
Abstract
The G protein-coupled estrogen receptor, GPER, also known as GPR30, belongs to the seven transmembrane receptor superfamily and is involved in the rapid non-genomic estrogenic responses. Nevertheless, GPER regulation of transcriptional activity also has been reported. GPER downstream signaling includes the activation of the phosphatidylinositol 3-kinase (PI3K)/Akt and mitogen-activated protein kinase (MAPK) pathways, the stimulation of adenylyl cyclase, and the mobilization of intracellular calcium. Over the last decade, the discovery of GPER specific agonists and antagonists has been crucial to understand its physiological functions, mechanisms of action and its putative usefulness as a therapeutic target. The GPER seems to have an important role in endocrine, reproductive, immune, nervous, and cardiovascular systems, and alterations in its expression or activity have been associated with several pathological conditions such as cardiovascular diseases, obesity, diabetes, Parkinson, stroke, and cancer. GPER has been linked with the carcinogenic process, though some ambiguity exists concerning its protective or causative role in different tissues, or even in the same tissue. This chapter summarizes the existent knowledge concerning the structural and molecular aspects of GPER, its known ligands and activated pathways, as well as its role over the known hallmarks of cancer: exacerbated proliferation, resistance to apoptosis, stimulated migration and invasion, induction of angiogenesis, and the metabolic reprogramming. A special focus will be given to prostate cancer.
Access provided by CONRICYT-eBooks. Download chapter PDF
Similar content being viewed by others

Keywords
Introduction
Estrogens are very important hormones playing a determinant role in mammalian biology by its wide action regulating several processes in a great variety of tissues. As all hormones, estrogens act through specific receptors that after recognizing and binding their ligands transmit the information to downstream effectors. The estrogen receptor α (ERα) was the first ER to be known in 1973 [1]; and was more than two decades after in 1996, that a second ER, the ERβ, was described [2]. Since then, several isoforms of ERα and ERβ have been identified known to have tissue specific functions or acting as negative regulators of full-length ERs, namely, the ERα-A-E, the ERα36 and the ERβ1–5 [3,4,5,6,7,8,9]. The ERα and ERβ are known as the classical ERs exerting their actions as transcription factors and regulating the gene expression network in target tissues [10]. Generally, after ligand binding in the cytoplasm, hormone–receptor complexes are translocated to the nucleus, where they dimerize and bind DNA modulating gene expression. Other alternative mechanisms of estrogens actions have been described, such as, the interaction of ERs with other transcription factors, and the hormone independent receptor phosphorylation and activation [11, 12]. In addition to the genomic actions, classical ERs also can trigger non-genomic actions. It has been described that ERs can associate with the cell membrane and lead to the activation of protein kinase signaling pathways, or cross-talk with the intracellular secondary messengers produced in response to the activation of G protein-coupled receptors (GPCRs) [11, 12].
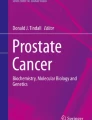
The landscape of estrogens signaling has gained increasing interest and complexity with the report of the G protein-coupled estrogen receptor (GPER), originally known as GPR30 [13]. GPER is a member of the GPCRs superfamily, and thus, displays the typical seven transmembrane helices and predominant location at the cell membrane (Fig. 5.1) [14].

Schematic representation of the human GPER: structural and molecular aspects . (a) Localization of GPER gene in the chromosome 7 and its structure consisting of three exons, with the coding region encoded by a single exon, the exon 3. (b) Structure of the GPER protein with the typical seven transmembrane α-helical regions, and the four extracellular and four cytosolic segments. The N-terminus is extracellular whereas the C-terminus is cytosolic
GPER expression has been found in multiple tissues and systems, including nervous, cardiovascular, gastrointestinal, immune, urinary and reproductive systems, and bone among others [15,16,17,18,19]. GPER is responsible for mediating the non-genomic actions of estrogens and is involved in the control of many biological processes. Its important role in several diseases including stroke, Parkinson, diabetes, cardiac diseases, bone diseases, epilepsy, autoimmune diseases, infection, and cancer has been suggested [20,21,22,23,24,25,26,27,28,29,30,31,32]. Concerning cancer, GPER has been detected in many types of tumors, including breast, ovarian, endometrial, prostate, testis, lung, thyroid, and others [33,34,35,36,37,38]. Also, its role in cancer development as a causative agent and associated with tumors aggressiveness, or as a tumor suppressor has been debated in the available literature [39, 40].
In this chapter, the molecular and structural aspects of GPER, as well as, its ligands, signaling activated pathways, and downstream effectors will be presented. Moreover, the GPER expression in cancer cases, and its role modulating the typical features of cancer cells will be discussed, with a special focus on prostate cancer (PCa).
Structural, Molecular and Cellular Aspects of GPER
The “life history” of GPER has begun some time ago, when it aroused from the shadows, like a ghost. Before the biochemical and structural characterization of GPER, researchers just have known about the possibility of alternative estrogens’ actions via non-genomic signaling mechanisms producing rapid cell effects. Over the years, as an attempt to explain the estrogenic effects in a time-frame not compatible with gene transcription and de novo protein synthesis, many theories were proposed concerning the existence of a membrane-bound ER [41, 42]. Amongst other hypotheses, it was shown that the classical nuclear ERs, the ERα and ERβ, were able to be translocated to the cell membrane through several mechanisms that involve post-translational modifications, such as palmitoylation or phosphorylation, interaction with caveolin-1, binding to adaptor and co-regulator molecules, and also the association with G proteins [43,44,45]. It was only later on that the idea of estrogens binding a GPCR at cell membrane has emerged [46]. At the end of 1990s several independent groups aimed at identifying a new GPCR characterized by its reduced homology to other GPCRs [14, 47,48,49,50,51], and for which no ligand was known. This orphan receptor was named GPR30 , even before 17β-estradiol (E2) has been identified as its ligand. Indeed, it was only a few years later that the “fate” of this orphan receptor has changed after the demonstration that it binds E2 with the activation of downstream signaling pathways [13, 52,53,54]. This lead the scientific community to rename the GPR30 that started to be known as GPER, a designation formally established by the International Union of Basic and Clinical Pharmacology in 2007 [55]. Even so, GPER’s “life” has been anything but consensual, and still today some groups question its role as an ER [56, 57].
The GPER is a member of the rhodopsin-like receptor superfamily highly homologous to the interleukin 8 receptor, and the angiotensin II receptor type 1 [47,48,49,50].
The human GPER gene is located on chromosome 7p22.3, and contains three exons (Fig. 5.1a), with the open reading frame of 1126 base pairs encoded by a single exon, the exon 3 [58]. As a GPCR, the GPER has a structure encompassing seven transmembrane α-helical regions, and four extracellular and four cytosolic segments (Fig. 5.1), which spans 375 amino acids and has a theoretical molecular mass of approximately 41 kDa [14, 15, 59]. The extracellular N-terminus has aspartic acid residues in its terminal region, which are targets for glycosylation; the C-terminal end is cytosolic [14, 15, 59]. Thus, ligand binding and receptor activation occur by interaction with the N-terminal domain, and the heterotrimeric G protein complex has been shown to bind the third loop of the intracellular domain (Fig. 5.1) [60, 61]. A PDZ domain located at the C-terminal region of GPER seems to be important for receptor location at cell membrane by its interaction with other plasma membrane proteins, namely, membrane-associated guanylate kinases and protein kinase A-anchoring protein 5 [14, 15, 62]. The C-terminal region also participates in receptor desensitization and internalization depending on phosphorylation by G protein-coupled receptor kinases [14, 15, 59]. Recently, a biosensor-based approach identified four distinct calmodulin-binding domains in the GPER protein [63, 64], though the effect of calmodulin regulating GPER-dependent signaling is at the moment unknown.
Although GPER was firstly identified as a membrane receptor , the question of its subcellular localization has deserved intense discussion. Several references exist indicating the presence of GPER in the endoplasmic reticulum, the Golgi apparatus, and also in the nucleus (Fig. 5.2) [54, 65,66,67,68,69,70,71]. The GPER expression in the endoplasmic reticulum and Golgi complex could be attributed at a first glance to the process of protein receptor synthesis and intracellular traffic before its translocation to the cell membrane. In fact, the GPER detected at the plasma membrane seems to be translocated from the cytoplasm 1 h after E2 stimulation, which also suggests that GPER activation is triggered at the cell membrane [54, 65]. However, some research groups defend that the GPER at the endoplasmic reticulum is signaling-active mediating cell responses by the mobilization of intracellular calcium (Ca2+) [52], though this is not a consensual matter. Concerning the nuclear location, besides its confirmed presence at the nuclear membrane [35, 67], it was recently shown that the GPER protein has a nuclear localization signal required for its nuclear translocation by an importin-dependent mechanism [69]. Moreover, the nuclear localization of GPER also seems to be induced by E2, and is associated with the regulation of gene transcription and promotion of physiological effects [69, 70]. Another study reported that GPER activation at the plasma membrane with the stimulation of cAMP production is followed by receptor internalization and intracellular localization in association with the cytokeratin intermediate filaments [68].

GPER subcellular localization . The receptor has been shown to be localized at the cell membrane and/or also in the endoplasmic reticulum and nucleus. Although not a consensual matter, there are reports indicating that E2 can interact with a signaling-active GPER at endoplasmic reticulum promoting cell responses [54, 65,66,67,68,69,70,71]. The Src, metalloproteinases (MMPs), calcium (Ca2+), and cAMP/protyein kinase A (PKA) mediated signaling pathways are detailed throughout the text and in Fig. 5.3. The GPER, as other GPCRs, enters the constitutive endocytic pathway but it is not recycled to the plasma membrane being instead accumulated in the endoplasmic reticulum and perinuclear region [72, 73]
It is also of worth note the constitutive retrograde transport of GPER from the plasma membrane towards the endosomal compartment (Fig. 5.2). Endocytosis is a common feature of GPCRs after ligand binding and activation to avoid excessive signaling. However, GPER endocytosis has some particularities. In contrast with other GPCRs that usually are degraded in lysosomes, the endocytosed GPER returns to the trans-Golgi network and undergoes ubiquitin-mediated proteasomal degradation [72,73,74]. Recently, it was shown that the Na+/H+ exchanger regulatory factor (NHERF1) can improve GPER stability by inhibiting its degradation through the ubiquitin-proteasome pathway [75].
Also in opposition with other GPCRs that after endocytosis are recycled to the plasma membrane, GPER enters early and recycling endosomes, but do not follows the plasma membrane route, and instead accumulates in the endoplasmic reticulum and perinuclear region [72, 73]. Interestingly, it has been proposed that GPER may mediate endocytic intracellular signaling linked to its constitutive endocytosis activity, which may be dependent on the PDZ domain that forms receptor complexes able to influence receptor dimerization, signaling and/or endocytosis [73]. Nevertheless, there is much to know about the factors that determine the preferred location of GPER at cell specific compartments, and its implications in intracellular signaling. The details and comprehensive analysis of the GPER signaling pathways will be explored in the following section of this chapter.
Overview of GPER Signaling Pathways
GPER is widely associated with the non-genomic effects of estrogens and estrogen-like substances, which are generally characterized as being: (1) very rapid, in minutes or even seconds; (2) insensitive to DNA transcription and protein synthesis inhibitors; and (3) activated by steroids coupled to high-molecular-weight molecules, such as bovine serum albumin (BSA), and thus incapable of cross the plasma membrane. GPER-mediated responses have been described in various cell types and involve several molecular targets and signaling pathways (Fig. 5.3), including, the mobilization of second messengers, such as Ca2+ and nitric oxide (NO), the interaction with other membrane receptors, such as insulin-like growth factor-1-receptor (IGF-1R) and epidermal growth factor receptor (EGFR), as well as, the activation of effector molecules, namely, the Src kinase and phosphatidylinositol 3-kinase (PI3K), the serine/threonine protein kinase Akt, mitogen-activated protein kinase (MAPK) family members, and the protein kinases A and C (PKA and PKC, respectively) [76].

GPER signaling pathways. GPER activates several downstream signaling cascades including the PI3K/AKT pathway, the Src pathway, the MAPKs/ERK1/2 pathway and the Notch signaling. The activation of MAPKs pathway influences the activation of Smad proteins and leads to the inhibition of the TGF-β signaling. GPER activation also leads to stimulation of adenylyl cyclase (AC) with an increase of cAMP concentrations and mobilization of intracellular Ca2+. GPER activation of intracellular signaling pathways also has been coupled with EGFR transactivation. GPER activation of Src-kinase stimulates MMPs that cleave the pro-HB-EGF leading to the release of free HB-EGF and EGFR activation. Alternatively, EGFR activation can be mediated by sphingosine 1 phosphate (S1P) a product of sphingosine kinase 1 (SphK1) activity
After ligand binding, GPER initiates intracellular signaling by activating heterotrimeric G proteins, composed of α, β and γ subunits, with the latter known as the βγ-complex [77]. In general, the Gα-subunit (Gαs) dissociates from the heterotrimeric Gαβγ complex and the free subunits (Gαs and Gβγ) activate distinct intracellular signaling pathways [78]. It has been demonstrated that both Gβγ [13] and Gαs [53] participate in the GPER-mediated signaling. Gαs activity stimulates the adenylyl cyclase producing an increase in cAMP concentration and mobilization of intracellular Ca2+ [52, 53, 79], whereas the Gβγ subunit and the downstream Src-related tyrosine kinases activate the MAPK transduction pathway [13], leading to phosphorylation of MAPKs/ERK1/2 [13]. In rat pachytene spermatocytes, the activation of GPER led to the initiation of ERK1/2 signaling cascade, correlated with an increased phosphorylation of c-Jun [80]. On the other hand, in breast cancer cell lines, the activation of MAPKs pathway influenced the activation of Smad proteins and led to the down-regulated signaling of the transforming growth factor beta (TGF-β) [81], since Smad2/3 proteins are essential signaling molecules mediating TGF-β effects [82]. The activation of ERKs signaling through GPER also was shown to activate the hypoxia-inducible factor 1α/vascular endothelial growth factor (HIF1α/VEGF) signaling, due to the upregulation of HIF1α and, consequently, to the upregulation of VEGF, a well-known marker of angiogenesis [83, 84].
GPER activation of the PI3K/Akt pathway has been reported in ER-negative endometrial cancer cells and seems to stimulate cell growth [85, 86]. GPER activity, in a Src kinase and PI3K/Akt dependent mechanism with the activation of NF-kB, was also shown to up-regulate cyclooxygenase 2 (COX2) expression in oviduct epithelial cells [87]. GPER may also contribute to the pro-tumorigenic effects of endothelin-1 in hepatocarcinoma cells and breast cancer via the activation of PI3K/ERK/c-Fos/AP1 transduction pathway [88].
GPER actions were also implicated in Notch signaling, inducing both the γ-secretase-dependent activation of Notch-1 and the expression of the Notch target gene Hes-1 [85, 89]. It was reported that GPER activation leads to the association of the intracellular domain of Notch-1 with the Hes-1 promoter inducing transcription of a Hes-1-reporter gene, as well as, to the down-regulation of VE-Cadherin and increased expression of Snail, a Notch target gene acting as a repressor of cadherin expression [89].
Interestingly, GPER activation of intracellular signaling pathways has been coupled with EGFR transactivation, through the Src-dependent stimulation of metalloproteinases (MMPs) (Fig. 5.3). MMPs have been shown to cleave the pro-HB-EGF leading to the release of free HB-EGF with resultant EGFR activation [13, 64, 90, 91]. Moreover, sphingosine 1-phosphate (S1P) , a product of sphingosine kinase 1 (Sphk1), seems to be another intermediate in the GPER-mediated transactivation of the EGFR [92]. SphK1 activation stimulated by E2 leads to the release of S1P, activating the S1P receptor Edg-3 and resulting in pro-HB-EGF cleavage [92]. A cross-talk of GPER with the IGF signaling pathway and GPER interaction with the IGFR and the ErbB receptors also has been described and associated with the progression of diverse types of cancer [93, 94].
Despite the transcriptional responses induced by estrogens are mainly associated to ERα- and ERβ-mediated actions, also the rapid signaling pathways activated by GPER have been shown to regulate gene expression in broad range of mammalian tissues and cells. These includes the upregulation of expression of several genes involved in relevant biological responses, for example, the transcription factor c-fos, the connective-tissue growth factor (CTGF), the early growth response 1 (Egr-1), pS2, sirtuins, cyclins A, D1, D2 and E, and the apoptotic regulators Bcl-2 and Bax; cyclins A1 and B1 were identified as down-regulated genes by GPER [80, 95,96,97,98,99,100,101].
Other important aspect to consider in GPER signaling is its interaction with the nuclear steroid receptors, namely, with the classical ERs, the glucocorticoid receptors, the mineralocorticoid receptors, and the vitamin D receptor. This cross-talk was elegantly reviewed by Prossnitz et al. [102] and will not be further explored in this chapter.
In the end, it is important to mention the receptor activity-modifying proteins (RAMPs) that interact with the GPCRs modifying their function, and acting as pharmacological switches and chaperones regulating signaling transduction [103]. Although GPER interaction with RAMP3 has been reported and linked to the receptor presentation at the cell membrane [104], the role of this regulatory proteins in the modulation of GPER function/activity still is in its infancy and more research is needed to clarify the liaison between RAMPs and GPER.
GPER Agonists and Antagonists: A Therapeutic Approach
From the time that was considered an orphan receptor to nowadays, many compounds have been identified with the ability to bind GPER, which substantially enriched its “molecular relationships”. Among the panoply of compounds that bind GPER, some of them are activators (agonists) whereas others inhibit receptor function/activity (antagonists). The identification of molecules able to modulate GPER activity (Table 5.1) and the disclosure of the underlying signaling pathways is an exciting field of research considering the exploitation of GPER as a therapeutic target.
Also, many studies have been performed to understand better the GPER structure and its binding characteristics. The specificity of GPER cavities and its several structural changes endows this receptor of a great ability to accept diverse ligands, some of them with large volume, and also that the same ligand can recognize different binding sites dependently on the structural conformation of GPER [105].
Natural Hormone Ligands
The first identified ligands for GPER, which gave the receptor’s name, were estrogens, particularly the E2. Competitive binding assays in GPER-transfected COS7 cells using E2 conjugated to the fluorophore Alexa 633 found a high-affinity for E2 (Kd 6 nM) contrarily to the non-physiological estrogen stereoisomer 17α-estradiol that fails to displace the fluorophore [52]. Similarly, studies with tritiated-hormone on membrane fractions also showed high-affinity of GPER for E2 (Kd 3 nM) but low-affinity for 17α-estradiol [53].
