
Abstract
Nurse practitioners in New Zealand are regulated as advanced practitioners who are fully authorized prescribers working independently or in collaborative teams. The NP role carries no requirements for oversight, supervision, protocols, enforced or formal collaboration nor limits to prescribing. In this regard, NPs have an enviable amount of freedom and autonomy to practice their craft. However, the growth of the NP workforce has been slow to materialize, with considerable variation in the establishment of their services across New Zealand. Over the years, nursing leadership has worked consistently and proactively to lobby for and progress the necessary changes in legislation that has enabled NPs to deliver services similar to those of a primary care or family physician and to receive equivalent government funding. Yet despite the ongoing shortage of physicians in the primary health and aged care sectors, the increasing prevalence of long-term conditions, and persisting health inequalities, NPs have not been recognized in policy as a solution. Through this chapter we describe the development of the NP workforce within the context of the health system in New Zealand, identifying current and future challenges.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
- Nurse practitioner
- Primary health care
- Primary care
- Health inequalities (or inequities)
- Advanced nursing
- Nursing leadership
1 Introduction
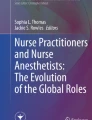
The first Nurse Practitioner (NP) was registered in New Zealand in 2001. By mid-2019, a total of 380 NPs had been registered with the Nursing Council of New Zealand, the regulatory authority responsible for the registration of nurses and NPs (Nursing Council of New Zealand n.d.-a) (see Fig. 11.1). Of these, just over half are thought to work in primary health care and community settings, including general practice (family/primary care practices), older adult care, palliative care, mental health, and sexual health. Other NPs work in hospitals (acute, rehabilitation, and long-term care), ambulatory settings, and in roles that help patients navigate between primary and secondary care services. Over the past two decades, considerable changes and clarification have been made to educational requirements, processes for registration, and legislation governing NP regulation and practice. Such changes have enabled a NP to work at a comparable level to a primary care physician as an authorized prescriber and access government funding to deliver mainstream primary care services to local populations. Within the hospital environment, NPs are generally considered to work at an equivalent level to registrars (a medically trained practitioner with at least 2 years postgraduate experience).

Growth of NPs in New Zealand. Data taken from annual reports provided by Nursing Council of New Zealand (Nursing Council of New Zealand n.d.-a)
New Zealand has a population approaching five million people and a land mass that approximates California or the United Kingdom. While the majority of the population are of European descent, 15% are Māori (the indigenous people of New Zealand), 7.5% Pacific, and 12% Asian. New Zealand, as in other countries, is facing a rising older population, increasing prevalence of long-term conditions, persisting health inequalities, all compounded by an over-stretched health service, a health workforce shortage, and increasing scarcity of primary care physicians (known as general practitioners in New Zealand). The opportunity for New Zealand to fully implement the NP role as mainstream, particularly in the primary health and community care sectors, has yet to be taken on board as a solution to current demographic, workforce, and health equity concerns (Carryer and Adams 2017; Adams and Carryer 2019).
In New Zealand, the development of advanced practice nursing, and more specifically that of the NP role, has been driven almost entirely by a small group of nurse leaders, pioneering clinical nurses, and academics who have worked from various angles over the last 20 years. Their work has been captured through a small number of doctoral theses (Jacobs 2005; Pirret 2013; Wilkinson 2007; Adams 2017) and other publications (Jacobs and Boddy 2008; Carryer and Yarwood 2015; Ministry of Health, Nursing Council of New Zealand, DHBNZ, NPAC-NZ 2009). More recently, given that we now have sufficient NPs for useful data collection, local research is emerging to add to the body of international literature (Carryer and Adams 2017; Adams and Carryer 2019; Carryer et al. 2011; Gagan et al. 2014; Pirret 2016; Pirret et al. 2015).
2 The Development of the NP Role in New Zealand
In 1998 in New Zealand, a Ministerial Taskforce on Nursing (Ministerial Taskforce on Nursing 1998) determined (amongst other recommendations, including nurse prescribing) that it was timely to develop an advanced practice nursing role, and agreed that this role would be the nurse practitioner. The strong union presence of the New Zealand Nurses Organisation (NZNO) initially objected to the need for masters-level education, arguing that clinical experience was an adequate prerequisite for advanced practice and specialist nursing roles. With nursing leadership provided through the College of Nurses Aotearoa (New Zealand), national consensus-making workshops were facilitated. Further, the NZNO consulted widely and in 2000 reversed its previous position, recommending the need for postgraduate education for advanced practice nursing roles. Clear agreement was ultimately reached within the nursing profession about the way forward for New Zealand NP development as outlined in a Ministry of Health publication (Hughes and Carryer 2002).
