
Abstract
The cancer epidemic causes more deaths in developing countries than the more hyped HIV, malaria, and TB combined. Sub-Saharan Africa has the highest prevalence of cancer in developing countries, and the most prevalent type of cancer is the cancer of the cervix, with 57,381 deaths yearly. Many medical scholars agree that the high death rate from the cervical cancer scourge is preventable with effective cervical cancer control strategies such as appropriate prevention strategies in the form of awareness campaigns, effective screening for early diagnosis, and treatment programs. There have been numerous calls for measures that can improve prevention, early detection, and treatment of cervical cancer among women in Sub-Saharan Africa, and numerous approaches have so far been piloted. This paper presents an analysis of the potential of social media technologies to effectively support prevention, early detection, and treatment of cervical cancer in Sub-Saharan Africa.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


1 Introduction
For the last 10 years, communicable diseases such as Ebola Virus Disease (EVD), malaria, and HIV/AIDS have been the major challenge to the health sector in many Sub-Saharan African countries [1]. Over 70 percent (about 24.7 million) of people living with HIV in the world are from Sub-Saharan Africa (SSA), with about 1.5 million new HIV infections, and 1.1 million AIDS-related deaths every year [2]. Furthermore, close to 90 percent of the yearly Malaria cases in the world are from Sub-Saharan Africa [3]. The outbreaks of deadly virus causing epidemics are a common phenomenon in Sub-Saharan Africa. For example, the 2014 outbreak of the EVD epidemic in the three West African countries, Guinea, Liberia, and Sierra Leone, was the deadliest and the most complex and challenging Ebola outbreak in recent history, which claimed 11,315 lives from about 27,000 infected and suspected cases [3,4,5]. Yet again, Sub-Saharan Africa continues to battle with frequent occurrences of other viral hemorrhagic fevers (VHF), such as Yellow Fever, Marburg Virus, Rift Valley Fever, or Congo-Crimean Hemorrhagic Fever Virus, and others [6].
The high prevalence of communicable diseases in Sub-Saharan Africa often highlights popular and repeated narratives in global health summits and conferences. However, whereas common knowledge within the global health fraternity constantly places communicable diseases such as Ebola, malaria, and HIV/AIDS at the forefront of raising money and supports efforts in both national and international settings, a disease that is yet to gain considerable attention for global health funding and advocacy is the cancer epidemic in Sub-Saharan Africa [1]. The cancer epidemic is not yet considered by many as a significant challenge in low-resource settings like Sub-Saharan Africa and needs urgent attention [1]. However, recent statistics have shown that this disease is swiftly becoming the next overwhelming hurdle, particularly for the under-resourced regions in the world. The cancer epidemic causes more mortalities and morbidities in developing countries than the more hyped HIV, malaria, and TB combined [1, 7]. Over 50 percent of all the new cancer cases worldwide are from developing countries [7]. Estimates from the International Agency for Research on Cancer (IARC) show that about 14.1 million new cancer cases were registered worldwide in 2012, and developing countries, inhabited by about 82 percent of global population, accounted for close to 60 percent (8 million) of these new diagnoses [8, 9]. Furthermore, out of the 236,000 women, who died from cervical cancer worldwide in 2013, about 90 percent of these women were in developing countries [10]. This shows that cancer is an emerging pandemic in developing countries and needs urgent attention. The next section discusses the state of cancer in the Sub-Saharan region.
2 Cancer in Sub-Saharan Africa (SSA)
Sub-Saharan Africa is the most hit region with the cancer epidemic in the developing world [11]. Studies have established that breast and cervical cancer in women and prostate cancer in men are the main causes of cancer deaths in Sub-Saharan Africa [9]. However, the most prevalent cancer in Sub-Saharan Africa is cancer of the cervix, or neck of the uterus, with 57,381 deaths, followed by breast cancer with 47,583 deaths, and then prostate cancer with 47,583 deaths as shown in Table 10.1.
Cervical cancer affects approximately 12 percent of the women population in the region. In 2013, 39 out of 48 countries, classified as part of the Sub-Saharan African region, identified cervical cancer as the most common cause of cancer-related death in women [9, 10]. Within the Sub-Saharan region, the Eastern Africa region, in particular, has the world’s highest occurrence and death rates for cervical cancer [11, 13]. The Eastern African countries, Zambia, Malawi, Mozambique, and Tanzania, have among the highest cervical cancer rates (50 cases per 100,000) worldwide [9]. Table 10.2 summarizes the incidence and mortality rate per 100,000 in Africa.
As seen in Table 10.2, the incidence and mortality rates are the highest in Eastern Africa compared to West, South, and Central Africa. Many scientists have associated the high prevalence of cervical cancer in the Eastern Africa region to a matching high prevalence of HIV/AIDS rates. HIV rates among women in Eastern Africa accounts for more than 50 percent of the total HIV infections in the region, and this has been reported to exacerbate the high prevalence of cervical cancer [2, 14]. There have been several other studies that have linked HIV infection and cervical cancer among women in Sub-Saharan Africa such as Bateman et al. [15] and Parham et al. [16]. As a result, cancer of the cervix is turning out to be an emerging major challenge for the health sector in Sub-Saharan Africa. Besides linking HIV to the high prevalence of cervical cancer in the region, the increased prevalence of cervical cancer has also been associated with the following factors: the ever-growing and aging population, increased prevalence of human papilloma virus and hepatitis B virus, as well as increased prevalence of key risk factors—including those associated with social and economic transition [9]. Despite the high prevalence of cervical cancer in Sub-Saharan Africa, the region seems to have inadequate capacity to curb the cervical cancer scourge as discussed in the next section.