Nonetheless, the involvement of some E2 metabolites in GPER activation has been reported. For example, the oxidised metabolite 2-methoxy-estradiol has been reported to act as an agonist of GPER [106] whereas the 2-hydroxyestradiol has been shown to antagonize GPER action [106, 107]. Glucuronidation and sulfonation of E2 generate other metabolites like 17β-estradiol-17-d-glucuronide, which also seems to be an agonist of GPER at high concentrations; 50 mM 17β-estradiol-17-d-glucuronide increased the levels of cAMP and PKA activity [108].
Other estrogens like estrone and estriol exhibited very low affinity for GPER, whereas progesterone and testosterone were unable to bind GPER [53]. In the case of estriol, it seems to act as an antagonist of GPER [109, 110].
Considering the weak androgens dehydroepiandrosterone (DHEA) and epiandrosterone, no studies exist reporting GPER binding or activity. However, the endogenous metabolite 7β-hydroxy-epiandrosterone (7β-OH-EpiA) was shown to be capable of antagonizing estrogenic actions mediated by GPER [111].
Curiously, aldosterone, a mineralocorticoid steroid hormone, also seems to have affinity for GPER, with agonistic activity increasing the ERK phosphorylation in rat aortic endothelial cells and the migration of renal cancer cells [112,113,114]. Moreover, it was shown that the non-genomic effect of aldosterone causing rapid sodium intake involves GPER [115]. However, other studies were unable to detect aldosterone binding to cell membrane fractions [116, 117], suggesting that aldosterone could act through GPER, but without direct receptor binding [102].
Stress related hormones such as cortisol or adrenocorticotropic hormone (ACTH) seem to modulate GPER expression, although their ability to bind the receptor remains to be evaluated [53, 118].
Synthetic Ligands
Tamoxifen, a synthetic non-steroidal anti-estrogen is a recognized selective estrogen receptor modulator (SERM) with demonstrated efficacy as an adjuvant therapy for ER-positive and metastatic breast cancer [119]. It is a substituted triphenylethylene with low binding affinity for ERs compared with E2, but with a similar binding affinity for both ER subtypes displaying tissue-dependent ER antagonist or partial agonist activity. The 4-hydroxy metabolite (4-hydroxytamoxifen) is a more potent ER ligand and its active metabolite [120, 121].
Another synthetic compound, the estrogen derivative ICI 182,780 binds ERs with high affinity and has anti-estrogenic activity, blocking the ER transactivation, impairing its dimerization and inducing its degradation [120]. Interestingly, both ERs antagonists, 4-hydroxytamoxifen and ICI 182,780, can bind GPER, acting as agonists [122, 123]. Moreover, the tamoxifen analog STX (a diphenylacrylamide) was shown to have rapid neurological responses through a mechanism unrelated to the classical ERs and dependent on a Gq protein, which suggests the involvement of GPER [124]. More recently, another SERM, raloxifene, also was shown to activate GPER in cells devoid of ERα, mediating Akt activation [35, 125].
The knowledge that the classical ER antagonists induce agonistic effects via GPER has stirred their application in cancer treatment. On the light of this information, extreme caution has to be placed on the application of anti-estrogens therapies when GPER is present in tumors, which can be overcome by the introduction of GPER analysis in clinical diagnosis. This would be particularly relevant in estrogen-related cancers, such as breast, endometrium and ovary.
The stilbene estrogen diethylstilbestrol (DES) a potent estrogenic compound binding both ER subtypes with an affinity similar to that of E2, do not display affinity for GPER [13, 52, 53, 122, 123, 126], though weak binding capability able to induce activation of CREB, and of the downstream targets PKA, Src, and ERK1/2 has been reported [53, 127]. Also, DES seems to inhibit GPER expression [128].
Interestingly, the widely used ERα-selective agonist propylpyrazole triol (PPT) has shown agonistic activity for GPER in a range of 10–100 nM concentrations, whereas diarylpropionitrile (DPN) the ERβ-selective agonist had no activity through GPER [35]. Therefore, the use of PPT to ascertain ERα specific actions in different tissues and physiological conditions may have confounding effects triggered by GPER.
Also, there are reports of compounds disrupting the GPER action transactivating EGFR (Fig. 5.3). The anti-estrogenic benzopyran derivative 2-[piperidinoethoxyphenyl]-3-[4-hydroxyphenyl]-2H-benzo(b)pyran (K-1) showed to interfere with GPER mediated-EGFR activation, decreasing phosphorylation of MEK, ERK and of its downstream effectors such as c-jun and c-fos. Moreover, K-1 decreased the expression of β-catenin, proliferating cell nuclear antigen (PCNA), Cdk4, cyclin D1, c-myc, p-CREB and Bcl-xl and increased the expression of apoptotic markers like NOXA, PUMAα, p21, p27 and Bax [129]. The newly synthesized compound MIBE (ethyl 3-[5-(2-ethoxycarbonyl-1-methylvinyloxy)-1-methyl-1Hindol-3-yl] but-2-enoate) prevented the GPER-mediated EGFR and ERK activation, with consequent effects on gene transcription and cell proliferation, and was, thus, indicated as a GPER antagonist [130].
Membrane-Impermeable Ligands
The development of ligands with membrane impermeable properties , through steroid association with large proteins (e.g. BSA), oligomeric/polymeric dendrimers (PAMAM) or cyclodextrins, as well as the ionic estrogen derivatives (e.g. NMe3+), have allowed studying membrane-associated ERs [131, 132], and to ascertain the existence of GPER effects triggered at cell membrane.
Revankar et al. [133] evaluated the properties of a set of 17α-substituted estrogen derivatives with differential cell permeability. For example, the cationic E2-NMe3+ with a high-affinity for GPER, but membrane impermeable, at least for short periods of incubation and at low concentrations, was incapable of generating Ca2+ rise responses, whereas the related neutral carboxamide E2-NB with membrane permeability similar to those of E2 rapidly activated both the ERα and GPER [133]. These observations were quite relevant to support the intracellular location of GPER and its functionality driven by the endoplasmic reticulum. Nevertheless, this matter is far away from being solved and widely accepted among the scientific community. Moreover, these novel ligands are important to evaluate the subcellular location of GPER in healthy and pathological tissues and cells, and to decipher whether it varies with different environmental conditions, tissue properties, and/or developmental or disease stage. Further research is needed to clarify all these issues.
Phytoestrogens and Xenoestrogens
In the last years, with the increasing relevance of compounds mimicking estrogens and the concerns about endocrine disruption, many studies have identified some phytoestrogens and xenoestrogens as possible GPER ligands.
Phytoestrogens mainly encompass phenolic compounds, which are structurally divided into flavones, isoflavones, lignans, coumestans, and stilbenes [134]. The potential of phenolic compounds as preventive or therapeutic agents in several human diseases has been under intense investigation, and a large variety of these compounds also has shown to be able to modulate GEPR activity.
(−)-Epicatechin, a flavonoid present in cacao and many other food products, increases the activity of ERK1/2 through GPER activation [135]. Icariin is a prenylated flavonol glycoside isolated from plants of the genus Epimedium, which is used as a food supplement; icaritin is its hydroxylated derivative. Both icariin and icaritin seem to induce cellular effects through GPER, also inducing c-fos expression and EGFR-MAPK signaling activation [136, 137]. Baicalein, the main flavonoid derived from the root of Scutellaria baicalensis Georgi, a plant widely used in traditional Chinese medicine, also was indicated to interfere with GPER signaling [138]. In breast cancer cells, baicalein does not directly affect GPER expression, but it can inhibit GPER signal transduction pathways, namely, by suppressing the phosphorylation of ERK1/2, Akt, and Src, as well as the transcription of GPER-regulated genes, like c-fos, CTGF, CYR61, and Egr-1 [139].
Genistein, an isoflavone found in soy products, has shown high-affinity for GPER, with agonistic activity leading to MAPKs activation via a Gβγ-associated pathway and requiring Src-related and EGFR kinase activity. Moreover, genistein seems to upregulate c-fos expression [95, 140,141,142]. Quercetin is a genistein related flavonoid that naturally occurs as the aglycone form of other flavonoid glycosides. At 1 mM concentration, quercetin showed the same behavior of genistein, acting as a GPER agonist with stimulation of c-fos expression [95]. The isoflavone daidzein present in many plants and fruits exhibited both estrogenic and anti-estrogenic actions, despite no GPER binding affinity has been reported. However, it has been shown that daidzein mediates glutamate-induced effects via GPER [143]. Intestinal flora can metabolize daidzein to equol, which also do not have GPER binding ability described, but it has been suggested that it is involved in the generation of mitochondrial reactive oxygen species via GPER-mediated EGFR transactivation [144]. Nevertheless, puerarine an 8-C-glucoside of daidzein, was able to activate and modulate GPER activity and expression [145]. Similar findings were observed with prunetin, an isoflavone found in several agricultural foods, which seems to bind GPER with activation of ERK/MAPK through adenylyl cyclase and cAMP [146]. Tectoridin, the 7-glucoside of the isoflavone tectorigenin, also exerted estrogenic effects mediated through GPER, whereas it binds ERα poorly [147].
Coumestrol is a phenolic phytoestrogen of the class of coumestans known to activate ER-mediated signaling pathways, but its ability to bind and activate GPER was not described yet [140].
Resveratrol, a stilbene derivative with important biological actions and indicated as an anti-cancer compound [148] had its activity inhibited in the presence of GPER antagonists, which suggests that its role depends on GPER, likely by promoting PKC activation [149].
Oleuropein, the glycosylated conjugate of elenolic acid present in olives, also has been included in the group of GPER agonists [150].
The flaxseed derivative secoisolariciresinol diglucoside (SDG), upon metabolization by mammalian cells, originates the metabolite enterolactone (ENL), that shares the similar binding site of GPER specific agonist G1 as indicated by docking simulations, suggesting that it can bind GPER [151].
Xenoestrogens include a wide variety of nonsteroidal chemicals including nonylphenols, polybrominated diphenyl ethers, organophosphates, chlorinated hydrocarbons, biphenyls and phthalates that can be found in daily-life products such as detergents, surfactants, resins, lubricants, plastics, fire retardants, and pesticides [152].
The nonylphenols used in plastic industry, despite having the low affinity for classical ERs, showed a higher binding affinity for GPER [140]. Both bisphenol A (BPA) and nonylphenol, are strong competitors of E2 displacing the tritiated-hormone from GPER-containing membrane fractions [140]. BPA induced a rapid activation of ERK1/2 and the transcription c-fos likely through an AP1-mediated pathway [153,154,155,156,157]. BPA also stimulates the upregulation of X-linked inhibitor of apoptosis protein (XIAP), with accompanying cell migration and angiogenesis [154, 158,159,160]. Moreover, BPA at 100 μmol/L seems to be able to increase GPER protein levels in the nucleus, but had no influence in the cytoplasmic fractions [161]. On the other hand, low doses of BPA did not seem to have stimulatory effects via GPER [162]. The 4,40-thiodiphenol (TDP), a BPA derivative that exhibits more potent estrogenic activity than BPA does, can increase the GPER expression and activate the GPER-PI3K/Akt and ERK1/2 pathways [163].
Commercial dichlorodiphenyltrichloroethane (DDT) products consist of a mixture of compounds with the p,p9- and o,p9-isomers, both of which showed binding affinity for GPER, although it was higher in the case of p,p9-isomer [164, 165]. The degradation of DDT produces isomers of dichlorodiphenyldichloroethylene (DDE), p,p9-DDE and o,p9-DDE, which also exhibit binding affinity for GPER [140]. The 2,20,4,40-tetrabromodiphenyl ether (BDE-47), a flame retardant frequently used in furniture, infant products, and electronics, also seems to have effects as a GPER agonist [166].
Several pesticides also have been indicated as activators of GPER. Methoxychor showed ability to bind GPER and activate the GPER/EGFR signaling transduction pathway [140], whereas atrazine, induced ERK1/2 activation and the expression of c-fos and other E2-target genes. Atrazine and others chlorotriazines, including cyanazine and simazine were also shown to regulate GPER expression in breast cancer cells [167].
Polychlorinated biphenyls (PCBs) are another group of environmental xenoestrogens, including the phenolic derivative 2,29,59-PCB-4-OH, which exhibited low binding affinity for GPER [140]. Contrastingly, the high-affinity binding of GPER to another chlorinated endocrine disrupting chemicals, such as the insecticide kepone was indicated [140].
Also, the lipophilic bis(4-hydroxyphenyl)[2-(phenoxysulfonyl)phenyl] methane, present in cell culture medium as an impurity of phenol red (phenolsulfonphthalein) used as a pH indicator, exhibits estrogenic properties, however, its interaction with GPER remains unclear [164, 168].
In an exhaustive study of Peter Thomas’ group [140] comparing the estrogenic activity of a panoply of phytoestrogens and environmental contaminants, it was possible to hierarchize several of the compounds mentioned above concerning its ability to bind GPER. The phytoestrogen genistein was the most effective competitor for GPER, and BPA, and nonylphenol also displayed relatively high binding affinity . Kepone, DDT, 2,2′,5′,-PCB-4-OH and o,p′-DDE had lower affinity for GPER whereas o,p′-DDT, p,p′-DDE, methoxychlor and atrazine caused less than 50% displacement of tritiated-estrogen from GPER-containing membrane fractions [140]. Moreover, it was shown that genistein, BPA, nonylphenol and kepone act as GPER agonists sharing the mechanistic of adenylyl cyclase activation [140].
Other Compounds
Calixpyrroles belong to the category of macrocyclic compounds and are made up of pyrrole units assembled by quaternary carbon atoms at their 2,5-positions [169, 170]. A derivative of these compounds, the calix[4]pyrrole derivative [meso-octamethylcalix[4]pyrrole (C4PY)], acts as an antagonist of GPER preventing the ERK activation by E2 although without trigger ERK phosphorylation. Moreover, C4PY inhibited the E2 and GPER agonist-induced expression of c-fos and Egr-1 and Akt phosphorylation [171].
The parabens, methyl-, propyl- and butylparaben, also seem to activate GPER, inducing the activation of the ERK1/2 pathway, an effect mediated by the G protein βγ dimer. No activation was perceived concerning the cAMP/PKA pathway, and propylparaben was the only paraben able to activate Akt [172].
Reports also exist indicating that metallic compounds actions are mediated by GPER. Copper, an essential trace element naturally occurring in soil, water and air, has been implicated in tumor initiation and progression [173]. A recent study showed that GPER (together with HIF-1α) is required for the copper sulfate (CuSO4)-induced VEGF expression and proliferation of breast cancer cells [174]. Nevertheless, the ability of copper to directly activate GPER signaling requires confirmation. Arsenite and cadmium, environmental contaminants acting as endocrine disruptors, were shown to activate GPER leading to MAPK activation [175], with cadmium directly activating the receptor [176]. Cadmium-induced effects mediated by GPER included the rapid activation of ERK1/2 and Akt and stimulation of breast cancer cells proliferation [177,178,179]. Zinc is essential in the regulation of several cellular functions, and a recent study also demonstrated that the stimulatory effects of zinc chloride (ZnCl2) in breast cancer cells and cancer associated fibroblasts (CAFs) with the activation of ERK and Akt pathways are dependent on GPER [180].
Nicotinic acid, also designated niacin or vitamin B3, and nicotinamide were reported as agonists of GPER, inducing GPER-mediated ERK activation and gene expression, stimulating cell proliferation and migration [181].
It is important to refer that, despite the high homology of GPER amino acid sequence with the chemokine receptor subfamily of GPCRs, chemokines did not seem to activate GPER [47].
GPER Specific Ligands
The majority of endogenous and synthetic compounds with affinity for GPER also has the ability to bind the classical nuclear ERs. For this reason, it was necessary to find out specific ligands for GPER that would allow separating the contribution of each receptor subtype to the physiological effects of estrogens.
Virtual and biomolecular screening for chemicals with similarity to estrogens in a library with thousands of compounds, retrieved 100 strong candidates to be tested for GPER binding activity. One of these compounds presented agonist activity for GPER and was inactive for the classical ERs. It was called G1 (GPR30 -specific compound 1, a substituted dihydroquinoline, with a tetrahydro-3H-cyclopenta[c]quinoline core structure) [182] that still today is the true selective GPER agonist being widely used in in vitro and in vivo studies.
Binding affinity studies demonstrated a high-binding affinity of G1 for GPER yielding a Ki of 11 nM whereas for E2 the Ki was 5.7 nM. No significant binding of G1 was perceived for ERα and ERβ at concentrations up to 1 μM [182]. Moreover, functional studies showed that the G1 effects inducing Ca2+ mobilization and PI3K activation were exclusive of cells harboring GPER, being absent in cells expressing either ERα or ERβ [182].
More recently, an antagonist of GEPR closely resembling G1 but lacking the ethanone moiety was identified, the so-called G15 [183]. Competitive binding assays demonstrated that G15 binds GPER with an affinity of, approximately, 20 nM. Similarly to G1, G15 poorly binds ERα or ERβ at concentrations up to 10 μM [183]. G15 seems to be able to reduce Akt phosphorylation, and NF-kβ signaling [184].
However, some low-affinity cross-reactivity of G15 with the classical ERα was described. For this reason, efforts were made to identify an antagonist with improved selectivity for GPER. In this way, an isosteric G1 derivative, the G36 was synthesized. This new GPER antagonist showed diminished capability of activating ERα, while maintaining its GPER antagonist activity. Moreover, G36 was shown to selectively inhibit GPER activation of PI3K but not of ERα. Also, it inhibited estrogen and G1 effects on Ca2+ mobilization andERK1/2 activation, with no effect on EGF-mediated ERK1/2 activation [185]. Thus, the identification of G36 as a GPER antagonist with improved ER counter selectivity represented a significant step towards the development of new highly GPER selective therapeutics for cancer and other diseases. Indeed, both G1 and G36 have been envisaged as therapeutic tools [35, 186,187,188].
Other two original compounds, GPER-L1 and GPER-L2, were developed as GPER selective agonists [189], representing also valuable tools to disclose the pharmacologic actions of GPER and to discriminate more accurately the actions driven by each particular ER subtype. These compounds showed high affinity for GPER and were also capable of upregulating the expression of GPER target genes with higher efficacy than G1 or E2 [189]. More recently, as a strategy to find out a new GPER antagonist, two novel compounds with a structure based on pyrroloquinoxaline were synthesized; PBX1 and PBX2, which were described as selective antagonists having the ability to suppress GPER-dependent signaling [190].