Perhaps most significantly, nursing leaders determined the title nurse practitioner would have a separate scope of regulated practice and the title would be endorsed by the national regulator, the Nursing Council of New Zealand. In order to protect the title prior to the enactment of the Health Practitioners Competence Assurance Act (Health Practitioners Competence Assurance Act 2003), the Nursing Council trademarked the term nurse practitioner in 2001. Importantly, these steps have not only enabled the Nursing Council’s legislative functions to protect public safety, by ensuring all NPs are competent and fit to practice, but also clarity has been given to the public, policy makers, and health professionals regarding the scope of the NP role. The first NP scope of practice was published in the New Zealand Gazette (the Government’s journal of constitutional record) in 2004. The scope was considerably revised in 2017 following extensive consultation, and particularly to include that NPs are authorized prescribers, and is shown in Box 11.1.
Box 11.1: Scope of Practice of NPs in New Zealand (2017) (Nursing Council of New Zealand n.d.-b)
Nurse practitioners have advanced education, clinical training, and the demonstrated competence and legal authority to practice beyond the level of a registered nurse. Nurse practitioners work autonomously and in collaborative teams with other health professionals to promote health, prevent disease, and improve access and population health outcomes for a specific patient group or community. Nurse practitioners manage episodes of care as the lead healthcare provider in partnership with health consumers and their families/whānau. Nurse practitioners combine advanced nursing knowledge and skills with diagnostic reasoning and therapeutic knowledge to provide patient-centered healthcare services including the diagnosis and management of health consumers with common and complex health conditions. They provide a wide range of assessment and treatment interventions, ordering and interpreting diagnostic and laboratory tests, prescribing medicines within their area of competence, and admitting and discharging from hospital and other healthcare services/settings. As clinical leaders they work across healthcare settings and influence health service delivery and the wider profession.
Nurse practitioners in New Zealand are required to be experienced registered nurses having completed a clinical master’s degree in nursing, and demonstrated the required advanced practice competencies (Nursing Council of New Zealand 2019) (see Box 11.2). Funding for postgraduate education is available on application through a workforce division of the Ministry of Health. At the outset of the NP project, nurse academics recognized that while the master’s degrees had a strong social science focus, the programs would need rapid development to include the core requirements of a clinical master’s degree to support advanced practice nursing. Programs were required to include pathophysiology, advanced assessment and diagnostics, pharmacology, and prescribing practice.
Box 11.2: Qualifications for NP in New Zealand
From: Nurse practitioner scope of practice: Guidelines for applicants (p. 4) (Nursing Council of New Zealand 2019)
-
(a)
be registered with the Nursing Council of New Zealand in the registered nurse scope of practice
-
(b)
complete an approved clinical master’s degree programme (or overseas equivalent) for the nurse practitioner scope of practice. The programme must include relevant theory and a minimum of 300 h of clinical learning
-
(c)
at least 4 years’ experience in an area of practice
-
(d)
pass an assessment against the nurse practitioner competencies, given by a Council-approved assessor
When the NP role was launched in New Zealand in 2001, the intention was that NPs would address broad population groups rather than specific disease categories or locations of practice. Possibly due to the reservoir of experienced senior clinical nurses and the clinical nurse specialist roles in discrete areas of practice, early NP candidates tended to be located more frequently in specialized or disease-specific areas, such as neonatology, gerontology, and diabetes. For primary health care, specific postgraduate programs provided the leverage for nurses to progress through their postgraduate education to a master’s degree, such as the rural nurse specialist diploma in the South Island, while other healthcare initiatives targeting areas, such as health inequalities and long-term conditions, prompted tertiary education institutes to develop specific postgraduate programs. The result was a range of different tertiary institution providers delivering a myriad of diverse courses leading to a clinical master’s in nursing.
Over the years, the variety of papers available within master’s programs has reduced while retaining the required 240 credits. The consequence has been that while the biomedical components of the programs have strengthened, the focus on population health, social justice, ethics, and other more nuanced subjects has perhaps diminished. The challenge is going to be how New Zealand ensures that the NP role continues to bridge the biomedical-nursing paradigm.
The Nursing Council of New Zealand has recently reaffirmed the commitment to ensuring that a NP is able to provide a broad spectrum of care. Since 2017, NPs are no longer restricted by a condition stating a specific area of practice, but as advanced practitioners are “trusted” to practice within their areas of competence and experience (Nursing Council of New Zealand n.d.-b). Such broad areas of practice include mental health, primary health, elder care, or care of children and young people. The educational preparation addresses the breadth of requirement by providing students with the framework for advanced nursing practice, which can then be applied to the context of their proposed advanced practice setting or specialty. Because New Zealand is a small country with limited population densities in any one city, NP education has been shared jointly in a clinical master’s program with students who may not be intending to seek authorization as a NP. The NP candidate is differentiated by completion of the 1 year supervised (academic and clinical) practicum as a component of the master’s degree to meet the required NP competencies, including prescribing practice (Nursing Council of New Zealand n.d.-c). The key NP competency themes, revised in 2017 (shown in Box 11.3), are further divided into multiple indicators. Clinical practice experience is supervised and completed in the employment situation. Concern with completion of specified hours of practice has not been a feature of the pathway in New Zealand. Hours have been addressed by requiring those entering the program to have at least 3 years prior nursing experience, the usual period of completing the degree, which is generally 4 years, at least, and the ability to demonstrate achievement of the competencies upon application.
