
Abstract
In Finland, the advanced practice nursing roles emerged in the early 2000s in university hospital settings. By 2018, there are around 80 clinical nurse specialists, and the numbers continue to rise. Currently the clinical nurse specialist roles are not regulated in Finland, and there is no title protection for these roles. Healthcare organizations control the use of titles and job descriptions; however, the need to push forward the regulation and licensure has been recognized as an important national goal concerning the development of these roles. The first national frameworks to guide the role development and implementation have commenced only recently. Although the national advanced practice nursing frameworks have taken time to evolve, the development of the clinical nurse specialist competencies is well on its way giving guidance to the role and practice development and implementation. Several central stakeholders, such as the Finnish Nurses Association, ministries, administrators, educators, and researchers, are working in close collaboration to support the clinical nurse specialist role and practice development.
This chapter has been written before the 2020 APN ICN guidelines were published and reflects the views of the authors.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
1 Brief History of CNS Role and Practice
In Finland, the advanced practice nursing (APN) roles emerged in the early 2000s to respond to the increasing complexity and needs of the healthcare environment, such as requirements of rapid access to high-quality care, managing changing environments, and developing evidence-based practices (EBP) (Fagerström 2009; Jokiniemi 2014). The first implementation of the APN role, the clinical nurse specialist (CNS), was carried out in 2001 at the Helsinki University Hospital (Meretoja and Vuorinen 2000; Meretoja et al. 2002). During the past 5 years, the numbers of CNS positions have tripled, with around 80 CNSs working around the country in 2018. The numbers of CNS positions continue to rise as the healthcare organizations are increasingly investing to these roles. By the year of 2025, the CNS positions are expected to double.
The CNS role and practice was initially developed and implemented in university hospital settings, and majority of the CNSs today practice in in-hospital practice settings. The CNS’s central focus of practice is advanced clinical nursing. The primary practice goal is to ensure and improve the quality of clinical care, support staff and multidisciplinary teams in clinical care provision, endorse organizations’ clinical performance, and foster the advancement of clinical nursing through scholarship activities (Jokiniemi 2014). In a country with 5.5 million people, Finland has around 80,000 registered nurses (RN), which account for 14.7 per 1000 population which is 4 times higher than the number of physicians (3.2 per 1000 population) (OECD.Stat 2018). As the numbers of CNSs are still low, representing less than 0.5% of the nursing population, a challenge is whether the CNSs are able to work in close proximity from the direct patient care. In several organizations, in this early phase of role development, placing the very few first CNSs has been strategic aiming to benefit and support healthcare organizations in increasing the quality of patient care and EBP by scholarship activities. Only in few instances, the CNS practice involves 50% of time allocated to advanced clinical nursing domain. More resources are needed to revenue the scope of practice into advanced clinical direct patient care.
2 Definition of CNS
The role and practice of the CNS is evolving in Finland. There is a national consensus definition of the role and scope of practice and recommendations for future development (Kotila et al. 2016; Jokiniemi et al. 2020). Based on the national research (Jokiniemi 2014; Jokiniemi et al. 2015a, 2018) and role and practice development (Kotila et al. 2016, 2018; Jokiniemi 2018, 2020), the CNS role may be defined as follows:
Clinical nurse specialist is an experienced master’s or doctoral prepared registered nurse whose central focus of practice is advanced clinical nursing. The aim of the role is to support healthcare organizations to achieve their strategic goals, to assure and increase the quality and effectiveness of patient care, and to improve the merging of evidence-based practice and scholarship activities. Clinical nurse specialist role domains are advanced clinical practice and practice development, consultation and staff education, transformational leadership, and scholarship activities. The role actualizes through direct and indirect evidence-based patient care influencing positively to the patient care, nursing profession, organization, scholarship, and the community at large.