The development of new and selective agonists and antagonists of GPER significantly advanced the current knowledge about the physiological roles of this receptor, controlling biological processes in healthy and pathological conditions. Also, this allowed and reinforced the consistency of targeting GPER as a potential therapeutic strategy, which could be achieved by activating or inhibiting its activity, depending on the deregulation of GPER identified in each particular disease.
Expression Pattern of GPER in Cancer Tissues
GPER is expressed practically in all organs and tissues of the human body and has several important physiological functions in healthy conditions. However, GPER deregulated expression has been associated with several diseases, such as cancer, which may include either upregulated or downregulated expression levels.
Cancer-related expression of GPER has been described both in male and female cancers, with a great representation in hormone-dependent cancers, but reports in other oncological conditions also exist (Table 5.2). However, GPER has been mainly associated with female cancers, particularly breast cancer, but also with the endometrium and ovary cancers. In man, testicular and prostate cancers are important targets of this estrogen receptor.
GPER was firstly identified in human breast cancer cases, and cell lines and, thus, not surprisingly, its function in carcinogenesis is intimately related to breast cancer. Several studies revealed that GPER is strongly expressed in normal breast tissue, with a variable expression among tumor specimens. However, studies show that GPER is detected in the majority of invasive breast tumors whereas only 42% of intraductal tumors were GPER-positive [191, 192]. Indeed, GPER association with breast cancer aggressiveness has been reported [39].
Concerning subcellular location (Table 5.2), GPER seems to be found in the cytoplasm [193], around the nucleus and specifically at the plasma membrane in breast cancer cases [194]. Moreover, the cytoplasmic location of GPER in breast cancer seems to be correlated with the less advanced tumor stages, better histologic differentiation, non-ductal histologic subtypes, and enhanced overall patient survival whereas GPER nuclear expression is associated with poorly differentiated carcinomas [195]. Also, GPER overexpression and plasma membrane localization were indicated as key events in breast cancer progression [194]. Oppositely, the absence of GPER at the plasma membrane is indicative of a better long-term prognosis of primary breast cancer [194], suggesting that membrane-triggered GPER signaling may favor tumor progression.
A significant association between GPER and ER expression, as well as a positive correlation of GPER with HER-2/neu, EGFR, C-erbB2 and CD133 expression, tumor size, metastasis, peri-nodal invasion, and lymph node status, were also described [39, 178, 192, 196,197,198]. Not consistently, other study found no correlation between GPER expression and ERα [193]. In the case of triple-negative breast cancers (TNBCs), which are defined by the absence of classical ERα, progesterone receptor (PR) and HER-2/neu, GPER expression is maintained [199,200,201] showing a nuclear location [195]. However, GPER expression seems to be restricted to a group of younger women and possibly associated with recurrence of disease since it happened in 22.2% of patients in the GPER-positive group against only 9.5% in the GPER-negative group [199]. This is further supported by findings showing that the in vitro inactivation of GPER reduces growth of TNBC cells, preventing the activation of the kinase Src [202]. Moreover, the phosphorylation of the EGFR was almost abolished, and c-fos induction was inhibited with GPER inactivation [202].
Other evidence exists implicating GPER in recurrence of breast cancer [198]. A study evaluating GPER expression in local and distant metastatic lesions found that almost 70% of specimens express GPER, and also identified a relationship between GPER positivity and resistance to tamoxifen because recurrent tumors displayed increased GPER expression [196, 203]. Accordingly, a more recent study evaluated 77 breast cancer tissues with 53 recurrent breast cancer specimens after tamoxifen treatment and found that GPER expression was increased in 73.58% of cases [204].
On the other hand, studies are proving that GPER expression decreases with the progression of breast cancer, in consequence of a reversible promoter inactivation by methylation [205, 206]. In addition, GPER down-regulated levels were suggested contributing to breast carcinogenesis and development of lymph node metastasis [34, 207]. Thus, GPER also has been proposed as a tumor suppressor gene [34, 207]. In line with these reports, the protective role of GPER in TNBC cells was described since its activation lead to inhibition of cancer cells growth [208]. Also, it was found that GPER expression in TNBC cases is negatively associated with high-grade tumors and lymph node metastasis, whereas displaying a significant and positive correlation with overall survival [209].
Concerning uterine tissues, GPER was described to be overexpressed in patients with endometriosis comparatively to the normal endometrium, suggesting the involvement of this receptor in disease onset [210, 211]. Endometriosis has been considered a risk factor for endometrial cancer, and in this way, it would be expectable a role for GPER in the endometrium cancer . Expectation confirmed by a study demonstrating that GPER modulates endometrial tumor growth by activation of its characteristic signaling pathways [35]. Besides that, GPER expression is augmented in endometrial carcinoma comparatively with non-neoplastic tissues, with 70% of endometrial carcinomas expressing GPER, against only 26.67% of normal endometrium [212]. However, contradictory reports also exist indicating a decreased expression of GPER in endometrial carcinoma comparatively to the normal endometrium [213, 214]. Moreover, GPER was found to be expressed in ER-negative endometrial carcinoma and in ER-positive and ER-negative endometrial cancer cell lines [212].
Endometrial cancers display GPER expression in the stroma and glandular tissue with protein expression being mainly cytoplasmic [215]. GPER expression was correlated with the grade of endometrial carcinoma but failed any association with FIGO stage, myometrial invasion, or peritoneal cytology [212]. On the other hand, others described that loss of GPER expression was significantly associated with more aggressive features of endometrial tumors and poor prognosis. This included high FIGO stage, non-endometrioid histology, presence of lymph node metastasis, aneuploidy, and ERα loss, which suggests a link between the absence of GPER and the development of an aggressive tumor phenotype [215].
In uterine carcinosarcoma, namely, in the glandular component, GPER expression is higher than that in the normal endometrium [216]. Moreover, GPER expression was higher in advanced stages of carcinosarcoma and seemed to be correlated with the expression of ERβ [216]. On the other hand, GPER is also highly expressed in uterine leiomyomas compared with their matched myometrium and, in this case, ERα also was overexpressed. Furthermore, GPER expression in uterine leiomyoma is detected in the nucleus, but in the myometrium, GPER localization is cytosolic [71].
GPER is expressed in ovarian cancer cell lines [217] and ovarian granulosa cell tumors [218, 219], and seems to be preferentially expressed in “high risk” epithelial ovarian cancer than in less aggressive ovarian tumors [40, 220]. Others also defended that GPER expression increases with the development and progression of ovarian cancer [40]. Accordingly, the high frequency of GPER expression in malignant ovarian endometriotic cysts comparatively with the benign forms was reported [221]. Moreover, GPER expression seems to be positively correlated with clinic pathological parameters, such as tumor stage, size, and lymph node metastasis, and also correlates with matrix MMP-9 expression, mainly in higher stage tumors [221]. In general, increased GPER expression is associated with aggressiveness of ovarian tumors and lower survival rates [40, 220, 221].
Testicular germ cell tumors (TGCTs) are the most common testicular solid cancer accounting for 90% of primary tumors and mainly affecting young men [222]. TGCTs are in majority seminomas, which were shown to overexpress GPER [37, 223,224,225]. The overexpression of GPER in seminomas comparatively to non-seminomas could be due to two polymorphisms frequently found in the promoter region of GPER in seminomas, rs3808350 and rs3808351 that cause a switch of the homozygous ancestral genotype GG to the homozygous AA genotype [223]. Thus, GPER has been considered a possible biomarker predictive of TGCTs [226]. It was also shown that GPER location in seminoma-derived cells was found at the cell membrane and cytoplasm, with a ratio of approximately 20%:80% [223]. The augmented expression of GPER was described for TGCTs, but GPER was also detected in Sertoli and Leydig cells tumors, embryonal carcinomas, and teratomas [224, 225].
The expression pattern of GPER and its biological roles in PCa will be discussed in a separate topic of the chapter.
Although GPER has been highly related to cancers of reproductive tissues, likely by their hormonal dependency, there are other cancer types displaying altered expression patterns of GPER.
In lung cancer, namely, adenocarcinomas, squamous cell carcinomas, and non-small cell lung carcinomas, GPER expression was significantly increased relatively to the surrounding non-tumor tissue, both at mRNA and protein level [36]. Also, non-small cell lung cancer cell lines display consistently higher expression of GPER relatively to immortalized normal lung bronchial epithelial cells [36]. Moreover, GPER expression in non-small cell lung cancer cells was shown to be nuclear and cytoplasmic, with cytoplasmic location following tumor stages IIIA–IV, lymph node metastasis, and poorly differentiated non-small cell lung cancer cells [227].
Although the expression pattern of GPER in human oral cancers needs to be fully characterized, this receptor was detected in non-neoplastic oral tissues, such as the submandibular and parotid glands, and tongue, and its functional role in oral squamous carcinoma cells also was suggested [184, 228].
In the case of thyroid cancer, a high expression of GPER comparatively to the nodular hyperplasia tissues was found, and associated with lymph node metastasis in papillary thyroid carcinoma [229]. Moreover, GPER , in cooperation with EGFR and CXCR1, seems to have an important role in the diagnosis screening to differentiate between malignant follicular thyroid carcinoma and benign follicular thyroid adenoma because it is highly expressed in malignancy [230].
GPER expression was also reported in other human cancers (Table 5.2), namely, leukemia [231], urothelial carcinoma [16, 232], pancreatic adenocarcinoma and mucinous neoplasm [233], cervical carcinoma [234], kidney carcinoma and adenocarcinoma [235], and pituitary tumors [236], which indicates a broad action of GPER in the control of cell fate and tissue homeostasis contributing to malignant transformation. Also, it is highly indicative that GPER expression is probably altered in other cancers that have not been evaluated yet.
The Role of GPER Controlling Cell Fate and Metabolism
GPER Actions in Cell Proliferation and Apoptosis
Abnormalities in the control of cell-fate decision commonly lead to the unbalance between proliferation and apoptosis being major drivers of carcinogenesis. GPER, the new actor in the estrogens’ “drama” that is expressed in a broad range of neoplastic and non-neoplastic tissues, seems to be one of the molecular protagonists in the regulation of cell fate, influencing cell proliferation, apoptosis and malignant features, such as, cell migration and invasion (Table 5.3).
Some studies have reported that GPER is able to stimulate cell growth, increasing the proliferative activity. Estrogens and the GPER selective agonist G1 were shown to increase the mitotic index in the epithelial non-neoplastic MCF10A breast cells, and also the proportion of dividing cells in normal and malignant human breast and breast cancer explants [237]. The dependency of GPER to promote breast cells growth was further confirmed by the estrogenic effects observed on ER-negative breast cancer cells [178]. Moreover, GPER activation in MCF10A cells led to the activation of ERK in a process requiring EGFR transactivation [237]. Interestingly, in breast CAFs, E2 seems to cause an interaction between GPER and phosphorylated EGFR, recruiting them to the cyclin D1 gene promoter [70]. In this CAFs, G1 activation of GPER resulted in transient increases in cell mitotic index, intracellular Ca2+, and ERK1/2 phosphorylation, linked with the promotion of proliferation and cell-cycle progression [238]. This supports the idea that GPER is involved in the functional connection between breast tumor cells and CAFs [239]. GPER activation in breast and endometrial cancer cells also was associated with the upregulation of Egr-1, a transcription factor involved in the promotion of cell proliferation. It was reported that G1 induces transcription of Egr-1 through GPER/EGFR/ERK signaling and induces the recruitment of Egr-1 to the CTGF and cyclin D1 promoter sequences [98].
In endometrial cancer cells and leiomyoma cells GPER increased cell proliferation also through the MEK/ERK MAPK pathway [126, 212, 240,241,242]. Pretreatment of endometriotic cells with G1 stimulated cell proliferation accompanied by rapid Akt phosphorylation, which was reversed by the GPER antagonist G15 [243]. Accordingly, a recent study showed that targeting GPER by the overexpression of the regulatory miR-424, decreased E2-induced cell proliferation by inactivation of the PI3K/Akt signaling [244].
In the case of ovarian cancer cells, an augmented proliferation was observed upon G1-stimulation and GPER activation, which was underpinned by an increased number of cells in S-phase, and upregulated levels of c-fos, cyclin D1, cyclin E, and cyclin A proteins [96, 245].
In primordial germ cells, precursors of both sperm and eggs, GPER activation by estrogens induced cell proliferation through Gβγ-subunit protein- and matrix metalloproteinase-dependent transactivation of the EGFR [17]. EGFR signaling activated the PI3K/Akt/β-catenin pathway, increasing c-fos, c-myc, and cyclin D1/E expression [17]. The proliferative effects of GPER over germ cells were confirmed at post-natal stages. G1 induced proliferation of the spermatogonial GC-1 cell line, with the upregulated expression of cyclin D1 and through a cross-talk between GPER and ERα, and activation of the EGFR/ERK/fos pathway [246].
Also in thyroid cancer cells, GPER activation caused transcriptional activity of c-fos promoter with increased expression of c-fos, cyclin A, and cyclin D1 [247].
The GPER also contributed to the proliferation and survival of mantle cell lymphoma cells, and its expression levels were correlated with Akt and MAPK phosphorylation, as well as, with cyclin D1 expression [248]. The activation of MAPK pathway by GPER also seems to be involved in the induction of proliferation in lung cancer cells [227].
There are also reports of GPER stimulation of cell proliferation through its activation by other compounds than estrogens or G1. It is the case of the estrogen-mimicking compound used in plastic production BPA that activates GPER with enhanced proliferation of breast cancer cells and augmented levels of c-fos, Egr-1, and CTGF proteins [98, 249]. BPA also was shown to increase proliferation of spermatogonial cells and the proliferative activity in testicular seminomas, effects mediated by the GPER [155, 156, 250, 251].
Also, the ER antagonist 4-hydroxytamoxifen, known to act as an agonist of GPER [126], stimulated breast [97, 98] and thyroid [247] cancer cells growth. Regarding thyroid cancer cells, similar effects were seen with the phytoestrogen genistein [247].
Overall, the facts described above argue for the “villain role” of GPER in tissue homeostasis by its ability to promote cell growth and proliferation. However, the other face of GPER as the “good guy” is sustained by many other studies that demonstrate it suppressive effects on cell proliferation, including in tissues where the pro-proliferative activity was described.
The activation of GPER inhibited the growth of ER-negative breast cancer cells with the cell cycle arrested at G2/M [252]. These effects were underpinned by the downregulated expression of G2-checkpoint regulator cyclin B and increased expression of p53, as well as, by enhanced p53 phosphorylation at serine 15, which promotes its nuclear translocation and inhibits ubiquitylation. The augmented levels of p53 were also accompanied by increased expression of cell cycle inhibitor p21 [252]. GPER also inhibited proliferation of ER-positive breast cancer cells, blocking cell cycle at G1, and decreasing the population of cells in S-phase, since both p53 and p21 proteins were upregulated by G1 administration [178]. G1 suppression of cell growth and arrest of cell cycle lead to caspase activation and apoptosis. Moreover, it was shown that G1 could bind the colchicine binding site of tubulin, inhibiting tubulin polymerization and the subsequent assembly of mitotic spindle apparatus in breast cancer cell mitosis [253].
In human cervical cancer cells, GPER activation induced G2/M cell cycle arrest and down regulated cyclin B expression, inhibiting cell proliferation through ERK1/2 and EGFR signaling [234]. Also, in human bladder-derived T24 carcinoma cells, E2 inhibited cell growth via GPER mediated phosphorylation of ERK [232].
In ovarian cancer cells, it was shown that G1 blocks tubulin polymerization hampering the assembly of microtubules, which led to the cell cycle arrest and suppression of proliferation [254]. Similar G1 effects were observed in endothelial cells, with inhibition of DNA synthesis and accumulation of cells in S and G2 phases of cell cycle [255], and adult female rats hippocampus that displayed significantly diminished cell proliferation [256].
The activation of GPER was also associated with the decreased proliferation of adrenocortical carcinoma cells [186], and GPER-positive endometrial adenocarcinoma cell lines HEC-1A and RL95-2, but not in GPER-negative endometrial adenocarcinoma HEC-1B cells [213].
In the other plate of the balance of tissue homeostasis, there is apoptosis, the fundamental biological process of programmed cell death that also seems to be regulated by the GPER. Curiously, and as discussed for cell proliferation, GPER actions in the control of apoptosis are the two faces of the same coin. Studies exist reporting that GPER activation diminishes apoptosis, while others defend the opposite.
The apoptotic process may be triggered by two distinct and interrelated pathways, the intrinsic (or mitochondrial) and the extrinsic (or death receptor) pathway that converge at the activation of apoptosis effector caspase-3 [257]. Nevertheless, the GPER effects have been mainly related to the mitochondrial pathway and altered expression or activity of the Bcl-2 protein family of apoptosis regulators [258]. The antiapoptotic effect of GPER was stated, for example, in the ERα-negative ovarian cancer cells OVCAR5, by diminishing the expression of cleaved-caspase-3 [245]. In rat Sertoli cells, GPER seems to decrease apoptosis, by increasing the expression of Bcl-2 and decreasing Bax levels [259], respectively, anti- and pro-apoptotic members of the Bcl-2 family [258]. The same effect of GPER activation elevating Bcl-2 levels and reducing Bax with the consequent inhibition of apoptosis was seen in myocardial cells following ischemia/reperfusion injury [260]. The GPER activation through the ERK pathway also was seen to be cardioprotective by inhibiting the opening of mitochondria permeability transition pore mPTP [261]. Furthermore, GPER stimulation enhanced mitochondrial function and decreased oxidative stress in cardiac muscle [262]. Moreover, decreased TNF-α levels were reported following ischemia-reperfusion and GEPR activation [260]. Accordingly, E2 enhanced Bcl-2 expression and CREB phosphorylation, preventing oxidative stress-induced apoptosis in keratinocytes by phosphorylating cAMP response element-binding protein via cAMP/PKA pathway, an effect mediated via membrane GPER [99]. The GPER also showed antiapoptotic and protective effects in spinal motor neurons after injury through the activation of PI3K/Akt pathway [263].
