
Abstract
Pivotal response treatment (PRT) is a comprehensive, evidence-based treatment model for individuals with autism spectrum disorder. This chapter will detail the development of PRT and introduce the basic behavioral and motivational strategies used to enhance social engagement, language, and play for young children with ASD. PRT has traditionally relied upon “parent training” or “parent education” as an integral component of intervention, and research studies focused on the parent-training components of PRT will be described. We also provide a rationale for earlier intervention to improve prognosis and enhance developmental gains for individuals with ASD. Thus, this chapter will address the justification and methods for adapting PRT for families of high-risk infants under 24 months of age and describe how a naturalistic, developmental, behavioral approach that targets social motivation is ideally suited for infant intervention. Preliminary research presented here suggests that the motivational strategies of PRT can be effective for improving social engagement and social communication for infants within the first two years of life.
Access provided by CONRICYT-eBooks. Download chapter PDF
Similar content being viewed by others
Keywords
- Naturalistic developmental behavioral intervention
- Early intervention
- Treatment
- Pivotal response treatment
- Infancy
- Social engagement
- Social communication
- Autism spectrum disorder
Pivotal Response Treatment to Support Families of High-Risk Children and Those with a Diagnosis of Autism Spectrum Disorder
Pivotal response treatment (PRT) is a naturalistic, developmental, behavioral intervention that was developed to improve motivation in children with autism spectrum disorder, consequently accelerating learning and triggering widespread gains. To target the pivotal area of motivation for children with ASD, a specific set of strategies is implemented as a package during teaching opportunities. These strategies can be applied throughout the child’s waking hours within natural settings and daily routines. Initial research on PRT focused on expressive communication (Koegel, O’Dell, & Koegel, 1987), but subsequent studies showed that the strategies are effective across a wide range of developmental domains. Importantly, research demonstrated that when targeting pivotal areas, widespread collateral gains in other untargeted areas were observed (e.g., Koegel & Koegel, 1995; Koegel, Koegel, Harrower, & Carter, 1999; Mundy, Sigman, & Kasari, 1990; Schreibman, Stahmer, & Pierce, 1996). Thus, intervention proved to be more efficient and effective when motivational components were included. The end goal of PRT is to provide an intervention that will result in improvements in a broad number of behaviors in a natural setting and provide young children with autism the tools to learn skills in language, socialization, and academics that are necessary to lead meaningful, independent lives.
PRT is based on behavior modification approaches that were originally developed to decrease disruptive behaviors and improve social and communicative functioning for children with ASD (Lovaas, Koegel, Simmons, & Long, 1973; Lovaas, Schreibman, & Koegel, 1974). These initial studies of PRT demonstrated significant improvements in the children’s behavior by using discrete trials and rewarding appropriate behavior (e.g., Lovaas, 1977). This type of research uses a standard “ABC” behavioral format in which an antecedent is presented, the child responds with a target behavior, and a consequence is provided to reinforce that behavior. Table 4.1 demonstrates an example of how discrete trial training (DTT) may be used to teach a child colors.
This paradigm is similar to teaching strategies that are commonly used in the classroom, wherein children are seated at desks or tables and can receive stickers or verbal reinforcement when they respond correctly to a teacher’s question. The reinforcement method in which stickers or tokens are provided for correct or good behavior, and can then later be exchanged for a reward or prize, is called a “token economy” and is commonly used with typically developing children and even adults. However, early work in autism treatment suggested that the motivation of typically developing children appears to differ from that of children with ASD (Koegel & Egel, 1979). Young children are generally motivated to learn in order to get social reinforcement from teachers and parents; yet social motivation is diminished in young children with ASD. The use of a token economy system that required children with ASD to work for favorite objects or activities was effective for teaching discrete skills in discrete settings. However it was quickly apparent that this discrete trial, behavioral approach (sometimes referred to simply as an “applied behavior analysis” or the “ABA” approach) lacked effectiveness in promoting generalization and maintenance of learned skills. That is, children with autism were acquiring new skills, but many did not maintain over time and were not generalizable to different settings or different behaviors.
PRT was developed to overcome some of these challenges and carries a few basic underlying tenets. First, parent education is a necessary component in the education of children with autism. Research shows that parents are not only helpful in implementing intervention for children with ASD but that parents are in fact an essential piece of the entire intervention process. Without their active involvement, their child’s gains are unlikely to generalize or maintain (Koegel, Glahn, & Nieminen, 1978). Second, intervention must be implemented in natural settings using child-preferred materials and activities that are found in those settings. Artificial settings do not result in the level of generalization and maintenance that occurs when inclusive settings with naturally occurring stimuli are used (Koegel, O’Dell, & Koegel, 1987). Third, a focus on improving the individual with autism’s motivation will accelerate learning and decrease frustration and disruptive avoidance and escape behaviors. It was observed that while using structured ABA procedures, children continued to have difficulty rapidly acquiring skills and they appeared to lack motivation to learn during intervention sessions. These challenges precipitated a line of research focused on using naturalistic methods to target underlying features of autism, such as motivation. Studies began to focus on procedures to strengthen the response-reinforcer relationship (Koegel & Egel, 1979; Williams, Koegel, & Egel, 1981). The thought was that the children may be experiencing “learned helplessness,” which occurs when there is a perceived absence of control over the response-consequence contingency, and subsequently an individual may stop trying or exhibit very low rates of responding (Seligman, 1972). To counteract this phenomenon, steps to motivate the individual were put in place. A number of individual areas were researched with the end goal of improving “motivation,” defined as improving children’s responsiveness, correct responding, and positive affect. In other words, by using strategies to improve motivation, collateral gains would be observed in multiple areas. Motivation would be the first pivotal behavior and the defining component in pivotal response treatment. It was hypothesized that motivation could be measured by changes in children’s affect. Affect in terms of enthusiasm, happiness, and interest became a critical measure in the initial intervention research leading to the development of PRT.
This new theoretical paradigm was tested by combining a general “ABA” stimulus-response-consequence framework with newly developed strategies for presenting teaching trials. A variety of systematic procedures were incorporated into both the presentation of the stimulus items (i.e., antecedent) and the reinforcement provided subsequent to the desired behavior (i.e., consequence). These antecedent and consequence strategies were developed to improve motivation, thus accelerating learning, improving affect, and decreasing disruptive behavior. Importantly, the target behaviors remained the same (e.g., language), while the treatment delivery method was altered in order to incorporate the motivational components. These modifications to the traditional ABA framework for teaching skills to children with ASD formed the earliest foundation for the development of pivotal response treatment. The general motivational procedures are described below.
Child Choice
Child choice or following the child’s lead makes an enormous difference in child responsiveness. Instead of using flash cards or arbitrary items that are usually uninteresting to the child, child-preferred items are identified and incorporated into treatment. This means that if the child is more motivated when playing on the swings, then intervention is moved to the playground. Implementing treatment in the child’s natural environment using child choice greatly increases the likelihood of generalization. Many studies document the importance of child choice in regard to responsiveness and engagement (e.g., Carter, 2001; Dunlap, 1994).