3 The Challenges of Controlling Cervical Cancer in Sub-Saharan Africa
The huge cancer burden coupled with the weak health systems incapable of handling the disease burden has greatly aggravated the cervical cancer pandemic in Sub-Saharan Africa. Many women diagnosed with cervical cancer are incapable of accessing comprehensive cancer care simply because of poor cervical cancer control strategies [11]. Poor cervical cancer control strategies have led to very high incidence rates per 100,000. For example, the age-specific incidence rate per 100,000 in Malawi-75.9, Mozambique-65.0, Comoros-61.3, Zambia-58.0, Zimbabwe-56.4, Tanzania-54.0, Swaziland-53.1, and Burundi-49.3 [17]. This, therefore, represents a massive failure in Sub-Saharan African countries to implement a functional cervical cancer control strategy [1, 10]. Data from global cancer incidence, mortality, and prevalence (GLOBOCAN portal) warn that if preventive actions are not taken, the problem of cervical cancer in Eastern and Southern Africa regions will only get worse in the years ahead [15]. Many medical scholars agree that the high death rate from the cervical cancer scourge is preventable with effective cervical cancer control strategies, which include prevention in the form of appropriate awareness campaigns, effective screening for early diagnosis, and treatment programs [18, 19]. However, these three major cervical cancer control strategies are extremely inadequate in Sub-Saharan Africa as discussed in the next section.
3.1 Prevention (Awareness Campaign)
Whereas 90 percent of the world’s cervical cancer deaths occur in Sub-Saharan African, cervical cancer is the most preventable of all the three most common types of cancers in the region [15]. As discussed earlier, a lot of urgency is usually given to communicable diseases such as Ebola, HIV, malaria, and tuberculosis. This has created a lot of awareness about these communicable diseases. However, a number of scholars agree that there is very limited knowledge about the existence and prevalence of cervical cancer in Sub-Saharan Africa, and this is happening across different literacy levels [20,21,22,23]. A study carried out in Nigeria in 2000 revealed that out of the 500 attendees of a maternal and child health clinic in Lagos-Nigeria, only 4.3 percent were found to have some knowledge on the existence of cervical cancer [24]. Another study carried out in Lagos-Nigeria in 2004 revealed that out of the 139 patients with advanced cervical cancer, over 80 percent had never heard of cervical cancer [24]. The same trend is seen in Eastern Africa as reported by [11, 25, 26]. Recent studies carried out in Zambia, for example, showed that one of the biggest challenges in curbing the cancer scourge was lack of awareness and the motivation to access cancer services. Many of the participants in the survey wondered how the proposed project (a mass country wide screening initiative by the Zambian government in 2016) would create awareness among women to come forward for screening [11]. Limited knowledge about the existence of cervical cancer among the female population in Sub-Saharan Africa demonstrates the critical need for communication efficiency about the disease. There is a need for a better communication strategy to reach out to the population and educate them about the cervical cancer disease, the need for vaccination, and the significance of early diagnosis and treatment.
3.2 Screening for Early Detection
Sub-Saharan Africa has the world’s lowest screening rates despite the availability of proven simple screening and treatment approaches to cervical cancer, and a majority of the few people who come for screening come in late when the cancer is in its advanced stages [11, 27]. In 2008, only about 1 percent of women in four West African countries had ever screened for cervical cancer, while in Nigeria, only 9 percent of healthcare professionals in two sampled healthcare institutions had ever administered a Pap smear [24]. It is further alarming that many of the women who turn up for screening came in late. For example, at the Ocean Road Cancer Institute in Tanzania, 91 percent of breast cancer patients were diagnosed with stage III or IV cancer [28], while in major cancer screening hospitals in Harare (Zimbabwe), 80 percent of cervical cancer cases are in advanced stages of the disease [11]. Yet, in regions, such as Europe and the United States, where cervical cancer screening is a routine care, research has shown that early screening prevents about 80 percent of potential cervical cancer mortalities [29]. The low screening rates in Sub-Saharan Africa are further aggravated by the limited availability of screening services especially in rural areas. The few that are available are only in urban centers. In 2006, there was only one pathologist, one colposcope, no cyto-technicians, and no facilities for cervical cancer screening or treatment in Malawi, a country which had 47 per 100,000 cervical cancer incidence rates of women by then [30]. Cervical cancer screening facilities in Sub-Saharan Africa are significantly inadequate, yet early screening is still the most viable way the high prevalence of cervical cancer in Sub-Saharan Africa can be curtailed. There are urgent calls for cost-effective cervical cancer screening methods [31].
3.3 Treatment (Adherence)
The cervical cancer advocacy efforts in low- and middle-income countries to date have arguably been heavily skewed toward prevention rather than treatment [1]. The management of invasive cervical cancer continues to be a major challenge in many Sub-Saharan African countries due to, among others, poor follow-up, as many of the women who get the disease are poor, live in distant villages, and find it difficult to travel to the urban center hospitals for follow-up after initial treatment [24]. Yet, WHO standards on cervical cancer recommend successful screening programs of above 80 percent coverage, appropriate follow-up, and management of patients with positive tests [19].
However, there have been numerous calls for measures that can improve prevention, early detection, and treatment of cervical cancer among women in Sub-Saharan Africa [11, 15, 26]. Numerous approaches have so far been piloted, and one of the approaches that have registered some success is the use of Social Media Technologies (SMTs) to provide the much-needed awareness and knowledge for the prevention, early detection, and treatment of cervical cancer among women in Sub-Saharan Africa. However, the scale of usage is still very low yet with the considerable ownership and growing use of smartphones in Sub Saharan Africa; this technology has a great potential to provide the much-needed knowledge and awareness about prevention, early detection, and treatment of the disease. The next section discusses social media technologies and their potential toward the prevention, early detection, and treatment of cervical cancer in Sub-Saharan Africa.