3 Conceptualizations/Model(s) of CNS Practice
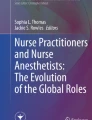
CNS is an APN role. In Finland, the APN roles currently include the roles of the CNS and nurse practitioner (NP). The CNS role development in Finland, while following closely to the international role development and visions, has been impacted by the healthcare needs and the current reform of the social and healthcare services. The initial CNS role conceptualization took place in the national doctoral dissertation study in 2014 (Jokiniemi 2014), where the CNS role conceptualization, implementation, and evaluation framework was developed. In this framework, the central concepts of the CNS roles and practice as well as continuous phases of analyzing the CNS role need, designing and implementing the role, and evaluating the role, were described. Following this initial research, the Finnish Nursing Association’s expert group has taken an active role in modeling nurses’ career from registered nurse to APN. The nurses’ clinical career model includes three competency levels: registered nurse, specialized nurse, and advanced practice nurse, which includes the roles of CNS and NP (Fig. 9.1). Furthermore, advanced practice nurses have an opportunity to get limited prescription rights, by completing a separate postgraduate training worth 45 European Credit Transfer and Accumulation System (ECTS) credits. Nurse prescribers are licensed by the National Supervisory Authority for Welfare and Health (Kotila et al. 2016).

Nurses’ clinical career (Modified from Jokiniemi et al. 2018). RN registered nurse, SRN specialized registered nurse, APN advanced practice nurse, CNS clinical nurse specialist, NP nurse practitioner, ECTS European Credit Transfer and Accumulation System
4 CNS Practice Competencies
To achieve the role expectations, CNSs need clinical knowledge and skills beyond the level of frontline nursing. Uppermost of importance in developing the advanced competencies needed are prior nursing experience and an education at master’s or doctoral level (ICN 2014; Sheer and Wong 2008). Furthermore, within the dynamic healthcare environment, the characteristics of capability, such as knowledge on learning, creativity, self-efficacy, and working with others, are utilized to support better role achievement (Hase and Davis 1999; Gardner et al. 2008).
The development of the CNS practice competency descriptions is ongoing in Finland. The initial competency descriptions were scientifically validated and first published in 2014 (Jokiniemi 2014). Hence in 2014, these competency descriptions have been further validated in a national study through rigorous mixed-method research project. The development of a competency scale for CNSs involved examination and comparison of the Finnish competencies against the US and Canadian competency sets (Baldwin et al. 2007; CNA 2014), as well as expert and practicing CNS evaluations of the competency scale. This scale has demonstrated strong content validity within the national context (Jokiniemi et al. 2018). It has been tested in terms of content and construct validity within the Scandinavian context (Jokiniemi et al. 2020).
The Finnish CNS competencies cover the spheres of patient, nursing, organization, and scholarship. The patient sphere encompasses evidence-based clinical practice, management of complex patient populations, and promotion of ethical patient-centered care. The nursing sphere involves CNS activities to ensure the quality of the nursing practice and support of staff knowledge as well as facilitation of healthy work environment. Organizational sphere competencies, in turn, involve integration and promotion of EBP, support of practice development and innovation, and transformational leadership. Lastly, the scholarship sphere competencies contain leadership and assessment of quality improvement projects/EBP as well as promotion of research and knowledge translation activities within the organization. The advanced-level competencies of the CNSs overlap with each other and are utilized in direct and indirect patient care to achieve the role expectations (Jokiniemi 2014; Jokiniemi et al. 2018, 2020).
5 Outcome Measures and Evaluation
Definition of specific outcome measures and research-based evaluation is still the most underdeveloped area of the CNS role and practice implementation in Finland. The importance of evaluating the outcomes of the CNS role and practice as well as economical evaluation is recognized (Jokiniemi 2018). However, in this early phase of the CNS role development, there are inconsistencies with the role definitions and the scope of practice within various healthcare organizations. Therefore, defining and measuring the CNS-sensitive outcomes in the role domains of advanced clinical practice and practice development, consultation and staff education, as well as transformational leadership and scholarship activities is challenging.
Individual PhD researchers and master’s students have conducted outcome assessments of the CNS roles, which have centered on the first experiences of the role implementation and perceptions of the roles (Viholainen 2018; Jokiniemi et al. 2015b). Evaluation research projects are greatly needed to show evidence of the CNS role impact on various aspects of direct and indirect patient care and EBP. Besides the outcomes in clinical nursing, the CNS role is influencing positively to the nursing profession, scholarship, and the community at large. In the future, it is imperative to collect evaluation data, conduct larger-scale national studies, and take part in international outcome studies, in order to evaluate the CNS practice structures, processes, and outcomes (Donabedian 2005; Kilpatrick et al. 2016) from the perspectives of patient, nursing, organization, and the community at large.