Interspersal of Acquisition and Maintenance Tasks
Acquisition tasks are targeted areas the child has not yet learned, and maintenance tasks are tasks the child has already mastered. Research shows that treatment targeting exclusively acquisition tasks results in increased child frustration and task avoidance. However, when previously learned tasks are interspersed with acquisition tasks, children learn faster and exhibit greater enthusiasm, happiness, and interest (Dunlap, 1984).
Task Variation
Closely related to task interspersal is task variation. Instead of repeatedly presenting the same target tasks until mastered, varying the tasks with other activities results in faster learning (Dunlap, 1984; Winterling, Dunlap, & O’Neill, 1987). Such variation, as opposed to massed practice, has similar results to the interspersal of maintenance and acquisition tasks in regard to reducing disruptive behavior and increasing the rapidity of skill acquisition (Winterling et al., 1987).
Consequences
Child choice ties nicely into the presentation of the reinforcer. When items that the child finds enjoyable are used in the intervention, the task becomes inherently rewarding, and the contingent provision of the preferred item is then naturally reinforcing.
Natural Reinforcers
In contrast to providing rewards that are unrelated to the task, reinforcers that are directly and functionally related to the task result in accelerated learning. If the child chooses the activity or item, then it can be provided contingent upon a correct response. Such natural rewards allow the child to more easily understand the response-consequence relationship. It also enhances generalization of skills as the child is likely to request preferred items or activities outside of intervention as well.
Rewarding Attempts
Rather than using a strict-shaping paradigm, common in behavioral intervention, children are rewarded for all genuine attempts. This is especially important for children having difficulty learning first words. When the child’s attempts are rewarded, regardless of how close the pronunciation is to the adult word, the children learn words faster than when each response is equal to or better than the previous (Koegel, O’Dell, & Dunlap, 1988).
The individual components described above were combined into a treatment package that was initially investigated for teaching first words and language to children with ASD. The first study published using this package focused on expressive verbal communication (Koegel et al., 1987). Participants in this early study were young children with autism who were minimally verbal, despite participating in intensive structured ABA programs. However, incorporation of motivational strategies resulted in rapid generalized gains in imitative and spontaneous utterances across all children. This treatment package of motivational procedures (previously called the natural language paradigm or NLP, now called pivotal response treatment) has demonstrated effectiveness in several developmental domains, such as play (Pierce & Schreibman, 1995; Stahmer, 1995), social initiations (Koegel, Carter, & Koegel, 2003), socialization in schools (Robinson, 2011), and academics (Koegel, Singh, & Koegel, 2010). Table 4.2 presents an overview of PRT components and treatment examples for caregivers.
The PRT package has been shown to be more effective than treatment as usual or structured ABA intervention in several single-subject design studies as well as randomized clinical trials (Mohammadzaheri, Koegel, Rezaee, & Rafiee, 2014). Research shows that compared to a traditional ABA format, teaching parents PRT leads to increased positive parent-child interactions, evidenced by increased positive communication style, increased parent happiness and interest, and reduced parent stress (Koegel, Bimbela, & Schreibman, 1996). This is important as stress levels of parents of children with autism are generally exceedingly high (Estes et al., 2009; Moes, Koegel, Schreibman, & Loos, 1992). Reduction of parent stress should be a key ingredient to any parent-implemented intervention and will likely lead to more frequent implementation of treatment strategies. PRT is designed to be play-based, naturalistic, and easily incorporated into daily routines. This ease of implementation along with improvements in affect fits nicely within a transactional model wherein both parents and their children may benefit from each other’s enjoyment, thereby reducing stress.
This leads us to consider the importance of the earliest possible onset of intervention for reducing parent stress, increasing motivation, and improving child communication while ameliorating potentially proliferating difficulties in order to help the child move toward an optimal developmental trajectory. PRT was originally developed as an early intervention for pre- and elementary school-aged children, focusing on improving social communication and motivation following diagnosis. Recently, however, the age of diagnosis has decreased to 18–24 months of age, and community screeners are available to help identify high-risk infants in the first year of life, prior to the full manifestation of ASD symptoms (see Chap. 2). Further, parental concerns about ASD may be present several years prior to a formal diagnosis of ASD, in some cases as early as 4–6 months of age (see Chap. 3; Koegel, Singh, Koegel, Hollingsworth, & Bradshaw, 2013). Other chapters in this section have also presented empirical and theoretical arguments for the critical importance and benefits of supporting families of high-risk infants before a confirmed diagnosis is possible. This work has motivated new research in adapting PRT to enrich social engagement and communication opportunities for high-risk infants in the first 2 years of life. That is, although a formal diagnosis may not occur prior to the point in time when expressive words are expected (around 12–16 months), preliminary research suggests that symptoms of social avoidance, lack of social responsiveness, and reduced social communication can be addressed (see Bradshaw, Steiner, Gengoux, & Koegel, 2015, for review). As such, families and interventionists can work together to intervene at the earliest possible time to improve the infant’s developmental trajectory.
For example, social communication and play are among the building blocks for later-developing, more sophisticated language and social skills. Social engagement emerges at as young as 2 months of age when infants begin to exhibit reciprocal social smiling with caregivers. This behavior sets off a cascade of mutually reinforcing social interactions that develop into a social-communicative repertoire consisting of gaze shifting, gestures, and language. In contrast, infants and toddlers with ASD do not show this typical trajectory of social-communicative development. Prospective and retrospective studies of infants later diagnosed with ASD have identified infant behaviors and behavioral symptoms between 6 and 24 months of age that deviate significantly from those of typically developing infants (e.g., Baranek, 1999; Clifford & Dissanayake, 2008; Macari et al., 2012; Maestro et al., 2002; Osterling & Dawson, 1994; Ozonoff et al., 2010; Shic, Macari, & Chawarska, 2014; Watson, Crais, Baranek, Dykstra, & Wilson, 2013; Werner, Dawson, Osterling, & Dinno, 2000). By 9–12 months of age, infants with ASD may exhibit an increasing number of behavioral atypicalities, including reduced eye contact, failure to orient to name, reduced social smiling, abnormal affect, fewer gestures, lower activity levels, and longer duration orienting to objects (see Boyd, Odom, Humphreys, & Sam, 2010, and Zwaigenbaum et al., 2005, for review). Overall, research to date has documented early prodromal features of ASD in infancy and suggests that these behaviors intensify in the second year of life. Thus, earlier onset of intervention is related to improved developmental trajectories for infants with ASD (Rogers et al., 2012), and treatment during the first year of life may be pivotal for optimal outcomes (Koegel, Koegel, Ashbaugh, & Bradshaw, 2014).
Adapting Pivotal Response Treatment to Support Families Before Diagnosis
Consider the social-communicative profile for typically developing infants during the first year of life. The emergence of social referencing includes the use of eye gaze, facial expression, and gestures for the purpose of sharing and requesting. Babbling transforms into functional vocalizations and primitive word approximations. A direct application of the original PRT strategies that focused on teaching first words (Koegel et al., 1987) and language (Koegel, Koegel, & Surratt, 1992) would not be completely appropriate for prelinguistic infants in the first year. However specific PRT components that have been shown to improve motivation by using a classical conditioning paradigm in the natural environment may be well-suited for treatment of infants beginning to demonstrate a lack of social engagement and social-communicative difficulties. In this context, foundational skills that provide a scaffold for first words and language development, such as eye contact, gestures, and intentional vocalizations, can be addressed. While the treatment targets are different for PRT with infants, the theoretical foundation and motivational principles central to PRT remain the same. Developmental considerations for adapting parent-implemented PRT for use with infants are described below.