Box 11.3: Themes Under Which NP Competence Is Assessed in New Zealand
From: Competencies for the nurse practitioner scope of practice (Nursing Council of New Zealand n.d.-c) (p. 1)
-
1.
Provides safe and accountable advanced practice
-
2.
Assesses, diagnoses, plans, implements and evaluates care
-
3.
Works in partnership with health consumers
-
4.
Works collaboratively with healthcare teams
-
5.
Works to improve the quality and outcomes of healthcare
A recent change has occurred in New Zealand with the commencement of government funded programs in two universities. These programs require the candidate to have completed at least half of the master’s degree upon entry, to have employer agreement that they have a NP position upon successful completion and will complete two specific practicums requiring 500 hours of clinical practice. After completion of the clinical master’s degree, applicants for NP authorization compile a portfolio demonstrating how they meet the NP competencies. Nursing Council conducts a desk audit of this document and, if the portfolio is satisfactory, the applicant progresses to attending an oral viva with an assessment panel. After this process, NP authorization may be conferred.
3 Challenges in the New Zealand Health Sector
A prolonged and interesting tension has occurred between the stated policy intentions of the New Zealand Government (Hughes and Carryer 2002) and the actual willingness to implement the NP workforce. Nurse leaders have had to work consistently and strategically to circumvent layers of obstruction and inactivity in order to progress the role. We will discuss several possible reasons for the very slow progress.
New Zealand has a hybridized health system with free hospital care but both primary health care and aged residential care are run under a private business model, albeit with heavy government subsidization and a requirement for patient co-payment. Theoretically, no one in the country should have limited or no access to care and services. However, New Zealand has many rural and demographically isolated areas and many small towns with low population numbers. The country has significant child poverty, homelessness, and high levels of health disparities between the most well off and those on low incomes or welfare benefits. Māori, our indigenous population, are disproportionately represented amongst the most vulnerable (Ministry of Health 2015) and the need to achieve equity remains a major challenge. Downes (2017) reported that 30% of New Zealanders are not able to access timely primary care (Downs 2017). Despite the rhetoric, a great many people in New Zealand have unmet needs who would be well served by a large workforce of NPs (Carryer and Adams 2017).
Since the Ministerial Taskforce on Nursing in 1998 (Ministerial Taskforce on Nursing 1998), it has become even more evident that a different approach to service delivery is urgently required. From the Ministry of Health to the front line we now recognize that old ways of doing things and a reliance on the traditional workforce configurations designed to meet acute biomedical care will not address unmet needs. Internationally, the WHO (2008) and others have called for redesigned health systems to transform the primary care workforce and delivery models with nursing central to such changes (Commission on Social Determinants of Health 2008; Bodenheimer and Bauer 2016; Pittman 2019; All-Party Parliamentary Group on Global Health 2016). However, despite various governmental strategies, discernible change for service users has been slow to materialize.
At the policy level Ministry officials have made frequent high-level calls for innovative disruption (Christensen et al. 2015), suggesting that the health sector is ready and willing to change from traditional medical models of service delivery. Multiple health strategies and action plans have been written and published by the Ministry of Health (Ministry of Health n.d.) with similar themes, including for primary health care, Māori, healthy ageing, suicide prevention, alcohol misuse, gambling, palliative care, and cancer control. These themes include calling for attention to health disparities, improving preventative care, managing the tide of long-term conditions more effectively, and increasing the use of the whole workforce at the top level of their license potential. The extent to which these strategies have ever been implemented is questionable, as while the vision has been exemplary, the operational structures or policy settings have not supported or facilitated the desired change and have certainly not supported any notion of significant disruption (Robertson et al. 2015).
One example has been the implementation of The Primary Health Care Strategy (Ministry of Health 2001), launched in 2001, which resulted in major structural changes to the sector. The strategy promised a population health approach to improve access to comprehensive primary healthcare services and remove health inequalities. Substantially increased government funding, in the form of capitation payments, meant in effect that services were purchased in advance on behalf of patients with the expectation that the service would be delivered by the best person to do so. This move was intended to increase the use of the wider multidisciplinary team and was seen as a way of validating the work done by nurses in such settings. The need for advanced practice nurses with a clearly defined career pathway, appropriate education, and improved employment arrangements was considered central to the success of the strategy. However, it quickly became apparent that medical practitioners, as practice owners, tended to regard the capitated funding as their direct income, or at least income over which they had jurisdiction. In reality, the transformational changes that had been anticipated through the strategy were not realized (Cumming 2016; Finlayson et al. 2012) and physician-led care has prevailed.