6 CNS Education
Finland has a dual system of higher education, with both universities and universities of applied sciences (UAS) offering master’s-level education in nursing. The entry requirement to both education systems is a bachelor’s degree in nursing (Ministry of Education and Culture 2014*). It takes 3.5 years to complete bachelor-level degree (210 European Credit Transfer and Accumulation System [ECTS] credits) and between 1½ and 3 years to get the master’s degree in nursing (300 ECTS credits). The content of master’s-level education that prepares nurses for advanced clinical nursing roles and practice, both in UAS (90 ECTS credits) and universities (300 ECTS credits), is currently under evaluation and further development. Universities have provided master’s-level education for nurses since 1979 with advanced clinical nursing programs in place since 1991 (Suominen and Leino-Kilpi 1995). The UAS, in turn, piloted degree program in advanced nursing practice the first time in 2006 (Fagerström and Glasberg 2011), which was formalized by the Ministry of Education and Culture in 2010. Typically, the CNSs have attained their education from the university.
Despite the rather long history of specialist-level practice and existing master’s-level educational programs, there is no nationally congruent curriculum for advanced practitioners or no uniform national education programs in place for these roles (Jokiniemi 2014; Hukkanen and Vallimes-Patomäki 2005). There are only singular governing national documents on the concept of advanced practitioners and their responsibilities or education. To better answer to the requirements of the advanced practitioner education, several stakeholders and institutions are presently examining the curriculums.
It is generally accepted that the minimum requirement for the CNS role is the master’s-level education. However, currently several CNSs in Finland held a doctoral degree or are pursuing one in nursing science. The doctoral degree in nursing science is a thesis based, and therefore is not clinically weighed, but prepares the CNSs to better achieve the scholarship aspects of the CNS role. Based on the initial national recommendations for nurse training, it may be concluded that the registered nurse has a possibility to advance in clinical nursing through three steps: (1) specializing in nursing (30 to 60 ECTS credits), (2) master’s-level advanced practice nurse education (210 + 90/300 ECTS credits), and (3) doctorate-level education (Jokiniemi 2014, 2020; MSAH 2012).
7 Credentialing: Regulatory, Legal, and Certification Requirements
National legislation closely regulates the professional practice of healthcare personnel. The National Supervisory Authority for Welfare and Health (Valvira) grants upon application the right to practice as a licensed or authorized professional and authorizes the use of the occupational title of healthcare professional. Currently there are no legislative and regulatory mechanisms or protected titles in place for advanced practitioners. The CNS roles are regulated by the legislation on registered nurses and guided by individual organizational policies (Kotila et al. 2016; Jokiniemi et al. 2014).
Although the need for credentialing the CNS roles was recognized within a national policy Delphi study, the probability of taking forward the individual aspects of credentialing such as title protection, national registration, and regulation was perceived as low (Jokiniemi et al. 2015a). Although regulatory issues may take a long time to actualize (Arslanian-Engoren et al. 2011; Bryant-Lukosius et al. 2010), and despite the challenges, developing the prospects of the role regulation and credentialing is the ambition of the central CNS role developers/pioneers. The Finnish Nurses Association’s APN expert group, set up in 2013, continues to strive for the clarification and integration of the advanced nursing roles and practice. Following the conceptualization of the advanced practice roles completed in 2016 (Kotila et al. 2016; Jokiniemi et al. 2020), the next step is to press for the development of the education and credentialing of these roles. The FNA’s expert group involves members from several facets such as education, healthcare organizations, researchers, as well as collaborators from the Ministries of Social Affairs and Health and Education and Culture, thus involving valuable expertise and leveraging on role development.
8 Moving Forward: Challenges and Opportunities
Some of the role and practice challenges for APN in Finland include further development of the scope of practice for CNSs as well as for NPs. The educational preparation/curriculum for these new advanced clinical roles needs to answer to the challenges in patient population and the society. Educational preparation for advanced clinical nursing requires high educator competencies in clinical nursing and clinical nursing science. It also requires strong educational collaboration with the medical faculty members and clinicians. Moreover, there is a need to develop continuous training possibilities for practicing CNSs to maintain and update their knowledge.