Social Motivation
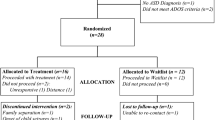
Socialization and language difficulties are among the core deficits of individuals with ASD. The motivational strategies of PRT, as described above, provide a practical framework that allows for a sustained, enjoyable parent-child interaction, while behavioral strategies serve to provide appropriate opportunities for communication and reinforcement. The adaptation of pivotal response treatment for use with infants is an organic extension given its naturalistic methodology and focus on motivation. Some researchers have postulated that social motivation is at the core of social deficits observed in individuals with ASD (Dawson, 2008; Koegel, Valdez-Menchaca, & Koegel, 1994). From a developmental perspective, this decreased social motivation may stem from, or at least manifest as, diminished interest in social interactions in infancy. Early parent-infant social interactions provide the necessary context for language learning, and decreased attention and interest in social interactions in infancy could have a critical impact on social-communicative development (Bradshaw, 2015). In the first 6 months of life, infants with typical social development enjoy face-to-face interactions with a caregiver. Around 6 months, infants become increasingly object-focused and gradually choose to engage in triadic interactions in which they shift gaze between objects and a caregiver (Bakeman & Adamson, 1984). Early referential exchanges allow caregivers to label objects and engage in a language- and object-embedded social interaction. These socially motivated joint attention episodes provide a context for promoting language development (see Mundy & Newell, 2007). Thus, PRT for infants in the first year of life focuses on increasing motivation to engage in a social interaction with a caregiver. We hypothesize that increasing attention to caregivers as well as positive affect during parent-infant interactions will create an inherently more reinforcing exchange that will improve social motivation and generate widespread gains in social communication in the first years of life (Fig. 4.1).

Theoretical model for targeting social engagement in infancy. PRT strategies work to create more motivating social interactions for infants. As infants become more socially motivated, and thus prefer to engage in social interactions, they will spend more time attending to social features in the environment, which will increase learning opportunities embedded in social interactions and ultimately improve social-communicative skills
Treatment Targets
As mentioned previously, social-communicative abilities are just emerging in the first years of life. An infant’s communicative repertoire consists primarily of nonverbal behaviors such as gestures, facial expression, and eye gaze, as well as communicative vocalizations and word approximations. An initial assessment of the infant’s current social-communicative functioning using standardized assessment can determine delays compared to established norms of chronologically age-matched peers. Such assessments might include the Communication and Symbolic Behavior Scales (CSBS : Wetherby & Prizant, 2002), Mullen Scales of Early Learning (Mullen, 1995), Bayley Scales of Infant Development (Bayley, 2006), and MacArthur Communicative Development Inventory (Fenson et al., 1993). Additional assessments provide quantitative information about frequency and quality of social-communicative behaviors as well as ASD symptoms: the Early Social Communication Scales (ESCS : Mundy et al., 2003); the Autism Diagnostic Observation Schedule, Toddler Module (ADOS: Rutter, DiLavore, Risi, Gotham, & Bishop, 2012); and the Autism Observation Scale for Infants (AOSI : Bryson, Zwaigenbaum, McDermott, Rombough, & Brian, 2008). For younger infants who exhibit variability in behavior, gathering observational data over a period of several days or weeks can be helpful in determining stability of perceived deficits (Bradshaw, Koegel, & Koegel, 2012). Treatment targets should then be selected considering both the child’s developmental skill level and chronological age. For example, 24-month-old infants should be engaging in pretend play and saying two- to four-word phrases. If a 24-month-infant with or at risk for ASD is exhibiting cause-and-effect play and is not communicating using vocalizations or gestures, treatment should be modified appropriately; treatment targets might include simple functional play and communication using gestures and intentional vocalizations. A focus on developmental precursors supports the emergence of skills and enhances developmental gains. For example, the development of initiating joint attention, a skill that occurs developmentally earlier than expressive verbal communication, is associated with advanced language skills in children with and without ASD (e.g., Mundy, Sigman, & Kasari, 1990). Similarly, treatment for infants younger than 12 months might include social engagement and heightened positive affect during face-to-face play, as social smiling has been associated with enhanced social responsivity and social initiations (Bradshaw, 2015; Parlade et al., 2009).
Self-Regulation
Infants have fewer capacities to self-regulate and often require caregiver support to assist in self-soothing. For example, infants in the first year of life show less awareness of social or task demands, and social exchanges are grounded in immediate motivations and perceptual stimuli, whereas 12- to 18-month-olds regulate their physical and emotional state based on social context (Kopp, 1982). In contrast, cognitive achievements of representational thinking and recall memory allow for self-control, observed through active behavioral compliance, by 2 years of age (Kopp, 1982). An understanding of the neurobehavioral organization of the infant informs approach to treatment in the first years of life. Intensity should be adjusted appropriately, and physiological state (e.g., sleepy, fussy) must be weighed more heavily than older children in decisions about treatment implementation. This is well suited for the naturalistic approach of PRT in which treatment can (and should) be implemented by caregivers on an ongoing basis and throughout daily routines. Parents should also be taught how to read their infant’s cues related to behavioral state so as to provide a maximally positive and reinforcing social interaction. An infant’s capacity to learn and respond is significantly related to behavioral state, and so intervention for younger infants should be implemented during appropriate times (Wolff, 1987). Although optimally motivating social interactions are encouraged, breaks in social interaction should be provided as necessary to maintain an optimal state for learning.
Parent Education and Coaching
Parent education is a critical piece of PRT for young children and infants with or at risk for ASD. The importance of implementation throughout daily routines and activities, the need for continued support in social-communicative skills, and developmentally appropriate stranger anxiety in young infants implore a parent-education and parent-implementation model. Research has shown that parents can master the motivational strategies of PRT and incorporate them into daily routines with a 5-day, 25 h parent-education program (Koegel, Symon, & Koegel, 2002). These gains proved to be long-lasting for at least up to 1 year post-intervention. Importantly, parents were also observed to exhibit more positive affect and interest when interacting with their children and also showed reductions in (untargeted) stress. A follow-up study showed that parents who learned PRT through this brief, high-intensity training program were able to train other significant caregivers to fidelity in the implementation of PRT with their child (Symon, 2005). Parent education has also been shown to be effective in improving language across contexts for parents of minimally verbal children with ASD younger than 3 years old (Koegel, Bruinsma, & Koegel, 2006; Bradshaw, Koegel, & Koegel, 2017). These studies showed improvements in the number of words produced expressively and vocabulary diversity from pre- to post-intervention during naturalistic language samples. Across all children, expressive language improvements ranged from 16 to 200 total words uttered with some children using 3–93 unique words. Additionally, parents corroborated the positive outcomes, reporting large increases in functional expressive words their children produced on the Vineland Adaptive Behavior Scales, Communication Domain (Sparrow, Cicchetti, & Balla, 2005). The feasibility and effectiveness of PRT parent-education programs have been independently replicated at other sites, outside of the original development research laboratories of PRT (e.g., Coolican, Smith, & Bryson, 2010). Group parent training of PRT has also been developed, demonstrating significant improvements in parent fidelity of implementation and child expressive language after 10 weeks (Gengoux et al., 2015; Minjarez, Williams, Mercier, & Hardan, 2011). Together, this research suggests that the motivational and behavioral strategies of PRT are feasible for parents to learn and train others in a relatively brief period of time and are effective for improving social communication in young children with ASD.
