
Abstract
Intestinal fibrosis is a common complication in inflammatory bowel disease. These fibrotic processes develop in genetically susceptible individuals, influenced by an interplay with environmental, immunological and disease-related factors. A deeper understanding of the genetic factors driving fibrogenesis might help to unravel the pathogenesis, and ultimately lead to development of new, anti-fibrotic therapies. Here we review the genetic factors that have been associated with the development of fibrosis in patients with both Crohn’s disease and ulcerative colitis, as well as their potential pathophysiological mechanism(s).
Access provided by CONRICYT-eBooks. Download chapter PDF
Similar content being viewed by others


Keywords
3.1 Introduction
The study of the genetic architecture of inflammatory bowel disease (IBD), with Crohn’s disease (CD) and ulcerative colitis (UC) as its main entities, has made great progress in the past decade. Genome-wide association studies and meta-analyses have identified a total of 242 IBD risk loci [1]. Although many patients with CD or UC undergo surgery during the course of their disease, with stricture formation being the most common indication for major intestinal surgery—especially in CD, a genomic basis that fully explains this disease heterogeneity has not yet been revealed [2, 3].
The development of fibrosis in IBD is likely influenced by various genetic, environmental, immunological and disease-related factors [4,5,6,7]. So far, the relative contribution of each component in the pathogenesis is not clear. This chapter aims to clarify the genetic contribution in developing fibrosis in patients with IBD.
3.2 Genetics and Fibrosis in Crohn’s Disease
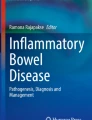
Published literature on the genetic background of fibrotic CD is broad and very often reports conflicting data. Identified variants are involved in different biological processes, suggesting that these processes contribute to the pathogenesis of fibrostenosis (Fig. 3.1). Below we provide an overview of individual variants and genes that have been associated with fibrotic disease in CD, and organized them according to the biological process they are involved in (Table 3.1). For each gene, we describe its general function, list the variants associated with fibrotic CD, and how they could be involved in the pathogenesis of fibrosis.

Biological processes affected by the variants associated with fibrostenotic CD
3.2.1 Bacterial Sensing
3.2.1.1 Nucleotide-Binding Oligomerization Domain-Containing Protein 2, NOD2
The NOD2 gene, located in the IBD1 locus on chromosome 16q12, is the most studied gene in relation to fibrostenotic disease in CD. NOD2 encodes CARD15, a member of the Apaf-1/NOD1 family of CARD (caspase recruitment domain containing protein) proteins [35, 36]. NOD2/CARD15 is mainly expressed by monocytes and macrophages, where it acts as a cytosolic sensor for bacterial products. It is involved in apoptosis and activates NF-κB in response to lipopolysaccharide (LPS), binding its leucine-rich repeating region (LRR) [11, 19]. Moreover, through its CARD-domain, CARD15 is able to induce interleukin1-beta (IL-1β) processing and release [37]. Importantly, NOD2 is also expressed in Paneth cells in the terminal ileum [38].
In the early 2000’s, three NOD2 variants, including two amino acid substitutions (R702W in exon 4, and G908R in exon 8) and one frameshift mutation (Leu1007fsinC in exon 11), were found to be associated with CD susceptibility [16, 35, 39,40,41]. Several other NOD2 SNPs were later added to this list, although the first three still represent the strongest association signals. Many genotype-phenotype studies were then performed to find their role in defining specific CD subtypes (CD disease location and/or behaviour). While practically all studies agree on an association between NOD2 and ileal disease location (Table 3.2), none of the NOD2 SNPs was uniformly found as an independent risk factor for developing fibrostenotic disease [6, 8,9,10,11,12,13,14,15,16,17,18,19,20,21,22,23,24, 26, 38, 42,43,44,45,46,47,48,49,50,51,52,53,54,55]. Some studies however did show associations between at least one of the three NOD2 variants and fibrostenotic disease [19,20,21, 24], often independent of an association with small bowel disease [11, 14, 17, 22, 23] (Table 3.2).
The lack of uniformity seems mainly based on the small sample sizes in the different studies (Table 3.2). In a Northern-French population of 205 CD patients, NOD2 R702W (rs2066844) was found a strong predictor of fibrostenotic disease, independently of ileal disease location [8], but no other group could confirm this association. An association of NOD2 G908R (rs2066845) and fibrostenotic disease was first reported in a Spanish CD cohort (n = 204), although fibrostenotic disease was mainly dependent on location of disease in the terminal ileum [9]. Later, a meta-analysis including a total of 8833 CD patients reported G908R as being associated with fibrostenotic disease (pooled RR = 1.90) [10]. It is important to highlight however, that only 12 of the included 49 studies in this meta-analysis had enough data to analyse individual NOD2 variants, and most included studies did not differentiate between G908R homo- and heterozygotes. Of the three NOD2 variants, the Leu1007fsinsC frameshift mutation (rs2066847) shows the strongest association with fibrostenotic disease, but again it is unclear whether this is dependent on ileal disease involvement [11,12,13,14]. Seiderer et al. calculated a positive predictive value (PPV) of 80% and a negative predictive value (NPV) of 75% for the diagnosis of small bowel stenosis in clinically symptomatic patients with a Leu1007fsinC variant. Furthermore, they noticed 62% of their patients being Leu1007fsinC homo- or heterozygous needed surgery, whereas the need for surgical intervention in patients without this variant was remarkably low [15]. A sub-analysis of another cohort with 19 patients, all Leu1007fsinC homozygous, identified a high-risk population, characterized by for instance long-segment stenosis, frequent need for surgery and high risk for re-stenosis afterwards [16]. The same group confirmed these findings later on in a prospective study [15], after which the European IBDchip project reported comparable results in a retrospective study (n = 38) [17], as did Schnitzler et al. [18]. Besides studying the association of individual NOD2 SNPs with a fibrostenotic CD phenotype, often the NOD2 SNPs are considered together. The pooled relative risk (RR) of stricturing disease with the presence of any NOD2 variant allele was 1.33 in the meta-analysis by Adler et al. [10]. Furthermore, Lesage et al. clearly described the ‘gene dosage effect’ of NOD2 SNPs: patients carrying two SNPs have a higher incidence of stenosis compared to patients with one or two wild-type alleles [22], which was afterwards confirmed by others [10, 23, 55]. There are also several studies that could not find an association between NOD2 variants and fibrostenotic disease: Louis et al. found that only disease location and number of flares per year are significantly different between different CD phenotypes, and that ileal disease location was associated with a stricturing disease pattern [51]. Although NOD2 variants were associated with CD susceptibility in a Brazilian population, Baptista et al. could not find a genotype-phenotype correlation [43]. The biggest study thus far looking into genotype-phenotype associations in IBD to date, also did not find an association between NOD2 and fibrotic disease, when considering disease location. They conclude that while disease location is in part genetically determined, it is considered an intrinsic aspect of a patient’s clinical disease, and the major driver to changes in disease behaviour over time [26]. Because of the strong correlation between NOD2 variants and ileal disease location, we assume that the observed association between fibrostenosis and NOD2 relies on a confounded association due to disease location.
How could the NOD2 variants be pathophysiologically linked to the development of fibrosis? They might induce fibrostenotic disease by shifting T lymphocytes towards Transforming Growth Factor beta (TGF-β) cytokine production, and by increasing collagen deposition by smooth muscle cells and fibroblasts in the intestine [11]. Functional data are primarily available for Leu1007fsinC: Leu1007fsinC leads to a truncated CARD15 protein, resulting in an altered activation of NF-κB following bacterial triggers [41]. It was previously thought that Leu1007fsinC was associated with an impaired IL-1β production and dendritic cell function, resulting in a dysregulation of the antibacterial host defence, increased intestinal permeability and impaired regulation of innate and adaptive immunity in the intestinal tract [15]. However, Maeda et al. later reported Leu1007fsinC is associated with enhanced NF-κB activation and IL-1β secretion in mice [37]. Additional mechanisms such as diminished mucosal alpha-defensin expression might also be involved [15]. It is possible that the other two variants also alter the structure of the LRR domain, resulting in abnormalities in bacterial recognition [46].
3.2.1.2 Toll-Like Receptors, TLRs
TLRs are transmembrane domain proteins with a tripartite structure: they contain an extracellular domain (including LRRs) responsible for ligand recognition, a single transmembrane spanning region, and a globular cytoplasmic Toll/IL-1 receptor (TIR) signalling domain. Currently, ten TLRs are described in humans [56]. They are expressed in myeloid cells and play a major role both in detecting microbes and in initiating innate immune responses. TLR4, expressed in the Golgi apparatus of intestinal epithelial cells, interacts with LPS, contributing to the perpetuation of inflammatory epithelial cell injury via Tumour Necrosis Factor Alpha (TNF-α)-induced alterations of enterocyte turnover in an (auto)paracrine matter [21].
Rs4986790 (Asp299Gly) located within TLR4 has been shown to be a susceptibility variant for CD [57], although this could not be confirmed in another study by Lakatos et al. (possibly because the variant allele is more present in their control population compared to the study by Franchimont et al.) [21]. Neither of the two studies found an association with CD sub-phenotype. This variant is associated with decreased responsiveness to endotoxins in humans [58, 59]. Although there is no genetic evidence for a role for TLR4 in the pathogenesis of fibrostenotic disease in CD, Rieder et al. suggested the first direct link between innate immunity to bacteria (via TLRs) and fibrosis in humans [60]. Furthermore, in other diseases like systemic sclerosis and liver fibrosis, TLR4 is thought to have a pathophysiological contribution [61, 62].
