hematuria, and shock.
The diagnosis of large aneurysms can be done with CT-angio or MR-angio techniques, but small (usually intraparenchimal) aneurysms still require angiography for a confident identification and subsequent characterization.
There are different papers concerning endovascular treatment of renal artery aneurysms and different options are suggested (Klein et al. 1997; Schneidereit et al. 2003). Until few years ago, “coiling” of the aneurysmatic sac with “free” or “detachable” coils (Fig. 7.18), with a typical neuroradiologic fashion, was the only adopted technique and it is particularly useful in the case of aneurysm located on the branch division. In the last years, with the availability of covered stent, this way of treatment was frequently reported and it is preferred when the aneurysm arises in the main trunk (Bruce and Kuan 2002; Liguori et al. 2002) (Fig. 7.19).

(a) Left kidney, selective angiography, the patient underwent a renal biopsy, and few days after, sudden hematuria appeared with decreased hemoglobin level. (b) Selective angiography of a polar artery shows the presence of a pseudoaneurysm (arrow). (c) Postprocedural, the feeding artery to the pseudoaneurysm was filled with coils (arrow) and lesion is no longer visible. (d) Direct image shows the coils in place (arrow)

(a) Contrast-enhanced MR shows right renal artery aneurysm (arrow), localized on the main trunk, a polar artery is also present (dashed arrow). (b) Same patient, selective angiography confirms the diagnosis. (c) After covered stent deployment (arrow), angiography shows complete exclusion of the aneurysmal sac
The possibility to use uncovered stent together with detachable coils in the case of wide-necked renal artery bifurcation aneurysms has also been reported (Manninen et al. 2008).
8 Arteriovenous Fistulas
Renal arteriovenous fistulas (RAVF) are a rare condition that can be acquired, congenital, or idiopathic. It usually affects patients who underwent a trauma or iatrogenic accidents. Iatrogenic RAVF are the most common and are usually asymptomatic, many regress spontaneously over time. However, symptoms due to high-output heart failure are reported. Imaging with CT or MR can be difficult, especially for the detection of the site of the fistula, and angiography is required for a definitive diagnosis using a selective catheterization. However, indirect signs may be easily detected on CTA as fast and high opacification of the renal vein and increase of its caliber. Traditionally, these arteriovenous fistulae were treated by surgery, but the mainstay of treatment has shifted to an endovascular approach by coil embolization (Sendi et al. 2005; Bozgeyik et al. 2008; Klein et al. 1996), (Fig. 7.20). Embolization procedures are often difficult secondary to problems due to “high flow” with a nonnegligible risk of distal embolization of coils. In these cases balloon occlusion angiography could be necessary (Mansueto et al. 2001). Recently, vascular plugs were also proposed (Campbell et al. 2009).

(a) Left kidney, selective angiography shows massive A-V fistula, from the main renal artery. (b) Later phase shows a dilated renal vein (arrow). (c) Postprocedural, the dilated feeding artery has been filled with several coils (arrow) and the A-V fistula is no longer visible
9 Trauma
Renal artery can be injured both in penetrating and nonpenetrating traumas. Moreover, iatrogenic accidents can be source of lesions affecting the main renal artery and distal branches.
Closed trauma consists mostly of renal contusions or small cortico-medullary tears: vascular pedicle of the kidney is injured only in fraction of cases, with thrombosis or dissection of the renal artery. More often than a nonpenetrating one, penetrating trauma can result in transection of the main renal artery. With the evolution of diagnostic imaging, mainly CT, there is always a more frequent possibility to detect bleeding lesions from the kidney caused by blunt traumas.
Angiography is required to assess if the lesion is amenable of treatment. Aortography is used to evaluate the basic anatomy and then selective renal angiography will be performed. From a diagnostic point of view, traumatic lesions appear as abnormal area of perfusion of the kidney with interrupted vessels or pseudoaneurysms or extravasation of contrast media and filling of the pyelocaliceal system. Angiography will also determine if the treatment could be endovascular or surgical (Fig. 7.21).