4 The Potential of Social Media Technologies in Prevention, Early Detection, and Treatment of Cervical Cancer
Although Scott and Jacka [32] recognized that there is no single definition of social media, they attempted to define social media as a set of Web-based broadcast technologies that enable the democratization of content, giving people the ability to emerge from consumers of content to publishers. The American Academy of Pediatrics on the other hand defines social media as any website that allows social interaction [33]. The English Oxford Living Dictionary [34] defines social media as “Websites and applications that enable users to create and share content or to participate in social networking.” While there are many loose descriptions of social media, Schein et al. [35] observe that social media is fundamentally defined by its ability to provide an interactive environment for users, where there is a two-way communication and discussion, and users are encouraged to contribute content. The restriction to the Web in the definitions by Scott and Jacka [32] and by O’Keeffe and Clarke-Person [33] does not seem appropriate. Based on the definition from English Oxford Living Dictionary, this paper considers the following websites and applications as social media tools or technologies: Facebook, Twitter, WhatsApp, BlackBerry Messenger, WeChat, PalmChat, SMS (Short Message Service), MMS (Multimedia Message Service), YouTube, and Instagram to mention but a few. With over 1.7 billion Facebook users, 900 million WhatsApp users, 1.12 billion WeChat users, and 320 million Twitter users, using such popular platforms to foster prevention, early detection, and treatment of cervical cancer would have a wide reach to millions of people [36]. As McNab [37] noted that one fact sheet or an emergency message about an outbreak of an infectious disease can be spread through Twitter faster than any influenza virus.
Rapid advances in social media technologies are currently supporting a burgeoning number of novel clinical and public health initiatives in Sub-Saharan Africa. Several studies have shown that mobile communication technologies, Internet access, and more particularly social media have demonstrated fundamental shifts in filling the communication gap in the health sector [38,39,40]. The increased access to the Internet and mobile communication technologies like smartphones, laptops, and digital personal assistants combined with strategic uses of social media like SMS, Facebook, WhatsApp, Instagram, and many others can bring public health information to many more people, more quickly and directly than at any time in history [37]. There is evidence throughout Sub-Saharan Africa, and beyond that, the exciting innovations in social media applications are occurring across the cancer spectrum, from primary prevention and early screening to treatment, survivorship, and end-of-life care in a number of Sub-Saharan African countries [11, 41,42,43]. For example, in regard to prevention by creating awareness about a particular disease, studies outside Sub-Saharan Africa also show promising results in using social media technologies in improving awareness and fostering early screening. A study carried out in the United States to test the feasibility and efficacy of a culturally tailored mobile health intervention designed to increase knowledge about, intent to obtain, and receipt of the HPV vaccine. In a quasi-experimental research design, a 7-day text message on HPV intervention was sent to 30 Korean-American women. The results of the study demonstrated substantial increases in knowledge of HPV with an intent to get vaccinated, and 30 percent of participants received the first dose of the HPV vaccine within 1 year [44]. Another survey conducted among an African diaspora in a high-income country revealed that there was a substantial readiness from users to receive information on cancer prevention and awareness delivered via SMS, WhatsApp, or Twitter on their mobile phones [45]. Social media technologies could also be used to create awareness about the different primary preventions measures such as healthy lifestyles, abstinence and safe sex, cessation of smoking, and HPV vaccination [19]. In 2014, 28 articles on the use of mobile applications in educating people on cancer prevention and management were identified and reviewed. The findings showed that cancer patients who engaged with health professionals using their mobile applications demonstrated increased understanding of both the importance of self-monitoring and knew how and where to seek medical assistance if needed [46]. In regard to early disease diagnosis, a feasibility study in Uganda demonstrated that it was possible for a trained pathologist to make an accurate diagnosis from images sent via MMS [47]. Images taken from a mobile phone have been proven to be very useful for dermatological diagnosis. Preliminary studies in Uganda and Egypt have shown the possibility of using mobile phones to take skin infection images and then send them via MMS to an expert for analysis. This has improved diagnostic rates of dermatological conditions [48, 49]. However, although MMS have significantly aided diagnosis of cervical cancer (with an average specificity of 82 percent), larger scale studies are still needed. In regard to treatment adherence, successes of using social media technologies to foster adherence have also been reported. For example, appointment and adherence SMS messages saw a significant adherence improvement mostly among TB patients in Malawi [31], and text messaging for treatment adherence with or without the use of smart pillboxes has been reported in Mozambique [50]. Generally, SMS-based reminders have been proven to reduce patient appointment nonadherence by 40 percent [51]. Reviews of clinical trials of SMS appointment reminders carried out in 2012 and 2013 concluded that the intervention is moderately effective in improving attendance [52]. From the findings, this paper would be right to state that the use of social media technologies such as SMS text messages can potentially increase the adherence rate to an average of 82 percent.
However, throughout the literature, there is very little empirical evidence on the extent to which social media technologies have leveraged prevention, early detection, and treatment of cervical cancer among women particularly in Sub-Saharan Africa. Yet, social media technologies have a great potential in raising awareness of cancer risks and symptoms, preliminary diagnosis by health workers, clinical appointment management, and diagnostic follow-up [53]. Although there are a few individual case studies done, they are isolated and do not provide a good overall picture on how social media have leveraged prevention, early diagnosis, and treatment of cervical cancer in Sub-Saharan Africa. There was a need to provide an overall assessment on the extent to which social media has leveraged prevention, early diagnosis, and treatment of cervical cancer in Sub-Saharan Africa.
Therefore, this paper presents the extent to which social media technologies can leverage the prevention, early detection, and treatment of cervical cancer among women in Sub-Saharan Africa.
5 Methodology
This paper used a systematic review of literature on the use of social media in prevention, early detection, and treatment of diseases in general and cervical cancer in particular to establish the potential social media can offer to prevention, early detection, and treatment of cervical cancer in Sub-Saharan Africa. A systematic review was the main method used in this paper. In 1984, Cooper [54] proposed a five-stage systematic review process that was followed in this chapter’
-
Problem formulation—Statement of objective
-
Data collection—An unbiased literature search
-
Data evaluation—Assessing the studies for inclusion in the review
-
Public presentation—Discussion and context of findings
The strength of systematic review method lies in using empirical evidence to establish what works and how it worked [55, 56]. The systematic review method has been extensively used in medical research and the natural sciences. It is commonly used by international agencies such as the Australian Agency for International Development (AusAID), the UK’s Department for International Development (DFID), and many others directly or indirectly by individuals or organizations contracted to do research on their behalf with the sole aim of finding what works and how it worked in generating development outcomes [55]. The purpose of the systematic review carried out in this paper was to establish the extent to which use of social media technologies can support the prevention, early detection, and treatment of cervical cancer among women in Sub-Saharan Africa.