3.2.2 Autophagy: Autophagy-Related 16-like 1, ATG16L1
The ATG16L1 gene, member of a large family of genes involved in autophagocytosis, is located on chromosome 2q37. ATG16L1 is essential in the targeting and destruction of pathogen-derived proteins in the innate immune response [63, 64]. Autophagy is also important for degrading cytoplasmic components, sequestered within vesicles, by the lysosome [38].
The ATG16L1 T300A variant (rs2241880) is an important susceptibility variant for CD [63, 65, 66]. This same variant has also been associated with ileal disease location, independent of NOD2 genotype or disease duration; the study did not mention an association with stricturing disease [64]. Later, Fowler et al. reported a significant association between fibrostenotic disease, the GG risk genotype and ileal disease, independent of NOD2 (although the number of NOD2 variants in their Australian CD population might be too small) [25]. However, the European IBDchip Project could not confirm this association between ATG16L1 T300A and fibrostenotic disease [17].
The T300A amino acid substitution is a highly-conserved residue that is located in the WD-repeat domain of ATG16L1, and may therefore affect interactions of the protein with other components of the autophagosome [64]. This variant plays an important role in pathogen clearance [67], resulting in imbalanced cytokine production [68]. Moreover, presence of this ATG16L1 risk allele seems associated with a reduced ability to generate a specific type of macrophages (Mφind, phenotypically closely resembling the anti-inflammatory CD206+ M2-macrophages), also implying an impaired anti-inflammatory functioning [69]. The resulting inflammatory signals could eventually stimulate mesenchymal cells to make enormous amounts of collagen and other fibrogenic molecules [70]. Moreover, the ATG16L1 T300A variant enhances NOD2-driven cytokine production in an autophagy independent manner [68, 71]. A link between NOD2 and ATG16L1 in the activation of autophagy could be relevant for intestinal fibrogenesis: it is possible that NOD2 and/or ATG16L1 variants jointly can alter the responsiveness of immune cells to bacterial components, thereby amplifying inflammatory signals leading to fibrosis [70].
Overall, based on the current genetic association data, there is currently no true genetic link between ATG16L1 and fibrostenosis. Similar to NOD2, the described associations might be driven by the confounding role of ileal disease location. This does not preclude a role for ATG16L1 or the autophagic process in general in the pathogenesis of fibrostenosis.
3.2.3 Antigen Presentation: Major Histocompatibility Complex (MHC)
The MHC region encodes many immunological proteins, including the antigen-presenting classical human leukocyte antigen (HLA) molecules. Genome-wide association studies of IBD have shown strong evidence of association to genes belonging to the MHC complex [72]. Because of the complexity of the region, many researchers avoid including this region into their analysis. One study by Ahmad et al. studied 340 SNPs in 24 genes from the HLA region in relation with fibrotic CD, but did not find any associations [19]. The IIBDGC genotype-phenotype study found a genome-wide significant association with rs77005575 located in the MHC region and disease behaviour, independent of disease location [26]. None of the included classical HLA alleles were independently associated with disease behaviour in the same study.
3.2.4 Cytokines and Their Receptors
3.2.4.1 Interleukin-23 Receptor, IL-23R
IL-23R is located on chromosome 1p31, and encodes a subunit of the receptor for the pro-inflammatory cytokine interleukin-23 [73]. IL-23R is highly expressed on the cell membrane of memory T cells and other immune cells, such as natural killer cells, monocytes and dendritic cells, which identify foreign substances to defend the body against infection. It is involved in the mediation of pro-inflammatory activities by the production of interleukin 17 via the activation of Th17 lymphocytes [38].
After Duerr et al. described IL-23R as a susceptibility gene for CD [73], Glas et al. published a genotype-phenotype correlation for the rs1004819 SNP within IL-23R. They found an increased incidence of ileal involvement and fibrostenotic disease in TT homozygous carriers compared to CC wildtype carriers, but this association did not withstand correction for multiple testing [27]. Another SNP within IL-23R, rs116630177, reached a statistically suggestive significance level in a nested case-control study focussing on the early development of fibrostenotic CD [34]. There is no evidence of an association of the main CD-associated SNP in IL-23R, rs11209026 [73], with intestinal fibrosis.
3.2.4.2 Fractalkine Receptor 1, CX3CR1
CX3CR1 (previously termed V28) is a leukocyte chemotactic and adhesion receptor that binds fractalkine (CX3CL1 or neurotactin, expressed in epithelial and endothelial cells), a CX3C chemokine that exhibits properties of both traditional chemokines and adhesion molecules [28]. CX3CR1 is expressed on natural killer cells, monocytes, CD8+ and some CD4+ T cells. By binding fractalkine, it regulates the migration of a subpopulation of CD8+ intraepithelial lymphocytes into the intestinal lamina propria, and their interaction with intestinal epithelial cells [28]. After stimulation by bacteria (or bacterial degradation products), CX3CR1-expressing cells rapidly adhere to the inflamed vascular endothelium and may play a role as a vascular gateway for cytotoxic effector cells [24].
After two strongly correlated (D’ = 0.99) CX3CR1 polymorphisms (V249I, rs3732379; and T280 M, rs3732378) were identified in HIV-positive patients [74], Brand et al. investigated these SNPs in the context of CD. They observed an association between both SNPs and fibrostenotic disease (without Bonferroni correction), but this was not independent of ileocolonic disease location [28]. Later, Sabate et al. again noticed a trend towards fibrostenotic behaviour in V249I carriers (not statistically significant after Bonferroni correction), especially in smokers, independent of NOD2 Leu1007fsinC carriage and ileal involvement [24]. Although the two SNPs are strongly correlated [74], Sabate et al. did not see a similar trend for T280M [24].
Several findings point towards CX3CR1 as a critical component in maintaining homeostasis of lamina propria macrophages, master regulators of inflammation and fibrosis [75]. Importantly, specifically for the described variants, it was shown in vitro that peripheral blood mononuclear cells (PBMCs) from individuals with wildtype CX3CR1 genotype adhere more potently to membrane-bound fractalkine than do PBMCs from homozygous V249I-T280M donors [28, 76]. Despite the limited data about an association between CX3CR1 and fibrostenotic disease, these functional data could point towards a true role for the CX3CR1/fractalkine axis in fibrosis in CD.
3.2.4.3 Transforming Growth Factor Beta (TGF-β)
TGF-β is encoded by a gene on chromosome 19q13. It is a regulatory protein that plays a key role in inflammatory, fibrotic and immunological events in the intestinal mucosa [29, 77]. Enhanced expression of TGF-β and its receptors seems to be involved in the pathogenesis of CD, and might contribute to fibrosis [78, 79]. After some SNPs (including C509T) in the TGF-β1-gene were described to lead to variations in the production of TGF-β serum levels in women [80, 81], some groups looked in vain for an association with susceptibility to CD [29, 79, 82]. However, Hume et al. observed a significant association between the AA genotype of a SNP in codon 25 in the TGF-β1 gene and a fibrostenotic phenotype. CD patients homozygous for the profibrotic A allele also tended to have a shorter time to intestinal resection [29].
3.2.4.4 Angiotensinogen
Angiotensinogen, mapped to chromosome 1q42, is meant to function locally as a cytokine in several organ systems, participating in the regulation of inflammation and fibrosis. After being cleaved by renin into angiotensin I and processed to angiotensin II, it may increase the production of TGF-β1 [29].
Hume et al. studied the association of a gain of function SNP located 6 bp from the transcription site of the angiotensinogen gene with CD and CD phenotype [83]. They reported a positive association for the A allele and CD, although without any genotype-phenotype association at the univariate or multivariate level [29].
3.2.4.5 Tumour Necrosis Factor Alpha (TNFα)
As TNFα plays a pivotal role in the pathophysiology of IBD, confirmed by the efficacy of anti-TNF drugs such as infliximab and adalimumab [84], Meijer et al. investigated the association between a SNP (G308A) in TNFα and fibrostenotic disease [31]. In line with other reports [85, 86], they could not find an association between this SNP and fibrostenotic CD [31].
3.2.5 Epithelial Barrier: Membrane Associated Guanylate Kinase, WW and PDZ Domain Containing 1, MAGI1
MAGI1 is located on chromosome 3p14 and encodes the membrane associated guanylate kinase WW and PDZ domain-containing protein 1 [30]. This protein plays an important role in the tight junction of intestinal epithelial cells through interaction with JAM4, a junctional adhesion transmembrane molecule. Disruption of this epithelial barrier can have dramatic effect on the mucosal integrity, which has been shown to contribute to the development of CD [30].
Alonso et al. recently published an interesting association between fibrostenotic CD and rs11924265, located in a 46.5 kb haplotype block inside a MAGI1 intron. They validated this association in an independent replication cohort [30]. Previously, other groups have shown a significant increase in intestinal permeability in patients with stricturing disease [87]. Rs11924265 might induce an alteration in the MAGI1 protein function, contributing to an exaggerated immune response, and to the subsequent transmural inflammation of the gastrointestinal tract [30].