(a) Right kidney, selective angiography: multiple iatrogenic pseudoaneurysms of the distal branches (arrow), secondary to nephron sparing nephrectomy, are present. (b) Early filling of the caliceal system (arrow) confirms bleeding in direct connection with the urinary system. (c) Postprocedural: embolization with metallic coils (arrow) shows there is no more filling of the aneurysmal lesions. (d) A CT-angio was done before the catheter angiography, but it was able to show just a single (arrow) psuedoaneurysmal lesion
Iatrogenic lesions happen usually during a percutaneous drainage, biopsies, nephron sparing surgery, pyelostomies, and extra corporeal shock wave litotripsy and present clinically with fresh hemorrhage in the drainage tube and may involve the renal parenchyma or the collecting system or both. More rarely, the event could result in retroperitoneal hematoma.
In selected cases, the option to manage these lesions with an endovascular approach may be considered (Dinkel et al. 2002; Brewer et al. 2009).
10 Renal Transplantation
Evaluation of transplanted kidneys as a standard of care is performed with cross-sectional imaging, and most often, with ultrasonography (Bankier and Antretter 2008).
Angiography is used to provide a definitive diagnosis of renal artery stenosis and it should only be performed when percutaneous revascularization is already planned. To preserve renal function, it should be done with the lowest amount of iodine contrast agent or using protective agents as carbon dioxide (CO2).
Understanding the postoperative anatomy is useful to select the correct approach for diagnostic catheter placement. The first year after transplantation is special, as it is characterized by the highest rates of acute rejection and opportunistic infections. During the first month in more than 10% of transplanted kidney, a vascular complication occurs. When there is an acute thrombosis, loss of the kidney can be expected in most of the cases, due to the lack of collateral supply in the transplanted organ. Thrombosis can present early (surgical complications, acute rejection) or late due to rejection or artery stenosis. The stenosis can appear in any point of the inflow artery or usually localize far from the anastomosis, occurring predominantly in the distal segments of the donor artery. Transplant renal artery stenosis is the most frequent vascular complication following transplantation and is a potential curable cause of resistant hypertension, allograft dysfunction, and graft loss. Percutaneous angioplasty is the treatment of choice, but the incidence of restenosis may be as high as 35%. Alternative treatment option combines the angioplastic procedure with the placement of a stent. In the experience of Valpreda and Rabbia (Valpreda et al. 2008) of the 30 allograft that underwent stent placement with a mean follow-up time of 7.1 years, all were patent at the last follow-up, with five restenosis (15.6%) of which only one needed to be retreated endoluminally.
In a similar fashion, venous thrombosis occurs early (more common, 4% of transplants) or late, the kidney can then be compromised as in arterial thrombosis.
Close to the anastomosis, pseudoaneurysms can develop, commonly caused by infection. When pseudoanerysms appear in the renal parenchyma, they are usually subsequent from a postbioptic infection. Another complication of percutaneous biopsies is the formation of A-V fistulas.
11 Neoplasms
A variety of productive lesions can affect the kidney, malignant or benign in nature. Nowadays, the role of angiography in the diagnosis of renal masses is limited and cross-sectional imaging is currently used for diagnosis and staging. Still, some angiographic details are useful to understand and manage these lesions.
Signs exist that there are always strong predictors for malignant processes, the most reliable is the venous invasion or invasion of nearby structures by the tumor.
11.1 Benign Tumors
11.1.1 Angiomyolipoma (AML)
Renal AML are benign tumors composed by smooth muscle cells, adipose cells and have a rich vasculature. They may be solitary tumors or multiple and be associated to other manifestations (Bourneville disease). When small in size, they are asymptomatic, but if they grow over 4–5 cm in size, the risk of spontaneous bleeding significantly increase. At angiography AML is characterized by notable neoangiogenesis, sometimes associated with small asymmetrical aneurysms, and absence of shunting.
There are many reports in the literature about endovascular management of bleeding AML (Chang et al. 2007; Unlu et al. 2006; Van Baal et al. 1990) and also some reports about preventive embolization treatment in larger than 4 cm AML to avoid the risk of shock (Soulen et al. 1994; Kothary et al. 2005).
11.1.2 Oncocytoma
Oncocytoma are uncommon benign tumors usually seen in middle and old aged people, with man more commonly affected than women (1.7:1). Angiography shows a hypervascular mass with a spoke-wheel arrangement of tumor vessels and a typically central scar. Other signs are the absence of encasement, the detection of vascular occlusions, arteriovenous shunts, and contrast lakes. Frequently, a homogeneous tumor contrast during the capillary phase, a sharp demarcation from the kidney and surroundings, and a peritumoral halo are observed. Also, CT scan is characteristic when able to demonstrate the central scar, which shows low attenuation values compared to the rest of the lesion generally showing homogeneous high attenuation value. This tumor has a slow growth and is generally asymptomatic, and no reports about endovascular management of this lesion are reported.