Research has also examined specific features of parent-education programs that decrease parent stress and enhance parent satisfaction and gains. Steiner (2011) examined the effect of a strength-based approach to parent training, which compared deficit-based statements to strength-based statements during coaching sessions. During the strength-based condition, the interventionist made statements that highlighted the child’s strengths, for example, “It seems like he has a lot of interests, that’s a good sign. One way to get his attention is...” This was compared to the deficit condition in which statements were made related to the child’s area of weakness, such as “It seems like it is hard to get his attention. One way to get his attention is...” Results demonstrated that the strength-based approach improved parent affect and enhanced parent-child interactions during parent coaching sessions not only compared to the deficit-based approach but also compared to pre-treatment interactions. Importantly, this suggests that parent-implemented intervention using a strength-based approach during feedback sessions may effectively help decrease, rather than induce, parent stress.
Modifications of PRT parent training can also lead to enhanced gains in socialization. For instance, Vernon, Koegel, Dauterman, and Stolen (2012) extended the motivational concept of child choice by embedding a social component into the child’s interests throughout intervention. In a traditional PRT paradigm for a child whose preferred activities included jumping on a trampoline, the child would be reinforced for saying the word “jump” by allowing her to jump on a trampoline. Using the socially embedded PRT paradigm, a social component would be embedded within the reinforcement, so the adult may jump with the child on the trampoline. In this way, the reinforcement comes from the adult jumping with the child rather than the trampoline itself, making social interaction a part of the preferred activity. Results of this study showed rapid gains in both parent acquisition of the teaching procedures and child behaviors. As expected in traditional and socially embedded PRT frameworks, all children showed substantial improvements in verbal initiations. Additionally, children in socially embedded PRT spent greater proportions of time making eye contact with their caregiver and showing positive affect. Moreover, parent-child interactions drastically improved in respect to increased synchronous engagement as well as parent positive affect.
Strategies for Parent Coaching
Introduction of the Topic
Sessions can begin with a check-in about the previous week, questions about concepts learned thus far, specific problem areas related to implementation of PRT strategies, and gains the child has made. Praise for caregivers should be provided for any examples of implementing the procedures or generating creative ideas for eliciting communication from their child. Attempts should be made to incorporate any problem areas or questions into the session for that day. PRT strategies can be explained to the parent with the child playing nearby while providing examples specific to their child. For example, a clinician introduction to child choice might be “Right now, Jackson is playing with the animal puzzle and it’s great that he’s so interested in the pieces. It also looks like instead of putting the puzzle pieces in, he prefers stacking the puzzle pieces and knocking them down. We can follow his lead by joining in his play and helping him stack and knock them down, and we can even have him make a vocalization or word attempt before he stacks every third puzzle piece. If we instead try to get him to put the pieces in the puzzle board, this would not be following his lead.” This initial introduction of the PRT strategy can remain relatively brief followed by clinician modeling where the clinician models how to use the strategy of child choice with Jackson.
Modeling
As the clinician models the strategy, she can provide narration of her actions and explain rationale for particular decisions. For example, “So I’m joining him in stacking the pieces, making sure to not be too intrusive and not interrupting his play, but still making sure that he exhibits the target behavior of using expressive words. You see that I first tried to knock down the tower too early. I knocked it down before all the pieces were stacked and he seemed to get a little frustrated with me. I’m glad he communicated his frustration and it is great that he is still sticking with the activity! So now I’m going to continue to follow his lead by allowing him to stack all the pieces before knocking over the tower. This is great because we have more opportunities to have him try and talk for the pieces. We will discuss at a later session how to make his play a little bit more flexible. But right now, let’s just focus on following his lead.” The clinician here is using several skills that deserve mention. First, she acknowledged that she had made a mistake in following the child’s lead, highlighting that even expert clinicians can misread child cues and cause frustration. Second, she utilized a strength-based approach by commending his interest in the puzzle, reframing his frustration as a method of communication, and praising his maintenance of motivation to engage in the activity. The clinician then ended with a reminder of the topic for the day – child choice.
Listening to Parent Concerns
The clinician might then incorporate some of the parent’s concerns into the topic for that day. For example, “You mentioned that Jackson had a hard time when you joined his play this week and would often choose to play something else. Why don’t we try to make this interaction more motivating for the both of you by adding a fun element to the animal puzzle? I’ve seen him enjoy animal books before when you make the animal noises, which is fantastic. Why don’t you try incorporating some of the animal noises, which he loves, into this puzzle game? Since he is already making verbal attempts to name many of the items, this would be a nice way to add to his repertoire of words.” At this point, the clinician would encourage the parent to try using the child choice strategy, while the clinician observes and provides feedback. We think of parent education as a practice-with-feedback process rather than learning through didactics, and so the rest of the session is spent interweaving practice, feedback, modeling, and discussion. The session then ends with a summary of the topic, a few statements about what the parent and child did well in the session, instructions for what to practice in the upcoming week, and troubleshooting as necessary.
Implementation of PRT for Families with High-Risk Infants
Preliminary research suggests that beginning intervention in the first year or two of life, when social engagement and social-communicative challenges are just emerging, can have a greater impact on prognosis and developmental outcome (Koegel, 2000; Rogers et al., 2012). Several studies have documented how parent implementation of PRT strategies for toddlers with ASD can lead to rapid and widespread gains. Implementation of parent-mediated interventions for high-risk infants, however, carries unique challenges. These challenges have been addressed in previous chapters, so here we focus on how pivotal response treatment is especially suited for parent-implemented intervention in infancy and present examples of how it can be implemented for 6- to 24-month-old high-risk infants to increase social engagement, improve nonverbal and verbal expressive communication, and decrease autism symptomology. The remainder of this chapter will provide strategies and examples for how to adapt PRT for use with high-risk infants, based on both chronological age and developmental level. We start with using PRT to teach first words to older infants (15–24 months) who are already showing basic nonverbal communicative attempts but who have yet to use consistent verbal communication (Bradshaw, Koegel, & Koegel, 2017). We then describe modifications made to PRT for improving nonverbal intentional communication, such as eye contact and gestures, for infants who are not yet exhibiting any social-communicative attempts. And finally, we describe how to use motivational PRT strategies to promote positive social engagement for our youngest infants between 6 and 9 months old. Examples of essential PRT strategies for promoting social engagement and communication in high-risk infants are displayed in Tables 4.3 and 4.4.
PRT Strategies for Teaching High-Risk Infants’ First Words
PRT strategies for improving verbal communication in high-risk infants in the second year of life require few modifications from the traditional PRT paradigm and use the fundamental PRT structure of providing a language opportunity, waiting for a response, and reinforcing the desired behavior (Bradshaw, Koegel, & Koegel, 2017; Bradshaw, Steiner, et al., 2015; Steiner, Gengoux, Klin, & Chawarska, 2013).