3.2.6 Cell Signalling: Janus Kinase 2 (JAK2)
JAK2, located on chromosome 9, encodes for an intracellular tyrosine kinase that transduces cytokine-mediated signals via the JAK-STAT pathway [17, 59]. The large, retrospective, multicentre IBDchip study found that rs10758669 (C allele), within the JAK2 gene, is associated with an increased risk for ileal involvement and stenosing disease behaviour. One mechanism by which JAK2 contributes to this fibrostenotic disease could be by altering intestinal permeability [17]. Indeed, Prager et al. previously demonstrated that patients carrying the rs10758669 C risk allele significantly more often had an increased permeability compared with patients without the C allele [88].
3.2.7 Matrix Metalloproteinases (MMPs) and Tissue Inhibitors of MMPs (TIMPs)
MMPs, Zn-activated endoproteinases, are subdivided into four groups, depending on their structure and substrate specificity: collagenases, gelatinases, stromelysins, and membrane-type MMPs [31, 89, 90]. They mediate degradation of essentially all components of the extracellular matrix and can cleave a wide range of molecules such as soluble factors, membrane receptors, adhesion factors, signalling molecules, cytoskeleton proteins and proteins inside the nucleus. Additionally, MMPs also have non-catalytic functions: they act as intracellular transcription factors or as cell ligands, hereby activating (inflammatory) signalling pathways [91]. The enzymatic activity of these potentially harmful proteinases is tightly controlled and counterbalanced by endogenous inhibitors such as alpha 2 macroglobulin and specific tissue inhibitors of MMPs, the so-called TIMPs. TIMPs are produced by the same cell types that produce MMPs, primarily in cells resembling macrophages and fibroblasts [90, 92].
The last decade many different SNPs in these genes were described, related to processes like foetal development [93], primary sclerosing cholangitis [94], and coronary atherosclerosis [95]. Meijer et al. also studied their role in relation to CD susceptibility and CD phenotype. They found that the 5T5T genotype (an additional thymidine insertion at −1613 of the MMP-3 promoter) at the MMP-3 locus was associated with fibrostenotic CD [31]. Expression data furthermore showed increased MMP-3 levels in stenotic and prestenotic resected CD ileum, pointing to an MMP-3 (stromelysin-1) mediated altered clinical course of CD patients [92]. These findings might explain the high recurrence rate of intestinal strictures, as tissue turnover is present in non-resected pre-stenotic CD ileum in which the anastomosis is made [92]. Conflicting evidence exists regarding the consequences of the 5T5T genotype: some groups reported upregulation of MMP-3 expression [96, 97] whereas others reported a downregulation [98]. In the study by Meijer et al., patients stratified according to MMP-3 genotype had similar MMP-3 total activity [31].
3.2.8 Other Processes
In 2009, Henckaerts et al. examined the influence of some CD-associated susceptibility loci on changes in disease behaviour. They found that homozygosity for the rs1363670 G-allele in a gene encoding a hypothetical protein near the IL-12B gene, located on chromosome 5, was independently associated with stricturing disease behaviour, especially in patients with ileal involvement [33, 59]. So far, the pathophysiological consequences of this SNP, leading to a non-coding transcript variant, are not fully understood [59].
Because inherited risk factors (factor V Leiden, methylenetetrahydrofolate reductase (MTHFR) C677T ) have been reported to be associated with fibrosis in other chronic inflammatory diseases, Novacek et al. performed a retrospective study in CD patients aiming to identify these risk factors in fibrostenotic CD. They concluded that the MTHFR 6777TT variant, factor V Leiden and the prothrombin G20210A variant are not associated with fibrostenosis in CD [99].
FUT2 , located on chromosome 19 [59], encodes the Secretor enzyme alpha(1,2)-fucosyltransferase (Lewis blood group system) which allows expression of ABO antigens on the gastrointestinal mucosa and in bodily secretions (secretor phenotype) [32]. After a nonsense allele in FUT2 , rs601338 (W143X), was identified as a susceptibility variant for CD [100, 101], Forni et al. found non-secretors to be at slightly higher risk of a stricturing/penetrating behaviour (OR 1.51, p = 0.046). Additionally, their analysis revealed patients with blood group O are less likely to develop a stricturing disease (OR 0.70, p = 0.038) [32]. Although it is known that FUT2 expression affects the composition of the gut microbiota [102], the pathophysiological link between this specific SNP and fibrostenotic disease has not been unravelled yet. Theoretically, an altered microbial environment might induce more severe inflammation, leading to a more aggressive phenotype.
Finally, a SNP (rs35223850) in MIS18BP1, located on chromosome 14 and encoding a protein which binds the SP1 transcription factor, has been found in a carefully phenotyped cohort to be associated with early development of fibrostenotic complications in CD [34].
3.3 The Combined Action of the Known Susceptibility Variants
Crohn’s disease is a complex genetic disease, where several small-effect risk variants combined could influence disease onset. Combining the many individually weak signals into a genetic risk score might be a more powerful approach to study the genetic association with subphenotypes, or to predict disease onset or behaviour [26, 103]. Such a genetic risk score was calculated in the IIBDGC genotype-phenotype study, and tested for association with several disease subphenotypes. A strong association with disease behaviour was found (p = 9.23 × 10−18), indicating that the known susceptibility loci combined can be a useful measurement of CD subtypes, but still do not have enough predictive ability to distinguish between the different subtypes [26].
3.4 Genetics and Fibrosis in Paediatric CD
Both very-early-onset (<6 years) and later-onset (6–16 years) patients with CD can present with a fibrostenotic phenotype [104]. Currently, not much is known about the genotype-phenotype association in paediatric CD. Russell et al. studied NOD2 variants in the Scottish early-onset CD population (aged <16 years), and noticed a relatively small contribution to CD susceptibility, but a major impact on phenotype. Presence of stricturing disease behaviour at diagnosis showed a trend toward an increase in carriers of NOD2 variant alleles, which became significant by 2 years of follow up [54]. The association of NOD2 variants and fibrostenotic paediatric CD was previously already reported by two other groups [105, 106]. Importantly, all three studies also report an association between NOD2 variants and ileal disease location, which may therefore confound the association with fibrostenotic disease.
In contrast with a study in adult CD [29], Liberek et al. could not find any significant correlation between 4 common SNPs in TGFβ and any specific clinical parameter [107].
In 2014, Strisciuglio et al. performed a genotype-phenotype correlation study, focussing on autophagy gene variants. They observed a trend towards switching to a fibrostenotic disease in children homozygous for the ATG16L1 T300A risk allele. They did not find an association between NOD2 variants and stricturing CD, but observed an association between NOD2 variants and ileal disease location [108].
Although data in children are currently limited, it is possible that the association with NOD2 and ATG16L1 is driven by a similar confounding by ileal disease location as in adult-onset cases. This would need to be considered in future studies in paediatric CD.
3.5 Genetics and Fibrosis in Ulcerative Colitis
Intestinal fibrosis in UC is a relatively new described entity, occurring in about 5% of UC patients. The common belief that extracellular matrix deposition was restricted to the mucosal and submucosal layers of the large bowels in UC, has recently been questioned [109, 110]. Ippolito et al. showed an upregulated expression of RhoA , important in the fibrogenic differentiation of intestinal smooth muscle cells, in the muscular layers of the colon in UC patients [109]. Despite clinically significant implications [111], lack of investigations explain why genetic associations with intestinal fibrosis in UC have not yet been reported.
3.6 Genetics and Fibrosis Around the World
Although the incidence of IBD is rising in developing countries [112, 113], epidemiological data on the clinical phenotype of disease, and genotype-phenotype association studies, in non-European populations are limited. Similar as for Caucasian populations, several smaller genotype-phenotype studies have been performed in non-Caucasian populations [43, 114,115,116,117,118,119]. These usually study the same variants as those considered in Caucasian populations (NOD2, IL23R…), but the only association found was between the IL23-R variant rs1004819 and stricturing and penetrating disease in a Korean patient population [118]. It is possibly not surprising that NOD2 variants are not found to be associated with disease (subtypes) in different populations, as NOD2 variants have been seen with different frequencies in geographically diverse populations. Whereas the prevalence of CD patients who carry at least one NOD2 susceptibility variant varies from 27–50% in most Caucasian European populations, observed frequencies are much lower (15–21%) in Scandinavian countries [120, 121], which are generally characterized by more homogenous study populations. Caucasian populations, relatively far from Europe, but with European ancestry with hardly no racial mixing, like the United States, Canada and Australia, have NOD2 variant frequencies comparable with those found across the rest of Europe [120]. In Asians (Japanese, Chinese and Korean), Arabs, Africans and African Americans, the NOD2 variants are rare or even absent [38, 114, 122].