11.2 Malignant Tumors
11.2.1 Advanced Renal Cell Carcinomas
Progress in the diagnosis of early stages of renal carcinomas as well as the improvement of both surgical techniques and anesthetic procedures has lead to a change in the selection of patients for embolization. The main indications for kidney embolization of advanced renal cell carcinomas are tumors with thrombus into the vena cava or T4 tumors. Other indications are bleeding from inoperable kidney tumor or symptomatic inoperable kidney tumor causing flank pain or paraneoplastic syndromes, but asymptomatic inoperable kidney tumor can also be treated if this is the patient’s wish (Hallscheidt et al. 2006). Other indications are patients with poor general conditions or with advanced metastatic disease. The complete occlusion of the vascular bed of the tumors leads to a considerable reduction in intraoperative blood loss and to simplification of the surgical preparation. By using particulate embolic agents derived from PVA or metallic coils (Fig. 7.22) or absolute alcohol or glue, palliation of a hemorrhage or of tumor-related pain in inoperable patients is usually successful in about 90% of patients (Hallscheidt et al. 2006). Although local control of the tumor disease, including complete tumor ablation, is achieved by embolization, the median survival rate of palliatively embolized patients is low (Hansmann et al. 1999). Complications of the procedure are pain due to renal infarction, which sometimes need to be treated with analgesics and transitory fever (Guy et al. 2007).

(a, b) CT-angio, coronal and sagittal reformats, show a renal tumor in a solitary malrotated kidney (arrow). (c) Aortography shows a main right renal artery (dashed arrow) and a polar artery (arrow). (d) Selective catheterism of this polar artery shows a highly vascularized tumor. (e, f) Angiography after embolization with particles and coils (arrow)
Kidney tumor embolization was proposed also in patients with solitary kidney (Deutz et al. 1988; Kozak et al. 1987).
11.2.2 Malignant Lesions
Renal cell carcinoma has a variable, but usually prominent degree of neoangiogenesis; it is hypervascular, with mass effect on nearby parenchima; shunting is present. Preoperative embolization may be helpful in patients undergoing laparoscopic “nephron-sparing surgery” with the aim to reduce intraoperative bleeding.
Transitional cell carcinoma usually presents neoangiogenesis; it is slightly hypervascular and can encase nearby structures; shunting is not an usual feature.
Lymphoma is predominantly avascular, with mass effects on normal surrounding renal vasculature.
Metastatic carcinoma, depending on the primary cancer, can present as avascular (breast, lung, gastrointestinal) or hypervascular (melanoma, sarcoma).
References
Akan H, Arik N, Saglam S et al. (2003) Evaluation of the patients with renovascular hypertension after percutaneous revascularization by doppler ultrasonography. Eur J Radiol 46(2):124–129
Bankier AA, Antretter H (2008) Imaging in transplantation. Springer, Berlin
Beckmann CF, Abrams HL (1979) Circumaortic venous ring: incidence and significance. AJR Am J Roentgenol 132(4):561–565
Beckmann CF, Abrams HL (1980) Renal venography: anatomy, technique, applications, analysis of 132 venograms, and a review of the literature. Cardiovasc Intervent Radiol 3(1):45–70
Blondin D, Lanzman R, Schellhammer F et al. (2009) Fibromuscular dysplasia in living renal donors: still a challenge to computed tomographic angiography. Eur J Radiol. [Epub ahead of print]
Blum U, Krumme B, Flugel P et al. (1997) Treatment of ostial renal-artery stenoses with vascular endoprostheses after unsuccessful balloon angioplasty. N Engl J Med 336(7):459–465
Bozgeyik Z, Ozdemir H, Orhan I et al. (2008) Pseudoaneurysm and renal arteriovenous fistula after nephrectomy: two cases treated by transcatheter coil embolization. Emerg Radiol 15(2):119–122