Through her doctoral research, Adams (Carryer and Adams 2017; Adams and Carryer 2019; Adams 2017) critically examined the establishment of NPs in rural New Zealand using institutional ethnography. Underpinned by a nursing paradigm that promotes social justice and health equity, the research explicated how both the neoliberal health policy environment and medical hegemony maintained the status quo, limiting the establishment of the rural NP workforce. Service fragmentation, a competitive and changeable funding environment with rapid turnover of contracts, and the ongoing policy support of small business models of general practice hampered the opportunity for health providers to invest in the NP workforce. Further, while the shortage of rural primary care physicians was considered critical, there was little willingness at all levels of the health sector to actively support and promote NPs as a solution. The rhetoric, presented through the national media, centered on schemes to recruit and retain physicians. However, despite such an adverse environment, years of sheer determination by nurse leaders together with extraordinary pioneering NPs has resulted in a growing number of NPs establishing service delivery.
4 Nursing Leadership and Ongoing NP Role Development
From the outset, nursing in New Zealand, under focused leadership, agreed with and aimed to support the vision behind the various strategies and policies. The commitment to the NP project has been supported by international evidence demonstrating the health outcomes achieved by NPs and their cost-effectiveness (Laurant et al. 2018; Swan et al. 2015; Martínez-González et al. 2014). Further, the nursing profession supported by the Nursing Council of New Zealand has acknowledged the contribution NPs can make to the health of New Zealanders.
The impetus towards the NP role in New Zealand has never been about a substitute for medical services but a serious attempt to reframe or transform the processes of service delivery. Kooienga and Carryer (Kooienga and Carryer 2015) have previously argued that:
After 100 years of health services framed by the culture of medicine, most countries report an epidemic of chronic disease, a resurgence of infectious diseases related to poverty, huge inequalities in access and outcomes, major expenditures occurring in the last year of life, and often insufficient investment in child and youth health. (p. 806)
However, it appears that medical hegemony remains strong at both overt and covert levels. While the rhetoric of reducing the burden of long-term conditions and health inequalities are evidenced in, for example the New Zealand Health Strategy 2016 (Ministry of Health 2016), even health bureaucrats are unconsciously invested in the maintenance of medicine as the default leadership position and the default solution to service gaps. Initial resistance by the medical profession to the development of the role was inevitable, challenging, and persistent, but is perhaps at last declining. Now many primary care physicians who work with NPs have recognized their contribution and value to the health of their communities.
Since the role was first mooted, we have participated in a steady process of eliminating barriers to practice through lobbying for and achieving legislative change. Changes to the Medicines Act (Medicines Amendment Act 2013), enacted in 2014, saw NPs achieve the status of authorized prescriber, the same level of prescribing autonomy as held by medical practitioners. A few years later, the Health Practitioners Statutory References Bill (Health Practitioners 2015) removed references to medical practitioner from eight separate pieces of legislation and changed the wording to either health practitioner or added NP alongside medical practitioner. These changes have freed up NPs to sign death and cremation certificates, sign “off work” certificates, and various other procedures. Other challenges have included securing the right for NPs to prescribe special authority medications, controlled drugs, and to write standing orders for other practitioners. All has been achieved, at this point, with one exception—that an NP cannot yet order ultra-sound for the first trimester of pregnancy prior to the woman’s care being passed directly to a lead maternity care provider, most usually a midwife. Changing this barrier requires attention to the Public Health and Disability Act (New Zealand Public Health and Disability Act 2000), section 88.
At the same time a steady process of successful policy challenge has occurred as NPs are now able to claim for first specialist assessments in hospitals, carry out required regular assessments and treatment plans in residential care facilities, and to claim the same government funding streams as general practitioners (primary care physicians) working in community settings and primary care practices. At this point all other funding streams are accessible by an NP with the minor exception of the Accident Compensation CommissionFootnote 1 which persists (despite lobbying) in paying a NP a different amount than a GP for delivering exactly the same service to a patient. These changes have created a platform for the viability of the role as a valuable addition to the New Zealand workforce. However, many challenges remain, which are proving more difficult to overcome.
While many barriers were concrete and amenable to legislative or policy change, other barriers relate more to persistent custom and practice and levels of ignorance amongst managers or medical leaders. One example, which captures this phenomenon, has been resistance to a NPs right to order radiology tests. Despite clear documentation that NPs are legally able to order radiology tests, we have seen repeated examples of service managers or radiologists professing their certainty that this cannot happen. In such circumstances, patients’ care is held up or even compromised. Additionally, certain specialist medical practitioners have also professed reluctance to accept referrals from NPs. In one instance, the specialist noted that while this was the most comprehensive referral letter ever received, it would not be accepted. Such behavior, while not legitimate, requires firm challenge especially if patients are not to suffer through delayed care.