Provide a Language Opportunity
Caregivers can easily embed infant-preferred activities and provide communication opportunities throughout daily routines and during play. Caregivers can wait to give their infant a highly preferred item until he or she provides some indication of intentional communication. Providing opportunities can be an easy part of any household activity by simply placing highly preferred items “in sight, out of reach” so the child has more opportunities to communicate, for example, placing a favorite toy on a high shelf or a favorite snack in a tightly sealed, clear container. However, verbal prompting for a language attempt may not be the most effective way to teach older infants their first words. In more challenging cases, verbal routines during motivating activities can work especially well. Common verbal routines include “ready, set...go” or “one, two...three.” A caregiver can provide an opportunity by first modeling the entire verbal routine and then pausing in anticipation of the last part of the routine as in “ready, set....” This rhythmic strategy builds behavioral momentum during a highly motivating activity. Similar strategies can be used with favorite songs or animal sounds. Many children with ASD begin to communicate when their parent pauses in the middle of singing a favorite song. For example, a caregiver can start singing “twinkle, twinkle, little...” and then pause so that the infant can continue with an approximation of the word “star” or any vocalization at all.
Provide Natural Contingent Reinforcement
Natural reinforcement involves a direct and natural relation between language and reinforcement. If the child’s motivating activity is getting tickled, a caregiver could reinforce any attempt of the word “tickle” by tickling contingently following the child’s response. This direct relation between the infant’s communicative attempt and reinforcement also promotes skill generalization.
Reinforce Attempts
Communication emerges gradually. At 12–18 months, we do not expect infants to say their first word perfectly, and so we do not expect infants and toddlers with or at risk for ASD to say their first words perfectly either. In fact, caregivers and clinicians may first focus on intentional communication rather than accurate or precise utterances. For example, when a child reaches for her doll and says “ah,” a caregiver can model the correct form of the word “doll” while immediately reinforcing the communication attempt by handing her the doll. Prompting the child for the correct word “doll” and waiting for a more accurate response runs the risk of losing the child’s motivation to communicate.
Supporting Families to Improve Nonverbal Intentional Communication in High-Risk Infants
Prior to saying first words, infants exhibit prelinguistic intentional communication, including sharing enjoyment by looking from an object to the caregiver or pointing to an object of interest. These nonverbal communication skills begin to emerge between 9 and 12 months, and high-risk infants have been reported to exhibit diminished quantity and quality of nonverbal communication. Pivotal response treatment has also been adapted to improve prelinguistic intentional communication in high-risk infants (e.g., Steiner et al., 2013). The following modified PRT strategies can be taught to parents of high-risk infants who are not yet exhibiting intentional communication: child choice, clear opportunities, interspersal of maintenance and acquisition tasks, immediate and contingent reinforcement, natural reinforcement, and reinforcing attempts. In contrast to traditional PRT models in which verbal communication is the primary focus of intervention, PRT can be adapted to target prelinguistic forms of social communication for infants as young as 12 months old, such as pointing, giving, showing, and other gestures.
As in traditional PRT, intervention is implemented during infant-preferred activities and tasks, such as peekaboo with a blanket. Clear opportunities are provided by first engaging the child in a highly engaging routine. For example, a caregiver may build a routine with the following sequence: (1) caregiver places the blanket over the child and says “Where’s Abby? Where is she? I think I see her…”; (2) caregiver pulls off the blanket, places the blanket on the ground, and says “peekaboo!” followed by tickling; and (3) caregiver says “let’s play again!” This routine has an easily identifiable beginning and end, which helps to build anticipation and maintain engagement but also serves as a clear opportunity for the infant to initiate a communicative attempt: the activity has suddenly stopped and the blanket is on the floor, leaving the infant to vocalize, gesture (give or point), or shift gaze from the blanket to the caregiver in order to continue the interaction. It also incorporates a rewarding social interaction, while also using an object (blanket) that can be used to teach a giving gesture.
As in verbal language, prompting strategies can be used if the infant is not yet demonstrating a target behavior, such as a give gesture. In their study of adapting PRT for high-risk 12-month-old infants, Steiner et al. (2013) utilized prompts that were organized into a hierarchy such that a physical prompt was the highest level (most supportive), followed by a model prompt , and an open-ended prompt at the lowest level (least supportive). Using this method, if a behavior is difficult to elicit, a clinician, or second caregiver, may begin with the most supportive prompt – physical prompting. In our blanket peekaboo example, a parent coach or second caregiver may sit behind the infant and physically prompt Abby using the give gesture by putting the blanket in Abby’s hand and guiding her hand toward her mother. This, of course, would be immediately followed by the caregiver putting the blanket over Abby and reinitiating the peekaboo routine in order to reinforce the “give” gesture. Moving up in the prompt hierarchy, model prompts are defined as the parent modeling the target behavior, for example, demonstrating a point to elicit a point from the infant or saying “more” to elicit an infant vocalization. Finally, the least supportive prompt is the open-ended prompt in which a parent would elicit a response from the infant without modeling, for example, asking, “What do you want?”
It is beneficial to create opportunities for activities in which the caregiver or clinician can easily join into the activity and engage with the infant. For example, some infants can become overly fixated on cause-and-effect objects, e.g., a toy telephone, in which interruption of the activity for the purpose of presenting a communication opportunity may elicit frustration. Clinicians and parents may choose to avoid such activities. Additionally, infants in early intervention may not have developed functional play, and so clinicians and caregivers may choose to incorporate learning opportunities into activities that involve food or physical play (e.g., tickling). Early learners can become easily frustrated with continued presentation of difficult tasks, and thus it is important to intersperse easy, already-mastered tasks, with new, more difficult tasks. For example, if an infant consistently gives objects to a caregiver to request but only occasionally pairs this behavior with eye contact, a caregiver might wait for the integration of these two behaviors once every five to seven trials.
Supporting Families to Improve Social Engagement in Very Young Infants
In the first year of life, infants engage in reciprocal, highly affective face-to-face dyadic interactions with a caregiver. These very early social interactions are critical for learning social contingencies, developing effective self-regulation, and acquiring later communicative competencies (Feldman, 2007). In an effort to address parental concerns about a lack of infant social responsivity and social engagement early in life, we have adapted PRT strategies to focus on improving positive social engagement during face-to-face play for very young high-risk infants. The larger developmental domain addressed is social engagement, and potential target behaviors to focus on include increasing the frequency of social smiling and eye contact during the interaction. PRT for very young infants focuses on improving positive affect and eye gaze during face-to-face play with a caregiver and incorporates three key motivational strategies adapted from the traditional PRT paradigm: child choice, task variation, and interspersal of neutral and preferred activities.