Brewer ME Jr, Strnad BT, Daley BJ et al. (2009) Percutaneous embolization for the management of grade 5 renal trauma in hemodynamically unstable patients: Initial experience. J Urol 181(4):1737–1741
Bruce M, Kuan YM (2002) Endoluminal stent-graft repair of a renal artery aneurysm. J Endovasc Ther 9(3):359–362
Cam A, Chhatriwalla AK, Kapadia SR (2010) Limitations of angiography for the assessment of renal artery stenosis and treatment implications. Catheter Cardiovasc Interv 75:38–42
Campbell JE, Davis C, Defade BP et al. (2009) Use of an amplatzer vascular plug for transcatheter embolization of a renal arteriovenous fistula. Vascular 17(1):40–43
Canzanello VJ, Millan VG, Spiegel JE et al. (1989) Percutaneous transluminal renal angioplasty in management of atherosclerotic renovascular hypertension: results in 100 patients. Hypertension 13(2):163–172
Chang YH, Wang LJ, Chuang CK et al. (2007) The efficacy and outcomes of urgent superselective transcatheter arterial embolization of patients with ruptured renal angiomyolipomas. J Trauma 62(6):1487–1490
Cluzel P, Raynaud A, Beyssen B et al. (1994) Stenoses of renal branch arteries in fibromuscular dysplasia: results of percutaneous transluminal angioplasty. Radiology 193(1):227–232
Corriere MA, Edwards MS, Pearce JD et al. (2009) Restenosis after renal artery angioplasty and stenting: incidence and risk factors. J Vasc Surg 50:813–819
Deutz FJ, Rubben H, Vorwerk D et al. (1988) Superselective embolization of inoperable renal carcinoma in patients with solitary kidney. Eur Urol 15(1–2):134–138
Dinkel HP, Danuser H, Triller J (2002) Blunt renal trauma: minimally invasive management with microcatheter embolization experience in nine patients. Radiology 223(3):723–730
Dorros G, Jaff M, Mathiak L et al. (1998) Four-year follow-up of palmaz-schatz stent revascularization as treatment for atherosclerotic renal artery stenosis. Circulation 98(7):642–647
English WP, Pearce JD, Craven TE et al. (2004) Surgical management of renal artery aneurysms. J Vasc Surg 40(1):53–60
Fauci AS, Harrison TR (2009) Harrison’s manual of medicine, 17th edn. McGraw-Hill, New York
Ferris EJ (1969) Venography of the inferior vena cava and its branches. Williams & Wilkins, Baltimore
Glodny B, Glodny DE (2006) John loesch, discoverer of renovascular hypertension, and harry goldblatt: Two great pioneers i Weinberg MD (2010) Stenting for atherosclerotic renal artery stenosis: one poorly designed trial after another. Cleveland Clinic Journal of Medicine 77(3); 164-171 n circulation research. Ann Intern Med 144(4):286–295
Goldblatt H (1934) The production of persistent elevation of sistolic blood pressure by means of renal ischemia. J Exp Med 59:347–379
Guy L, Alfidja AT, Chabrot P et al. (2007) Palliative transarterial embolization of renal tumors in 20 patients. Int Urol Nephrol 39(1):47–50
Guyton AC, Hall JE (2006) Textbook of medical physiology, 11th edn. Elsevier Saunders, Philadelphia
Hallscheidt P, Besharati S, Noeldge G et al. (2006) Preoperative and palliative embolization of renal cell carcinomas: follow-up of 49 patients. Rofo 178(4):391–399
Hansmann HJ, Hallscheidt P, Aretz K et al (1999) [Renal tumor embolization]. Radiologe 39(9):783–789
Harrington DP, Levin DC, Garnic JD et al. (1983) Compound angulation for the angiographic evaluation of renal artery stenosis. Radiology 146(3):829–831
Hartman RP, Kawashima A (2009) Radiologic evaluation of suspected renovascular hypertension. Am Fam Physician 80(3):273–279
Henry M, Henry I, Klonaris C et al. (2003) Renal angioplasty and stenting under protection: the way for the future? Catheter Cardiovasc Interv 60(3):299–312
Jokhi PP, Ramanathan K, Walsh S et al. (2009) Experience of stenting for atherosclerotic renal artery stenosis in a cardiac catheterization laboratory: technical considerations and complications. Can J Cardiol 25(8):e273–e278