New Zealand nurse leaders are proud to have resisted the process of medical appeasement and can note that the role in New Zealand carries no requirement for oversight, supervision, protocols, enforced or formal collaboration nor limits to prescribing. Nurse practitioners in New Zealand have an enviable amount of freedom and autonomy to practice their craft without impediment and frustration created by supervisory relationships.
The uptake of the NP role in New Zealand thus proceeded initially at a glacial pace with considerable wastage of investment and energy. The momentum is now gathering considerable speed. According to Ministry of Health workforce data in 2019, in addition to NPs, a further 2000 registered nurses hold a master’s degree and are potentially eligible to apply for an NP role. This represents a considerable potential resource for addressing health deficits and general practitioner shortages.
Media accounts are released almost daily, which report the rapid decline in availability of primary health physicians for many New Zealanders (Royal New Zealand College of General Practitioners 2019). The NP role alongside RNs working to the top of their scope stands poised to provide the exact new or “disruptive” model of service for which frequent calls are made. A persistent challenge over the years has been to encourage the media to take up the positive news about the growth of NPs and their potential. Instead, the media have focused on the crisis of the shortage of primary care physicians, perpetually seeking solutions that maintain a sector dominated by medicine.
In 2019, with a major review of the health system under way, it is clear that primary care physicians are determined to protect their private business model, despite significant reports of its flaws and the lack of attention to the needs of the most vulnerable (Downs 2017). A national patient care survey was launched by the Health Quality Safety Commission New Zealand (Health Quality and Safety Commission New Zealand 2019). In a most subtle form of resistance or ignorance, NPs were omitted as an option that respondents could select to identify as their provider. This occurred despite the fact that a fairly significant number of people are now enrolled with an NP as their primary provider. Nursing leadership challenges to this omission were not successful during the drafting of the survey.
In New Zealand, we are seemingly producing a health workforce of NPs who are small in numbers, largely because of the barriers (mostly now imagined), conflicts, and vested interests associated with a partly private and partly publicly funded system of service delivery for primary care services. The net result is that the focus of health service development and investment has remained very much on primary care as the narrow response to presenting acute problems rather than the intended focus on the broader and much needed concept of primary health care. This continued focus on first contact medical care is at the expense of appropriate care for children in the first 1000 days of life, attention to the growing mental distress of young people, the vast numbers of people living with complex comorbidities, an ageing population, and the health inequalities facing indigenous and other deprived and vulnerable communities.
Nursing leadership in NZ has been advancing the NP role in the belief that there is genuine impetus for change. Despite the fact that an NP is now (and has been for many years) a fully viable income generating member of a general practice team, the myth is still widely promulgated that general practice cannot afford to employ NPs. This development is frustrating and can only be addressed by time and attempts to publicize the facts. We have hope in many practices where NPs are working successfully and collegially alongside medical colleagues. Nursing is also optimistic that as the focus on the lack of equity for much of the NZ population intensifies then greater attention will be provided to NPs as a solution.
5 Social Justice and Health Inequalities
Māori, the indigenous people of New Zealand, experience significant health inequalities. Socio-economic determinants and low health literacy relate to poorer health outcomes for life expectancy and morbidity across the life span, including long-term conditions, cancers, oral health and rheumatic fever; and smoking prevalence, obesity, alcohol and drug use, gambling, suicide rates, and family violence remain unacceptably high (Ministry of Health 2015; Marriott and Sim 2014). New Zealand is a bicultural nation based upon its founding document, the Treaty of Waitangi, yet despite the principles of the Treaty being incorporated into health service policy in the late 1980s, institutional racism persists (Came 2014). The reductionist biomedical western models of health care that predominate do not meet the needs of Māori and require alternative, culturally appropriate models (Came 2014; Sheridan et al. 2011; Durie 1998).
New Zealand NPs in primary health care work within a social justice paradigm, embracing principles to promote health and well-being, and reduce health inequalities for individuals, families, and communities (Carryer and Yarwood 2015; Browne and Tarlier 2008). One of the nursing professions’ key strengths in New Zealand has been the adoption of Irihapeti Ramsden’s (Ramsden 2015) work on cultural safety. This has manifested in the development of an educational framework to analyze the power relationships between health professionals and those with whom they work, particularly Māori. Striving for an approach that understands and accommodates cultural difference is a key component of all nursing education and a required competency for nursing practice.
A number of the extant NPs in New Zealand have established their work in rural and Māori communities, in precisely the locations necessary to achieve the international and national goals of the Primary Health Care Strategy (Ministry of Health 2001; World Health Organization 2018). Through our qualitative research (Carryer and Adams 2017; Adams and Carryer 2019), we have learned that NPs are passionate about the health of their communities and work in ways that demonstrate their commitment to improving health and well-being. Such NPs have worked to reshape health services and inform policy direction. They model how to work across organizational and policy boundaries, focusing on the social, cultural, and political contexts in which people live and work (Adams and Carryer 2019).