Recently, the first trans-ancestry association study of IBD was published by the IIBDGC [122]. They collected subphenotype data on 1991 patients with CD from East Asia, India and Iran and compared these data with available clinical phenotypes for 19,290 Europeans [7]. They showed some demographic differences, with for example more stricturing behaviour and perianal and less inflammatory CD in the non-European population compared to the European population, in line with previously reported prospectively collected clinical findings in incident cases of IBD in non-Europeans [113]. It will be interesting to see if these differences are explained by genetic factors that differ between populations, or rather by environmental factors (including different health care systems), ascertainment bias, or a combination of these. The trans-ancestry association study showed that although for most of the IBD risk loci, the direction and magnitude of effect are consistent in European and non-European cohorts, genetic heterogeneity was seen between divergent populations at several established risk loci, driven by differences in allele frequency (NOD2), effect size (TNFSF15 and ATG16L1), or a combination of both (IL23-R and IRGM). A large trans-ancestry genotype-phenotype study is under way, undoubtedly shedding light on possible genetic heterogeneity of disease subphenotypes in different populations.
3.7 Clinical Implications of the Found Associations
Based on current evidence, it is too early to adjust treatment in IBD according to genetic profiles to personalize treatment [26]. NOD2 is by far the most studied genetic predictor for fibrostenotic disease in CD. Although many studies suggest an important role for NOD2 variants in developing fibrostenotic CD, the low sensitivity of a single NOD2 variant for predicting fibrostenotic disease does not justify NOD2 genotyping in all patients [44]. It has been suggested that targeted early-intensive therapy for high-risk patients with two NOD2 mutations might be beneficial, if proven by prospective trials [10], but so far there is no adequate scientific evidence for a top-down medical therapy based solely on NOD2 variants. Importantly, based on the IIBDGC study including over 19,000 CD patients, it was found that none of the NOD2 variants are associated with fibrostenotic disease after correcting for disease location. Disease location thus seems to be the major driver to changes in disease behaviour over time [26], although important influences of environmental factors (e.g. smoking) and therapeutic strategies (early top down versus step up) cannot be excluded. Preferential involvement of the terminal ileum could be explained by NOD2 variants abrogating normal Paneth cell behaviour, as Paneth cells express NOD2/CARD15 throughout the small intestine, with maximal expression in the terminal ileum [46, 123].
3.8 Conclusions and Future Directions
Several genotype-phenotype studies have been performed to find which genetic variants play a role in defining disease location and behaviour, but hardly any variant was uniformly found as independent risk factor for developing fibrostenotic disease. Different reasons can be put forward. A first one is related to power of the individual studies. Many studies indeed included relatively small patient numbers (Table 3.1), and sub-analyses make the sample sizes even smaller. It should also be noted that various studies may include patient groups from either population-based registries and/or from secondary or tertiary referral centres. This has a direct influence on the proportion of patients with more severe disease as opposed to inflammatory disease, which in turn could lead to over- or under-representation of certain genetic associations. An example are the Scandinavian registries which are population-based, and where indeed a lower proportion of stenosing and penetrating CD is seen [7]. NOD2 frequencies in these populations are also lower (see above) [121], but this could be linked to the population-based character of the study population. Third, most susceptibility variants are not the pathophysiological causal ones, but are in LD with the true causal variant(s) at that locus, which might have more qualitative or quantitative effects and explain the association with a certain clinical features. Fourth, many studies apply different definitions for stenosing disease or use a limited number of variables given in the Vienna Classification [52]. This of course is an important bias in genetic association studies which rely heavily on the robustness of the phenotypical information. In addition, patients with only subclinical fibrosis without any (sub)obstructive complaints may incorrectly be classified in the unaffected, rather than the affected subgroup which may lead to false or inconclusive findings. Extensive and consistent phenotypical data collections are key to identify novel, and potential causal, SNPs associated with fibrostricturing disease.
Another reason could be the dramatic change in disease behaviour over the course of the disease, implying disease behaviour of CD cannot be analysed without considering the duration of disease [51, 124]. Also, because of the importance of disease location in driving changes of disease behaviour over time [26], disease location should always be considered when analysing risk factors for stenosing disease. In the case of for example NOD2, there is a strong correlation of NOD2 and ileal disease location [125], which might induce a false, confounded association between NOD2 variants and fibrostenotic disease in those cases where disease location is not considered in the analysis. Finally, disease behaviour is influenced by environmental factors [126], which can be dramatically different in the different studies. Examples include smoking and NSAIDs use, but also specific treatments may hide patients at risk to develop certain subtypes of disease. Any disease behaviour and severity analysis should be interpreted with caution, when there is no access to medication use and response to medications, especially for patients in the biologics era.
Among the 163 genome-wide significant IBD susceptibility loci as identified in the study by Jostins et al. [127], genetic variants in immune system components (NOD2, IL23R, IL-12B, JAK2, FUT2) and autophagy (ATG16L1, leucine-rich repeat kinase 2 (LRRK2)) could (jointly) contribute to the activation of mesenchymal cells and pathogenesis of fibrosis [127,128,129]. Although these susceptibility genes might pathophysiologically contribute to fibrostenotic processes, not all have been found to be associated with stricturing CD. For example, the LRRK2 CD-associated M2397 allele inhibits Nuclear Factor of Activated T cells (NFAT) [130], which is known to control fibroblast plasticity in the heart [131]. LRRK2 might thus also be involved in fibrosis in the gut, although so far this has not been reported. The development of fibrosis is preceded by a period of initial inflammation, and not all patients with CD express a fibrostenotic phenotype [124, 132, 133]. This highlights the possible difference between loci predisposing to overall disease (CD or UC), and loci predisposing to clinical phenotypes or disease course [127, 129, 134, 135]. It is thus important to consider the idea of different genes driving susceptibility on the one hand, and disease behaviour on the other. The IIBDGC study for the first time does this on a large scale, but hardly finds any genome-wide significant loci for disease behaviour independent from disease location, except from rs77005575 (MHC) [26].
Despite the lack of validated genotype-phenotype associations in large genome-wide studies, reported SNPs identified in smaller cohorts (as described earlier) contributed to unravelling fibrostenotic CD pathogenesis. The different biological processes that might be suggested based on genetics findings are summarized in Fig. 3.1. We feel that genetics alone will not be able to predict the development of fibrostenotic complication in IBD, largely owing to the large environmental component in disease pathogenesis and its interaction with the genetic background of the individual. We therefore want to advocate that future studies need to be integrated with transcriptomics and clinical, serological, and microbial characteristics. The key predictors found in all these different fields might lead to an integrated, clinically relevant multi-omics biomarker panel, guiding diagnosis and therapeutic decisions in fibrostenotic disease [1].
References
Umicevic Mirkov M, Verstockt B, Cleynen I. Genetics of inflammatory bowel disease: beyond NOD2. Lancet Gastroenterol Hepatol. 2017;2(3):224–34.
Rieder F, Kessler S, Sans M, Fiocchi C. Animal models of intestinal fibrosis: new tools for the understanding of pathogenesis and therapy of human disease. Am J Physiol Gastrointest Liver Physiol. 2012;303(7):G786–801. https://doi.org/10.1152/ajpgi.00059.2012.
Verstockt B, Cleynen I. Genetic influences on the development of fibrosis in Crohn’s disease. Front Med (Lausanne). 2016;3:24. https://doi.org/10.3389/fmed.2016.00024.
Chang CW, Wong JM, Tung CC, Shih IL, Wang HY, Wei SC. Intestinal stricture in Crohn’s disease. Intest Res. 2015;13(1):19–26. https://doi.org/10.5217/ir.2015.13.1.19.
Latella G, Di Gregorio J, Flati V, Rieder F, Lawrance IC. Mechanisms of initiation and progression of intestinal fibrosis in IBD. Scand J Gastroenterol. 2015;50(1):53–65. https://doi.org/10.3109/00365521.2014.968863.
Latella G, Rogler G, Bamias G, Breynaert C, Florholmen J, Pellino G, et al. Results of the 4th scientific workshop of the ECCO (I): pathophysiology of intestinal fibrosis in IBD. J Crohns Colitis. 2014;8(10):1147–65. https://doi.org/10.1016/j.crohns.2014.03.008.
Cleynen I, Boucher G, Jostins L, Schumm LP, Zeissig S, Ahmad T, et al. Genetic determinants of Crohn’s disease and ulcerative colitis phenotypes in 34,819 patients. Lancet. 2015;387(10014):156–67.
Heresbach D, Gicquel-Douabin V, Birebent B, D’halluin PN, Heresbach-Le Berre N, Dreano S, et al. NOD2/CARD15 gene polymorphisms in Crohn’s disease: a genotype- phenotype analysis. Eur J Gastroenterol Hepatol. 2004;16(1):55–62.
Mendoza JL, Murillo LS, Fernández L, Peña AS, Lana R, Urcelay E, et al. Prevalence of mutations of the NOD2/CARD15 gene and relation to phenotype in Spanish patients with Crohn disease. Scand J Gastroenterol. 2003;38(12):1235–40.
Adler J, Rangwalla SC, Dwamena BA, Higgins PD. The prognostic power of the NOD2 genotype for complicated Crohn’s disease: a meta-analysis. Am J Gastroenterol. 2011;106(4):699–712. https://doi.org/10.1038/ajg.2011.19.
Abreu MT, Taylor KD, Lin YC, Hang T, Gaiennie J, Landers CJ, et al. Mutations in NOD2 are associated with fibrostenosing disease in patients with Crohn’s disease. Gastroenterology. 2002;123(3):679–88.