Other mechanism associated with the GPER inhibition of apoptosis was reported in the ER-positive MCF7 breast cancer cell line, and involves FOXO3a inactivation [264]. FOXO3 is a transcription factor that specifically induces the transcription of proapoptotic genes, such as Bim, p21, and p27 [265]. The activation of GPER leads to rapid FOXO3a translocation to the cytoplasm, and this process seems to be achieved by the p110α catalytic subunit of PI3K as a result of EGFR transactivation. Additionally, G1 stimulation of MCF7 cells resulted in decreased caspase activation under proapoptotic conditions [264]. In this report, the SERMs tamoxifen and raloxifene, as well as ICI 182,780, also were able to mediate FOXO3a inactivation in a GPER-dependent mechanism [264].
The antiapoptotic action of GPER was also evidenced by the use of GPER antagonist G15. Administration of this compound induced apoptosis of human oral squamous carcinoma cells, indicating that GPER activation is needed to sustain cell survival and diminish apoptosis [184].
Nevertheless, a substantial number of studies report the proapoptotic nature of GPER. In ER-positive MCF7 breast cancer cells, and contrastingly with the stated above, the proapoptotic role of GPER also was described. Knockdown of receptor was linked to decreased basal expression of tumor suppressor protein p53, and increased apoptosis and decreased cell-cycle progression [266]. This proapoptotic action of GPER was also found in the ER-negative SK-BR-3 breast cancer cells, concomitantly with enhanced expression of Bax, Bim, and cleaved-caspase-3, and diminished expression of Bcl-2 [205, 252]. Similar effects were seen in the triple-negative MDA-MB-231 and MDA-MB-468 breast cancer cells [208] that, despite devoid of classical ERs, are known to express GPER [208], which demonstrates the importance of GPER inducing apoptosis.
Also in other tumor types, the GPER effects inducing apoptosis were indicated. It is the case of tumor Leydig cells, in which GPER activation led to apoptosis, with decreased Bcl-2 and increased Bax expression, diminished cytochrome c release, and decreased activation of caspase-3 and poly (ADP-ribose) polymerase 1 (PARP-1) [267]. In ovarian cancer cells, the GPER agonist G1 caused DNA fragmentation, increased the expression of cell-cycle inhibitor p21, and decreased the expression of Bcl-2 and cleavage of PARP and fodrin, two important markers of apoptosis [254]. Enhanced caspase-3 activation and apoptosis in response to G1 stimulation and on the dependency of GPER actions were also reported in human ovarian endometriotic stromal cells [268], lung cancer cells [269] and adult T-cell leukemia cells [231].
Moreover, also in the adrenocortical H295R carcinoma cells, G1 treatment was shown to cause morphological changes in cell nuclei, DNA damage and apoptosis by the activation of the intrinsic pathway [186]. GPER agonist treatment increased Bax expression whereas decreasing Bcl-2, and increased cytosolic cytochrome c levels decreasing its content in the mitochondrial compartment. Accordingly, activation of the initiator caspase-9, as well as, the executioners caspase-3/7 was detected [186].
There is also the example of rat pachytene spermatocytes, in which GPER activation by E2 or G1 up-regulates the expression of proapoptotic factor Bax whereas downregulating the cell cycle regulators cyclin A1 and B1 [80]. Moreover, it was demonstrated that the rapid EGFR/ERK/c-Jun pathway modulates gene expression towards the balance between cellular proliferation and apoptosis [80]. Similarly, in the mouse spermatocyte-derived cell line GC-2, GPER activation caused rapid ERK, c-Jun and p38 phosphorylation, Bax upregulation, Bcl-2 downregulation, cytochrome c release, caspase-3 and PARP activation, DNA damage and increased expression of cell cycle inhibitor p21 [270].
GPER regulation of cell proliferation and apoptosis has also been linked with the regulation of other associated processes, namely, oxidative stress and Ca2+ homeostasis. In lung cancer cells, it was shown that GPER regulates the NO levels, and superoxide dismutase (SOD), catalase and glutathione peroxidase (GPx) activity, contributing to decreased cell proliferation and increased apoptosis [269, 271]. GPER was able to increase T-type Ca2+ channels currents in trigeminal ganglion [272], and the activity of L-type Ca2+ channel α 1D subunit in endometrial carcinoma cells and breast cancer cells, which was required for the E2-stimulated Ca2+ influx associated with the promotion of cell proliferation, and development of endometrial cancer [273, 274].
In the scenario of cell-fate decision and maintenance of tissue homeostasis, it became evident the opposite effects of GPER in the control of cell proliferation and apoptosis. This duality of action most likely depends on a panoply of factors that may include the type of tissue and physiological context, the dose of activators and time of exposure, as well as other unforeseeable variables. The different effects of GPER also would be explained by a regulatory role of GPER shaped by the tissue specificity in particular environmental and biological conditions.
GPER Influence Over Cell Migration and Invasiveness
Cell migration and invasiveness are coordinated biological processes that play a major role in cancer progression being closely related to metastization . The loss of cell-cell adhesion is a driven event for malignant cells evasion from their primary sites, which also depends on the degradation of the extracellular matrix, acquisition of an invasion phenotype, and finally, invading and metastasizing to other organs/tissues [275]. Indeed, the great majority of cancer deaths (>90%) are caused by metastasis rather than by the primary tumors [276], which renders cell migration a therapeutically relevant target point. Both migration and invasion seem to be promoted by GPER in ER-negative breast cancer cells through the activation of ERK and Akt pathways, nuclear translocation of NF-κB and increased expression of interleukin-8 (IL-8) [277]. The role of this cytokine in the progression and metastasis of a variety of human cancers has been discussed [278]. GPER activation also leads to migration and invasiveness of TNBC cells and inflammatory breast cancer cells, responses mediated by the activation of the ERK1/2 pathway [279, 280]. Furthermore, GPER seems to upregulate β1-integrin expression, through EGFR/ERK signaling pathway, which promotes migration of CAFs and epithelial-mesenchymal transition of tamoxifen-resistant breast cancer cells [204], contributing to tamoxifen resistance via interaction with the tumor microenvironment [204, 281]. Moreover, GPER activation can lead to the increased expression of IL1β in CAFs and IL1 receptor 1 (IL1R1) in breast cancer cells, promoting the interaction between these two cell types, the upregulation of inflammatory target genes, inducing migration and invasion of breast cancer cells [282]. Accordingly, GPER inhibition with G15 seems to increase the sensitivity of epithelial breast cancer cells to doxorubicin by preventing epithelial-mesenchymal transition [283].
GPER actions prompting cell migration and invasion were also described in ER-positive breast cancer cells, through the activation of ErbB2-ERK signaling transduction pathway [284]. In this breast cancer cell type, GPER enhanced migration also by mediating the dramatic proteolysis of cyclin E, with the involvement of EGFR signaling [281]. Other results showed that E2 and ICI 182,780 enhanced adhesion of MCF7 breast cancer cells to matrigel, with increased autolysis of calpain 1 and proteolysis of focal adhesion kinase (FAK), with calpain activation through the ERK1/2pathway [285]. Also, the xenoestrogen BPA stimulated migration of breast cancer cells and CAFs via GPER [249] by FAK, Src and ERK2-dependent pathways [286].
Interestingly, antagonizing GPER activity by natural compounds, like baicalein, diminished the expression of GPER target genes, including cysteine-rich 61 (CYR61) and CTGF, and suppressed E2-stimulation of migration and invasion of breast cancer cells [138].
The pro-invasiveness effects of GPER were also identified in ovarian cancer cells OVCAR-5 and SKOV3 with modulation of expression and activity of MMP-2 and MMP-9, extracellular matrix proteins with a determinant role in cancer cell invasion and metastasis [287, 288]. Similar effects dependent on increased MMP-2 and MMP-9 production were seen in the endometrial Ishikawa and KLE cancer cells [241]. In the endometrial cancer cell line RL95-2, GPER mediated carcinogenesis and invasion via the activation of MEK/ERK MAPK pathway [240]. Moreover, the phosphorylation of FAK, a tyrosine kinase with a key role in tumor cells invasiveness [289], also was involved in the migration of Ishikawa and RL95-2 cells induced by GPER activation [290]. The association of MAPK pathway with cell migration and invasion in response to GPER activation also was described in lung cancer cells [199]. Also in lung cancer and mesothelioma, GPER contributes to the chemotaxis and migration, through IGF-I actions [291].
In renal cell carcinoma, GPER activation mediated cell invasiveness via PI3K/Akt/MMP-9 signals [235].
The environmental pollutant BDE-47 increased migration and invasion of neuroblastoma SH-SY5Y cells in a mechanism dependent on GPER [166]. The associated molecular events included the downregulated expression of E-cadherin and zona occludin-1, and the upregulated expression of MMP-9, via activation of PI3K/Akt signaling pathway [166].
Nevertheless, contrary evidence exists depicting the role of GPER suppressing cell migration and invasion (Table 5.3). A recent study has shown that the activation of PI3K/Akt and ERK1/2 pathways by the GPER specific agonist G1 suppress migration and invasion of TNBC cells. Other responses included the inhibition of the epithelial mesenchymal transition by reducing the phosphorylation, nuclear localization, and transcriptional activity of NF-kB, [209]. There is also evidence that E2-effects mediated by the membrane GPER in human metastatic breast cancers lead to decreased cell adhesion, through a PKA-dependent mechanism requiring the activity of voltage-gated sodium channels (VGSCs) [292].
In granulosa cell tumors, E2 decreased cell migration and matrix invasion, effects accompanied by GPER inhibition of ERK1/2 signaling through a non-genomic mechanism [219]. Other studies with ovarian cancer cells suggested that E2 inhibits tumor invasion, by inhibiting EGF-induced cell migration and the expression of urokinase plasminogen activator receptor (uPAR) expression , effects mediated by GPER [293]. Also in lung, and contrarily to the studies mentioned above, the activation of GPER showed to inhibit the migration of non-small cell lung cancer cells, suppressing the activity of IKK-β and NF-κB [294].
Angiogenesis, Inflammation and the GPER
Angiogenesis and inflammation are other important hallmarks in tumor progression fueling cancer cell growth within the “hostile” tumor microenvironment. GPER activation increased VEGF levels in ER-negative breast cancer cells and CAFs via upregulation of the HIF1α in consequence of activation of the EGFR/ERK/c-fos signaling pathway [83]. Moreover, the receptor seems to be involved in the formation of human endothelial tube, enhancing angiogenesis and tumor progression [83].
The GPER knockout mice display a pro-inflammatory phenotype with augmented levels of the pro-inflammatory and immunomodulatory cytokines IL-1β, IL-6, IL-12, TNFα, monocyte chemotactic protein-1 (MCP-1) , interferon γ-induced protein 10 (IP-10) and monokine induced by γ interferon (MIG), concomitantly with the decreased expression of the adipose tissue-specific cytokine adiponectin [295]. Contrastingly, the anti-inflammatory role of GPER was shown in endothelial cells, in which, receptor activation counteracted the TNF effects inducing upregulation of pro-inflammatory proteins, namely, intercellular cell adhesion molecule-1 (ICAM-1) and vascular cell adhesion molecule-1 (VCAM-1) [296]. Moreover, airway inflammation was suppressed by the GPER agonist G1 in a mouse model of asthma, apparently via IL-10 [297]. In human breast cancer cells, GPER inhibited the TNFα-induced IL-6 expression, probably through blockage of NF-κB promoter activity [298]. Consistent with that findings, a recent study in a GPER knockout mouse model, showed accelerated development of liver tumors, with immune cell infiltration, fibrosis, and production of inflammatory factors, including IL-6. More studies are warranted to establish the role of GPER in angiogenesis and inflammation.
GPER as a Regulator of Cancer Cell Metabolism?
In the last years, the ability of tumor cells to reprogram metabolism, sustaining their high energy requirements, proliferation, and survival, has been indicated as a characteristic of malignant transformation and recognized as a hallmark of cancer [299]. However, the most well-known adaptation of cancer cell metabolism was described in the 1930s by Otto Warburg and is known as the “Warburg effect” that consists in the increased glucose consumption followed by the augmented production of lactate instead of the oxidation of pyruvate in mitochondria, even under aerobic conditions [300]. In the light of available literature, GPER has “something to say” in the control of the metabolic process. GPER knockout female mice showed increased plasma glucose levels, leading to hyperglycemia and glucose intolerance, associated with the decreased expression of insulin in isolated pancreatic islets and diminished insulin release both in vitro and in vivo [301]. Likewise, glucose intolerance and insulin resistance were reported in the GPER knockout male mice [295]. In agreement, GPER seems to induce insulin secretion in pancreatic β-cells under low- and high-glucose conditions, through the activation of EGFR, ERK and PI3K/Akt pathways [302]. Curiously, insulin resistance is closely related to endometrial oncogenesis, and it seems to up-regulate Ten-Eleven Translocation 1 (TET1) that can up-regulate the GPER expression, activating PI3K/AKT signaling pathway and promoting cell proliferation [303]. Available data revealed an important role of GPER in glucose metabolism though in the particular case of cancer cells, information relating GPER with glycolytic metabolism is scarce, being an issue that deserves attention of direct studies. Nevertheless, Yu et al. [304] first reported the interplay between breast cancer cells and CAFs concerning glucose metabolism. This study showed that the activation of the PI3K/AKT signaling pathway in breast cancer cells induces the cytoplasmic translocation of GPER in CAFs, leading to the activation of GPER/cAMP/PKA/CREB signaling and to the aerobic glycolysis switch in CAFs. In turn, the glycolytic CAFs feed breast tumor cells with extra pyruvate and lactate augmenting mitochondrial activity. Moreover, cytoplasmic GPER expression in stromal fibroblasts predicted high tumor metabolic activity and potent energy transfer between the stroma and cancer cells [304].
Besides glycolysis, other energy routes are involved in the metabolic adaptation of cancer cells, namely, glutamine metabolism, and its resulting product glutamate [305]. The glutamate transporter-1 (GLT-1) is an essential player removing the extracellular excess of glutamate. GLT-1 expression was shown to be increased by GPER activation triggered by G1 in rat primary astrocytes, which was accompanied by the increased uptake of glutamate [306]. The expression of glutamate aspartate transporter (GLAST), other transporter involved in glutamate uptake, was also increased in response to G1 [307]. Moreover, the mechanistic under this regulation was outlined with effects reported to occur via the MAPK/ERK, PI3K/Akt, TGF-α/EGFR, Src, NF-κB and CREB pathways [307]. Further studies are warranted to confirm whether GPER actions regulate glutamine and glutamate metabolism in cancer cells, and if it has impact on disease progression and aggressiveness.
GPER also seems to have a major role in the regulation of lipid metabolism, another energetic pathway widely altered in cancer cells . Besides having a glucose intolerance phenotype, GPER knockout male mice display an altered lipid profile with increased cholesterol and triglyceride levels [295], which was corroborated by in vitro findings. GPER activation decreased triglyceride accumulation in cultured rodent β cells and reduced lipid synthesis in pancreatic islets by reducing the expression and activity of fatty acid synthase (FAS), the master effector of de novo lipogenesis [308]. This study also showed that the β cell transcription factor pancreatic and duodenal homeobox 1 (Pdx1) and the downstream target genes, such as proinsulin 1 (Ins1), glucose transporter 2 (GLUT2), and glucokinase (Gckr) were downregulated by E2 via GPER action [308]. Furthermore, the FAS is the target of lipogenic transcriptional regulators, namely, the sterol regulatory element-binding protein 1c (SREBP1c), the carbohydrate response element binding protein (ChREBP), and the liver X receptor (LXR) [309,310,311], which were suppressed in response to GPER activation [312].
However, in breast (SkBr3), colorectal (LoVo), and hepatocarcinoma (HepG2) cancer cells and CAFs, GPER seems to up-regulate FAS expression and activity, through the EGFR/ERK/c-fos/AP1 transduction pathway [313]. Other studies reported that the GPER action increased the expression of low-density lipoprotein (LDL) receptor, and that G1 stimulation induced the uptake of LDL in liver cells [314, 315]. Curiously, GPER promoted adipogenesis in vitro and seems to be involved in the development of obesity in female mice exposed to a high-fat diet since GPER knockout mice were resistant to diet induced-obesity, glucose intolerance and insulin resistance [316].
Malate dehydrogenases (MDHs) are metabolic enzymes that function as transcriptional factors to regulate the expression of oncogenes and tumor suppressor genes. The expression of MDH2, one of the isoforms of MDHs involved in citric acid cycle in mitochondria [317], was shown to be increased in endometrial cancer cells in response to GPER activation [318]. Moreover, the augmented expression of MDH2 lead to enhanced cell proliferation, migration and invasion but inhibited apoptosis of endometrial cancer cells by suppressing PTEN expression [318].
In sum, GPER has important roles in insulin sensitivity, glucose tolerance, adiposity and energy balance in many cell types, which ignites the curiosity about the activity of GPER in the metabolic reprogramming of cancer cells. Also, it is liable to speculate that GPER selective ligands would have therapeutic value for cancer treatment targeting metabolism.
GPER in Prostate Cancer
PCa is one of the most common oncological disorders in men, being highly frequent in men over the age of 50 [319]. Indeed, aging is the main risk factor for PCa, which raises the concern about its incidence in the next years considering the population aging in consequence of the increased expectancy of life. The vast majority of PCa patients (90%) develop castration-resistant PCa (CRPC) , an advanced metastatic form of disease, characterized by its aggressiveness and resistance to the classical anti-androgen therapies , which remains incurable with an average survival time of only 16–18 months [320, 321]. The search for new and effective approaches for better management and treatment of both localized and metastatic PCa remains crucial and urgent.
It is well established that the development and progression of PCa are strongly regulated by sex steroid hormones, with the male hormones androgens highly implicated in the regulation of prostate functions from the embryonic development to adulthood, but also in the onset of prostate malignancy [322]. Estrogens, classically viewed as female hormones, also seem to have a relevant role in PCa with some studies reporting their actions as causative factors in prostate carcinogenesis [323, 324]. On the other hand, estrogens have been used to treat PCa by its negative feedback actions at the hypothalamus and pituitary reducing circulating androgens levels [325]. However, has also been shown that estrogens have beneficial direct effects on PCa cells [326]. Independent studies have indicated that these steroids can be protective against PCa by their proapoptotic and antiproliferative actions over prostate cells [326, 327].
Estrogenic actions through the interaction with the classical nuclear estrogen receptors, ERα and ERβ, and involving genomic responses characterized by changes in gene transcription and protein de novo synthesis have been reported in both non-neoplastic and neoplastic prostate cells [328]. However, the activity of these receptors in PCa relies on the paradigm that ERα is responsible for the proliferative effects of estrogens being oncogenic whereas ERβ is considered protective, anti-carcinogenic and related with the activation of apoptosis [329].