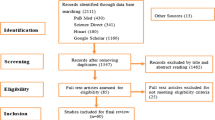
Data collection: An extensive and unbiased literature search was conducted on the extent to which social media technologies can leverage the much-needed services in the areas of cervical cancer prevention, early diagnosis, and treatment in Sub-Saharan Africa, and the likely challenges of deploying social media technologies in fighting cervical cancer in the region. The review covered reports, journals, conference proceedings, books, and Web sites. Google Scholar and PubMed journal sites were of much help for this review.
About 52 journal/conference/book chapters/articles on topics related to the use of social media in the prevention, early detection, and treatment of diseases in general and cervical cancer in particular were selected for the review. The review included two papers on the use of social media technologies to support the prevention (creating awareness) of cervical cancer in Sub-Saharan Africa, with five supporting papers (on the use of social media technologies to support awareness in other diseases); three papers on the use of social media technologies to support early diagnosis of cervical cancer in Sub-Saharan Africa, with five supporting papers (on the use of social media technologies to support early detection in other diseases); and one paper on the use of social media technologies to support treatment (adherence) of cervical cancer in Sub-Saharan Africa, with four supporting papers (on the use of social media technologies to support treatment in other diseases) (see the Appendix for details). About 33 research articles were removed because they were found to be irrelevant. The remaining 20 (six papers on the use of social media technologies to support the prevention, early detection, and treatment of cervical cancer in Sub-Saharan Africa and 14 supporting papers) were reviewed.
Data evaluation: Khan et al. (2010) observe that selected papers for a systematic review must be subjected to a more refined quality assessment procedure. This can be done through general critical appraisal guides and design-based quality checklists. In this paper, we used a simple data extraction table to organize the information extracted from each review (e.g., authors, country, publication year, study design/number of participants, the technology used, and the outcomes of these study). The findings of the review are presented in the next section.
6 Finding from the Systematic Review
6.1 Prevention (Awareness Campaign)
Throughout the search for scientific literature, very few published papers were found on the use of social media technologies in creating awareness about cervical cancer in Sub-Saharan Africa. However, this paper managed to identify two published papers as presented below.
In an attempt to raise awareness of cervical cancer and dispel myths, misconceptions and advocate for early screening, the Tanzania Youth Alliance (TAYOA) in partnership with the Ministry of Health and Social Welfare (MoHSW) deployed a free SMS and toll-free helpline service to raise awareness about cervical cancer and the importance of early screening nationwide. About 41,751 SMS subscribers were registered, and a total of 843,496 text messages were sent out. In addition, 22,172 calls were made during the pilot scheme. Each subscriber received 20 text messages for a period of 20 days (at least one text message a day). As a result, the total number of women who had a screening visit as a result of receiving a text message was 9,247, representing about 22 percent of SMS subscribers [57].
Another study was conducted in Kenya, in 2012, to establish the extent of mobile phone and Internet used by cervical cancer patients would increase access to information related to cancer treatment and management. The study recruited 205 participants, and about 96.5 percent (n = 192) of the participants owned mobile phones. The participants were asked to give their opinion on how mobile phones could be used in cancer management. About 31.7 percent (n = 63) of the participants recommended that educational messages via SMS text should be sent through their mobile phones [58]. Table 10.3 summarizes the cases studies from Tanzania and Kenya.
6.2 Screening for Early Detection
The scarcity of literature suggests that the application of social media technologies in cervical cancer screening is still in its infancy [59]. A few Sub-Saharan African countries are currently piloting the use of social media-based technologies to foster early screening as presented below.
In Botswana, a pilot study was conducted with about 95 HIV-positive women in Gaborone. Visual inspection of the cervix with the application of 4 percent acetic acid (VIA) was performed among 95 participants, and the images of the cervix were then taken using a mobile phone camera and sent via MMS to an expert gynecologist. The expert received the pictures and made definitive positive or negative reading based on the PIA results. The average specificity of all the 95 readings was 82 percent. Hence, social media technologies may be useful in improving access to cervical cancer screening for women in remote areas utilizing the VIA ‘see-and-treat’ method [43].
The Zambian program called electronic cervical cancer control (eC3) uses a digital camera to capture images of the cervix (Cervigrams). The images are then shared via MMS with remote experts based in tertiary hospitals in Lusaka for consultation and further diagnosis. One of the goals of eC3 is to bridge the gap between screening and diagnosis in order to facilitate screen and treat model thereby minimizing the loss of patients to follow-up [16]. The program was found to be successful with an average specificity of 83 percent and was rolled out to the other parts of Zambia. An evaluation of the initiative was carried out in 2013 which found out that a total of 102,942 women had been screened for cervical cancer in Lusaka alone through the initiative. This represented a 95 percent screening uptake by the women who were offered the chance to screen [11].
A similar successful approach (using eC3 and digital cameras) to the Zambian model was also piloted in Madagascar. The study in Madagascar recruited 332 women for the exercise. To improve VIA screening performance, digital images of the cervix were taken after acid acetic application (D-VIA). The aim of this study was to evaluate the use of a smartphone for on- and off-site D-VIA diagnosis. The study found out that the on-site physician had a sensitivity of 66.7 percent (95 percent CI: 30.0–90.3) and a specificity of 85.7 percent (95 percent CI: 76.7–91.6). The off-site physician on the other hand who received images on MMS had consensus sensitivity of 66.7 percent (95 percent CI: 30.0–90.3) with a specificity of 82.3 percent (95 percent CI: 72.4–89.1) [42]. Table 10.4 summarizes the cases studies from Botswana, Zambia, and Madagascar.