Despite recent progress on the CNS role and practice development in Finland, we still have many challenges ahead. In the future, we need to focus more closely to the clinical aspects of the advanced direct patient care and to further develop the implementation of full scope of APN and autonomous role to better answer to the needs of patient population and the society. Furthermore, we need to push for credentialing of these roles to foster the role and practice recognition and sustainability of these roles.
The role and practice opportunities of the CNSs are vast yet underutilized in Finland. There is great interest to develop and create these roles with the ongoing social and healthcare reform; thus the advanced nursing roles have a significant position in the production of future healthcare services. Significant factors for success are the influential national APN expert network engaged in advancing the APN role development and visibility. This work is supported by the involvement and close collaboration of Ministry of Social Affairs and Health and Ministry of Education and Culture in the development of the APN roles.
Furthermore, the research in the area of CNS role development and implementation is expanding rapidly. There is a growing body of national research on the CNS role and practice from master’s to postdoctoral study. Funding is available for strong proposals on the CNS/APN research. Furthermore, the development and research of these roles is supported by the national legislation regulating the healthcare and healthcare professionals (Healthcare Professionals Act 1994, Health Care Act 2010) supporting the continuous efforts of CNS practice and role development.
9 Exemplar of Clinical Nurse Specialist Practice
9.1 Description of Neuroscience Specialty Practice
In specialist medical healthcare, the CNSs work usually within specialty patient population; however, CNS practice varies across different organizations. In some organizations, it has been specified that the CNS should spent 50% of time in clinical practice and 50% in other activities, but it is not the case in all of the organizations. Our example of specialty practice area comes from neuroscience nursing. The Neuro Center (NC) consists of 5 hospitals, with neurology or neurosurgery polyclinics and 14 wards. Surgery, emergency, and power control operations are mainly concentrated in main Helsinki University Hospital area. NC has 670 staff, of which 127 are doctors and 442 are nurses. The NC has almost 17,000 transcripts every year; it manages approximately 9500 emergency patients and makes approximately 3500 operations. The NC also has national responsibility for the leadership of the neuroscience specialty. One CNS works at the NC, where her practice focuses on facilitating EBP within the specialty, supporting the multidisciplinary team, and working at a system level to foster change. To enact these priorities, the CNS serves as an expert educator, consultant, transformational leader, a mentor, and a facilitator of research.
9.2 Exemplary CNS Project in the Specialty of Neuroscience
One exemplary CNS-led project relates to prevention of ventilator-associated pneumonia (VAP). The goal was to focus on VAP prevention by utilizing endotracheal tubes with subglottic secretion drainage ports for patients expected to require greater than 48 or 72 hours of mechanical ventilation. During the project, the CNS-led team developed a VAP prevention protocol (VAP-PP) and education program for NC. The CNS implemented the staff education, carefully explaining each VAP-PP step to the nursing staff to build up their skill and confidence level. During the initial implementation of the VAP-PP, it was important for the CNS, nurse manager, and the critical care physician to provide support for staff and lead by example to demonstrate the skills necessary to facilitate the desired change.
Another CNS-led project was the creation of the Nurses’ Neuroscience Handbook (NNH) (2021). The idea was drawn from nursing students’ quality improvement project. The goal of the NNH was to provide nurses an easy access guide related to neuroscience nursing, its policies, procedures, and outcomes. The NNH encompasses both research evidence and the silent knowledge gathered from the organization. The creation of the NNH actualized through series of steps and decisions. Today NNH works as an evidence-based road map for nurses on how to operate within neuroscience nursing. Standardized practice protocols, such as the NNH, incorporate evidence into the nursing practice and assist nurses to improve their performance.
9.3 Practice Competencies Used in the Projects
In the described projects, the CNS had a vital role in applying research evidence into nursing practice, educating and consulting staff, and leading the transformation of nursing practice. Moreover, several competencies were required to accomplish the projects’ goals. The CNS utilized competencies within all of the spheres of patient, nursing, organization, and scholarship working in close collaboration with the multidisciplinary team within the NC.
9.4 Outcomes of CNS Practice Within the Projects
The VAP-PP was developed, implemented, and reinforced by the CNS-led team. The CNS leadership of the project was time-consuming and required extensive preparation for meetings, assisting nurses with their work, providing feedback to the units, and facilitating the multidisciplinary involvement in the project. Implementation of evidence-informed VAP prevention protocol reduced significantly the incidence of VAP.