Vavassori P, Borgiani P, D’Apice MR, De Negris F, Del Vecchio Blanco G, Monteleone I, et al. 3020insC mutation within the NOD2 gene in Crohn’s disease: frequency and association with clinical pattern in an Italian population. Dig Liver Dis. 2002;34(2):153.
Radlmayr M, Török HP, Martin K, Folwaczny C. The c-insertion mutation of the NOD2 gene is associated with fistulizing and fibrostenotic phenotypes in Crohn’s disease. Gastroenterology. 2002;122(7):2091–2.
Annese V, Lombardi G, Perri F, D’Incà R, Ardizzone S, Riegler G, et al. Variants of CARD15 are associated with an aggressive clinical course of Crohn’s disease--an IG-IBD study. Am J Gastroenterol. 2005;100(1):84–92. https://doi.org/10.1111/j.1572-0241.2005.40705.x.
Seiderer J, Brand S, Herrmann KA, Schnitzler F, Hatz R, Crispin A, et al. Predictive value of the CARD15 variant 1007fs for the diagnosis of intestinal stenoses and the need for surgery in Crohn’s disease in clinical practice: results of a prospective study. Inflamm Bowel Dis. 2006;12(12):1114–21. https://doi.org/10.1097/01.mib.0000235836.32176.5e.
Seiderer J, Schnitzler F, Brand S, Staudinger T, Pfennig S, Herrmann K, et al. Homozygosity for the CARD15 frameshift mutation 1007fs is predictive of early onset of Crohn’s disease with ileal stenosis, entero-enteral fistulas, and frequent need for surgical intervention with high risk of re-stenosis. Scand J Gastroenterol. 2006;41(12):1421–32. https://doi.org/10.1080/00365520600703900.
Cleynen I, González JR, Figueroa C, Franke A, McGovern D, Bortlík M, et al. Genetic factors conferring an increased susceptibility to develop Crohn’s disease also influence disease phenotype: results from the IBDchip European Project. Gut. 2013;62(11):1556–65. https://doi.org/10.1136/gutjnl-2011-300777.
Schnitzler F, Friedrich M, Wolf C, Angelberger M, Diegelmann J, Olszak T, et al. The NOD2 p.Leu1007fsX1008 mutation (rs2066847) is a stronger predictor of the clinical course of Crohn’s disease than the FOXO3A intron variant rs12212067. PLoS One. 2014;9(11):e108503. https://doi.org/10.1371/journal.pone.0108503.
Ahmad T, Armuzzi A, Bunce M, Mulcahy-Hawes K, Marshall SE, Orchard TR, et al. The molecular classification of the clinical manifestations of Crohn’s disease. Gastroenterology. 2002;122(4):854–66.
Heliö T, Halme L, Lappalainen M, Fodstad H, Paavola-Sakki P, Turunen U, et al. CARD15/NOD2 gene variants are associated with familially occurring and complicated forms of Crohn’s disease. Gut. 2003;52(4):558–62.
Lakatos PL, Lakatos L, Szalay F, Willheim-Polli C, Osterreicher C, Tulassay Z, et al. Toll-like receptor 4 and NOD2/CARD15 mutations in Hungarian patients with Crohn’s disease: phenotype-genotype correlations. World J Gastroenterol. 2005;11(10):1489–95.
Lesage S, Zouali H, Cézard JP, Colombel JF, Belaiche J, Almer S, et al. CARD15/NOD2 mutational analysis and genotype-phenotype correlation in 612 patients with inflammatory bowel disease. Am J Hum Genet. 2002;70(4):845–57. https://doi.org/10.1086/339432.
Brant SR, Picco MF, Achkar JP, Bayless TM, Kane SV, Brzezinski A, et al. Defining complex contributions of NOD2/CARD15 gene mutations, age at onset, and tobacco use on Crohn’s disease phenotypes. Inflamm Bowel Dis. 2003;9(5):281–9.
Sabate JM, Ameziane N, Lamoril J, Jouet P, Farmachidi JP, Soulé JC, et al. The V249I polymorphism of the CX3CR1 gene is associated with fibrostenotic disease behavior in patients with Crohn’s disease. Eur J Gastroenterol Hepatol. 2008;20(8):748–55. https://doi.org/10.1097/MEG.0b013e3282f824c9.
Fowler EV, Doecke J, Simms LA, Zhao ZZ, Webb PM, Hayward NK, et al. ATG16L1 T300A shows strong associations with disease subgroups in a large Australian IBD population: further support for significant disease heterogeneity. Am J Gastroenterol. 2008;103(10):2519–26. https://doi.org/10.1111/j.1572-0241.2008.02023.x.
Cleynen I, Boucher G, Jostins L, Schumm LP, Zeissig S, Ahmad T, et al. Inherited determinants of Crohn’s disease and ulcerative colitis phenotypes: a genetic association study. Lancet. 2016;387(10014):156–67. https://doi.org/10.1016/S0140-6736(15)00465-1.
Glas J, Seiderer J, Wetzke M, Konrad A, Török HP, Schmechel S, et al. rs1004819 is the main disease-associated IL23R variant in German Crohn’s disease patients: combined analysis of IL23R, CARD15, and OCTN1/2 variants. PLoS One. 2007;2(9):e819. https://doi.org/10.1371/journal.pone.0000819.
Brand S, Hofbauer K, Dambacher J, Schnitzler F, Staudinger T, Pfennig S, et al. Increased expression of the chemokine fractalkine in Crohn’s disease and association of the fractalkine receptor T280M polymorphism with a fibrostenosing disease phenotype. Am J Gastroenterol. 2006;101(1):99–106. https://doi.org/10.1111/j.1572-0241.2005.00361.x.
Hume GE, Fowler EV, Lincoln D, Eri R, Templeton D, Florin TH, et al. Angiotensinogen and transforming growth factor beta1: novel genes in the pathogenesis of Crohn’s disease. J Med Genet. 2006;43(10):e51. https://doi.org/10.1136/jmg.2005.040477.
Alonso A, Domènech E, Julià A, Panés J, García-Sánchez V, Mateu PN, et al. Identification of risk loci for Crohn’s disease phenotypes using a genome-wide association study. Gastroenterology. 2015;148(4):794–805. https://doi.org/10.1053/j.gastro.2014.12.030.
Meijer MJ, Mieremet-Ooms MA, van Hogezand RA, Lamers CB, Hommes DW, Verspaget HW. Role of matrix metalloproteinase, tissue inhibitor of metalloproteinase and tumor necrosis factor-alpha single nucleotide gene polymorphisms in inflammatory bowel disease. World J Gastroenterol. 2007;13(21):2960–6.
Forni D, Cleynen I, Ferrante M, Cassinotti A, Cagliani R, Ardizzone S, et al. ABO histo-blood group might modulate predisposition to Crohn’s disease and affect disease behavior. J Crohns Colitis. 2014;8(6):489–94. https://doi.org/10.1016/j.crohns.2013.10.014.
Henckaerts L, Van Steen K, Verstreken I, Cleynen I, Franke A, Schreiber S, et al. Genetic risk profiling and prediction of disease course in Crohn’s disease patients. Clin Gastroenterol Hepatol. 2009;7(9):972–80.e2. https://doi.org/10.1016/j.cgh.2009.05.001.
Holvoet T, Bossuyt P, Cleynen I, De Cock I, Hindryckx P, Vermeire S et al. Early fibrostenosis in Crohn’s disease is associated with multiple susceptibility loci on Immunochip analysis. 12th Congress of ECCO, Barcelona; 2017.
Hugot JP, Chamaillard M, Zouali H, Lesage S, Cezard JP, Belaiche J, et al. Association of NOD2 leucine-rich repeat variants with susceptibility to Crohn’s disease. Nature. 2001;411(6837):599–603.
Ogura Y, Inohara N, Benito A, Chen FF, Yamaoka S, Nunez G. Nod2, a Nod1/Apaf-1 family member that is restricted to monocytes and activates NF-kappaB. J Biol Chem. 2001;276(7):4812–8. https://doi.org/10.1074/jbc.M008072200.
Maeda S, Hsu LC, Liu H, Bankston LA, Iimura M, Kagnoff MF, et al. Nod2 mutation in Crohn’s disease potentiates NF-kappaB activity and IL-1beta processing. Science. 2005;307(5710):734–8. https://doi.org/10.1126/science.1103685.
Naser SA, Arce M, Khaja A, Fernandez M, Naser N, Elwasila S, et al. Role of ATG16L, NOD2 and IL23R in Crohn’s disease pathogenesis. World J Gastroenterol. 2012;18(5):412–24. https://doi.org/10.3748/wjg.v18.i5.412.
Cuthbert AP, Fisher SA, Mirza MM, King K, Hampe J, Croucher PJ, et al. The contribution of NOD2 gene mutations to the risk and site of disease in inflammatory bowel disease. Gastroenterology. 2002;122(4):867–74.
Hampe J, Cuthbert A, Croucher PJ, Mirza MM, Mascheretti S, Fisher S, et al. Association between insertion mutation in NOD2 gene and Crohn’s disease in German and British populations. Lancet. 2001;357(9272):1925–8. https://doi.org/10.1016/S0140-6736(00)05063-7.
Ogura Y, Bonen DK, Inohara N, Nicolae DL, Chen FF, Ramos R, et al. A frameshift mutation in NOD2 associated with susceptibility to Crohn’s disease. Nature. 2001;411(6837):603–6.