Also, the GPER has been identified in normal human prostate, and benign and neoplastic conditions. The prostate gland mainly encompasses two compartments : the fibromuscular stroma and the glandular tissue. In the glandular epithelium, it is possible to distinguish two histological layers, the secretory luminal layer consisting of tall columnar cells responsible for the production of prostatic secretions, and an underpinning basal layer of cuboidal epithelial cells. The population of basal epithelial cells has shown to be heterogeneous and containing adult prostate stem cells, which have been proposed as cancer stem cells in the origin of PCa [330]. In the human benign prostate gland, a strong GPER expression was observed in the cytoplasm of basal epithelial cells [331]. Therefore, it is liable to assume that GPER may the mediator of estrogenic actions in this proliferative prostatic compartment. Accordingly, GPER expression was found in prostaspheres derived from human normal adult prostate stem cells [332].
GPER also was found in human prostate epithelial cells, displaying both membrane and cytoplasm localization [332,333,334]. Furthermore, a weak staining in the cytoplasm of stromal cells of benign prostate was also detected, suggesting the possible involvement of this receptor in estrogen signaling between stromal and epithelial prostatic compartments [331]. Accordingly, GPER was found to be expressed in human primary prostate stroma cells, derived from fresh surgical prostate specimens of benign prostate hyperplasia (BPH) , and in the normal human prostate stroma cell line, WPMY-1 [335].
The reports characterizing the GPER expression in neoplastic conditions are relatively scarce, but a study found that GPER was expressed in 97.5% of all prostate tumor cases evaluated [336]. It was described that pre-neoplastic lesions (high-grade prostatic intra-epithelial neoplasia) show higher GPER expression comparatively with non-neoplastic tissues, and that GPER expression decreases from moderately to poorly differentiated PCa [331]. Moreover, GPER expression was correlated with the Gleason score of prostate adenocarcinoma being intense in Gleason patterns 2 and 3, and weak to moderate in Gleason pattern 4 [331], which indicates an inverse relationship between GPER expression and neoplastic cell differentiation. Despite the predominant, and sometimes nearly exclusive, cytoplasmic expression of GPER in PCa cases, areas with membrane and nuclear staining were also found [331, 336, 337].
Considering the androgen-sensitive stage of disease and CRPC, GPER seems to be more expressed in CRPC cases; 80% of metastatic CRPC highly express GPER, against only 54% of the primary PCa cases [338]. However, no correlation was found between GPER expression and, age, the Gleason score of primary cancer or PSA level. The type of androgen deprivation therapy, or duration of treatment also were not associated with GPER [338]. These results are not totally in agreement with the findings obtained in PCa cell lines. GPER expression levels were markedly higher in the normal progenitor prostate cells relatively to the androgen-sensitive PCa cell line LNCaP [332]. In CRPC cell line models PC3 and DU145, GPER expression was higher in PC3 cells, which mimic a more aggressive metastatic stage of disease [334]. Recent findings from our research group also demonstrated that GPER expression tends to be lost with the acquisition of the castration phenotype and aggressiveness of PCa cell line models; GPER expression in LNCaP > PC3 > DU145 cells (results to be published elsewhere).
As previously discussed for other cancer types, also in PCa, the GPER dual-mode of action has been described with opposite effects arising from separate independent studies. Some authors argue that GPER is involved in PCa development and progression based on the assumption that GPER may mediate the estrogen-initiated transformation of prostate epithelium derived from normal human prostate stem-progenitor cells, and promote the progression to invasive adenocarcinoma [332]. These data were obtained in a novel chimeric mice prostate model containing human-rat prostate tissues . Human prostate progenitor cells cytodifferentiated in chimeric prostate tissue originating epithelial hyperplasia, prostate intraepithelial neoplasia and PCa after exposure of nude mice to elevated concentrations of testosterone plus E2 [332]. The pro-tumor action of GPER was also supported by the fact that its activation by the specific agonist G1 induced growth of normal stromal prostate cells, but not of BPH-derived cells [339]. Furthermore, GPER activation induced ERK1/2 phosphorylation , which was suggested contributing to PCa progression and hormonal independence in the PC3 cell line [333].
On the contrary, a substantial body of evidence defends the protective role of GPER in PCa. Treatment of LAPC-4 (androgen-sensitive) and PC3 (castration-resistant) PCa cells with E2 or DES identified the growth inhibitory activity of GPER triggered by different mechanisms [340]. Also, G1 administration showed to inhibit growth of both androgen-sensitive (LNCaP) and CRPC (DU145 and PC3) cell line models [334]. The agonist G1 induced a persistent cell-cycle arrest at the G2/M phase in LNCaP and PC3 cells , which resulted in enhanced apoptotic activity, as indicated by the increase in the Annexin V–positive cell population [334]. Moreover, G1 effects mediated by GPER induced the activation of ERK1/2 and c-jun/c-fos dependent upregulation of p21, which was accompanied by the downregulated expression of G2-checkpoint regulators, such as cyclin B1, cyclin dependent kinase 1 (cdc2) and its phosphorylated proteins, as well as by the diminished levels of cdc25C and cyclin A2 [334]. The mechanism involved in the GPER sustained activation of ERK1/2 was disclosed recently being shown that it depends on the activation of Gαi1 proteins, which are highly expressed in PCa cells [341].
Interestingly, the low GPER expression described in poorly differentiated PCa was associated with an increased expression and activity of Akt, and the transcription factor CREB [331], indicating that loss of GPER may promote PCa cell survival and proliferative activity.
Other relevant study in this field, using LNCaP (androgen-sensitive cell line) and PC3 (castration-resistant cell line) xenografts as PCa models, reported that GPER activation by G1 inhibited growth of castration-resistant, but not of androgen-sensitive tumors with no observable toxicity [338]. Growth inhibition of castration-resistant tumors by G1 was underpinned by the increased apoptosis, demonstrated by the increased number of cleaved caspase 3-positive cells [338]. Other study, similarly described the in vivo anti-cancer role of GPER in PC3 xenografts. G1 administration significantly suppressed tumor growth having no effect on growth and histological features in the prostates of intact mice [334]. Moreover, this study showed that G1 treatment only inhibited the growth of PCa and actively proliferating BPH cells without affecting growth of quiescent cells.
In agreement with the in vitro and in vivo anti-tumorigenic actions of GPER mediated by estrogens and G1, a study with natural compounds also found decreased proliferation and increased apoptosis of PCa cells in response to GPER activation. The SDG, a lignan extracted from flaxseed was shown to suppress the development of BPH in a rat model [151]. ENL, the metabolite of SDG inhibited prostate cell growth, which significantly restricted the enlargement of rat prostate [151]. Mechanistically ENL activated the ERK pathway causing cell cycle arrest with upregulation of p53 and p21 and downregulation of cyclin D1 [151].
The available literature unquestionably places GPER as a modulator of PCa cells growth regulating the expression of cell cycle-regulators and other cellular elements, but its influence over the control of metastatic features also was reported. G1 treatment inhibited migration and the invasion properties of both PC3 and DU145 cells by reducing the formation of filopodia and stress fibers [341]. G1 administration in vivo was also capable of reducing the intratumoral microvessel density in a castration-resistant xenograft tumor model [338], suggesting the anti-angiogenic role of GPER in PCa.
Other described effect of GPER in prostate is related with inflammation , with its activation leading to increased expression of COX-2 and augmented secretion of IL-8 by human prostate cells [342]. The pro-inflammatory actions of GPER were further supported by the observed marked intratumoral infiltration of neutrophils and upregulated expression of neutrophil-related chemokines and inflammation-mediated cytokines in a CRPC model after treatment with G1 [338].
In what concerns cancer cells metabolism, there are no reports implicating estrogens and GPER actions in the metabolic reprogramming. However, the emergent impact of metabolism as a therapeutic target together with others and ours recent findings highlighting the role of sex steroid hormones as metabolic regulators [343,344,345] strongly encourage opening this “avenue” of research.
Overall, the high expression of GPER in PCa, particularly in CRPC, and the demonstrated beneficial effects of G1 agonist counteracting the malignant behavior of PCa and BPH cells, without affecting non-proliferating cells, confer GPER the “status” of a therapeutic target. However, and despite some important advances characterizing GPER activity in prostate cells and tissues, much more investigation is needed to fully resolve the multiple GPER’ actions in PCa and its therapeutic potential.
Conclusions
GPER is a seven-transmembrane receptor with a wide mode of action activating several intracellular signaling pathways involved in the genomic and non-genomic effects of estrogens. In addition to E2 and G1, the most potent activators of GPER, several other compounds with the ability of binding GPER acting as agonists or antagonists have been pointed out. The astonishingly increasing list of these compounds, encompass hormone ligands, synthetic compounds and environmental phytoestrogens and xenoestrogens, which places GPER in the physiological context of normal and oncological conditions, but also as a target of endocrine disruption. The diversity of biological processes under GPER control mainly includes cell proliferation, apoptosis, cell migration and invasion, angiogenesis, inflammation, and metabolism.
The multifaceted GPER is expressed in a broad range of neoplastic and non-neoplastic tissues, which further extends its broad scope of action. The development of GPER specific agonists and antagonists, as well as cell and animal knockout models have contributed greatly to ascertain its role in cancer and other diseases. GPER was associated with the development and progression of breast, ovarian, endometrial and testicular cancers. However, other strong evidence of GPER actions counteracting known hallmarks of cancer as exacerbated proliferative activity and resistance to apoptosis support its role as a tumor suppressor.
In prostatic tissues, GPER is expressed both in normal gland and PCa. Also in this case, a duality in the GPER role has been reported. Studies arguing the causative role of GPER in prostate carcinogenesis are available in the literature, co-existing with others defending the protective action of GPER in PCa development. Reports indicating the high expression of GPER in PCa cases, together with its effects suppressing cell growth, also allow speculating about its usefulness as a therapeutic target. Nevertheless, future research is needed to deeply clarify the role of GPER in PCa and establish its potential as a therapeutic point of intervention.
Overall, we can discuss that the distinct functions of GPER in different tissues, or even within the same tissue, may depend on the specific physiological/environmental conditions in each tissue at a given moment, and/or of the experimental design including the type of ligand and the concentrations tested. The question of concentration would be quite relevant. For example, in the context of testicular apoptosis and male infertility, it was shown that at low concentrations estrogens act as survival factors whereas at high concentrations have the opposite effect inducing cell death [346, 347].
Finally, GPER can be viewed as a “cell guardian”, with their functions modulated by tissue specificity and environmental conditions, i.e., GPER would act protecting cells that need to be protected from harmful stimulus, or destroying those that are “dangerous” for tissue homeostasis.
References
Jensen EV, DeSombre ER. Estrogen-receptor interaction. Science (New York, NY). 1973;182(4108):126–34.
Kuiper GG, Enmark E, Pelto-Huikko M, Nilsson S, Gustafsson JA. Cloning of a novel receptor expressed in rat prostate and ovary. Proc Natl Acad Sci U S A. 1996;93(12):5925–30.
Wang Z, Zhang X, Shen P, Loggie BW, Chang Y, Deuel TF. Identification, cloning, and expression of human estrogen receptor-alpha36, a novel variant of human estrogen receptor-alpha66. Biochem Biophys Res Commun. 2005;336(4):1023–7. https://doi.org/10.1016/j.bbrc.2005.08.226.
Maruyama K, Endoh H, Sasaki-Iwaoka H, Kanou H, Shimaya E, Hashimoto S, Kato S, Kawashima H. A novel isoform of rat estrogen receptor beta with 18 amino acid insertion in the ligand binding domain as a putative dominant negative regular of estrogen action. Biochem Biophys Res Commun. 1998;246(1):142–7.
Mosselman S, Polman J, Dijkema R. ER beta: identification and characterization of a novel human estrogen receptor. FEBS Lett. 1996;392(1):49–53.
Grandien K. Determination of transcription start sites in the human estrogen receptor gene and identification of a novel, tissue-specific, estrogen receptor-mRNA isoform. Mol Cell Endocrinol. 1996;116(2):207–12.
Ye Q, Chung LW, Cinar B, Li S, Zhau HE. Identification and characterization of estrogen receptor variants in prostate cancer cell lines. J Steroid Biochem Mol Biol. 2000;75(1):21–31.
Lewandowski S, Kalita K, Kaczmarek L. Estrogen receptor beta. Potential functional significance of a variety of mRNA isoforms. FEBS Lett. 2002;524(1–3):1–5.
Fujimura T, Takahashi S, Urano T, Ogawa S, Ouchi Y, Kitamura T, Muramatsu M, Inoue S. Differential expression of estrogen receptor beta (ERbeta) and its C-terminal truncated splice variant ERbetacx as prognostic predictors in human prostatic cancer. Biochem Biophys Res Commun. 2001;289(3):692–9. https://doi.org/10.1006/bbrc.2001.6038.
Gibson DA, Saunders PT. Estrogen dependent signaling in reproductive tissues - a role for estrogen receptors and estrogen related receptors. Mol Cell Endocrinol. 2012;348(2):361–72. https://doi.org/10.1016/j.mce.2011.09.026.
Laurentino S, Pinto P, Correia S, Cavaco JE, Canário AVM, Socorro S. Structural variants of sex steroid hormone receptors in the testis: from molecular biology to physiological roles. OA Biotechnol. 2012;1(2):4.
Bjornstrom L, Sjoberg M. Mechanisms of estrogen receptor signaling: convergence of genomic and nongenomic actions on target genes. Mol Endocrinol. 2005;19(4):833–42. https://doi.org/10.1210/me.2004-0486.
Filardo EJ, Quinn JA, Bland KI, Frackelton AR Jr. Estrogen-induced activation of Erk-1 and Erk-2 requires the G protein-coupled receptor homolog, GPR30, and occurs via trans-activation of the epidermal growth factor receptor through release of HB-EGF. Mol Endocrinol. 2000;14(10):1649–60. https://doi.org/10.1210/mend.14.10.0532.
Carmeci C, Thompson DA, Ring HZ, Francke U, Weigel RJ. Identification of a gene (GPR30) with homology to the G-protein-coupled receptor superfamily associated with estrogen receptor expression in breast cancer. Genomics. 1997;45(3):607–17. https://doi.org/10.1006/geno.1997.4972.
Vrtacnik P, Ostanek B, Mencej-Bedrac S, Marc J. The many faces of estrogen signaling. Biochem Med. 2014;24(3):329–42. 10.11613/bm.2014.035.
Chavalmane AK, Comeglio P, Morelli A, Filippi S, Fibbi B, Vignozzi L, Sarchielli E, Marchetta M, Failli P, Sandner P, Saad F, Gacci M, Vannelli GB, Maggi M. Sex steroid receptors in male human bladder: expression and biological function. J Sex Med. 2010;7(8):2698–713. https://doi.org/10.1111/j.1743-6109.2010.01811.x.
Ge C, Yu M, Zhang C. G protein-coupled receptor 30 mediates estrogen-induced proliferation of primordial germ cells via EGFR/Akt/beta-catenin signaling pathway. Endocrinology. 2012;153(7):3504–16. https://doi.org/10.1210/en.2012-1200.
Szwejser E, Maciuszek M, Casanova-Nakayama A, Segner H, Verburg-van Kemenade BM, Chadzinska M. A role for multiple estrogen receptors in immune regulation of common carp. Dev Comp Immunol. 2017;66:61–72. https://doi.org/10.1016/j.dci.2016.04.003.
Maggioli E, McArthur S, Mauro C, Kieswich J, Kusters DH, Reutelingsperger CP, Yaqoob M, Solito E. Estrogen protects the blood-brain barrier from inflammation-induced disruption and increased lymphocyte trafficking. Brain Behav Immun. 2016;51:212–22. https://doi.org/10.1016/j.bbi.2015.08.020.
Cote M, Bourque M, Poirier AA, Aube B, Morissette M, Di Paolo T, Soulet D. GPER1-mediated immunomodulation and neuroprotection in the myenteric plexus of a mouse model of Parkinson’s disease. Neurobiol Dis. 2015;82:99–113. https://doi.org/10.1016/j.nbd.2015.05.017.
Seto K, Hoang M, Santos T, Bandyopadhyay M, Kindy MS, Dasgupta S. Non-genomic oestrogen receptor signal in B lymphocytes: an approach towards therapeutic interventions for infection, autoimmunity and cancer. Int J Biochem Cell Biol. 2016;76:115–8. https://doi.org/10.1016/j.biocel.2016.04.018.
Meyer MR, Fredette NC, Daniel C, Sharma G, Amann K, Arterburn JB, Barton M, Prossnitz ER. Obligatory role for GPER in cardiovascular aging and disease. Sci Signal. 2016;9(452):ra105. https://doi.org/10.1126/scisignal.aag0240.
Zhao TZ, Ding Q, Hu J, He SM, Shi F, Ma LT. GPER expressed on microglia mediates the anti-inflammatory effect of estradiol in ischemic stroke. Brain Behav. 2016;6(4):e00449. https://doi.org/10.1002/brb3.449.
Barton M, Prossnitz ER. Emerging roles of GPER in diabetes and atherosclerosis. Trends Endocrinol Metab. 2015;26(4):185–92. https://doi.org/10.1016/j.tem.2015.02.003.
Bourque M, Morissette M, Cote M, Soulet D, Di Paolo T. Implication of GPER1 in neuroprotection in a mouse model of Parkinson’s disease. Neurobiol Aging. 2013;34(3):887–901. https://doi.org/10.1016/j.neurobiolaging.2012.05.022.
Bourque M, Morissette M, Di Paolo T. Neuroprotection in Parkinsonian-treated mice via estrogen receptor alpha activation requires G protein-coupled estrogen receptor 1. Neuropharmacology. 2015;95:343–52. https://doi.org/10.1016/j.neuropharm.2015.04.006.
Kang WB, Deng YT, Wang DS, Feng D, Liu Q, Wang XS, Ru JY, Cong Y, Zhao JN, Zhao MG, Liu G. Osteoprotective effects of estrogen membrane receptor GPR30 in ovariectomized rats. J Steroid Biochem Mol Biol. 2015;154:237–44. https://doi.org/10.1016/j.jsbmb.2015.07.002.
Broughton BR, Brait VH, Guida E, Lee S, Arumugam TV, Gardiner-Mann CV, Miller AA, Tang SC, Drummond GR, Sobey CG. Stroke increases g protein-coupled estrogen receptor expression in the brain of male but not female mice. Neurosignals. 2013;21(3–4):229–39. https://doi.org/10.1159/000338019.