6 Future Hopes and Challenges
A new phenomenon occurring in the last year or two is a rapid increase in the number of advertisements for NP positions especially in general practice or community settings and to a lesser extent in palliative and aged care. Advertising for an NP at this early stage assumes that there are many NPs actively job searching which is not the case. Rather we have advocated for a “grow your own” approach as it is far more successful for such settings to identify their RNs who are on the pathway to holding a clinical master’s degree and formally recognize them as NP candidates with a future position available. Registered nurses are the only health workforce well distributed across NZ and as such, they are a resource worthy of investment towards advanced practice. In this case, a small investment will pay quick dividends in meeting unmet need.
The strength of the NP role, as it was anticipated, was to provide patients with access to nursing care in the course of consultation and management of presenting problems. Such work, if done properly, takes time and is challenged by the tyranny of the acute and the time pressures, which characterize general practice and many other settings especially when driven by a profit agenda.
Our next challenge is now becoming clear as primary healthcare NPs especially find themselves under pressure to work faster and see patients in short appointment times in order to secure profit for business owners. This contrasts strongly with their desired focus on the social determinants of health, their awareness of equity issues, and the value of improving health literacy and health education. As previously noted, the entire health system in New Zealand is the subject of a government commissioned major review process. Nurse leaders need to clearly articulate the value of NPs as a role with a strong primary health care and social justice focus (Browne and Tarlier 2008). To this end there is growing global support.
The World Health Organization (WHO) has long recognized that a new model of healthcare delivery is required to meet the current global health crisis (Commission on Social Determinants of Health 2008). In New Zealand, we have determined that NPs offer the exact transformation in care that the WHO seeks. As we have previously argued (Carryer and Adams 2017), NPs can only deliver the full transformative potential of the role if the nature of their employment facilitates rather than limits their practice. We argue that the impetus of NPs towards transformative care must not be inhibited by funding patterns or management decisions, which continue to suggest medical solutions to health problems arising from lack of equity, lack of access, and lifestyles constrained by homelessness, poverty, and poor nutrition.
In order to support this perspective, we challenge the international impetus to continue conducting research demonstrating direct comparisons or equivalence between nurse practitioners (NP) and physicians or physician-led care in terms of outcomes. This work has been done and done well and the findings are unequivocal (Laurant et al. 2018; Swan et al. 2015; Martínez-González et al. 2014). Such research however strengthens a world view that the NP role is a substitutive role rather than one of promoting service transformation. More importantly, the future research focus could be on demonstrating how NPs, when given the freedom and autonomy and appropriate employment settings, can provide a type of care which spans medicine and nursing and health and offers a qualitatively different but much needed type of care. Capturing short and long-term outcomes of transformative care by NPs is vitally important if models of care are to be genuinely redesigned.
The establishment of the NP role in New Zealand has been a 20-year journey, which is finally gaining real impetus. Nursing leadership activity has been persistent and courageous in combatting both visible and covert barriers to the role establishment. Perhaps we have too often naively assumed that the high levels of unmet need should be sufficient to ensure receptivity, but it has not been so. Health is a business, first and foremost, even in this country of largely free health care, and the powerful historical acceptance of medical leadership continues to shape the debate.
Notes
- 1.
The Accident Compensation Corporation (ACC) is New Zealand’s universal no-fault scheme for work and non-work injuries. The scheme provides contributions to treatment costs, loss of earnings, return to work schemes, and home and vehicle modifications.
References
Adams S. Nurse practitioners in rural primary health care in New Zealand: an institutional ethnography. PhD thesis. New Zealand: Massey University; 2017. https://mro.massey.ac.nz/handle/10179/12816. Accessed 1 July 2019.
Adams S, Carryer J. Establishing the nurse practitioner workforce in rural New Zealand: barriers and facilitators. J Prim Health Care. 2019;11(2):8–14. https://doi.org/10.1071/HC18089.
All-Party Parliamentary Group on Global Health. Triple Impact - how developing nursing will improve health, promote gender equality and support economic growth. London: All-Party Parliamentary Group on Global Health; 2016.
Bodenheimer T, Bauer L. Rethinking the primary care workforce-an expanded role for nurses. N Engl J Med. 2016;375(11):1015–7. https://doi.org/10.1056/NEJMp1606869.
Browne AJ, Tarlier DS. Examining the potential of nurse practitioners from a critical social justice perspective. Nurs Inq. 2008;15(2):83–93. https://doi.org/10.1111/j.1440-1800.2008.00411.x.
Came H. Sites of institutional racism in public health policy making in New Zealand. Soc Sci Med. 2014;106:214–20. https://doi.org/10.1016/j.socscimed.2014.01.055.