Alvarez-Lobos M, Arostegui JI, Sans M, Tassies D, Plaza S, Delgado S, et al. Crohn’s disease patients carrying Nod2/CARD15 gene variants have an increased and early need for first surgery due to stricturing disease and higher rate of surgical recurrence. Ann Surg. 2005;242(5):693–700.
Baptista ML, Amarante H, Picheth G, Sdepanian VL, Peterson N, Babasukumar U, et al. CARD15 and IL23R influences Crohn’s disease susceptibility but not disease phenotype in a Brazilian population. Inflamm Bowel Dis. 2008;14(5):674–9. https://doi.org/10.1002/ibd.20372.
Brand S. Homozygosity for the NOD2 p.Leu1007fsX1008 variant is the main genetic predictor for fibrostenotic Crohn’s disease. Inflamm Bowel Dis. 2012;18(2):393–4. https://doi.org/10.1002/ibd.21914.
Brand S. Moving the genetics of inflammatory bowel diseases from bench to bedside: first steps towards personalised medicine. Gut. 2013;62(11):1531–3. https://doi.org/10.1136/gutjnl-2012-304151.
Economou M, Trikalinos TA, Loizou KT, Tsianos EV, Ioannidis JP. Differential effects of NOD2 variants on Crohn’s disease risk and phenotype in diverse populations: a metaanalysis. Am J Gastroenterol. 2004;99(12):2393–404. https://doi.org/10.1111/j.1572-0241.2004.40304.x.
Glas J, Seiderer J, Tillack C, Pfennig S, Beigel F, Jürgens M, et al. The NOD2 single nucleotide polymorphisms rs2066843 and rs2076756 are novel and common Crohn’s disease susceptibility gene variants. PLoS One. 2010;5(12):e14466. https://doi.org/10.1371/journal.pone.0014466.
Hampe J, Grebe J, Nikolaus S, Solberg C, Croucher PJ, Mascheretti S, et al. Association of NOD2 (CARD 15) genotype with clinical course of Crohn’s disease: a cohort study. Lancet. 2002;359(9318):1661–5. https://doi.org/10.1016/S0140-6736(02)08590-2.
Ippoliti A, Devlin S, Mei L, Yang H, Papadakis KA, Vasiliauskas EA, et al. Combination of innate and adaptive immune alterations increased the likelihood of fibrostenosis in Crohn’s disease. Inflamm Bowel Dis. 2010;16(8):1279–85. https://doi.org/10.1002/ibd.21196.
Jürgens M, Brand S, Laubender RP, Seiderer J, Glas J, Wetzke M, et al. The presence of fistulas and NOD2 homozygosity strongly predict intestinal stenosis in Crohn’s disease independent of the IL23R genotype. J Gastroenterol. 2010;45(7):721–31. https://doi.org/10.1007/s00535-010-0231-7.
Louis E, Michel V, Hugot JP, Reenaers C, Fontaine F, Delforge M, et al. Early development of stricturing or penetrating pattern in Crohn’s disease is influenced by disease location, number of flares, and smoking but not by NOD2/CARD15 genotype. Gut. 2003;52(4):552–7.
Oostenbrug LE, Nolte IM, Oosterom E, van der Steege G, te Meerman GJ, van Dullemen HM, et al. CARD15 in inflammatory bowel disease and Crohn’s disease phenotypes: an association study and pooled analysis. Dig Liver Dis. 2006;38(11):834–45.
Rieder F, Lawrance IC, Leite A, Sans M. Predictors of fibrostenotic Crohn’s disease. Inflamm Bowel Dis. 2011;17(9):2000–7. https://doi.org/10.1002/ibd.21627.
Russell RK, Drummond HE, Nimmo EE, Anderson N, Smith L, Wilson DC, et al. Genotype-phenotype analysis in childhood-onset Crohn’s disease: NOD2/CARD15 variants consistently predict phenotypic characteristics of severe disease. Inflamm Bowel Dis. 2005;11(11):955–64.
Schnitzler F, Brand S, Staudinger T, Pfennig S, Hofbauer K, Seiderer J, et al. Eight novel CARD15 variants detected by DNA sequence analysis of the CARD15 gene in 111 patients with inflammatory bowel disease. Immunogenetics. 2006;58(2–3):99–106. https://doi.org/10.1007/s00251-005-0073-2.
De Nardo D. Toll-like receptors: activation, signalling and transcriptional modulation. Cytokine. 2015;74(2):181–9. https://doi.org/10.1016/j.cyto.2015.02.025.
Franchimont D, Vermeire S, El Housni H, Pierik M, Van Steen K, Gustot T, et al. Deficient host-bacteria interactions in inflammatory bowel disease? The toll-like receptor (TLR)-4 Asp299gly polymorphism is associated with Crohn’s disease and ulcerative colitis. Gut. 2004;53(7):987–92.
Arbour NC, Lorenz E, Schutte BC, Zabner J, Kline JN, Jones M, et al. TLR4 mutations are associated with endotoxin hyporesponsiveness in humans. Nat Genet. 2000;25(2):187–91. https://doi.org/10.1038/76048.
Yates A, Akanni W, Amode MR, Barrell D, Billis K, Carvalho-Silva D, et al. Ensembl 2016. Nucleic Acids Res. 2016;44(D1):D710–6. https://doi.org/10.1093/nar/gkv1157.
Rieder F, Schirbel A, Ouyang Z, West G, Rho H, de la Motte C, Fiocchi C. Pro-Fibrogenic activity of Toll-Like Receptor (TLR) and NOD-Like Receptor (NLR) ligands on Human Intestinal Myofibroblasts (HIF) – linking bacterial innate immunity to intestinal fibrosis. Gastroenterology. 2010;38(5):S35.
Bhattacharyya S, Varga J. Emerging roles of innate immune signaling and toll-like receptors in fibrosis and systemic sclerosis. Curr Rheumatol Rep. 2015;17(1):474. https://doi.org/10.1007/s11926-014-0474-z.
Petrasek J, Csak T, Szabo G. Toll-like receptors in liver disease. Adv Clin Chem. 2013;59:155–201.
Hampe J, Franke A, Rosenstiel P, Till A, Teuber M, Huse K, et al. A genome-wide association scan of nonsynonymous SNPs identifies a susceptibility variant for Crohn disease in ATG16L1. Nat Genet. 2007;39(2):207–11. https://doi.org/10.1038/ng1954.
Prescott NJ, Fisher SA, Franke A, Hampe J, Onnie CM, Soars D, et al. A nonsynonymous SNP in ATG16L1 predisposes to ileal Crohn’s disease and is independent of CARD15 and IBD5. Gastroenterology. 2007;132(5):1665–71. https://doi.org/10.1053/j.gastro.2007.03.034.
Cummings JR, Cooney R, Pathan S, Anderson CA, Barrett JC, Beckly J, et al. Confirmation of the role of ATG16L1 as a Crohn’s disease susceptibility gene. Inflamm Bowel Dis. 2007;13(8):941–6. https://doi.org/10.1002/ibd.20162.
Rioux JD, Xavier RJ, Taylor KD, Silverberg MS, Goyette P, Huett A, et al. Genome-wide association study identifies new susceptibility loci for Crohn disease and implicates autophagy in disease pathogenesis. Nat Genet. 2007;39(5):596–604. https://doi.org/10.1038/ng2032.
Begun J, Lassen KG, Jijon HB, Baxt LA, Goel G, Heath RJ, et al. Integrated genomics of Crohn’s disease risk variant identifies a role for CLEC12A in antibacterial autophagy. Cell Rep. 2015;11(12):1905–18. https://doi.org/10.1016/j.celrep.2015.05.045.
Salem M, Ammitzboell M, Nys K, Seidelin JB, Nielsen OH. ATG16L1: a multifunctional susceptibility factor in Crohn disease. Autophagy. 2015;11(4):585–94. https://doi.org/10.1080/15548627.2015.1017187.
Levin AD, Koelink PJ, Bloemendaal FM, Vos AC, D’Haens GR, van den Brink GR, et al. Autophagy contributes to the induction of anti-TNF induced macrophages. J Crohns Colitis. 2016;10(3):323–9. https://doi.org/10.1093/ecco-jcc/jjv174.
Zorzi F, Calabrese E, Monteleone G. Pathogenic aspects and therapeutic avenues of intestinal fibrosis in Crohn’s disease. Clin Sci (Lond). 2015;129(12):1107–13. https://doi.org/10.1042/CS20150472.
Sorbara MT, Ellison LK, Ramjeet M, Travassos LH, Jones NL, Girardin SE, et al. The protein ATG16L1 suppresses inflammatory cytokines induced by the intracellular sensors Nod1 and Nod2 in an autophagy-independent manner. Immunity. 2013;39(5):858–73. https://doi.org/10.1016/j.immuni.2013.10.013.
Goyette P, Boucher G, Mallon D, Ellinghaus E, Jostins L, Huang H, et al. High-density mapping of the MHC identifies a shared role for HLA-DRB1*01:03 in inflammatory bowel diseases and heterozygous advantage in ulcerative colitis. Nat Genet. 2015;47(2):172–9. https://doi.org/10.1038/ng.3176.