Challenges in the implementation of the NNH existed at each stage of the process due to general opposition from multiple areas to practice change, as well as the diversity of specialties (such as neurosurgery and neurology) which had their own customs of practice. Despite the challenges, it is imperative to CNS practice to focus on providing the best possible care for patients. Implementing the NNH created an opportunity to engage staff nurses in EBP and to improve the care of patients by harmonizing and integrating the nursing practices within the NC. Nowadays, the NNH is widely used in other university hospitals in Finland. Next step is to develop digital NNH as a part of digital Health Village.
References
Arslanian-Engoren C, Struble L, Sullivan B (2011) An innovative approach to revising a clinical nurse specialist curriculum to meet core competencies in 3 specialty tracks (adult health, gerontology, and psychiatric-mental health). 2011 National Association of clinical nurse specialists National Conference Abstracts, Baltimore, Maryland, March 10 to 12. Clin Nurse Spec 25:77–77
Baldwin KM, Lyon BL, Clark AP, Fulton J, Davidson S, Dayhoff N (2007) Developing clinical nurse specialist practice competencies. Clin Nurse Spec 21:297–303
Bryant-Lukosius D, Carter N, Kilpatrick K, Martin-Misener R, Donald F, Kaasalainen S et al (2010) The clinical nurse specialist role in Canada. Nurs Leadersh 23:140–166
CNA (2014) Pan-Canadian core competencies for the clinical nurse specialist. https://www.cna-aiic.ca/~/media/cna/files/en/clinical_nurse_specialists_convention_handout_e.pdf?la=en. Accessed 15 May 2018
Donabedian A (2005) Evaluating the quality of medical care. Milbank Q 83:691–729
Fagerström L (2009) Developing the scope of practice and education for advanced practice nurses in Finland. Int Nurs Rev 56:269–272
Fagerström L, Glasberg A (2011) The first evaluation of the advanced practice nurse role in Finland—the perspective of nurse leaders. J Nurs Manag 19:925–932
Gardner A, Hase S, Gardner G, Dunn SV, Carryer J (2008) From competence to capability: a study of nurse practitioners in clinical practice. J Clin Nurs 17:250–258
Hase S, Davis L From competence to capability: the implications for human resource development and management. Paper presented to Millennial challenges in management, education, cybertechnology, and leadership: Association of International Management, 17th Annual Conference, San Diego, 6–8 August 1999. https://epubs.scu.edu.au/cgi/viewcontent.cgi?referer=https://scholar.google.ca/&httpsredir=1&article=1126&context=gcm_pubs. Accessed 15 May 2018
Healthcare Professionals Act. No. 559/1994. [English]. http://www.finlex.fi/en/laki/kaannokset/1994/en19940559.pdf. Accessed 15 May 2018
Health Care Act. No. 1326/2010. [English]. https://www.finlex.fi/fi/laki/kaannokset/2010/en20101326_20131293.pdf. Accessed 22 April 2021
Hukkanen E, Vallimes-Patomäki M Co-operation and Division of Labour in securing access to care. A survey of the pilot projects on Labour Division carried out within the National Health Care Project. Reports of the Ministry of Social Affairs and Health: 21, Finland. 2005
ICN. International Council of Nurses (2014) Definition of nurse practitioner/advance practice nurse. Definition and characteristics of the role. http://international.aanp.org/Practice/APNRoles. Accessed 15 May 2018
Jokiniemi K (2014) Clinical nurse specialist role in Finnish Health Care. Doctoral dissertation, University of Eastern Finland. http://epublications.uef.fi/pub/urn_isbn_978-952-61-1579-5/urn_isbn_978-952-61-1579-5.pdf. Accessed 15 May 2018
Jokiniemi K (2018) Advanced practice nursing roles—towards optimal role utilization. Pro Terveys. [Finnish]