Carryer J, Adams S. Nurse practitioners as a solution to transformative and sustainable health services in primary health care: a qualitative exploratory study. Collegian. 2017;24(6):525–31. https://doi.org/10.1016/j.colegn.2016.12.001.
Carryer J, Yarwood J. The nurse practitioner role: solution or servant in improving primary health care service delivery. Collegian. 2015;22(2):169–74. https://doi.org/10.1016/j.colegn.2015.02.004.
Carryer J, Boddy J, Budge C. Rural nurse to nurse practitioner: an ad hoc process. J Prim Health Care. 2011;3(1):23–8. https://doi.org/10.1071/HC11023.
Christensen CM, Raynor ME, McDonald R. What is disruptive innovation? Harv Bus Rev. 2015;93(12):44–53.
Commission on Social Determinants of Health. Closing the gap in a generation: health equity through action on the social determinants of health. Geneva: World Health Organization; 2008. http://www.who.int/social_determinants/thecommission/finalreport/en/. Accessed 5 June 2019.
Cumming J. Commissioning in New Zealand: learning from the past and present. Aus J Prim Health. 2016;22(1):34–9. https://doi.org/10.1071/PY15164.
Downs A. From theory to practice: the promise of primary care in New Zealand Fulbright New Zealand; 2017. https://www.fulbright.org.nz/wp-content/uploads/2017/09/DOWNS-From-Theory-to-Practice-The-Promise-of-Primary-Care-in-New-Zealand-.pdf. Accessed 1 July 2019.
Durie M. Whaiora: Māori health development. Oxford: Oxford University Press; 1998.
Finlayson M, Sheridan N, Cumming J, Fowler S. The impact of funding changes on the implementation of primary health care policy. Prim Health Care Res Dev. 2012;13(2):120–9. https://doi.org/10.1017/S1463423611000363.
Gagan MJ, Boyd M, Wysocki K, Williams DJ. The first decade of nurse practitioners in New Zealand: a survey of an evolving practice. J Am Assoc Nurse Pract. 2014;26(2014):612–9. https://doi.org/10.1002/2327-6924.12166.
Health Practitioners (Replacement of Statutory References to Medical Practitioners) Bill. New Zealand Government; 2015. http://www.legislation.govt.nz/bill/government/2015/0036/23.0/versions.aspx. Accessed 1 July 2019.
Health Practitioners Competence Assurance Act. New Zealand Government; 2003. http://www.legislation.govt.nz/act/public/2003/0048/latest/DLM203312.html?src=qs.Accessed 12 June 2019.
Health Quality & Safety Commission New Zealand. Patient experience. 2019. https://www.hqsc.govt.nz/our-programmes/health-quality-evaluation/projects/patient-experience/. Accessed 3 July 2019.
Hughes F, Carryer J. Nurse practitioners in New Zealand. Wellington: Ministry of Health; 2002.
Jacobs S. Advanced nursing practice and the nurse practitioner: New Zealand nursing’s professional project in the late 20th century. PhD thesis. New Zealand: Massey University; 2005. http://mro.massey.ac.nz/handle/10179/1553. Accessed 1 July 2019.
Jacobs S, Boddy J. The genesis of advanced nursing practice in New Zealand: policy, politics and education. Nurs Prax NZ. 2008;24(1):11–22.
Kooienga SA, Carryer J. Globalization and advancing primary health care nurse practitioner practice. J Nurse Pract. 2015;11(8):804–11. https://doi.org/10.1016/j.nurpra.2015.06.012.
Laurant M, van der Biezen M, Wijers N, Watananirun K, Kontopantelis E, van Vught A. Nurses as substitutes for doctors in primary care (review). Cochrane Database Syst Rev. 2018; https://doi.org/10.1002/14651858.CD001271.pub3. Accessed 3 July 2019.
Marriott L, Sim D. Indicators of inequality for Māori and Pacific People. Working Paper 09/2014. Wellington: Victoria University of Wellington; 2014. http://www.victoria.ac.nz/sacl/centres-and-institutes/cpf/publications/pdfs/2015/WP09_2014_Indicators-of-Inequality.pdf. Accessed 5 June 2019.
Martínez-González NA, Djalali S, Tandjung R, Huber-Geismann F, Markun S, Wensing M, et al. Substitution of physicians by nurses in primary care: a systematic review and meta-analysis. BMC Health Serv Res. 2014;14:214. https://doi.org/10.1186/1472-6963-14-214.
Medicines Amendment Act. Wellington: New Zealand Government; 2013. http://www.legislation.govt.nz/act/public/2013/0141/latest/DLM4096106.html. Accessed 25 June 2019.
Ministerial Taskforce on Nursing. Report of the Ministerial Taskforce on Nursing: releasing the potential of nursing. Wellington: Ministry of Health; 1998.