Broughton BR, Brait VH, Kim HA, Lee S, Chu HX, Gardiner-Mann CV, Guida E, Evans MA, Miller AA, Arumugam TV, Drummond GR, Sobey CG. Sex-dependent effects of G protein-coupled estrogen receptor activity on outcome after ischemic stroke. Stroke. 2014;45(3):835–41. https://doi.org/10.1161/strokeaha.113.001499.
Prabhushankar R, Krueger C, Manrique C. Membrane estrogen receptors: their role in blood pressure regulation and cardiovascular disease. Curr Hypertens Rep. 2014;16(1):408. https://doi.org/10.1007/s11906-013-0408-6.
Boscia F, Passaro C, Gigantino V, Perdona S, Franco R, Portella G, Chieffi S, Chieffi P. High levels of GPR30 protein in human testicular carcinoma in situ and seminomas correlate with low levels of estrogen receptor-beta and indicate a switch in estrogen responsiveness. J Cell Physiol. 2015;230(6):1290–7. https://doi.org/10.1002/jcp.24864.
Han G, White RE. G-protein-coupled estrogen receptor as a new therapeutic target for treating coronary artery disease. World J Cardiol. 2014;6(6):367–75. https://doi.org/10.4330/wjc.v6.i6.367.
Ignatov T, Modl S, Thulig M, Weissenborn C, Treeck O, Ortmann O, Zenclussen A, Costa SD, Kalinski T, Ignatov A. GPER-1 acts as a tumor suppressor in ovarian cancer. J Ovarian Res. 2013;6(1):51. https://doi.org/10.1186/1757-2215-6-51.
Ignatov T, Weissenborn C, Poehlmann A, Lemke A, Semczuk A, Roessner A, Costa SD, Kalinski T, Ignatov A. GPER-1 expression decreases during breast cancer tumorigenesis. Cancer Investig. 2013;31(5):309–15. https://doi.org/10.3109/07357907.2013.789901.
Petrie WK, Dennis MK, Hu C, Dai D, Arterburn JB, Smith HO, Hathaway HJ, Prossnitz ER. G protein-coupled estrogen receptor-selective ligands modulate endometrial tumor growth. Obstet Gynecol Int. 2013;2013:472720. https://doi.org/10.1155/2013/472720.
Jala VR, Radde BN, Haribabu B, Klinge CM. Enhanced expression of G-protein coupled estrogen receptor (GPER/GPR30) in lung cancer. BMC Cancer. 2012;12:624. https://doi.org/10.1186/1471-2407-12-624.
Chevalier N, Vega A, Bouskine A, Siddeek B, Michiels JF, Chevallier D, Fenichel P. GPR30, the non-classical membrane G protein related estrogen receptor, is overexpressed in human seminoma and promotes seminoma cell proliferation. PLoS One. 2012;7(4):e34672. https://doi.org/10.1371/journal.pone.0034672.
Kumar A, Klinge CM, Goldstein RE. Estradiol-induced proliferation of papillary and follicular thyroid cancer cells is mediated by estrogen receptors alpha and beta. Int J Oncol. 2010;36(5):1067–80.
Aiad HA, Wahed MM, Asaad NY, El-Tahmody M, Elhosary E. Immunohistochemical expression of GPR30 in breast carcinoma of Egyptian patients: an association with immunohistochemical subtypes. APMIS. 2014;122(10):976–84. https://doi.org/10.1111/apm.12241.
Fujiwara S, Terai Y, Kawaguchi H, Takai M, Yoo S, Tanaka Y, Tanaka T, Tsunetoh S, Sasaki H, Kanemura M, Tanabe A, Yamashita Y, Ohmichi M. GPR30 regulates the EGFR-Akt cascade and predicts lower survival in patients with ovarian cancer. J Ovarian Res. 2012;5(1):35. https://doi.org/10.1186/1757-2215-5-35.
Lieberherr M, Grosse B, Kachkache M, Balsan S. Cell signaling and estrogens in female rat osteoblasts: a possible involvement of unconventional nonnuclear receptors. J Bone Miner Res. 1993;8(11):1365–76. https://doi.org/10.1002/jbmr.5650081111.
Benten WP, Stephan C, Lieberherr M, Wunderlich F. Estradiol signaling via sequestrable surface receptors. Endocrinology. 2001;142(4):1669–77. https://doi.org/10.1210/endo.142.4.8094.
Evinger AJ III, Levin ER. Requirements for estrogen receptor alpha membrane localization and function. Steroids. 2005;70(5–7):361–3. https://doi.org/10.1016/j.steroids.2005.02.015.
Manavathi B, Kumar R. Steering estrogen signals from the plasma membrane to the nucleus: two sides of the coin. J Cell Physiol. 2006;207(3):594–604. https://doi.org/10.1002/jcp.20551.
Kelly MJ, Lagrange AH, Wagner EJ, Ronnekleiv OK. Rapid effects of estrogen to modulate G protein-coupled receptors via activation of protein kinase A and protein kinase C pathways. Steroids. 1999;64(1–2):64–75.
Prossnitz ER, Arterburn JB, Sklar LA. GPR30: a G protein-coupled receptor for estrogen. Mol Cell Endocrinol. 2007;265–266:138–42. https://doi.org/10.1016/j.mce.2006.12.010.
Owman C, Blay P, Nilsson C, Lolait SJ. Cloning of human cDNA encoding a novel heptahelix receptor expressed in Burkitt’s lymphoma and widely distributed in brain and peripheral tissues. Biochem Biophys Res Commun. 1996;228(2):285–92. https://doi.org/10.1006/bbrc.1996.1654.
Takada Y, Kato C, Kondo S, Korenaga R, Ando J. Cloning of cDNAs encoding G protein-coupled receptor expressed in human endothelial cells exposed to fluid shear stress. Biochem Biophys Res Commun. 1997;240(3):737–41. https://doi.org/10.1006/bbrc.1997.7734.
Kvingedal AM, Smeland EB. A novel putative G-protein-coupled receptor expressed in lung, heart and lymphoid tissue. FEBS Lett. 1997;407(1):59–62.
O’Dowd BF, Nguyen T, Marchese A, Cheng R, Lynch KR, Heng HH, Kolakowski LF Jr, George SR. Discovery of three novel G-protein-coupled receptor genes. Genomics. 1998;47(2):310–3. https://doi.org/10.1006/geno.1998.5095.
Feng Y, Gregor P. Cloning of a novel member of the G protein-coupled receptor family related to peptide receptors. Biochem Biophys Res Commun. 1997;231(3):651–4. https://doi.org/10.1006/bbrc.1997.6161.
Revankar CM, Cimino DF, Sklar LA, Arterburn JB, Prossnitz ER. A transmembrane intracellular estrogen receptor mediates rapid cell signaling. Science (New York, NY). 2005;307(5715):1625–30. https://doi.org/10.1126/science.1106943.
Thomas P, Pang Y, Filardo EJ, Dong J. Identity of an estrogen membrane receptor coupled to a G protein in human breast cancer cells. Endocrinology. 2005;146(2):624–32. https://doi.org/10.1210/en.2004-1064.
Funakoshi T, Yanai A, Shinoda K, Kawano MM, Mizukami Y. G protein-coupled receptor 30 is an estrogen receptor in the plasma membrane. Biochem Biophys Res Commun. 2006;346(3):904–10. https://doi.org/10.1016/j.bbrc.2006.05.191.
Alexander SP, Benson HE, Faccenda E, Pawson AJ, Sharman JL, McGrath JC, Catterall WA, Spedding M, Peters JA, Harmar AJ, Abul-Hasn N, Anderson CM, Anderson CM, Araiksinen MS, Arita M, Arthofer E, Barker EL, Barratt C, Barnes NM, Bathgate R, Beart PM, Belelli D, Bennett AJ, Birdsall NJ, Boison D, Bonner TI, Brailsford L, Broer S, Brown P, Calo G, Carter WG, Catterall WA, Chan SL, Chao MV, Chiang N, Christopoulos A, Chun JJ, Cidlowski J, Clapham DE, Cockcroft S, Connor MA, Cox HM, Cuthbert A, Dautzenberg FM, Davenport AP, Dawson PA, Dent G, Dijksterhuis JP, Dollery CT, Dolphin AC, Donowitz M, Dubocovich ML, Eiden L, Eidne K, Evans BA, Fabbro D, Fahlke C, Farndale R, Fitzgerald GA, Fong TM, Fowler CJ, Fry JR, Funk CD, Futerman AH, Ganapathy V, Gaisnier B, Gershengorn MA, Goldin A, Goldman ID, Gundlach AL, Hagenbuch B, Hales TG, Hammond JR, Hamon M, Hancox JC, Hauger RL, Hay DL, Hobbs AJ, Hollenberg MD, Holliday ND, Hoyer D, Hynes NA, Inui KI, Ishii S, Jacobson KA, Jarvis GE, Jarvis MF, Jensen R, Jones CE, Jones RL, Kaibuchi K, Kanai Y, Kennedy C, Kerr ID, Khan AA, Klienz MJ, Kukkonen JP, Lapoint JY, Leurs R, Lingueglia E, Lippiat J, Lolait SJ, Lummis SC, Lynch JW, MacEwan D, Maguire JJ, Marshall IL, May JM, McArdle CA, McGrath JC, Michel MC, Millar NS, Miller LJ, Mitolo V, Monk PN, Moore PK, Moorhouse AJ, Mouillac B, Murphy PM, Neubig RR, Neumaier J, Niesler B, Obaidat A, Offermanns S, Ohlstein E, Panaro MA, Parsons S, Pwrtwee RG, Petersen J, Pin JP, Poyner DR, Prigent S, Prossnitz ER, Pyne NJ, Pyne S, Quigley JG, Ramachandran R, Richelson EL, Roberts RE, Roskoski R, Ross RA, Roth M, Rudnick G, Ryan RM, Said SI, Schild L, Sanger GJ, Scholich K, Schousboe A, Schulte G, Schulz S, Serhan CN, Sexton PM, Sibley DR, Siegel JM, Singh G, Sitsapesan R, Smart TG, Smith DM, Soga T, Stahl A, Stewart G, Stoddart LA, Summers RJ, Thorens B, Thwaites DT, Toll L, Traynor JR, Usdin TB, Vandenberg RJ, Villalon C, Vore M, Waldman SA, Ward DT, Willars GB, Wonnacott SJ, Wright E, Ye RD, Yonezawa A, Zimmermann M. The concise guide to PHARMACOLOGY 2013/14: overview. Br J Pharmacol. 2013;170(8):1449–58. https://doi.org/10.1111/bph.12444.
Levin ER. G protein-coupled receptor 30: estrogen receptor or collaborator? Endocrinology. 2009;150(4):1563–5. https://doi.org/10.1210/en.2008-1759.
Otto C, Rohde-Schulz B, Schwarz G, Fuchs I, Klewer M, Brittain D, Langer G, Bader B, Prelle K, Nubbemeyer R, Fritzemeier KH. G protein-coupled receptor 30 localizes to the endoplasmic reticulum and is not activated by estradiol. Endocrinology. 2008;149(10):4846–56. https://doi.org/10.1210/en.2008-0269.
Lafferty AR, Torpy DJ, Stowasser M, Taymans SE, Lin JP, Huggard P, Gordon RD, Stratakis CA. A novel genetic locus for low renin hypertension: familial hyperaldosteronism type II maps to chromosome 7 (7p22). J Med Genet. 2000;37(11):831–5.
Gurevich EV, Tesmer JJ, Mushegian A, Gurevich VV. G protein-coupled receptor kinases: more than just kinases and not only for GPCRs. Pharmacol Ther. 2012;133(1):40–69. https://doi.org/10.1016/j.pharmthera.2011.08.001.
Moreira IS. Structural features of the G-protein/GPCR interactions. Biochim Biophys Acta. 2014;1840(1):16–33. https://doi.org/10.1016/j.bbagen.2013.08.027.
Wong SK. G protein selectivity is regulated by multiple intracellular regions of GPCRs. Neurosignals. 2003;12(1):1–12. https://doi.org/10.1159/000068914.
Broselid S, Berg KA, Chavera TA, Kahn R, Clarke WP, Olde B, Leeb-Lundberg LM. G protein-coupled receptor 30 (GPR30) forms a plasma membrane complex with membrane-associated guanylate kinases (MAGUKs) and protein kinase A-anchoring protein 5 (AKAP5) that constitutively inhibits cAMP production. J Biol Chem. 2014;289(32):22117–27. https://doi.org/10.1074/jbc.M114.566893.
Tran QK, Vermeer M. Biosensor-based approach identifies four distinct calmodulin-binding domains in the G protein-coupled estrogen receptor 1. PLoS One. 2014;9(2):e89669. https://doi.org/10.1371/journal.pone.0089669.
Filardo EJ. Epidermal growth factor receptor (EGFR) transactivation by estrogen via the G-protein-coupled receptor, GPR30: a novel signaling pathway with potential significance for breast cancer. J Steroid Biochem Mol Biol. 2002;80(2):231–8.
Filardo E, Quinn J, Pang Y, Graeber C, Shaw S, Dong J, Thomas P. Activation of the novel estrogen receptor G protein-coupled receptor 30 (GPR30) at the plasma membrane. Endocrinology. 2007;148(7):3236–45. https://doi.org/10.1210/en.2006-1605.
Sakamoto H, Matsuda K, Hosokawa K, Nishi M, Morris JF, Prossnitz ER, Kawata M. Expression of G protein-coupled receptor-30, a G protein-coupled membrane estrogen receptor, in oxytocin neurons of the rat paraventricular and supraoptic nuclei. Endocrinology. 2007;148(12):5842–50. https://doi.org/10.1210/en.2007-0436.
Matsuda K, Sakamoto H, Mori H, Hosokawa K, Kawamura A, Itose M, Nishi M, Prossnitz ER, Kawata M. Expression and intracellular distribution of the G protein-coupled receptor 30 in rat hippocampal formation. Neurosci Lett. 2008;441(1):94–9. https://doi.org/10.1016/j.neulet.2008.05.108.
Sanden C, Broselid S, Cornmark L, Andersson K, Daszkiewicz-Nilsson J, Martensson UE, Olde B, Leeb-Lundberg LM. G protein-coupled estrogen receptor 1/G protein-coupled receptor 30 localizes in the plasma membrane and traffics intracellularly on cytokeratin intermediate filaments. Mol Pharmacol. 2011;79(3):400–10. https://doi.org/10.1124/mol.110.069500.
Pupo M, Vivacqua A, Perrotta I, Pisano A, Aquila S, Abonante S, Gasperi-Campani A, Pezzi V, Maggiolini M. The nuclear localization signal is required for nuclear GPER translocation and function in breast Cancer-Associated Fibroblasts (CAFs). Mol Cell Endocrinol. 2013;376(1–2):23–32. https://doi.org/10.1016/j.mce.2013.05.023.
Madeo A, Maggiolini M. Nuclear alternate estrogen receptor GPR30 mediates 17beta-estradiol-induced gene expression and migration in breast cancer-associated fibroblasts. Cancer Res. 2010;70(14):6036–46. https://doi.org/10.1158/0008-5472.can-10-0408.
Tian R, Wang Z, Shi Z, Li D, Wang Y, Zhu Y, Lin W, Gui Y, Zheng XL. Differential expression of G-protein-coupled estrogen receptor-30 in human myometrial and uterine leiomyoma smooth muscle. Fertil Steril. 2013;99(1):256–63. https://doi.org/10.1016/j.fertnstert.2012.09.011.
Cheng SB, Graeber CT, Quinn JA, Filardo EJ. Retrograde transport of the transmembrane estrogen receptor, G-protein-coupled-receptor-30 (GPR30/GPER) from the plasma membrane towards the nucleus. Steroids. 2011;76(9):892–6. https://doi.org/10.1016/j.steroids.2011.02.018.
Gaudet HM, Cheng SB, Christensen EM, Filardo EJ. The G-protein coupled estrogen receptor. GPER. 2015;418(Pt 3):207–19. https://doi.org/10.1016/j.mce.2015.07.016.
Cheng SB, Quinn JA, Graeber CT, Filardo EJ. Down-modulation of the G-protein-coupled estrogen receptor, GPER, from the cell surface occurs via a trans-Golgi-proteasome pathway. J Biol Chem. 2011;286(25):22441–55. https://doi.org/10.1074/jbc.M111.224071.
Meng R, Qin Q, Xiong Y, Wang Y, Zheng J, Zhao Y, Tao T, Wang Q, Liu H, Wang S, Jiang WG, He J. NHERF1, a novel GPER associated protein, increases stability and activation of GPER in ER-positive breast cancer. Oncotarget. 2016;7(34):54983–97. 10.18632/oncotarget.10713.
Ho KJ, Liao JK. Non-nuclear actions of estrogen: new targets for prevention and treatment of cardiovascular disease. Mol Interv. 2002;2(4):219–28. https://doi.org/10.1124/mi.2.4.219.
Hurowitz EH, Melnyk JM, Chen YJ, Kouros-Mehr H, Simon MI, Shizuya H. Genomic characterization of the human heterotrimeric G protein alpha, beta, and gamma subunit genes. DNA Res. 2000;7(2):111–20.
Luttrell LM, van Biesen T, Hawes BE, Koch WJ, Krueger KM, Touhara K, Lefkowitz RJ. G-protein-coupled receptors and their regulation: activation of the MAP kinase signaling pathway by G-protein-coupled receptors. Adv Second Messenger Phosphoprotein Res. 1997;31:263–77.
Filardo EJ, Quinn JA, Frackelton AR Jr, Bland KI. Estrogen action via the G protein-coupled receptor, GPR30: stimulation of adenylyl cyclase and cAMP-mediated attenuation of the epidermal growth factor receptor-to-MAPK signaling axis. Mol Endocrinol. 2002;16(1):70–84. https://doi.org/10.1210/mend.16.1.0758.
Chimento A, Sirianni R, Delalande C, Silandre D, Bois C, Ando S, Maggiolini M, Carreau S, Pezzi V. 17 beta-estradiol activates rapid signaling pathways involved in rat pachytene spermatocytes apoptosis through GPR30 and ER alpha. Mol Cell Endocrinol. 2010;320(1–2):136–44. https://doi.org/10.1016/j.mce.2010.01.035.