Child Choice
Child choice refers to incorporating activities or items that are motivating to the child, or infant in this case. Infant-preferred activities are identified through systematic evaluation of the infant’s interest and affect during parent-infant interactions. A clinician observes multiple parent-infant interactions in which the parent is utilizing multiple activities and strategies to try and engage their infant. These simple observations of the infant’s play preferences in a naturalistic setting can illuminate the contexts in which he or she will be most motivated to interact. Each activity is then categorized as preferred, activities in which the infant exhibits indications of enjoyment such as high positive affect and eye contact; neutral, activities in which the infant appears to passively accept the activity without indication of wanting the interaction to continue or cease; or not preferred, activities in which the infant exhibits dislike for the activity such as gaze aversion combined with negative affect. Although infants use gaze aversion to self-regulate their arousal during highly stimulating activities, gaze aversion accompanied with negative affect likely reflects a non-preferred activity. In our research with high-risk infants exhibiting very early concern for ASD, these initial assessments of parent-infant interactions revealed that the motivational property of the interaction appeared to be constrained by specific activities rather than generalized to social interactions, in contrast to typically developing infants who exhibit consistently positive social affect with their caregiver regardless of activity. The goal of PRT for very young high-risk infants therefore is to expand their social engagement to a variety of social activities with their caregiver, thus potentially transferring their activity-centered engagement to a social-centered engagement.
Task Variation
During parent-infant interactions, parents are taught how to read their infants’ cues and vary the activity frequently, thus consistently providing novel activities and maintaining social engagement. Although looking away during social interaction serves as a self-regulatory behavior for young infants, potential cues for infant social disengagement included prolonged looking away accompanied with negative affect and a trend of decreasing affect over several seconds. Thus, varying the enjoyable activities before the infant satiates is important.
Reinforcement
To increase social motivation in such young infants, this intervention relies on a classical conditioning paradigm in which parents become the preferred activity. This is in contrast to a traditional operant conditioning paradigm in which natural reinforcers are provided contingent upon appropriate communicative responding. Again, the goal here is to make the parent and the social interaction as reinforcing as possible and to condition the child to associate the parents’ interactions with the positive and enjoyable activities.
Intersperse Acquisition and Maintenance Activities
Once an infant is exhibiting high levels of social engagement, including making eye contact and smiling, throughout the preferred activities for three consecutive sessions, neutral activities are incorporated. That is, the activities that had previously been considered neutral are gradually and systematically incorporated into the rotation of the preferred play activities. As the infant begins to demonstrate improved affect with the neutral activity, another is added, and so on, until all of the parent-infant activities that were presented in the initial assessment period are incorporated into play. An emphasis on reading infant cues and providing highly rewarding activities will help to improve the parent’s understanding of his or her infant’s individual preferences and communicative style, thus increasing the likelihood of increasingly contingent and rewarding social interactions for at-risk infants and their parents.
Summary
The overarching goal in adapting parent-implemented PRT for high-risk infants before an ASD diagnosis is to help caregivers understand typical social-communicative development, discern concerning behaviors, and learn basic motivational and behavioral strategies for improving social engagement and communication. It should be noted that infant behaviors can be unstable in the first year of life and vary greatly. Assessing for stable patterns of difficulties with socialization is important, so that other natural environmental factors (such as fatigue) are not erroneously evaluated as an at-risk symptom. However, a strength of beginning intervention during infancy is that the interventions are not as labor intensive as those needed in the preschool years and beyond. Emerging studies suggest that parents can be taught strategies in a relatively short period of time and that the bulk of the intervention hours can be implemented by parents throughout the infant’s waking hours. This cost and time efficiency supports the use of adapting interventions for families with high-risk infants. Although teaching first words and language has historically been among the first steps in using PRT for young children with ASD, this target seems inappropriate for high-risk infants younger than 12 months who do not yet have a diagnosis and may be inappropriate for older infants who are not yet demonstrating prelinguistic communication. In adapting PRT for high-risk infants, we had to develop new, appropriate target areas for young infants and early learners. We found that working to improve the positive affect and social attention during social interactions, as well as teaching nonverbal intentional communication, led to observable gains and parent satisfaction. The core theoretical underpinning of PRT – to improve social motivation – remains the same in working with high-risk infants, but the strategies and intervention goals are slightly modified to address developmental stage.
The transition from working with children with a diagnosis of ASD to teaching PRT to parents of high-risk infants carries unique challenges. For example, learning that an infant is at risk for social-communicative impairments can induce parent stress and anxiety, and clinicians should be provided tools to help reduce parental anxiety while promoting self-efficacy and confidence. Research suggests that interventions, such as PRT, that can be implemented during play and daily routines reduce parent stress when compared to other strategies that require the parent to take time out of the day to implement drill-type activities (Koegel et al., 1996). Although clinician-parent alliances are important in all forms of parent-mediated interventions, we have learned that this is an especially important aspect of adapting PRT for high-risk infants. Given the high levels of stress accompanied with uncertainty of their infant’s outcome, clinicians who are compassionate while also focusing on parent coaching of PRT procedures are most successful. Further, outcomes will be improved if parents are considered as valuable and important team members when developing goals and implementing intervention programs (Brookman-Frazee & Koegel, 2004). Parents should be both recognized and respected as experts relating to their own infant. As well, families’ cultural and socioeconomic variables and values should be considered during parent-education programs (Baker & George, 2013; Santarelli, Koegel, Casas, & Koegel, 2001). Consistent recognition and celebration of parent and infant strengths are essential for creating a positive environment and promoting optimal learning and development (Steiner, Koegel, Koegel, & Ence, 2012).
References
Bakeman, R., & Adamson, L. B. (1984). Coordinating attention to people and objects in mother-infant and peer-infant interaction. Child Development, 55, 1278–1289.
Baker, C., & George, A. (2013). Positive behavior supports and multicultural concerns. Journal of Border Educational Research, 7(1), 127–132.
Baranek, G. T. (1999). Autism during infancy: A retrospective video analysis of sensory-motor and social behaviors at 9–12 months of age. Journal of Autism and Developmental Disorders, 29(3), 213–224.
Bayley, N. (2006). Bayley scales of infant and toddler development: Bayley-III. Harcourt Assessment, Psych. Corporation.
Boyd, B. A., Odom, S. L., Humphreys, B. P., & Sam, A. M. (2010). Infants and toddlers with autism spectrum disorder: Early identification and early intervention. Journal of Early Intervention, 32(2), 75–98.
Bradshaw, J., Koegel, L., & Koegel, R. (2012). Assessment and improvement of social engagement and communication in infancy. International Meeting for Autism Research 2012. Toronto, ON.
Bradshaw, J. (2015). Clinical Correlates of Social Affect in Early Infancy: Implications for Early Identification of Autism Spectrum Disorder. (Doctoral dissertation). University of California, Santa Barbara, Santa Barbara, CA.
Bradshaw, J., Steiner, A. M., Gengoux, G., & Koegel, L. K. (2015). Feasibility and effectiveness of very early intervention for infants at-risk for autism spectrum disorder: A systematic review. Journal of Autism and Developmental Disorders, 45(3), 778–794.
Bradshaw, J., Koegel, L. K., Koegel, R. L. (2017) Improving Functional Language and Social Motivation with a Parent-Mediated Intervention for Toddlers with Autism Spectrum Disorder. Journal of Autism and Developmental Disorders 47(8):2443–2458.
Brookman-Frazee, L., & Koegel, R. L. (2004). Using parent/clinician partnerships in parent education programs for children with autism. Journal of Positive Behavior Interventions, 6(4), 195–213.