6.3 Treatment (Adherence)
There is very little evidence on the use of social media technology for cervical cancer patient follow-up and adherence [11, 60]. However, a study conducted by Karanja [60] gives, to some extent, clear results on the effectiveness of social media technologies in fostering cervical cancer patient follow-up and adherence. Karanja [60] accessed the use of mobile phone short text message service in enhancing cervical cancer screening in the Thika Level 5 Hospital; four SMS reminders were sent to women on the next cervical cancer screening dates. The study revealed that, out of the 286 recruited participants, 67.1 percent of the participants in the intervention group re-attended to schedule repeat cervical cancer screening compared to only 20.3 percent in the control group. The study concluded that the re-attendance for cervical cancer screening as scheduled was found to be eight times more likely when SMS reminders were sent [60]. Table 10.5 summarizes the study conducted in Kenya.
7 Discussion
Whereas there is scientific literature on the use of social media technologies to leverage disease prevention, diagnosis, and treatment in Sub-Saharan African, much of the literature focuses on Ebola, HIV, malaria, and TB. The literature on the use of social media to combat cervical cancer in Sub-Saharan Africa is still limited in many respects. More so, many of these initiatives are still being piloted. Therefore, there is a need for full scales, enabling more rigorous experimental and quasi-experimental studies to be undertaken in order to strengthen the evidence base [61]. Furthermore, the variety of social media technology that has been so far used in the prevention, early detection, and treatment of cervical cancer has so far been limited to SMS and MMS, yet there are more social media technologies with more useful functionalities like interaction one on one or as a group; easier sharing with other individuals or groups; safe storage of messages; and better multimedia capabilities like sharing video, audios, and pictures. Hence, there is need to explore the potential of these too.
However, the reviewed studies present a promising role of the use of text SMS and MMS in cervical cancer prevention, diagnosis, and adherence in Sub-Saharan Africa as exemplified by the two successful cases under prevention, three successful cases under early detection, and one successful case under treatment.
7.1 Prevention (Awareness Campaign)
It is unfortunate that 90 percent of cervical cancer infections and deaths are found in Sub-Saharan Africa cervical cancer, yet, cervical cancer is the most preventable of all the three most common types of cancers. However, social media technologies can be leveraged as prevention tools. From the studies, there is evidence that the appropriate use social media technologies can help prevent cervical cancer by creating awareness about the existence of cervical cancer, the importance of routine screening and change of behavioral life styles. From the findings, an initiative by TAYOA in Tanzania on the use of SMS messages to encourage women to screen for cervical cancer saw over 9000 women (22 percent) who had registered for the initiative participate in the cervical cancer screening exercise. Likewise, in Kenya, 31.7 percent of the participants in the study recommended receiving educational SMS messages on their mobile phones. From the findings, the use of social media technologies to promote awareness has been found to encourage routine cervical cancer screening by an average of 28 percent. Generally, successful trials on the use of social media technologies to create awareness about cancer in developed country setting have been done, and this kind of initiative has seen information delivered by SMS increase in female screening rates by 23 percent [62]. When using social media technologies to create awareness among the population, it is important to note that, it is not the social media channel which will be successful but the effect the message it contains has on the recipient. It is therefore important that message content itself be tailored appropriately—if the health awareness initiative using social media technologies is to be successful in promoting awareness cancer prevention and self-management.
7.2 Early Detection/Screening/Diagnosis
Social media technologies have also been deployed to aid early screening of cervical cancer. Promising levels of accuracy have been reported. From the findings, an initiative in Botswana, Zambia, and Madagascar was taken where the images of the cervix are taken using a mobile phone camera during the screening process and then sent via MMS to an expert gynecologist who makes diagnosis with a specificity of 82 percent in Botswana, 83 percent in Zambia, and 82.3 percent in Madagascar. Using social media technologies to transmit images for remote expert analysis and interpretation could be a perfect solution to shortages of specialist physicians in developing countries [61]. Studies have established that smartphone cameras have adequately high resolutions that make it possible for an expert to see key infectious agents and hematological signs [61].
7.3 Treatment (Adherence)
In cervical cancer treatment, social media technologies are majorly deployed in follow-ups and adherence. From the findings, SMS text messages sent to cervical cancer patients to remind them of scheduled appointments have been piloted in Nigeria and Kenya. SMS message reminders enabled 67.1 percent of cervical cancer patients to honor their appointments in Kenya.
This paper, therefore, concludes this discussion with the following observations. First, there is a significant contribution of social media technologies toward leveraging the prevention, early diagnosis, and treatment of cervical cancer in Sub-Saharan Africa and is substantial as seen in Kenya and Tanzania (prevention/awareness), Botswana, Zambia, and Madagascar (diagnosis) and Kenya (treatment). Second, it should be noted that the most widely used form of social media technology for prevention, early diagnosis, and treatment of cervical cancer in Sub-Saharan Africa is SMS text messaging and MMS. Finally, as future research, there is a need to conduct a systematic review of the challenges of using social media technologies in the prevention, diagnosis, and treatment of cervical cancer in Sub-Saharan Africa.
8 Conclusion
There is evidence that social media technologies have been useful in improving prevention (encouraging routine screening by 28 percent), early detection/diagnosis (specificity of 82 percent), and treatment of cervical cancer in Sub-Saharan Africa (improving adherence rate by 67.1 percent). From the findings, the most commonly used social media technologies for preventing, diagnosing, and treating cervical cancer are SMS text messaging for prevention and treatment and MMS for diagnosis. Other forms of social media are rarely used despite their potential. Whereas there are very limited scientific studies on the use of social media technologies to prevent, diagnose, and treat cervical cancer in Sub-Saharan Africa, substantial studies have been conducted on their use in the prevention, diagnosis, and treatment of other communicable diseases like HIV, malaria, and TB [63]. Therefore, cervical cancer researchers and practitioners have an opportunity to leverage the potential of social media technology in its application to prevention (health awareness campaigns), diagnosis (interpretation), and treatment (appointment tracking and follow-up, patient reminders) in other diseases. The current initiative on the use of social media technologies to prevent, diagnose, and treat communicable diseases like HIV, malaria, and TB in Sub-Saharan Africa allows replicability and avoids the need to reinvent the wheel.