Ministry of Health. The primary health care strategy. Wellington: Ministry of Health; 2001.
Ministry of Health. Tatau kahukura: Māori health chart book 2015. 3rd ed. Wellington: Ministry of Health; 2015.
Ministry of Health. New Zealand Health Strategy: future direction. Wellington: Ministry of Health; 2016.
Ministry of Health. Publications. [n.d.]. https://www.health.govt.nz/publications. Accessed 3 July 2019.
Ministry of Health, Nursing Council of New Zealand, DHBNZ, NPAC-NZ. Nurse Practitioners: a healthy future for New Zealand. Wellington: Ministry of Health; 2009. https://www.health.govt.nz/system/files/documents/publications/nurse-practitioners-a-healthy-future-for-nz.pdf. Accessed 12 June 2019.
New Zealand Public Health and Disability Act. New Zealand Government; 2000. http://www.legislation.govt.nz/act/public/2000/0091/latest/DLM80051.html?search=ts_act%40bill%40regulation%40deemedreg_health+and+disability_resel_25_a&p=1. Accessed 25 June 2019.
Nursing Council of New Zealand. Nurse practitioner scope of practice: guidelines for applicants. Wellington: Nursing Council of New Zealand; 2019.
Nursing Council of New Zealand. Reports and worforce statistics. [n.d.-a]. http://www.nursingcouncil.org.nz/Publications/Reports-and-workforce-statistics. Accessed 3 July 2019.
Nursing Council of New Zealand. Nurse practitioner. [n.d.-b]. http://www.nursingcouncil.org.nz/Nurses/Scopes-of-practice/Nurse-practitioner. Accessed 12 June 2019.
Nursing Council of New Zealand. Competencies for the nurse practitioner scope of practice. Wellington: Nursing Council of New Zealand; [n.d.-c]. http://www.nursingcouncil.org.nz/Education/Nurse-practitioner. Accessed 3 July 2019.
Pirret AM. Nurse practitioner diagnostic reasoning. PhD thesis. New Zealand: Massey University; 2013. http://mro.massey.ac.nz/handle/10179/4929. Accessed 1 July 2019.
Pirret AM. Nurse practitioners’ versus physicians’ diagnostic reasoning style and use of maxims: a comparative study. J Nurse Pract. 2016;12(6):381–9. https://doi.org/10.1016/j.nurpra.2016.02.006.
Pirret AM, Neville SJ, La Grow SJ. Nurse practitioners versus doctors diagnostic reasoning in a complex case presentation to an acute tertiary hospital: a comparative study. Int J Nurs Stud. 2015;52(3):716–26. https://doi.org/10.1016/j.ijnurstu.2014.08.009.
Pittman P. Activating nursing to address unmet needs in the 21st century. Princeton: Robert Wood Johnson Foundation; 2019.
Ramsden I. Towards cultural safety. In: Wepa D, editor. Cultural safety in Aotearoa New Zealand. 2nd ed. Port Melbourne: Cambridge University Press; 2015.
Robertson H, Carryer J, Neville S. Diffusion of the Primary Health Care Strategy in a small district health board in New Zealand. Nurs Prax NZ. 2015;31(3):17–26.
Royal New Zealand College of General Practitioners. 2018 general practice workforce survey: part 1. Wellington: Royal New Zealand College of General Practitioners; 2019.
Sheridan N, Kenealy T, Connolly M, Mahony F, Barber P, Boyd MA, et al. Health equity in the New Zealand health care system: a national survey. Int J Equity Health. 2011;10(45):1–14. https://doi.org/10.1186/1475-9276-10-45.
Swan M, Ferguson S, Chang A, Larson E, Smaldone A. Quality of primary care by advanced practice nurses: a systematic review. International J Qual Health Care. 2015;27(5):396–404. https://doi.org/10.1093/intqhc/mzv054.
Wilkinson J. The New Zealand nurse practitioner polemic: a discourse analysis. PhD thesis. New Zealand: Massey University; 2007. http://mro.massey.ac.nz/handle/10179/533. Accessed 1 July 2019.
World Health Organization. Declaration of Astana: global conference on primary health care 2018. https://www.who.int/docs/default-source/primary-health/declaration/gcphc-declaration.pdf. Accessed 3 July 2019.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2020 Springer Nature Switzerland AG
About this chapter

Cite this chapter
Carryer, J., Adams, S. (2020). Advanced Practice Nursing in New Zealand. In: Hassmiller, S.B., Pulcini, J. (eds) Advanced Practice Nursing Leadership: A Global Perspective. Advanced Practice in Nursing. Springer, Cham. https://doi.org/10.1007/978-3-030-20550-8_11
Download citation
DOI: https://doi.org/10.1007/978-3-030-20550-8_11
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-030-20549-2
Online ISBN: 978-3-030-20550-8
eBook Packages: MedicineMedicine (R0)