Bryson, S. E., Zwaigenbaum, L., McDermott, C., Rombough, V., & Brian, J. (2008). The autism observation scale for infants: Scale development and reliability data. Journal of Autism and Developmental Disorders, 38(4), 731–738.
Carter, C. M. (2001). Using choice with game play to increase language skills and interactive behaviors in children with autism. Journal of Positive Behavior Interventions, 3(3), 131–151.
Clifford, S. M., & Dissanayake, C. (2008). The early development of joint attention in infants with autistic disorder using home video observations and parental interview. Journal of Autism and Developmental Disorders, 38(5), 791–805.
Coolican, J., Smith, I. M., & Bryson, S. E. (2010). Brief parent training in pivotal response treatment for preschoolers with autism. Journal of Child Psychology and Psychiatry, 51(12), 1321–1330.
Dawson, G. (2008). Early behavioral intervention, brain plasticity, and the prevention of autism spectrum disorder. Development and Psychopathology, 20(03), 775–803.
Dunlap, G. (1984). The influence of task variation and maintenance tasks on the learning and affect of autistic children. Journal of Experimental Child Psychology, 37(1), 41–64.
Dunlap, G. (1994). Choice making to promote adaptive behavior for students with emotional and behavioral challenges. Journal of Applied Behavior Analysis, 27(3), 505.
Estes, A., Munson, J., Dawson, G., Koehler, E., Zhou, X. H., & Abbott, R. (2009). Parenting stress and psychological functioning among mothers of preschool children with autism and developmental delay. Autism, 13(4), 375–387.
Feldman, R. (2007). Parent–infant synchrony and the construction of shared timing; physiological precursors, developmental outcomes, and risk conditions. Journal of Child Psychology and Psychiatry, 48(3–4), 329–354.
Fenson, L., Dale, P. S., Reznick, J. S., Thal, D., Bates, E., Hartung, J. P., … Reilly, J. S. (1993). The MacArthur communicative development inventories: Users guide and technical manual. Baltimore, MD: Paul Brookes.
Gengoux, G. W., Berquist, K. L., Salzman, E., Schapp, S., Phillips, J. M., Frazier, T. W., … Hardan, A. Y. (2015). Pivotal response treatment parent training for autism: Findings from a 3-month follow-up evaluation. Journal of Autism and Developmental Disorders, 45, 1–10.
Koegel, L. K. (2000). Interventions to facilitate communication in autism. Journal of Autism and Developmental Disorders, 30(5), 383–391.
Koegel, L. K., Carter, C. M., & Koegel, R. L. (2003). Teaching children with autism self-initiations as a pivotal response. Topics in Language Disorders, 23(2), 134–145.
Koegel, L. K., Koegel, R. L., Ashbaugh, K., & Bradshaw, J. (2014). The importance of early identification and intervention for children with or at risk for autism spectrum disorders. International Journal of Speech-Language Pathology, 16(1), 50–56.
Koegel, L. K., Koegel, R. L., Harrower, J. K., & Carter, C. M. (1999). Pivotal response intervention I: Overview of approach. The Journal of the Association for Persons with Severe Handicaps., 24(3), 174–186.
Koegel, L. K., Singh, A., & Koegel, R. (2010). Improving motivation for academics in children with autism. Journal of Autism and Developmental Disorders, 40(9), 1057–1066.
Koegel, L. K., Singh, A. K., Koegel, R. L., Hollingsworth, J. R., & Bradshaw, J. (2013). Assessing and improving early social engagement in infants. Journal of Positive Behavior Interventions, 16(2), 69–80.
Koegel, L. K., Valdez-Menchaca, M. C., & Koegel, R. L. (1994). Autism: Social communication difficulties and related behaviors. In Advanced abnormal psychology (pp. 165–187). New York, NY: Springer.
Koegel, R. L., Bimbela, A., & Schreibman, L. (1996). Collateral effects of parent training on family interactions. Journal of Autism and Developmental Disorders, 26(3), 347–359.
Koegel, R. L., Bruinsma, Y., & Koegel, L. K. (2006). Developmental trajectories in early intervention. In R. Koegel & L. Koegel (Eds.), Pivotal response treatments for autism: Communication, social, and academic development (pp. 131–140). Baltimore, MD: Brookes Publishing Co.
Koegel, R. L., & Egel, A. L. (1979). Motivating autistic children. Journal of Abnormal Psychology, 88(4), 418.
Koegel, R. L., Glahn, T. J., & Nieminen, G. S. (1978). Generalization of parent-training results. Journal of Applied Behavior Analysis, 11(1), 95–109.
Koegel, R. L., & Koegel, L. K. (1995). Teaching children with autism: Strategies for initiating positive interactions and improving learning opportunities. Baltimore, MD: Paul H Brookes Publishing.
Koegel, R. L., Koegel, L. K., & Surratt, A. (1992). Language intervention and disruptive behavior in preschool children with autism. Journal of Autism and Developmental Disorders, 22(2), 141–153.
Koegel, R. L., O’Dell, M., & Dunlap, G. (1988). Producing speech use in nonverbal autistic children by reinforcing attempts. Journal of Autism and Developmental Disorders, 18(4), 525–538.
Koegel, R. L., O’Dell, M. C., & Koegel, L. K. (1987). A natural language teaching paradigm for nonverbal autistic children. Journal of Autism and Developmental Disorders, 17(2), 187–200.
Koegel, R. L., Symon, J. B., & Koegel, L. K. (2002). Parent education for families of children with autism living in geographically distant areas. Journal of Positive Behavior Interventions, 4(2), 88–103.
Kopp, C. B. (1982). Antecedents of self-regulation: A developmental perspective. Developmental Psychology, 18(2), 199.
Lovaas, O. I. (1977). The autistic child: Language development through behavior modification. New York, NY: Irvington.
Lovaas, O. I., Koegel, R., Simmons, J. Q., & Long, J. S. (1973). Some generalization and follow-up measures on autistic children in behavior therapy. Journal of Applied Behavior Analysis, 6(1), 131.
Lovaas, O. I., Schreibman, L., & Koegel, R. L. (1974). A behavior modification approach to the treatment of autistic children. Journal of Autism and Childhood Schizophrenia, 4(2), 111–129.
Macari, S. L., Campbell, D., Gengoux, G. W., Saulnier, C. A., Klin, A. J., & Chawarska, K. (2012). Predicting developmental status from 12 to 24 months in infants at risk for autism spectrum disorder: A preliminary report. Journal of Autism and Developmental Disorders, 42(12), 2636–2647.
Maestro, S., Muratori, F., Cavallaro, M. C., Pei, F., Stern, D., Golse, B., & Palacio-Espasa, F. (2002). Attentional skills during the first 6 months of age in autism spectrum disorder. Journal of the American Academy of Child & Adolescent Psychiatry, 41(10), 1239–1245.
Minjarez, M. B., Williams, S. E., Mercier, E. M., & Hardan, A. Y. (2011). Pivotal response group treatment program for parents of children with autism. Journal of Autism and Developmental Disorders, 41(1), 92–101.