Kleuser B, Malek D, Gust R, Pertz HH, Potteck H. 17-Beta-estradiol inhibits transforming growth factor-beta signaling and function in breast cancer cells via activation of extracellular signal-regulated kinase through the G protein-coupled receptor 30. Mol Pharmacol. 2008;74(6):1533–43. https://doi.org/10.1124/mol.108.046854.
Malek D, Gust R, Kleuser B. 17-Beta-estradiol inhibits transforming-growth-factor-beta-induced MCF-7 cell migration by Smad3-repression. Eur J Pharmacol. 2006;534(1–3):39–47. https://doi.org/10.1016/j.ejphar.2006.01.025.
De Francesco EM, Pellegrino M, Santolla MF, Lappano R, Ricchio E, Abonante S, Maggiolini M. GPER mediates activation of HIF1alpha/VEGF signaling by estrogens. Cancer Res. 2014;74(15):4053–64. https://doi.org/10.1158/0008-5472.can-13-3590.
De Francesco EM, Lappano R, Santolla MF, Marsico S, Caruso A, Maggiolini M. HIF-1alpha/GPER signaling mediates the expression of VEGF induced by hypoxia in breast cancer associated fibroblasts (CAFs). Breast Cancer Res. 2013;15(4):R64. https://doi.org/10.1186/bcr3458.
Wei Y, Zhang Z, Liao H, Wu L, Wu X, Zhou D, Xi X, Zhu Y, Feng Y. Nuclear estrogen receptor-mediated Notch signaling and GPR30-mediated PI3K/AKT signaling in the regulation of endometrial cancer cell proliferation. Oncol Rep. 2012;27(2):504–10. https://doi.org/10.3892/or.2011.1536.
Ge X, Guo R, Qiao Y, Zhang Y, Lei J, Wang X, Li L, Hu D. The G protein-coupled receptor GPR30 mediates the nontranscriptional effect of estrogen on the activation of PI3K/Akt pathway in endometrial cancer cells. Int J Gynecol Cancer. 2013;23(1):52–9. https://doi.org/10.1097/IGC.0b013e31827912b8.
Popli P, Sirohi VK, Manohar M, Shukla V, Kaushal JB, Gupta K, Dwivedi A. Regulation of cyclooxygenase-2 expression in rat oviductal epithelial cells: evidence for involvement of GPR30/Src kinase-mediated EGFR signaling. J Steroid Biochem Mol Biol. 2015;154:130–41. https://doi.org/10.1016/j.jsbmb.2015.07.019.
Bartella V, De Francesco EM, Perri MG, Curcio R, Dolce V, Maggiolini M, Vivacqua A. The G protein estrogen receptor (GPER) is regulated by endothelin-1 mediated signaling in cancer cells. Cell Signal. 2016;28(2):61–71. https://doi.org/10.1016/j.cellsig.2015.11.010.
Pupo M, Pisano A, Abonante S, Maggiolini M, Musti AM. GPER activates Notch signaling in breast cancer cells and cancer-associated fibroblasts (CAFs). Int J Biochem Cell Biol. 2014;46:56–67. https://doi.org/10.1016/j.biocel.2013.11.011.
Razandi M, Pedram A, Park ST, Levin ER. Proximal events in signaling by plasma membrane estrogen receptors. J Biol Chem. 2003;278(4):2701–12. https://doi.org/10.1074/jbc.M205692200.
Filardo EJ, Thomas P. GPR30: a seven-transmembrane-spanning estrogen receptor that triggers EGF release. Trends Endocrinol Metab. 2005;16(8):362–7. https://doi.org/10.1016/j.tem.2005.08.005.
Sukocheva O, Wadham C, Holmes A, Albanese N, Verrier E, Feng F, Bernal A, Derian CK, Ullrich A, Vadas MA, Xia P. Estrogen transactivates EGFR via the sphingosine 1-phosphate receptor Edg-3: the role of sphingosine kinase-1. J Cell Biol. 2006;173(2):301–10. https://doi.org/10.1083/jcb.200506033.
Lappano R, De Marco P, De Francesco EM, Chimento A, Pezzi V, Maggiolini M. Cross-talk between GPER and growth factor signaling. J Steroid Biochem Mol Biol. 2013;137:50–6. https://doi.org/10.1016/j.jsbmb.2013.03.005.
De Marco P, Bartella V, Vivacqua A, Lappano R, Santolla MF, Morcavallo A, Pezzi V, Belfiore A, Maggiolini M. Insulin-like growth factor-I regulates GPER expression and function in cancer cells. Oncogene. 2013;32(6):678–88. https://doi.org/10.1038/onc.2012.97.
Maggiolini M, Vivacqua A, Fasanella G, Recchia AG, Sisci D, Pezzi V, Montanaro D, Musti AM, Picard D, Ando S. The G protein-coupled receptor GPR30 mediates c-fos up-regulation by 17beta-estradiol and phytoestrogens in breast cancer cells. J Biol Chem. 2004;279(26):27008–16. https://doi.org/10.1074/jbc.M403588200.
Albanito L, Madeo A, Lappano R, Vivacqua A, Rago V, Carpino A, Oprea TI, Prossnitz ER, Musti AM, Ando S, Maggiolini M. G protein-coupled receptor 30 (GPR30) mediates gene expression changes and growth response to 17beta-estradiol and selective GPR30 ligand G-1 in ovarian cancer cells. Cancer Res. 2007;67(4):1859–66. https://doi.org/10.1158/0008-5472.can-06-2909.
Pandey DP, Lappano R, Albanito L, Madeo A, Maggiolini M, Picard D. Estrogenic GPR30 signalling induces proliferation and migration of breast cancer cells through CTGF. EMBO J. 2009;28(5):523–32. https://doi.org/10.1038/emboj.2008.304.
Vivacqua A, Romeo E, De Marco P, De Francesco EM, Abonante S, Maggiolini M. GPER mediates the Egr-1 expression induced by 17beta-estradiol and 4-hydroxitamoxifen in breast and endometrial cancer cells. Breast Cancer Res Treat. 2012;133(3):1025–35. https://doi.org/10.1007/s10549-011-1901-8.
Kanda N, Watanabe S. 17beta-estradiol inhibits oxidative stress-induced apoptosis in keratinocytes by promoting Bcl-2 expression. J Invest Dermatol. 2003;121(6):1500–9. https://doi.org/10.1111/j.1523-1747.2003.12617.x.
Kanda N, Watanabe S. 17beta-estradiol stimulates the growth of human keratinocytes by inducing cyclin D2 expression. J Invest Dermatol. 2004;123(2):319–28. https://doi.org/10.1111/j.0022-202X.2004.12645.x.
Santolla MF, Avino S, Pellegrino M, De Francesco EM, De Marco P, Lappano R, Vivacqua A, Cirillo F, Rigiracciolo DC, Scarpelli A, Abonante S, Maggiolini M. SIRT1 is involved in oncogenic signaling mediated by GPER in breast cancer. Cell Death Dis. 2015;6:e1834. https://doi.org/10.1038/cddis.2015.201.
Prossnitz ER, Barton M. Estrogen biology: new insights into GPER function and clinical opportunities. Mol Cell Endocrinol. 2014;389(1–2):71–83. https://doi.org/10.1016/j.mce.2014.02.002.
Hay DL, Pioszak AA. Receptor activity-modifying proteins (RAMPs): new insights and roles. Annu Rev Pharmacol Toxicol. 2016;56:469–87. https://doi.org/10.1146/annurev-pharmtox-010715-103120.
Lenhart PM, Broselid S, Barrick CJ, Leeb-Lundberg LM, Caron KM. G-protein-coupled receptor 30 interacts with receptor activity-modifying protein 3 and confers sex-dependent cardioprotection. J Mol Endocrinol. 2013;51(1):191–202. https://doi.org/10.1530/jme-13-0021.
Mendez-Luna D, Martinez-Archundia M, Maroun RC, Ceballos-Reyes G, Fragoso-Vazquez MJ, Gonzalez-Juarez DE, Correa-Basurto J. Deciphering the GPER/GPR30-agonist and antagonists interactions using molecular modeling studies, molecular dynamics, and docking simulations. J Biomol Struct Dyn. 2015;33(10):2161–72. https://doi.org/10.1080/07391102.2014.994102.
Koganti S, Snyder R, Gumaste U, Karamyan VT, Thekkumkara T. 2-methoxyestradiol binding of GPR30 down-regulates angiotensin AT(1) receptor. Eur J Pharmacol. 2014;723:131–40. https://doi.org/10.1016/j.ejphar.2013.10.064.
Chourasia TK, Pang Y, Thomas P. The catecholestrogen, 2-hydroxyestradiol-17beta, acts as a G protein-coupled estrogen receptor 1 (GPER/GPR30) antagonist to promote the resumption of meiosis in zebrafish oocytes. Biol Reprod. 2015;92(3):69. https://doi.org/10.1095/biolreprod.114.125674.
Zucchetti AE, Barosso IR, Boaglio AC, Basiglio CL, Miszczuk G, Larocca MC, Ruiz ML, Davio CA, Roma MG, Crocenzi FA, Pozzi EJ. G-protein-coupled receptor 30/adenylyl cyclase/protein kinase A pathway is involved in estradiol 17ss-D-glucuronide-induced cholestasis. Hepatology (Baltimore, MD). 2014;59(3):1016–29. https://doi.org/10.1002/hep.26752.
Lappano R, Rosano C, De Marco P, De Francesco EM, Pezzi V, Maggiolini M. Estriol acts as a GPR30 antagonist in estrogen receptor-negative breast cancer cells. Mol Cell Endocrinol. 2010;320(1–2):162–70. https://doi.org/10.1016/j.mce.2010.02.006.
Girgert R, Emons G, Grundker C. Inhibition of GPR30 by estriol prevents growth stimulation of triple-negative breast cancer cells by 17beta-estradiol. BMC Cancer. 2014;14:935. https://doi.org/10.1186/1471-2407-14-935.
Sandra N, Ester P, Marie-Agnes P, Robert M, Olivier H. The DHEA metabolite 7beta-hydroxy-epiandrosterone exerts anti-estrogenic effects on breast cancer cell lines. Steroids. 2012;77(5):542–51. https://doi.org/10.1016/j.steroids.2012.01.019.
Gros R, Ding Q, Liu B, Chorazyczewski J, Feldman RD. Aldosterone mediates its rapid effects in vascular endothelial cells through GPER activation. Am J Physiol Cell Physiol. 2013;304(6):C532–40. https://doi.org/10.1152/ajpcell.00203.2012.
Feldman RD, Ding Q, Hussain Y, Limbird LE, Pickering JG, Gros R. Aldosterone mediates metastatic spread of renal cancer via the G protein-coupled estrogen receptor (GPER). FASEB J. 2016. https://doi.org/10.1096/fj.15-275552.
Hermidorff MM, de Assis LV, Isoldi MC. Genomic and rapid effects of aldosterone: what we know and do not know thus far. Heart Fail Rev. 2017;22(1):65–89. https://doi.org/10.1007/s10741-016-9591-2.
Qiao H, Hu B, Zhou H, Yan J, Jia R, Lu B, Sun B, Luo X, Fan Y, Wang N. Aldosterone induces rapid sodium intake by a nongenomic mechanism in the nucleus tractus solitarius. Sci Rep. 2016;6:38631. https://doi.org/10.1038/srep38631.
Cheng SB, Dong J, Pang Y, LaRocca J, Hixon M, Thomas P, Filardo EJ. Anatomical location and redistribution of G protein-coupled estrogen receptor-1 during the estrus cycle in mouse kidney and specific binding to estrogens but not aldosterone. Mol Cell Endocrinol. 2014;382(2):950–9. https://doi.org/10.1016/j.mce.2013.11.005.
Gros R, Ding Q, Sklar LA, Prossnitz EE, Arterburn JB, Chorazyczewski J, Feldman RD. GPR30 expression is required for the mineralocorticoid receptor-independent rapid vascular effects of aldosterone. Hypertension. 2011;57(3):442–51. https://doi.org/10.1161/hypertensionaha.110.161653.
Heublein S, Vrekoussis T, Kuhn C, Friese K, Makrigiannakis A, Mayr D, Lenhard M, Jeschke U. Inducers of G-protein coupled estrogen receptor (GPER) in endometriosis: potential implications for macrophages and follicle maturation. J Reprod Immunol. 2013;97(1):95–103. https://doi.org/10.1016/j.jri.2012.10.013.
Cameron DA, Keen JC, Dixon JM, Bellamy C, Hanby A, Anderson TJ, Miller WR. Effective tamoxifen therapy of breast cancer involves both antiproliferative and pro-apoptotic changes. Eur J Cancer. 2000;36(7):845–51.
Ariazi EA, Ariazi JL, Cordera F, Jordan VC. Estrogen receptors as therapeutic targets in breast cancer. Curr Top Med Chem. 2006;6(3):181–202.
Jordan VC. SERMs: meeting the promise of multifunctional medicines. J Natl Cancer Inst. 2007;99(5):350–6. https://doi.org/10.1093/jnci/djk062.
Long N, Long B, Mana A, Le D, Nguyen L, Chokr S, Sinchak K. Tamoxifen and ICI 182,780 activate hypothalamic G protein-coupled estrogen receptor 1 to rapidly facilitate lordosis in female rats. Horm Behav. 2017;89:98–103. https://doi.org/10.1016/j.yhbeh.2016.12.013.
Zhang L, Li Y, Lan L, Liu R, Wu Y, Qu Q, Wen K. Tamoxifen has a proliferative effect in endometrial carcinoma mediated via the GPER/EGFR/ERK/cyclin D1 pathway: a retrospective study and an in vitro study. Mol Cell Endocrinol. 2016;437:51–61. https://doi.org/10.1016/j.mce.2016.08.011.
Qiu J, Bosch MA, Tobias SC, Grandy DK, Scanlan TS, Ronnekleiv OK, Kelly MJ. Rapid signaling of estrogen in hypothalamic neurons involves a novel G-protein-coupled estrogen receptor that activates protein kinase C. J Neurosci. 2003;23(29):9529–40.
Bourque M, Morissette M, Di Paolo T. Raloxifene activates G protein-coupled estrogen receptor 1/Akt signaling to protect dopamine neurons in 1-methyl-4-phenyl-1,2,3,6-tetrahydropyridine mice. Neurobiol Aging. 2014;35(10):2347–56. https://doi.org/10.1016/j.neurobiolaging.2014.03.017.
Vivacqua A, Bonofiglio D, Recchia AG, Musti AM, Picard D, Ando S, Maggiolini M. The G protein-coupled receptor GPR30 mediates the proliferative effects induced by 17beta-estradiol and hydroxytamoxifen in endometrial cancer cells. Mol Endocrinol. 2006;20(3):631–46. https://doi.org/10.1210/me.2005-0280.
Zhang X, Li JH, Duan SX, Lin QJ, Ke S, Ma L, Huang TH, Jiang XW. G protein-coupled estrogen receptor-protein kinase A-ERK-CREB signaling pathway is involved in the regulation of mouse gubernaculum testis cells by diethylstilbestrol. Arch Environ Contam Toxicol. 2014;67(1):97–103. https://doi.org/10.1007/s00244-013-9976-3.
Zhang X, Ke S, Chen KH, Li JH, Ma L, Jiang XW. Diethylstilbestrol affects the expression of GPER in the gubernaculum testis. Int J Clin Exp Pathol. 2015;8(6):7217–22.
Chandra V, Fatima I, Saxena R, Hussain MK, Hajela K, Sankhwar P, Roy BG, Chandna S, Dwivedi A. Anti-tumorigenic action of 2-[piperidinoethoxyphenyl]-3-[4-hydroxyphenyl]-2H-benzo(b)pyran: evidence for involvement of GPR30/EGFR signaling pathway. Gynecol Oncol. 2013;129(2):433–42. https://doi.org/10.1016/j.ygyno.2013.02.005.
Lappano R, Santolla MF, Pupo M, Sinicropi MS, Caruso A, Rosano C, Maggiolini M. MIBE acts as antagonist ligand of both estrogen receptor alpha and GPER in breast cancer cells. Breast Cancer Res. 2012;14(1):R12. https://doi.org/10.1186/bcr3096.
Shaul PW. Regulation of endothelial nitric oxide synthase: location, location, location. Annu Rev Physiol. 2002;64:749–74. https://doi.org/10.1146/annurev.physiol.64.081501.155952.
Harrington WR, Kim SH, Funk CC, Madak-Erdogan Z, Schiff R, Katzenellenbogen JA, Katzenellenbogen BS. Estrogen dendrimer conjugates that preferentially activate extranuclear, nongenomic versus genomic pathways of estrogen action. Mol Endocrinol. 2006;20(3):491–502. https://doi.org/10.1210/me.2005-0186.
Revankar CM, Mitchell HD, Field AS, Burai R, Corona C, Ramesh C, Sklar LA, Arterburn JB, Prossnitz ER. Synthetic estrogen derivatives demonstrate the functionality of intracellular GPR30. ACS Chem Biol. 2007;2(8):536–44. https://doi.org/10.1021/cb700072n.
Sirotkin AV, Harrath AH. Phytoestrogens and their effects. Eur J Pharmacol. 2014;741:230–6. https://doi.org/10.1016/j.ejphar.2014.07.057.
Moreno-Ulloa A, Mendez-Luna D, Beltran-Partida E, Castillo C, Guevara G, Ramirez-Sanchez I, Correa-Basurto J, Ceballos G, Villarreal F. The effects of (−)-epicatechin on endothelial cells involve the G protein-coupled estrogen receptor (GPER). Pharmacol Res. 2015;100:309–20. https://doi.org/10.1016/j.phrs.2015.08.014.
Ma HR, Wang J, Chen YF, Chen H, Wang WS, Aisa HA. Icariin and icaritin stimulate the proliferation of SKBr3 cells through the GPER1-mediated modulation of the EGFR-MAPK signaling pathway. Int J Mol Med. 2014;33(6):1627–34. https://doi.org/10.3892/ijmm.2014.1722.
Li YC, Ding XS, Li HM, Zhang C. Icariin attenuates high glucose-induced type IV collagen and fibronectin accumulation in glomerular mesangial cells by inhibiting transforming growth factor-beta production and signalling through G protein-coupled oestrogen receptor 1. Clin Exp Pharmacol Physiol. 2013;40(9):635–43. https://doi.org/10.1111/1440-1681.12143.