References
Olsen M (2015) Cancer in sub-Saharan Africa: the need for new paradigms in Global Health. Trustees of Boston University. http://www.bu.edu/pardee/files/2015/12/PardPap17_120215sing.pdf. Accessed 22 June 2017
UNAIDS (2016) Global statistics 2015 (Fact sheets 2016) Geneva, Switzerland: United Nations Joint Programme on HIV and AIDS, p 8. Retrieved from http://www.unaids.org/sites/default/files/media_asset/ UNAIDS_FactSheet_en.pdf. Accessed 29 May 2017
WHO – World Health Organization, Ebola Situation Report – 30 December (2015).http://apps.who.int/ebola/current-situation/ebola-situation-report-30-december-2015. Accessed 29 May 2017
UNDG – United Nations Development Group Report (2015). Socio-economic impact of Ebola virus disease in west African countries a call for national and regional containment, recovery and Prevention. www.africa.undp.org/content/dam/rba/docs/Reports/ebola-west-africa.pdf. Accessed 28 May 2017
USAID (2014) Use of technology in the Ebola response in West Africa. Technical brief
IPIN – The Institut Pasteur International Network: Sub-Saharan Africa and the Indian Ocean- Report (2012) http://www.who.int/bulletin/africanhealth/en/23 May 2016. Accessed on 24, October 2016
The Economist (2014) Worse than AIDS the burden of cancer is falling increasingly heavily on the poor. The Economist Online. Retrieved from http://www.economist.com/news/international/21597962-burden-cancerfalling-increasingly-heavily-poor-worse-aids. Accessed 29 June 2017
Jemal A, Bray F, Melissa M, Ferlay CJ, Ward E, Forman D (2011) Global cancer statistics. A Cancer J Clin 61(2):69–90
The American Cancer Society. Global cancer facts & figures 3rd Edition (2012). https://www.cancer.org/content/dam/cancer-org/research/cancer-facts-and-statistics/global-cancer-facts-and-figures/global-cancer-facts-and-figures-3rd-edition.pdf. Accessed 29 June 2017
Ferlay J, Soerjomataram I, Dikshit R, Eser S, Mathers C, Rebelo M, Parkin DM, Forman D, Bray F (2012) Cancer incidence and mortality worldwide: sources, methods and major patterns in GLOBOCAN 2012 Int J Cancer 2015. 136(5):E359–E386.https://doi.org/10.1002/ijc.29210
Owuor J, Chengo C, Kapambwe S (2016) The use of telehealth in cervical cancer screening and care in Zambia. A needs assessment undertaken for SPIDER June–August (2016). https://spidercenter.org/files/2017/03/Report-Telehealth-Zambia-170309-web.pdf. Accessed 22 June 2017
IARC-International Agency for Research on Cancer (2013) GLOBOCAN 2012 v1.0, Cancer incidence and mortality worldwide: IARC CancerBase no. 11. IARC Library, Lyon
Campos NG, Kim JJ, Castle PE, Ortendahl JD, O’Shea M, Diaz M (2012) Health and economic impact of HPV 16/18 vaccination and cervical cancer screening in eastern Africa. Int J Cancer 130:2672. https://doi.org/10.1002/ijc.26269
Kapambwe S, Sahasrabuddhe VV, Blevins M, Mwanahamuntu MH, Mudenda V, Shepherd BE, Parham GP (2015) Implementation and operational research: age distribution and determinants of invasive cervical Cancer in a screen-and-treat program integrated with HIV/AIDS care in Zambia. J Acquir Immune Defic Syndr 70(1):e20
Bateman AC, Katundu K, Mwanahamuntu MH, Kapambwe S, Sahasrabuddhe VV, Hicks ML, Chibwesha CJ (2015) The burden of cervical pre-cancer and cancer in HIV positive women in Zambia a modelling study. BMC Cancer 15:541–551
Parham GP, Mwanahamuntu MH, Pfaendler KS, Sahasrabuddhe VV, Myung D, Mkumba G, Hicks ML (2010) eC3—a modern telecommunications matrix for cervical cancer prevention in Zambia. J Low Genit Tract Dis 14(3):23–32
Afri-DevInfor (2014) Africa cervical cancer multi indicator incidence & mortality score card, Summary scorecard & research findings at end of scorecard including global /Africa Continental/sub regional and country trends; & Links with SRH, HIV/AIDS, adolescent & maternal health
Richter K, Becker P, Horton A, Dreyer G (2013) Age-specific prevalence of cervical human papillomavirus infection and cytological abnormalities in women in Gauteng Province, South Africa. S Afr Med J 103:313–317
Jordaan S, Michelow P, Richter K, Simoens C, Bogers J (2016) A review of cervical cancer in South Africa: previous, current and future health care current reviews. An open access journal 4(4):1000180
Ajayi IO, Adewole IF (1998) Knowledge and attitude of out patients’ attendants in Nigeria to cervical cancer. Cent Afr J Med 44(2):41–44
Buga GA (1998) Cervical cancer awareness and risk factors among female university students. East Afr Med J 75(7):411–416
Walker ARP, Michelow PM, Walker BF (2002) Cervix cancer in African women in Durban, South Africa. Int J Gynecol Obstet 79:45–46