Moes, D., Koegel, R. L., Schreibman, L., & Loos, L. M. (1992). Stress profiles for mothers and fathers of children with autism. Psychological Reports, 71(3f), 1272–1274.
Mohammadzaheri, F., Koegel, L. K., Rezaee, M., & Rafiee, S. M. (2014). A randomized clinical trial comparison between pivotal response treatment (PRT) and structured applied behavior analysis (ABA) intervention for children with autism. Journal of Autism and Developmental Disorders, 44, 1–9.
Mundy, P., & Newell, L. (2007). Attention, joint attention, and social cognition. Current Directions in Psychological Science, 16(5), 269–274.
Mullen, E. M. (1995). Mullen scales of early learning. Circle Pines, MN: American Guidance Service.
Mundy, P., Delgado, C., Block, J., Venezia, M., Hogan, A., & Seibert, J. (2003). Early social communication scales (ESCS). Coral Gables, FL: University of Miami.
Mundy, P., Sigman, M., & Kasari, C. (1990). A longitudinal study of joint attention and language development in autistic children. Journal of Autism and Developmental Disorders, 20(1), 115–128.
Osterling, J., & Dawson, G. (1994). Early recognition of children with autism: A study of first birthday home videotapes. Journal of Autism and Developmental Disorders, 24(3), 247–257.
Ozonoff, S., Iosif, A. M., Baguio, F., Cook, I. C., Hill, M. M., Hutman, T., … Young, G. S. (2010). A prospective study of the emergence of early behavioral signs of autism. Journal of the American Academy of Child & Adolescent Psychiatry, 49(3), 256–266.
Parlade, M. V., Messinger, D. S., Delgado, C. E., Kaiser, M. Y., Van Hecke, A. V., & Mundy, P. C. (2009). Anticipatory smiling: Linking early affective communication and social outcome. Infant Behavior and Development, 32(1), 33–43.
Pierce, K., & Schreibman, L. (1995). Increasing complex social behaviors in children with autism: Effects of peer-implemented pivotal response training. Journal of Applied Behavior Analysis, 28(3), 285.
Robinson, S. E. (2011). Teaching paraprofessionals of students with autism to implement pivotal response treatment in inclusive school settings using a brief video feedback training package. Focus on Autism and Other Developmental Disabilities, 26(2), 105–118.
Rogers, S. J., Estes, A., Lord, C., Vismara, L., Winter, J., Fitzpatrick, A., … Dawson, G. (2012). Effects of a brief Early Start Denver Model (ESDM)–based parent intervention on toddlers at risk for autism spectrum disorders: A randomized controlled trial. Journal of the American Academy of Child & Adolescent Psychiatry, 51(10), 1052–1065.
Rutter, M., DiLavore, P. C., Risi, S., Gotham, K., & Bishop, S. L. (2012). Autism diagnostic observation schedule: ADOS-2. Los Angeles, CA: Western Psychological Services.
Santarelli, G., Koegel, R. L., Casas, J. M., & Koegel, L. K. (2001). Culturally diverse families participating in behavior therapy parent education programs for children with developmental disabilities. Journal of Positive Behavior Interventions, 3(2), 120.
Schreibman, L., Stahmer, A. C., & Pierce, K. L. (1996). Alternative applications of pivotal response training: Teaching symbolic play and social interaction skills. In Positive behavioral support: Including people with difficult behavior in the community (pp. 353–371). Baltimore, MD: Brookes.
Seligman, M. E. (1972). Learned helplessness. Annual Review of Medicine, 23(1), 407–412.
Shic, F., Macari, S., & Chawarska, K. (2014). Speech disturbs face scanning in 6-month-old infants who develop autism spectrum disorder. Biological Psychiatry, 75(3), 231–237.
Sparrow, S. S., Cicchetti, D. V., & Balla, D. A. (2005). Vineland adaptive behavior scales: (Vineland II), survey interview form/caregiver rating form. Livonia, MN: Pearson Assessments.
Stahmer, A. C. (1995). Teaching symbolic play skills to children with autism using pivotal response training. Journal of Autism and Developmental Disorders, 25(2), 123–141.
Steiner, A. M. (2011). A strength-based approach to parent education for children with autism. Journal of Positive Behavior Interventions, 13(3), 178–190.
Steiner, A. M., Gengoux, G. W., Klin, A., & Chawarska, K. (2013). Pivotal response treatment for infants at-risk for autism spectrum disorders: A pilot study. Journal of Autism and Developmental Disorders, 43(1), 91–102.
Steiner, A. M., Koegel, L. K., Koegel, R. L., & Ence, W. A. (2012). Issues and theoretical constructs regarding parent education for autism spectrum disorders. Journal of Autism and Developmental Disorders, 42(6), 1218–1227.
Symon, J. B. (2005). Expanding interventions for children with autism: Parents as trainers. Journal of Positive Behavior Interventions, 7(3), 159–173.
Vernon, T. W., Koegel, R. L., Dauterman, H., & Stolen, K. (2012). An early social engagement intervention for young children with autism and their parents. Journal of Autism and Developmental Disorders, 42(12), 2702–2717.
Watson, L. R., Crais, E. R., Baranek, G. T., Dykstra, J. R., & Wilson, K. P. (2013). Communicative gesture use in infants with and without autism: A retrospective home video study. American Journal of Speech-Language Pathology, 22(1), 25–39.
Werner, E., Dawson, G., Osterling, J., & Dinno, N. (2000). Brief report: Recognition of autism spectrum disorder before one year of age: A retrospective study based on home videotapes. Journal of Autism and Developmental Disorders, 30(2), 157–162.
Wetherby, A. M., & Prizant, B. M. (2002). Communication and symbolic behavior scales: Developmental profile. Baltimore, MD: Paul H Brookes Publishing.
Williams, J. A., Koegel, R. L., & Egel, A. L. (1981). Response-reinforcer relationships and improved learning in autistic children. Journal of Applied Behavior Analysis, 14(1), 53–60.
Winterling, V., Dunlap, G., & O’Neill, R. E. (1987). The influence of task variation on the aberrant behaviors of autistic students. Education and Treatment of Children, 10, 105–119.
Wolff, P. H. (1987). The development of Behavioral states and the expression of emotions in early infancy: New proposals for investigation. Chicago, IL: University of Chicago Press.
Zwaigenbaum, L., Bryson, S., Rogers, T., Roberts, W., Brian, J., & Szatmari, P. (2005). Behavioral manifestations of autism in the first year of life. International Journal of Developmental Neuroscience, 23(2), 143–152.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2018 Springer International Publishing AG, part of Springer Nature
About this chapter

Cite this chapter
Bradshaw, J., Koegel, L. (2018). Adapting Pivotal Response Treatment to Support the Families of High-Risk Infants. In: Siller, M., Morgan, L. (eds) Handbook of Parent-Implemented Interventions for Very Young Children with Autism. Autism and Child Psychopathology Series. Springer, Cham. https://doi.org/10.1007/978-3-319-90994-3_4
Download citation
DOI: https://doi.org/10.1007/978-3-319-90994-3_4
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-90992-9
Online ISBN: 978-3-319-90994-3
eBook Packages: Behavioral Science and PsychologyBehavioral Science and Psychology (R0)