Kadir S, Brothers MF (1991) Atlas of normal and variant angiographic anatomy, 1st edn. Saunders, Philadelphia
Kahn (1973) Selective venography of the branches. In: Krieger (ed) Venography of the inferior vena cava and its branches. Huntington, NY, 154–224
Kaufman JA (2003) Vascular and interventional radiology. Mosby, St. Louis
Kidney DD, Deutsch LS (1996) The indications and results of percutaneous transluminal angioplasty and stenting in renal artery stenosis. Semin Vasc Surg 9(3):188–197
Klein GE, Szolar DH, Breinl E et al. (1997) Endovascular treatment of renal artery aneurysms with conventional non-detachable microcoils and guglielmi detachable coils. Br J Urol 79(6):852–860
Klein GE, Szolar DH, Karaic R et al. (1996) Extracranial aneurysm and arteriovenous fistula: embolization with the guglielmi detachable coil. Radiology 201(2):489–494
Kothary N, Soulen MC, Clark TW et al. (2005) Renal angiomyolipoma: long-term results after arterial embolization. J Vasc Interv Radiol 16(1):45–50
Kozak BE, Keller FS, Rosch J et al. (1987) Selective therapeutic embolization of renal cell carcinoma in solitary kidneys. J Urol 137(6):1223–1225
Kumar V (2009) Robbins and cotran pathologic basis of disease, 8th edn. Saunders, Philadelphia
Liguori G, Trombetta C, Bucci S et al. (2002) Percutaneous management of renal artery aneurysm with a stent-graft. J Urol 167(6):2518–2519
Leonardi M, Barbara C, Simonetti L et al. (2002) Glubran 2: a new acrylic glue for neuroradiological endovascular use experimental study on animals. Interv Neuroradiol 8:245–250
Manninen HI, Berg M, Vanninen RL (2008) Stent-assisted coil embolization of wide-necked renal artery bifurcation aneurysms. J Vasc Interv Radiol 19(4):487–492
Mansueto G, D’onofrio M, Minniti S et al. (2001) Therapeutic embolization of idiopathic renal arteriovenous fistula using the “Stop-flow” technique. J Endovasc Ther 8(2):210–215
Morita T, Uekado Y, Kyoku I et al. (1989) [Transcatheter arterial embolization in patients with renal arteriovenous malformation: a report of two cases]. Hinyokika Kiyo 35(10):1761–1765
Olin JW (2007) Recognizing and managing fibromuscular dysplasia. Cleve Clin J Med 74(4):273–274, 277–282
Olin JW, Piedmonte M, Young JR et al. (1995) The utility of duplex ultrasound scanning of the renal arteries for diagnosing significant renal artery stenosis. Ann Intern Med 122:833–836
Ozkan U, Oguzkurt L, Tercan F et al. (2006) Renal artery origins and variations: angiographic evaluation of 855 consecutive patients. Diagn Interv Radiol 12(4):183–186
Parenti GC, Palmarini D, Bilzoni M et al. (2008) Role of color-doppler sonography in the follow-up of renal artery stenting. Radiol Med 113(2):242–248
Plouin PF, Chatellier G, Darne B et al. (1998) Blood pressure outcome of angioplasty in atherosclerotic renal artery stenosis: a randomized trial. Essai multicentrique medicaments vs angioplastie (emma) study group. Hypertension 31(3):823–829
Raynaud AC, Beyssen BM, Turmel-Rodrigues LE et al. (1994) Renal artery stent placement: Immediate and midterm technical and clinical results. J Vasc Interv Radiol 5(6):849–858
Rocha-Singh K, Jaff MR, Lynne Kelley E (2008) Renal artery stenting with noninvasive duplex ultrasound follow-up: 3-year results from the renaissance renal stent trial. Catheter Cardiovasc Interv 72(6):853–862
Safian RD, Textor SC (2001) Renal-artery stenosis. N Engl J Med 344(6):431–442
Satyapal KS, Kalideen JM, Haffejee AA et al. (1999) Left renal vein variations. Surg Radiol Anat 21(1):77–81
Scheinert D, Braunlich S, Nonnast-Daniel B et al. (2001) Transradial approach for renal artery stenting. Catheter Cardiovasc Interv 54(4):442–447
Schneidereit NP, Lee S, Morris DC et al. (2003) Endovascular repair of a ruptured renal artery aneurysm. J Endovasc Ther 10(1):71–74
Schreiber MJ, Pohl MA, Novick AC (1984) The natural history of atherosclerotic and fibrous renal artery disease. Urol Clin North Am 11(3):383–392