Wellensiek N, Moodley M, Moodley J et al (2002) Knowledge of cervical cancer screening and use of cervical screening facilities among women from various socioeconomic backgrounds in Durban, Kwazulu Natal, South Africa. Int J Gynecol Cancer 12:376–382
Anorlu RI, Banjo AAF, Odoemhum C et al (2003) Cervical cancer and cervical cancer screening: level of awareness in women attending a primary health care facility in Lagos. Niger Postgrad Med J 70:25–28
Gichangi P, Estamble B, Bwayo J et al (2003) Knowledge and practice about cervical cancer and pap smear testing among patients at Kenyatta National Hospital, Nairobi, Kenya. Int J Gynecol Cancer 13:827–833
Kidanto HL, Kilewo CD, Moshiro C (2002) Cancer of the cervix: knowledge and attitudes of female patients admitted at Muhimbili National Hospital, Dar es salaam. East Afr Med J 467–69(2002):79
Mwanahamuntu MH, Sahasrabuddhe VV, Kapambwe S, Pfaendler KS, Chibwesha C, Mkumba G (2011) Advancing cervical Cancer prevention initiatives in resource-constrained settings: insights from the cervical cancer prevention program in Zambia. PLoS Med 8:e1001032. https://doi.org/10.1371/journal.pmed.1001032
Nelson S, Kim J, Wilson FA, Soliman AS, Ngoma T, Kahesa C, Mwaiselage J (2016) Cost-effectiveness of screening and treatment for cervical cancer in Tanzania: implications for other sub-Saharan African countries. Value Health Reg Issues 10:1–6. https://doi.org/10.1016/j.vhri.2016.03.002
Finocchario-Kessler S, Wexler C, Maloba M, Mabachi N, Ndikum-Moffor F, Bukusi E (2016) Cervical cancer prevention and treatment research in Africa: a systematic review from a public health perspective. BMC Womens Health 16(1):1–25
Denny L, Quinn M, Sankaranarayanan R (2006) Screening for cervical cancer in developing countries. Vaccine 24(Suppl 3):71–77
Mahmud N, Rodriguez J, Nesbit J (2010) A text message-based intervention to bridge the healthcare communication gap in the rural developing world. Technol Health Care 18:137–144
Scott PR, Jacka JM (2015) Chapter 1: Social media: an overview. In: Scott, Jacka (eds) Auditing social media: a governance and risk guide. Wiley Online Library. https://doi.org/10.1002/9781119202585.ch1
O’Keeffe GS, Clarke-Pearson K (2011) The impact of social media on children, adolescents, and families. Pediatrics 127(4):800
English Oxford Living Dictionary (2017) https://en.oxforddictionaries.com/definition/us/social_media. Accessed 29 May 2017
Schein R, Wilson K, Keelan J (2010) Literature review on the effectiveness of the use of social media. A report for peel public health. Region of Peel, Canada, July 2010
Smith K (2016) Marketing; amazing social media statistics and facts Mark Theory https://www.brandwatch.com/blog/96-amazing-social-media-statistics-and-facts-for-2016/. Accessed 29 June 2017
McNab C (2009) What social media offers to health professionals and citizens. Bull World Health Organ 8(7):566–566. https://doi.org/10.2471/BLT.09.0667122008
Kamara M (2016) Changing cultures: changing lives—mobilising social media during a health crisis. In: Robertson M (ed) Communicating, networking: interacting. springerbriefs in global understanding. Springer, Cham
Neuhauser L, Kreeps GL (2010) E-health communication and behaviour change: promise and performance. Soc Semiot 20:7–24
Waters JK (2011) The everything guide to social media. Adams Media
Baron RC, Melillo S, Rimer BK, Coates RJ, Kerner J, Habarta N, Chattopadhyay S, Sabatino SA, Elder R, Leeks KJ (2010) Task force on community preventive services intervention to increase recommendation and delivery of screening for breast, cervical, and colorectal cancers by healthcare providers a systematic review of provider reminders. Am J Prev Med Jan 38(1):110–117n
Catarino R, Vassilakos P, Scaringella S, Undurraga-Malinverno M, Meyer-Hamme U, Ricard-Gauthier D, Petignat P (2015) Smartphone use for cervical cancer screening in low-resource countries: a pilot study conducted in Madagascar. PLoS ONE 10(7):e0134309. https://doi.org/10.1371/journal.pone.0134309
Quinley K E, Gormley RH, Ratcliffe SJ, Shih T, Szep Z, Steiner A, Masire DR Kovarik CL (2013) Use of mobile telemedicine for cervical cancer screening https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3746464/. Accessed 29 June 2017
Lee HY, Koopmeiners JS, McHugh J, Raveis HV, Ahluwalia SJ (2016) mHealth pilot study: text messaging intervention to promote HPV vaccination. Am J Health Behav 40(1):67–76. https://doi.org/10.5993/AJHB.40.1.8
Schoenberger YM, Phillips JM, Mohiuddin MO (2015) J Canc Educ (2015) 30:636. https://doi.org/10.1007/s13187-014-0743-6
Davis SW, Girvan IO (2014) mHealth education applications along the Cancer continuum. J Cancer Educ Dec 9. 30(2):388–394. https://doi.org/10.1007/s13187-014-0761-4.