Duerr RH, Taylor KD, Brant SR, Rioux JD, Silverberg MS, Daly MJ, et al. A genome-wide association study identifies IL23R as an inflammatory bowel disease gene. Science. 2006;314(5804):1461–3.
Faure S, Meyer L, Costagliola D, Vaneensberghe C, Genin E, Autran B, et al. Rapid progression to AIDS in HIV+ individuals with a structural variant of the chemokine receptor CX3CR1. Science. 2000;287(5461):2274–7.
Medina-Contreras O, Geem D, Laur O, Williams IR, Lira SA, Nusrat A, et al. CX3CR1 regulates intestinal macrophage homeostasis, bacterial translocation, and colitogenic Th17 responses in mice. J Clin Invest. 2011;121(12):4787–95. https://doi.org/10.1172/JCI59150.
Daoudi M, Lavergne E, Garin A, Tarantino N, Debré P, Pincet F, et al. Enhanced adhesive capacities of the naturally occurring Ile249-Met280 variant of the chemokine receptor CX3CR1. J Biol Chem. 2004;279(19):19649–57. https://doi.org/10.1074/jbc.M313457200.
Schulte CM, Dignass AU, Goebell H, Röher HD, Schulte KM. Genetic factors determine extent of bone loss in inflammatory bowel disease. Gastroenterology. 2000;119(4):909–20.
di Mola FF, Friess H, Scheuren A, Di Sebastiano P, Graber H, Egger B, et al. Transforming growth factor-betas and their signaling receptors are coexpressed in Crohn’s disease. Ann Surg. 1999;229(1):67–75.
Schulte CM, Goebell H, Röher HD, Schulte KM. C-509T polymorphism in the TGFB1 gene promoter: impact on Crohn’s disease susceptibility and clinical course? Immunogenetics. 2001;53(2):178–82.
Grainger DJ, Heathcote K, Chiano M, Snieder H, Kemp PR, Metcalfe JC, et al. Genetic control of the circulating concentration of transforming growth factor type beta1. Hum Mol Genet. 1999;8(1):93–7.
Yamada Y, Miyauchi A, Goto J, Takagi Y, Okuizumi H, Kanematsu M, et al. Association of a polymorphism of the transforming growth factor-beta1 gene with genetic susceptibility to osteoporosis in postmenopausal Japanese women. J Bone Miner Res. 1998;13(10):1569–76. https://doi.org/10.1359/jbmr.1998.13.10.1569.
García-González MA, Crusius JB, Strunk MH, Bouma G, Pérez-Centeno CM, Pals G, et al. TGFB1 gene polymorphisms and inflammatory bowel disease. Immunogenetics. 2000;51(10):869–72.
Inoue I, Nakajima T, Williams CS, Quackenbush J, Puryear R, Powers M, et al. A nucleotide substitution in the promoter of human angiotensinogen is associated with essential hypertension and affects basal transcription in vitro. J Clin Invest. 1997;99(7):1786–97. https://doi.org/10.1172/JCI119343.
Van Deventer SJ. Tumour necrosis factor and Crohn’s disease. Gut. 1997;40(4):443–8.
Cantor MJ, Nickerson P, Bernstein CN. The role of cytokine gene polymorphisms in determining disease susceptibility and phenotype in inflammatory bowel disease. Am J Gastroenterol. 2005;100(5):1134–42. https://doi.org/10.1111/j.1572-0241.2005.40979.x.
Zipperlen K, Peddle L, Melay B, Hefferton D, Rahman P. Association of TNF-alpha polymorphisms in Crohn disease. Hum Immunol. 2005;66(1):56–9. https://doi.org/10.1016/j.humimm.2004.10.004.
Benjamin J, Makharia GK, Ahuja V, Kalaivani M, Joshi YK. Intestinal permeability and its association with the patient and disease characteristics in Crohn’s disease. World J Gastroenterol. 2008;14(9):1399–405.
Prager M, Büttner J, Haas V, Baumgart DC, Sturm A, Zeitz M, et al. The JAK2 variant rs10758669 in Crohn’s disease: altering the intestinal barrier as one mechanism of action. Int J Color Dis. 2012;27(5):565–73. https://doi.org/10.1007/s00384-011-1345-y.
Huppertz B, Kertschanska S, Demir AY, Frank HG, Kaufmann P. Immunohistochemistry of matrix metalloproteinases (MMP), their substrates, and their inhibitors (TIMP) during trophoblast invasion in the human placenta. Cell Tissue Res. 1998;291(1):133–48.
Matrisian LM. Metalloproteinases and their inhibitors in matrix remodeling. Trends Genet. 1990;6(4):121–5.
de Bruyn M, Vandooren J, Ugarte-Berzal E, Arijs I, Vermeire S, Opdenakker G. The molecular biology of matrix metalloproteinases and tissue inhibitors of metalloproteinases in inflammatory bowel diseases. Crit Rev Biochem Mol Biol. 2016;51(5):295–358. https://doi.org/10.1080/10409238.2016.1199535.
Warnaar N, Hofker HS, Maathuis MH, Niesing J, Bruggink AH, Dijkstra G, et al. Matrix metalloproteinases as profibrotic factors in terminal ileum in Crohn’s disease. Inflamm Bowel Dis. 2006;12(9):863–9. https://doi.org/10.1097/01.mib.0000231568.43065.ed.
Fujimoto T, Parry S, Urbanek M, Sammel M, Macones G, Kuivaniemi H, et al. A single nucleotide polymorphism in the matrix metalloproteinase-1 (MMP-1) promoter influences amnion cell MMP-1 expression and risk for preterm premature rupture of the fetal membranes. J Biol Chem. 2002;277(8):6296–302. https://doi.org/10.1074/jbc.M107865200.
Satsangi J, Chapman RW, Haldar N, Donaldson P, Mitchell S, Simmons J, et al. A functional polymorphism of the stromelysin gene (MMP-3) influences susceptibility to primary sclerosing cholangitis. Gastroenterology. 2001;121(1):124–30.
Zhi H, Wang H, Ren L, Shi Z, Peng H, Cui L, et al. Functional polymorphisms of matrix metallopeptidase-9 and risk of coronary artery disease in a Chinese population. Mol Biol Rep. 2010;37(1):13–20. https://doi.org/10.1007/s11033-009-9482-x.
Borghaei RC, Rawlings PL, Javadi M, Woloshin J. NF-kappaB binds to a polymorphic repressor element in the MMP-3 promoter. Biochem Biophys Res Commun. 2004;316(1):182–8. https://doi.org/10.1016/j.bbrc.2004.02.030.
Medley TL, Kingwell BA, Gatzka CD, Pillay P, Cole TJ. Matrix metalloproteinase-3 genotype contributes to age-related aortic stiffening through modulation of gene and protein expression. Circ Res. 2003;92(11):1254–61. https://doi.org/10.1161/01.RES.0000076891.24317.CA.
Samnegård A, Silveira A, Lundman P, Boquist S, Odeberg J, Hulthe J, et al. Serum matrix metalloproteinase-3 concentration is influenced by MMP-3 -1612 5A/6A promoter genotype and associated with myocardial infarction. J Intern Med. 2005;258(5):411–9. https://doi.org/10.1111/j.1365-2796.2005.01561.x.
Novacek G, Papay P, Miehsler W, Reinisch W, Lichtenberger C, Sunder-Plassmann R, et al. Are inherited thrombotic risk factors associated with fibrostenosis in Crohn’s disease? Inflamm Bowel Dis. 2011;17(12):2505–11. https://doi.org/10.1002/ibd.21648.
Franke A, McGovern DP, Barrett JC, Wang K, Radford-Smith GL, Ahmad T, et al. Genome-wide meta-analysis increases to 71 the number of confirmed Crohn’s disease susceptibility loci. Nat Genet. 2010;42(12):1118–25. https://doi.org/10.1038/ng.717.
McGovern DP, Jones MR, Taylor KD, Marciante K, Yan X, Dubinsky M, et al. Fucosyltransferase 2 (FUT2) non-secretor status is associated with Crohn’s disease. Hum Mol Genet. 2010;19(17):3468–76. https://doi.org/10.1093/hmg/ddq248.
Mäkivuokko H, Lahtinen SJ, Wacklin P, Tuovinen E, Tenkanen H, Nikkilä J, et al. Association between the ABO blood group and the human intestinal microbiota composition. BMC Microbiol. 2012;12:94. https://doi.org/10.1186/1471-2180-12-94.
Sleegers K, Bettens K, De Roeck A, Van Cauwenberghe C, Cuyvers E, Verheijen J, et al. A 22-single nucleotide polymorphism Alzheimer’s disease risk score correlates with family history, onset age, and cerebrospinal fluid Abeta42. Alzheimers Dement. 2015;11(12):1452–60. https://doi.org/10.1016/j.jalz.2015.02.013.
Bequet E, Sarter H, Fumery M, Vasseur F, Armengol-Debeir L, Pariente B, et al. Incidence and phenotype at diagnosis of very-early-onset compared with later-onset paediatric inflammatory bowel disease: a population-based study [1988-2011]. J Crohns Colitis. 2016;11(5):519–26. https://doi.org/10.1093/ecco-jcc/jjw194.