Sendi P, Toia D, Nussbaumer P (2005) Percutaneous embolization of renal arteriovenous fistula. Vasa 34(3):207–210
Sharafuddin MJ, Raboi CA, Abu-Yousef M et al. (2001) Renal artery stenosis: duplex us after angioplasty and stent placement. Radiology 220(1):168–173
Slovut DP, Olin JW (2004) Fibromuscular dysplasia. N Engl J Med 350(18):1862–1871
Soulen MC, Faykus MH Jr, Shlansky-Goldberg RD et al. (1994) Elective embolization for prevention of hemorrhage from renal angiomyolipomas. J Vasc Interv Radiol 5(4):587–591
Soulez G, Pasowicz M, Benea G et al. (2008) Renal artery stenosis evaluation: Diagnostic performance of gadobenate dimeglumine-enhanced mr angiography–comparison with dsa. Radiology 247(1):273–285
Steinwender C, Schutzenberger W, Fellner F et al. (2009) 64-detector ct angiography in renal artery stent evaluation: prospective comparison with selective catheter angiography. Radiology 252(1):299–305
Talovic E, Kulenovic A, Voljevica A et al. (2004) Angiographic imaging of supernumerary kidney arteries by nonselective angiography. Med Arh 58(5):263–267
Tello R, Thomson KR, Witte D et al. (1998) Standard dose Gd-DTPA dynamic MR of renal arteries. J Magn Reson Imaging 8(2):421–426
Tham G, Ekelund L, Herrlin K et al. (1983) Renal artery aneurysms. Natural history and prognosis. Ann Surg 197(3):348–352 The Astral Investigators (2009) Revascularization versus medical therapy for renal artery stenosis. N Eng J Med 361; 1953–1962
Tollefson DF, Ernst CB (1991) Natural history of atherosclerotic renal artery stenosis associated with aortic disease. J Vasc Surg 14(3):327–331
Unlu C, Lamme B, Nass P et al. (2006) Retroperitoneal haemorrhage caused by a renal angiomyolipoma. Emerg Med J 23(6):464–465
Valpreda S, Messina M, Rabbia C (2008) Stenting of transplant renal artery stenosis: outcome in a single center study. J Cardiovasc Surg (Torino) 49(5):565–570
Van Baal JG, Lips P, Luth W et al. (1990) Percutaneous transcatheter embolization of symptomatic renal angiomyolipomas: a report of four cases. Neth J Surg 42(3):72–77
Van De Ven PJ, Beutler JJ, Kaatee R et al. (1995) Transluminal vascular stent for ostial atherosclerotic renal artery stenosis. Lancet 346(8976):672–674
Verschuyl EJ, Kaatee R, Beek FJ et al. (1997a) Renal artery origins: location and distribution in the transverse plane at ct. Radiology 203(1):71–75
Verschuyl EJ, Kaatee R, Beek FJ et al. (1997b) Renal artery origins: best angiographic projection angles. Radiology 205(1):115–120
Weinberg MD (2010) Stenting for atherosclerotic renal artery stenosis: one poorly designed trial after another. Cleveland Clinic Journal of Medicine 77(3); 164–171
Zahringer M, Sapoval M, Pattynama PM et al. (2007) Sirolimus-eluting versus bare-metal low-profile stent for renal artery treatment (great trial): angiographic follow-up after 6 months and clinical outcome up to 2 years. J Endovasc Ther 14(4):460–468
Zeller T (2005) Renal artery stenosis: epidemiology, clinical manifestation, and percutaneous endovascular therapy. J Interv Cardiol 18(6):497–506
Zeller T, Frank U, Muller C et al. (2003) Technological advances in the design of catheters and devices used in renal artery interventions: Impact on complications. J Endovasc Ther 10(5):1006–1014
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2010 Springer Berlin Heidelberg
About this chapter
Cite this chapter
Pozzi-Mucelli, F., Pellegrin, A. (2010). Renal Angiography and Vascular Interventional Radiology. In: Quaia, E. (eds) Radiological Imaging of the Kidney. Medical Radiology(). Springer, Berlin, Heidelberg. https://doi.org/10.1007/978-3-540-87597-0_7
Download citation
DOI: https://doi.org/10.1007/978-3-540-87597-0_7
Published:
Publisher Name: Springer, Berlin, Heidelberg
Print ISBN: 978-3-540-87596-3
Online ISBN: 978-3-540-87597-0
eBook Packages: MedicineMedicine (R0)