Tuijn CJ, Hoefman BJ, Van Beijma H, Oskam L, Chevrollier N (2011) Data and image transfer using mobile phones to strengthen microscopy-based diagnostic services in low and middle income country laboratories. PLoS ONE 6, e28348
Tran K, Ayad M, Weinberg J, Cherng A, Chowdhury M, Monir S (2011) Mobile tele dermatology in the developing world: implications of a feasibility study on 30 Egyptian patients with common skin diseases. J Am Acad Dermatol 64:302–309
Fruhauf J, Hofman-Wellenhof R, Kovarik C, Mulyowa G, Alitwala C, Soyer HP (2013) Mobile tele dermatology in sub-Saharan Africa: a useful tool in supporting health workers in low-resource centres. Acta Derm Venereol 93:122–135
Davey DJ, Hares S, Ponce W, et al (2012) Evaluating SMS reminders in improving ART and PMTCT adherence in Mozambique: challenges in achieving scale. In: 7th international conference on appropriate healthcare technologies for developing countries. vol. 41, London, UK
Downer SR, Meara JG, Da-Costa AC (2005) Use of SMS text messaging to improve outpatient attendance. Med J Aust.Oct 3;183(7):366–368. [PubMed]
Dey S (2014) Preventing breast cancer in LMICs via screening and/or early detection: the real and the surreal. World J Clin Oncol Aug 10;5(3):509–519. https://doi.org/10.5306/wjco.v5.i3.509
Eskandar H, Land AM, Arnold V, Pujari S, Prasad MV, Susanna R (2015) Mobile technology in cancer control for emerging health systems: digital divide or digital provide. Cancer Control 2015 World Health Organization/International Telecommunications Union Report, pp 65–70
Cooper HM (1984) 1: The integrative research review: a systematic approach. In: Applied Social Research Methods Series, vol 2. Sage, Beverly Hills
Zanker JH Mallett R (2013) How to do a rigorous, evidence focused literature review in international development. A Guidance Note https://www.odi.org/sites/odi.org.uk/files/odi-assets/publications-opinion-files/8572.pdf. Accessed 17 Apr 2016
Khan KS et al (2003) Five steps to conducting a systematic review. J R SocMed 96(3):118–121
Ndakidemi E, Masika P, Luvanda B, Oluwole B, Asante E, Olateju A (2014) Increasing access to information and demand for cervical cancer screening services in Mwanza, Tanzania Utilizing Mobile Technology. Project report. http://www.tayoa.org/tayoa/wp-content/uploads/2016/04/Final-Poster.pdf. Accessed on 25 Apr 2017
Kivuti LWB, McDonnell G, Pokhariyal GP, Roudsari AV (2012) Self-reported use of internet by cervical cancer clients in two National Referral Hospitals in Kenya. BMC Res Notes 20125:559. https://doi.org/10.1186/1756-0500-5-559
Owuor J, Kabukye JK, Stephen R, Gahenda G, Lun JN (2016) The use of telehealth in cervical cancer screening and care in Rwanda. A needs assessment undertaken for SPIDER. https://spidercenter.org/files/2017/07/Report-Telehealth-Rwanda-100710-Web.pdf. Accessed 22 June 2017
Karanja WA (2015) Use of mobile phone short text message service to enhance cervical cancer screening at the Thika level 5 hospital, Kiambu County, Kenya. PhD Thesis
Charles S, Hall SC, Fottrell E, Wilkinson S, Byass P (2014) Assessing the impact of mHealth interventions in low- and middle income countries what has been shown to work. Glob Health Action 7:25606. https://doi.org/10.3402/gha.v7.25606
Lee HY, Koopmeiners JS, Rhee TG, Raveis VH, Ahluwalia JS (2014) Mobile phone text messaging intervention for cervical Cancer screening: changes in knowledge and behavior pre-post intervention. J Med Internet Res 16(8):e196
Bigna JJ, Noubiap JJ, Kouanfack C, Plottel CS, Koulla-Shiro S (2014) Effect of mobile phone reminders on follow-up medical care of children exposed to or infected with HIV in Cameroon (MORE CARE): a multicentre, single-blind, factorial, randomised controlled trial. Lancet Infect Dis Jul 14(7):600–612
Anorlu RI (2008) Cervical cancer: the sub-Saharan African perspective. Elsevier Journal on Reproductive Health Matters 16(32):41–49
Misrahi Y (2016) Results from a visual-based cervical cancer screening program. The 1st annual Future of Health: Telemedicine and AI summit held in Ho Chi Minh City, Vietnam. 1:1
Louie KS, de Sanjose S, Mayaud P (2009) Epidemiology and prevention of human papillomavirus and cervical cancer in sub-Saharan Africa. A comprehensive review. Trop Med Int Health 14:1287–1302
Author information
Authors and Affiliations
Editor information
Editors and Affiliations
Appendix
Appendix
Strategies | Papers (use of SMT in cervical cancer) | Supporting papers (use of SMT in other diseases) | Other literature |
|---|---|---|---|
Prevention (creating awareness) | Lee et al. (2014) [62] Lee et al. (2016) [58] Schoenberger et al. (2014) [45] Jordaan et al. (2016) [19] Davis and Girvan (2014) [46] | Buga (1998) [21]; Ajayi and Adewole (1998) [20]; Walker et al. (2002) [22]; Wellensiek (2002) [23]; Anorlu et al. (2003) [24]; Anorlu (2008) [64]; Gichangi et al. (2003) [25]; Kidanto et al. (2002) [26]; Owuor et al. (2016) [11]; Kamara (2015) [38]; Neuhauser and Kreeps (2010) [39]; Waters (2011) [40]; McNab (2009) [37]; Olsen (2016) [1]; Karanja (2015) [60] | |
Early screening/diagnosis | Charles et al. (2014) [61] Tuijn et al. (2011) [47] Tran et al. (2011) [48] Fruhauf et al. (2013) [49] Misrahi (2017) [65] | Mwanahamuntu et al. (2011) [27]; Owour et al. (2016) [1]; Anorlu (2008) [64]; Finocchario-Kessler et al. (2016) [29]; Denny et al. (2006) [30]; Louie (2009) [66]; Owuor et al. (2016) [59] | |
Treatment (adherence) | Karanja (2015) [60] | Ndakidemi et al. (2014) [57] Davey et al. (2012) [50] Downer et al. (2005) [51] Dey (2014) [52] | Olsen (2016) [1]; Anorlu (2008) [64]; Owuor et al. (2016) [11]; Karanja (2015) [60] |
Rights and permissions
Copyright information
© 2019 Springer International Publishing AG, part of Springer Nature
About this chapter

Cite this chapter
Eilu, E., Baguma, R. (2019). Prevention, Early Detection, and Treatment of Cervical Cancer in Sub-Saharan Africa (SSA): A Mobile Social Media Approach. In: Paiva, S. (eds) Mobile Solutions and Their Usefulness in Everyday Life. EAI/Springer Innovations in Communication and Computing. Springer, Cham. https://doi.org/10.1007/978-3-319-93491-4_10
Download citation
DOI: https://doi.org/10.1007/978-3-319-93491-4_10
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-93490-7
Online ISBN: 978-3-319-93491-4
eBook Packages: EngineeringEngineering (R0)