Kugathasan S, Collins N, Maresso K, Hoffmann RG, Stephens M, Werlin SL, et al. CARD15 gene mutations and risk for early surgery in pediatric-onset Crohn’s disease. Clin Gastroenterol Hepatol. 2004;2(11):1003–9.
Sun L, Roesler J, Rösen-Wolff A, Winkler U, Koch R, Thürigen A, et al. CARD15 genotype and phenotype analysis in 55 pediatric patients with Crohn disease from Saxony, Germany. J Pediatr Gastroenterol Nutr. 2003;37(4):492–7.
Liberek A, Jakóbkiewicz-Banecka J, Kloska A, Świderska J, Kmieć Z, Łuczak G, et al. Clinical parameters of inflammatory bowel disease in children do not correlate with four common polymorphisms of the transforming growth factor β1 gene. Acta Biochim Pol. 2011;58(4):641–4.
Strisciuglio C, Auricchio R, Martinelli M, Staiano A, Giugliano FP, Andreozzi M, et al. Autophagy genes variants and paediatric Crohn’s disease phenotype: a single-Centre experience. Dig Liver Dis. 2014;46(6):512–7. https://doi.org/10.1016/j.dld.2014.02.016.
Ippolito C, Colucci R, Segnani C, Errede M, Girolamo F, Virgintino D, et al. Fibrotic and vascular remodelling of Colonic Wall in patients with active ulcerative colitis. J Crohns Colitis. 2016;10(10):1194–204. https://doi.org/10.1093/ecco-jcc/jjw076.
Latella G, Rieder F. Intestinal fibrosis: ready to be reversed. Curr Opin Gastroenterol. 2017;33(4):239–45. https://doi.org/10.1097/MOG.0000000000000363.
Gordon IO, Agrawal N, Goldblum JR, Fiocchi C, Rieder F. Fibrosis in ulcerative colitis: mechanisms, features, and consequences of a neglected problem. Inflamm Bowel Dis. 2014;20(11):2198–206. https://doi.org/10.1097/MIB.0000000000000080.
Molodecky NA, Soon IS, Rabi DM, Ghali WA, Ferris M, Chernoff G, et al. Increasing incidence and prevalence of the inflammatory bowel diseases with time, based on systematic review. Gastroenterology. 2012;142(1):46–54 e42.; quiz e30. https://doi.org/10.1053/j.gastro.2011.10.001.
Ng SC, Tang W, Ching JY, Wong M, Chow CM, Hui AJ, et al. Incidence and phenotype of inflammatory bowel disease based on results from the Asia-pacific Crohn’s and colitis epidemiology study. Gastroenterology. 2013;145(1):158–65.e2. https://doi.org/10.1053/j.gastro.2013.04.007.
Adeyanju O, Okou DT, Huang C, Kumar A, Sauer C, Galloway C, et al. Common NOD2 risk variants in African Americans with Crohn’s disease are due exclusively to recent Caucasian admixture. Inflamm Bowel Dis. 2012;18(12):2357–9. https://doi.org/10.1002/ibd.22944.
Mahurkar S, Banerjee R, Rani VS, Thakur N, Rao GV, Reddy DN, et al. Common variants in NOD2 and IL23R are not associated with inflammatory bowel disease in Indians. J Gastroenterol Hepatol. 2011;26(4):694–9. https://doi.org/10.1111/j.1440-1746.2010.06533.x.
Meddour Y, Chaib S, Bousseloub A, Kaddache N, Kecili L, Gamar L, et al. NOD2/CARD15 and IL23R genetic variability in 204 Algerian Crohn’s disease. Clin Res Hepatol Gastroenterol. 2014;38(4):499–504. https://doi.org/10.1016/j.clinre.2014.02.003.
Yamazaki K, Takahashi A, Takazoe M, Kubo M, Onouchi Y, Fujino A, et al. Positive association of genetic variants in the upstream region of NKX2-3 with Crohn’s disease in Japanese patients. Gut. 2009;58(2):228–32. https://doi.org/10.1136/gut.2007.140764.
Yang SK, Park M, Lim J, Park SH, Ye BD, Lee I, et al. Contribution of IL23R but not ATG16L1 to Crohn’s disease susceptibility in Koreans. Inflamm Bowel Dis. 2009;15(9):1385–90. https://doi.org/10.1002/ibd.20921.
Zouiten-Mekki L, Kharrat M, Karoui S, Serghimi M, Fekih M, Matri S, et al. Tolllike receptor 4 (TLR4) polymorphisms in Tunisian patients with Crohn’s disease: genotype-phenotype correlation. BMC Gastroenterol. 2009;9:62. https://doi.org/10.1186/1471-230X-9-62.
Barreiro-de-Acosta M, Mendoza JL, Lana R, Domínguez-Muñoz JE, Díaz-Rubio M. NOD2/CARD15: geographic differences in the Spanish population and clinical applications in Crohn’s disease. Rev Esp Enferm Dig. 2010;102(5):321–6.
Ernst A, Jacobsen B, Østergaard M, Okkels H, Andersen V, Dagiliene E, et al. Mutations in CARD15 and smoking confer susceptibility to Crohn’s disease in the Danish population. Scand J Gastroenterol. 2007;42(12):1445–51. https://doi.org/10.1080/00365520701427102.
Liu JZ, van Sommeren S, Huang H, Ng SC, Alberts R, Takahashi A, et al. Association analyses identify 38 susceptibility loci for inflammatory bowel disease and highlight shared genetic risk across populations. Nat Genet. 2015;47(9):979–86. https://doi.org/10.1038/ng.3359.
Lala S, Ogura Y, Osborne C, Hor SY, Bromfield A, Davies S, et al. Crohn’s disease and the NOD2 gene: a role for paneth cells. Gastroenterology. 2003;125(1):47–57.
Louis E, Collard A, Oger AF, Degroote E, Aboul Nasr El Yafi FA, Belaiche J. Behaviour of Crohn’s disease according to the Vienna classification: changing pattern over the course of the disease. Gut. 2001;49(6):777–82.
Vermeire S, Wild G, Kocher K, Cousineau J, Dufresne L, Bitton A, et al. CARD15 genetic variation in a Quebec population: prevalence, genotype-phenotype relationship, and haplotype structure. Am J Hum Genet. 2002;71(1):74–83. https://doi.org/10.1086/341124.
Dotan I. Disease behavior in adult patients: are there predictors for stricture or fistula formation? Dig Dis. 2009;27(3):206–11. https://doi.org/10.1159/000228551.
Jostins L, Ripke S, Weersma RK, Duerr RH, McGovern DP, Hui KY, et al. Host-microbe interactions have shaped the genetic architecture of inflammatory bowel disease. Nature. 2012;491(7422):119–24. https://doi.org/10.1038/nature11582.
Cleynen I, Vermeire S. The genetic architecture of inflammatory bowel disease: past, present and future. Curr Opin Gastroenterol. 2015;31(6):456–63. https://doi.org/10.1097/MOG.0000000000000215.
Li C, Kuemmerle JF. Mechanisms that mediate the development of fibrosis in patients with Crohn’s disease. Inflamm Bowel Dis. 2014;20(7):1250–8. https://doi.org/10.1097/MIB.0000000000000043.
Liu Z, Lee J, Krummey S, Lu W, Cai H, Lenardo MJ. The kinase LRRK2 is a regulator of the transcription factor NFAT that modulates the severity of inflammatory bowel disease. Nat Immunol. 2011;12(11):1063–70. https://doi.org/10.1038/ni.2113.
Lighthouse JK, Small EM. Transcriptional control of cardiac fibroblast plasticity. J Mol Cell Cardiol. 2016;91:52–60. https://doi.org/10.1016/j.yjmcc.2015.12.016.
Cosnes J, Cattan S, Blain A, Beaugerie L, Carbonnel F, Parc R, et al. Long-term evolution of disease behavior of Crohn’s disease. Inflamm Bowel Dis. 2002;8(4):244–50.
Van Assche G, Geboes K, Rutgeerts P. Medical therapy for Crohn’s disease strictures. Inflamm Bowel Dis. 2004;10(1):55–60.
Lee J, Anderson C, Wesley E, Ahmad T, Edwards C, Parkes M et al. Identification of a polymorphism that predisposes to longitudinal disease behaviour in Crohn’s disease and may have prognostic utility (abstract). Fifth Congress of ECCO, Capri; 2010.
Lee JC, Biasci D, Roberts R, Gearry RB, Mansfield JC, Ahmad T, et al. Genome-wide association study identifies distinct genetic contributions to prognosis and susceptibility in Crohn’s disease. Nat Genet. 2017;49(2):262–8. https://doi.org/10.1038/ng.3755.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2018 Springer International Publishing AG, part of Springer Nature
About this chapter

Cite this chapter
Verstockt, B., Verstockt, S., Cleynen, I. (2018). Genetic Influences on the Development of Fibrosis in Inflammatory Bowel Disease. In: Rieder, F. (eds) Fibrostenotic Inflammatory Bowel Disease. Springer, Cham. https://doi.org/10.1007/978-3-319-90578-5_3
Download citation
DOI: https://doi.org/10.1007/978-3-319-90578-5_3
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-90577-8
Online ISBN: 978-3-319-90578-5
eBook Packages: MedicineMedicine (R0)