Jokiniemi K, Haatainen K, Pietilä A (2014) Advanced practice nursing roles: the phases of the successful role implementation process. Int J Caring Sci 7:946
Jokiniemi K, Haatainen K, Meretoja R, Pietilä A (2015a) The future of the clinical nurse specialist role in Finland. J Nurs Scholarsh 47:78–86
Jokiniemi K, Haatainen K, Pietilä A (2015b) From challenges to advanced practice registered nursing role development: qualitative interview study. Int J Nurs Pract 21:896–903
Jokiniemi K, Pietilä A, Meretoja R (2018) Constructing content validity of clinical nurse specialist core competencies. Scand J Caring Sci 32(4):1428–1436
Jokiniemi K, Suutarla A, Meretoja R, Kotila J, Axelin A, Flinkman M, Fagerström L (2020) Evidence‐informed policymaking: modelling nurses’ career pathway from registered nurse to advanced practice nurse. Int J Nurs Pract 26(1):e12777. https://doi.org/10.1111/ijn.12777
Jokiniemi K, Pietilä AM, Mikkonen S (2020) Construct validity of clinical nurse specialist core competency scale: an exploratory factor analysis. J Clin Nurs https://doi.org/10.1111/jocn.15587
Kilpatrick K, Tchouaket E, Carter N, Bryant-Lukosius D, DiCenso A (2016) Structural and process factors that influence clinical nurse specialist role implementation. Clin Nurse Spec 30:89–100
Kotila J, Axelin A, Fagerström L, Flinkman M, Heikkinen K, Jokiniemi K et al (2016) New roles for nurses—quality to future social welfare and health care services. Publication of the Finnish Nurses Association, Helsinki
Kotila J, Salonen A, Meretoja R (2018) Competence framework clarifies work roles. Pro Terveys. [Finnish]
Meretoja R, Vuorinen R (2000) Clinical nurse specialist in clinical practice. Sairaanhoitaja 73:24–25. [Finnish]
Meretoja R, Kaira A, Puualainen A, Santala I, Vuorinen R (2002) Asiantuntijasairaanhoitaja muutoksen tekijä kliinisessä hoitotyössä. Clinical nurse specialist: a change-maker in clinical nursing. Sairaanhoitaja 75:8–9. [Finnish]
Ministry of Social Affairs and Health, Finland Healthcare Professionals Act. No. 559/1994. [English]. http://www.finlex.fi/en/laki/kaannokset/1994/en19940559.pdf. Accessed 15 May 2018
Ministry of Social Affairs and Health, Finland. Health Care Act. No. 1326/2010. [English]. http://www.finlex.fi/en/laki/kaannokset/2010/en20101326.pdf. Accessed 15 May 2018
MSAH (2012) Koulutuksella osaamista asiakaskeskeisiin ja moniammatillisiin palveluihin. Ehdotukset hoitotyön toimintaohjelman pohjalta. Publications of the Ministry of Social Affairs and Health vol 7, pp 1–29. [Finnish] https://julkaisut.valtioneuvosto.fi/bitstream/handle/10024/71627/URN%3ANBN%3Afi-fe201504224497.pdf?sequence=1. Accessed 15 May 2018
Nurses’ Neuroscience Handbook. Publications of The Neuro Center. Helsinki University Hospital, Helsinki 2021
OECD.Stat (2018). http://stats.oecd.org/index.aspx?DataSetCode=HEALTH_STAT. Accessed 15 May 2018
Sheer B, Wong F (2008) The development of advanced nursing practice globally. J Nurs Scholarsh 40:204–211
Suominen T, Leino-Kilpi H (1995) More expertise to nursing. Sairaanhoitaja 68:35–36. [Finnish]
Viholainen K (2018) Nurses’ expertise in advanced practice nursing in specialised medical care. Master’s thesis, University of Eastern Finland. [Finnish]
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2021 Springer Nature Switzerland AG
About this chapter

Cite this chapter
Jokiniemi, K., Meretoja, R., Kotila, J. (2021). Clinical Nurse Specialist Role and Practice in Finland. In: Fulton, J.S., Holly, V.W. (eds) Clinical Nurse Specialist Role and Practice. Advanced Practice in Nursing. Springer, Cham. https://doi.org/10.1007/978-3-319-97103-2_9
Download citation
DOI: https://doi.org/10.1007/978-3-319-97103-2_9
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-97102-5
Online ISBN: 978-3-319-97103-2
eBook Packages: MedicineMedicine (R0)