Shang D, Li Z, Zhu Z, Chen H, Zhao L, Wang X, Chen Y. Baicalein suppresses 17-beta-estradiol-induced migration, adhesion and invasion of breast cancer cells via the G protein-coupled receptor 30 signaling pathway. Oncol Rep. 2015;33(4):2077–85. https://doi.org/10.3892/or.2015.3786.
Chen Y, Wang J, Hong DY, Chen L, Zhang YY, Xu YN, Pan D, Fu LY, Tao L, Luo H, Shen XC. Baicalein has protective effects on the 17beta-estradiol-induced transformation of breast epithelial cells. Oncotarget. 2017;8(6):10470–84. 10.18632/oncotarget.14433.
Thomas P, Dong J. Binding and activation of the seven-transmembrane estrogen receptor GPR30 by environmental estrogens: a potential novel mechanism of endocrine disruption. J Steroid Biochem Mol Biol. 2006;102(1–5):175–9. https://doi.org/10.1016/j.jsbmb.2006.09.017.
Pisani SL, Neese SL, Doerge DR, Helferich WG, Schantz SL, Korol DL. Acute genistein treatment mimics the effects of estradiol by enhancing place learning and impairing response learning in young adult female rats. Horm Behav. 2012;62(4):491–9. https://doi.org/10.1016/j.yhbeh.2012.08.006.
Lucki NC, Sewer MB. Genistein stimulates MCF-7 breast cancer cell growth by inducing acid ceramidase (ASAH1) gene expression. J Biol Chem. 2011;286(22):19399–409. https://doi.org/10.1074/jbc.M110.195826.
Kajta M, Rzemieniec J, Litwa E, Lason W, Lenartowicz M, Krzeptowski W, Wojtowicz AK. The key involvement of estrogen receptor beta and G-protein-coupled receptor 30 in the neuroprotective action of daidzein. Neuroscience. 2013;238:345–60. https://doi.org/10.1016/j.neuroscience.2013.02.005.
Rowlands DJ, Chapple S, Siow RC, Mann GE. Equol-stimulated mitochondrial reactive oxygen species activate endothelial nitric oxide synthase and redox signaling in endothelial cells: roles for F-actin and GPR30. Hypertension. 2011;57(4):833–40. https://doi.org/10.1161/hypertensionaha.110.162198.
Cheng YF, Zhu G, Wu QW, Xie YS, Jiang Y, Guo L, Guan YL, Liu YS, Zhang J. GPR30 activation contributes to the Puerarin-mediated neuroprotection in MPP+-induced SH-SY5Y cell death. J Mol Neurosci. 2017;61(2):227–34. https://doi.org/10.1007/s12031-016-0856-y.
Khan K, Pal S, Yadav M, Maurya R, Trivedi AK, Sanyal S, Chattopadhyay N. Prunetin signals via G-protein-coupled receptor, GPR30(GPER1): stimulation of adenylyl cyclase and cAMP-mediated activation of MAPK signaling induces Runx2 expression in osteoblasts to promote bone regeneration. J Nutr Biochem. 2015;26(12):1491–501. https://doi.org/10.1016/j.jnutbio.2015.07.021.
Kang K, Lee SB, Jung SH, Cha KH, Park WD, Sohn YC, Nho CW. Tectoridin, a poor ligand of estrogen receptor alpha, exerts its estrogenic effects via an ERK-dependent pathway. Mol Cells. 2009;27(3):351–7. https://doi.org/10.1007/s10059-009-0045-8.
Varoni EM, Lo Faro AF, Sharifi-Rad J, Iriti M. Anticancer molecular mechanisms of resveratrol. Front Nutr. 2016;3:8. https://doi.org/10.3389/fnut.2016.00008.
Dong WH, Chen JC, He YL, Xu JJ, Mei YA. Resveratrol inhibits K(v)2.2 currents through the estrogen receptor GPR30-mediated PKC pathway. Am J Physiol Cell Physiol. 2013;305(5):C547–57. https://doi.org/10.1152/ajpcell.00146.2013.
Chimento A, Casaburi I, Rosano C, Avena P, De Luca A, Campana C, Martire E, Santolla MF, Maggiolini M, Pezzi V, Sirianni R. Oleuropein and hydroxytyrosol activate GPER/GPR30-dependent pathways leading to apoptosis of ER-negative SKBR3 breast cancer cells. Mol Nutr Food Res. 2014;58(3):478–89. https://doi.org/10.1002/mnfr.201300323.
Ren GY, Chen CY, Chen WG, Huang Y, Qin LQ, Chen LH. The treatment effects of flaxseed-derived secoisolariciresinol diglycoside and its metabolite enterolactone on benign prostatic hyperplasia involve the G protein-coupled estrogen receptor 1. Appl Physiol Nutr Metab. 2016;41(12):1303–10. https://doi.org/10.1139/apnm-2016-0332.
Shanle EK, Xu W. Endocrine disrupting chemicals targeting estrogen receptor signaling: identification and mechanisms of action. Chem Res Toxicol. 2011;24(1):6–19. https://doi.org/10.1021/tx100231n.
Dong S, Terasaka S, Kiyama R. Bisphenol A induces a rapid activation of Erk1/2 through GPR30 in human breast cancer cells. Environ Pollut. 2011;159(1):212–8. https://doi.org/10.1016/j.envpol.2010.09.004.
Li M, Guo J, Gao W, Yu J, Han X, Zhang J, Shao B. Bisphenol AF-induced endogenous transcription is mediated by ERalpha and ERK1/2 activation in human breast cancer cells. PLoS One. 2014;9(4):e94725. https://doi.org/10.1371/journal.pone.0094725.
Sheng ZG, Huang W, Liu YX, Zhu BZ. Bisphenol A at a low concentration boosts mouse spermatogonial cell proliferation by inducing the G protein-coupled receptor 30 expression. Toxicol Appl Pharmacol. 2013;267(1):88–94. https://doi.org/10.1016/j.taap.2012.12.014.
Sheng ZG, Zhu BZ. Low concentrations of bisphenol A induce mouse spermatogonial cell proliferation by G protein-coupled receptor 30 and estrogen receptor-alpha. Environ Health Perspect. 2011;119(12):1775–80. https://doi.org/10.1289/ehp.1103781.
Ge LC, Chen ZJ, Liu HY, Zhang KS, Liu H, Huang HB, Zhang G, Wong CK, Giesy JP, Du J, Wang HS. Involvement of activating ERK1/2 through G protein coupled receptor 30 and estrogen receptor alpha/beta in low doses of bisphenol A promoting growth of Sertoli TM4 cells. Toxicol Lett. 2014;226(1):81–9. https://doi.org/10.1016/j.toxlet.2014.01.035.
Zhang KS, Chen HQ, Chen YS, Qiu KF, Zheng XB, Li GC, Yang HD, Wen CJ. Bisphenol A stimulates human lung cancer cell migration via upregulation of matrix metalloproteinases by GPER/EGFR/ERK1/2 signal pathway. Biomed Pharmacother. 2014;68(8):1037–43. https://doi.org/10.1016/j.biopha.2014.09.003.
Liu J, Jin X, Zhao N, Ye X, Ying C. Bisphenol A promotes X-linked inhibitor of apoptosis protein-dependent angiogenesis via G protein-coupled estrogen receptor pathway. J Appl Toxicol. 2015;35(11):1309–17. https://doi.org/10.1002/jat.3112.
Ge LC, Wang HS. A commentary on “Involvement of activating ERK1/2 trough G protein coupled receptor 30 and estrogen receptor alpha/beta in low doses of bisphenol A promoting growth of Sertoli TM4 cells”. Toxicol Lett. 2016;240(1):236–7. https://doi.org/10.1016/j.toxlet.2015.09.021.
Mahemuti L, Chen Q, Coughlan MC, Zhang M, Florian M, Mailloux RJ, Cao XL, Scoggan KA, Willmore WG, Jin X. Bisphenol A exposure alters release of immune and developmental modulators and expression of estrogen receptors in human fetal lung fibroblasts. J Environ Sci (China). 2016;48:11–23. https://doi.org/10.1016/j.jes.2016.02.013.
Song H, Zhang T, Yang P, Li M, Yang Y, Wang Y, Du J, Pan K, Zhang K. Low doses of bisphenol A stimulate the proliferation of breast cancer cells via ERK1/2/ERRgamma signals. Toxicol In Vitro. 2015;30(1 Pt B):521–8. https://doi.org/10.1016/j.tiv.2015.09.009.
Lei B, Peng W, Xu G, Wu M, Wen Y, Xu J, Yu Z, Wang Y. Activation of G protein-coupled receptor 30 by thiodiphenol promotes proliferation of estrogen receptor alpha-positive breast cancer cells. Chemosphere. 2017;169:204–11. https://doi.org/10.1016/j.chemosphere.2016.11.066.
Bindal RD, Carlson KE, Katzenellenbogen BS, Katzenellenbogen JA. Lipophilic impurities, not phenolsulfonphthalein, account for the estrogenic activity in commercial preparations of phenol red. J Steroid Biochem. 1988;31(3):287–93.
Kajta M, Litwa E, Rzemieniec J, Wnuk A, Lason W, Zelek-Molik A, Nalepa I, Grzegorzewska-Hiczwa M, Tokarski K, Golas A, Guzik E, Grochowalski A, Szychowski KA, Wojtowicz AK. Isomer-nonspecific action of dichlorodiphenyltrichloroethane on aryl hydrocarbon receptor and G-protein-coupled receptor 30 intracellular signaling in apoptotic neuronal cells. Mol Cell Endocrinol. 2014;392(1–2):90–105. https://doi.org/10.1016/j.mce.2014.05.008.
Tian PC, Wang HL, Chen GH, Luo Q, Chen Z, Wang Y, Liu YF. 2,2′,4,4′-Tetrabromodiphenyl ether promotes human neuroblastoma SH-SY5Y cells migration via the GPER/PI3K/Akt signal pathway. Hum Exp Toxicol. 2016;35(2):124–34. https://doi.org/10.1177/0960327115578974.
Florian CP, Mansfield SR, Schroeder JR. Differences in GPR30 regulation by chlorotriazine herbicides in human breast cells. Biochem Res Int. 2016;2016:2984081. https://doi.org/10.1155/2016/2984081.
Leblanc K, Sexton E, Parent S, Belanger G, Dery MC, Boucher V, Asselin E. Effects of 4-hydroxytamoxifen, raloxifene and ICI 182 780 on survival of uterine cancer cell lines in the presence and absence of exogenous estrogens. Int J Oncol. 2007;30(2):477–87.
PA. Gale, JL Sessler, Kral V (1998) Calixpyrroles. Chem Commun (1):1–8. doi:https://doi.org/10.1039/A706280J.
Gale PA, Anzenbacher P Jr, Sessler JL. Calixpyrroles II. Coord Chem Rev. 2001;222(1):57–102. https://doi.org/10.1016/S0010-8545(01)00346-0
Lappano R, Rosano C, Pisano A, Santolla MF, De Francesco EM, De Marco P, Dolce V, Ponassi M, Felli L, Cafeo G, Kohnke FH, Abonante S, Maggiolini M. A calixpyrrole derivative acts as an antagonist to GPER, a G-protein coupled receptor: mechanisms and models. Dis Model Mech. 2015;8(10):1237–46. https://doi.org/10.1242/dmm.021071.
Wrobel AM, Gregoraszczuk EL. Action of methyl-, propyl- and butylparaben on GPR30 gene and protein expression, cAMP levels and activation of ERK1/2 and PI3K/Akt signaling pathways in MCF-7 breast cancer cells and MCF-10A non-transformed breast epithelial cells. Toxicol Lett. 2015;238(2):110–6. https://doi.org/10.1016/j.toxlet.2015.08.001.
Gupte A, Mumper RJ. Elevated copper and oxidative stress in cancer cells as a target for cancer treatment. Cancer Treat Rev. 2009;35(1):32–46. https://doi.org/10.1016/j.ctrv.2008.07.004.
Rigiracciolo DC, Scarpelli A, Lappano R, Pisano A, Santolla MF, De Marco P, Cirillo F, Cappello AR, Dolce V, Belfiore A, Maggiolini M, De Francesco EM. Copper activates HIF-1alpha/GPER/VEGF signalling in cancer cells. Oncotarget. 2015;6(33):34158–77. 10.18632/oncotarget.5779.
Huff MO, Todd SL, Smith AL, Elpers JT, Smith AP, Murphy RD, Bleser-Shartzer AS, Hoerter JE, Radde BN, Klinge CM. Arsenite and cadmium activate MAPK/ERK via membrane estrogen receptors and G-protein coupled estrogen receptor signaling in human lung adenocarcinoma cells. Toxicol Sci. 2016;152(1):62–71. https://doi.org/10.1093/toxsci/kfw064.
Yu X, Filardo EJ, Shaikh ZA. The membrane estrogen receptor GPR30 mediates cadmium-induced proliferation of breast cancer cells. Toxicol Appl Pharmacol. 2010;245(1):83–90. https://doi.org/10.1016/j.taap.2010.02.005.
Liu Z, Yu X, Shaikh ZA. Rapid activation of ERK1/2 and AKT in human breast cancer cells by cadmium. Toxicol Appl Pharmacol. 2008;228(3):286–94. https://doi.org/10.1016/j.taap.2007.12.017.
Ariazi EA, Brailoiu E, Yerrum S, Shupp HA, Slifker MJ, Cunliffe HE, Black MA, Donato AL, Arterburn JB, Oprea TI, Prossnitz ER, Dun NJ, Jordan VC. The G protein-coupled receptor GPR30 inhibits proliferation of estrogen receptor-positive breast cancer cells. Cancer Res. 2010;70(3):1184–94. https://doi.org/10.1158/0008-5472.can-09-3068.
Zhu P, Liao LY, Zhao TT, Mo XM, Chen GG, Liu ZM. GPER/ERK&AKT/NF-kappaB pathway is involved in cadmium-induced proliferation, invasion and migration of GPER-positive thyroid cancer cells. Mol Cell Endocrinol. 2017;442:68–80. https://doi.org/10.1016/j.mce.2016.12.007.
Pisano A, Santolla MF, De Francesco EM, De Marco P, Rigiracciolo DC, Perri MG, Vivacqua A, Abonante S, Cappello AR, Dolce V, Belfiore A, Maggiolini M, Lappano R. GPER, IGF-IR, and EGFR transduction signaling are involved in stimulatory effects of zinc in breast cancer cells and cancer-associated fibroblasts. Mol Carcinog. 2017;56(2):580–93. https://doi.org/10.1002/mc.22518.
Santolla MF, De Francesco EM, Lappano R, Rosano C, Abonante S, Maggiolini M. Niacin activates the G protein estrogen receptor (GPER)-mediated signalling. Cell Signal. 2014;26(7):1466–75. https://doi.org/10.1016/j.cellsig.2014.03.011.
Bologa CG, Revankar CM, Young SM, Edwards BS, Arterburn JB, Kiselyov AS, Parker MA, Tkachenko SE, Savchuck NP, Sklar LA, Oprea TI, Prossnitz ER. Virtual and biomolecular screening converge on a selective agonist for GPR30. Nat Chem Biol. 2006;2(4):207–12. https://doi.org/10.1038/nchembio775.
Dennis MK, Burai R, Ramesh C, Petrie WK, Alcon SN, Nayak TK, Bologa CG, Leitao A, Brailoiu E, Deliu E, Dun NJ, Sklar LA, Hathaway HJ, Arterburn JB, Oprea TI, Prossnitz ER. In vivo effects of a GPR30 antagonist. Nat Chem Biol. 2009;5(6):421–7. https://doi.org/10.1038/nchembio.168.
Bai LY, Weng JR, Hu JL, Wang D, Sargeant AM, Chiu CF. G15, a GPR30 antagonist, induces apoptosis and autophagy in human oral squamous carcinoma cells. Chem Biol Interact. 2013;206(2):375–84. https://doi.org/10.1016/j.cbi.2013.10.014.
Dennis MK, Field AS, Burai R, Ramesh C, Petrie WK, Bologa CG, Oprea TI, Yamaguchi Y, Hayashi S, Sklar LA, Hathaway HJ, Arterburn JB, Prossnitz ER. Identification of a GPER/GPR30 antagonist with improved estrogen receptor counterselectivity. J Steroid Biochem Mol Biol. 2011;127(3–5):358–66. https://doi.org/10.1016/j.jsbmb.2011.07.002.
Chimento A, Sirianni R, Casaburi I, Zolea F, Rizza P, Avena P, Malivindi R, De Luca A, Campana C, Martire E, Domanico F, Fallo F, Carpinelli G, Cerquetti L, Amendola D, Stigliano A, Pezzi V. GPER agonist G-1 decreases adrenocortical carcinoma (ACC) cell growth in vitro and in vivo. Oncotarget. 2015;6(22):19190–203. 10.18632/oncotarget.4241.
Alencar AK, Montes GC, Montagnoli T, Silva AM, Martinez ST, Fraga AG, Wang H, Groban L, Sudo RT, Zapata-Sudo G. Activation of GPER ameliorates experimental pulmonary hypertension in male rats. Eur J Pharm Sci. 2017;97:208–17. https://doi.org/10.1016/j.ejps.2016.11.009.
Mendes-Oliveira J, Lopes Campos F, Videira RA, Baltazar G. GPER activation is effective in protecting against inflammation-induced nigral dopaminergic loss and motor function impairment. Brain Behav Immun. 2017;64:296–307. https://doi.org/10.1016/j.bbi.2017.04.016.
Lappano R, Rosano C, Santolla MF, Pupo M, De Francesco EM, De Marco P, Ponassi M, Spallarossa A, Ranise A, Maggiolini M. Two novel GPER agonists induce gene expression changes and growth effects in cancer cells. Curr Cancer Drug Targets. 2012;12(5):531–42.
Maggiolini M, Santolla MF, Avino S, Aiello F, Rosano C, Garofalo A, Grande F. Identification of two benzopyrroloxazines acting as selective GPER antagonists in breast cancer cells and cancer-associated fibroblasts. Future Med Chem. 2015;7(4):437–48. https://doi.org/10.4155/fmc.15.3.
Arias-Pulido H, Royce M, Gong Y, Joste N, Lomo L, Lee SJ, Chaher N, Verschraegen C, Lara J, Prossnitz ER, Cristofanilli M. GPR30 and estrogen receptor expression: new insights into hormone dependence of inflammatory breast cancer. Breast Cancer Res Treat. 2010;123(1):51–8. https://doi.org/10.1007/s10549-009-0631-7.
Filardo EJ, Graeber CT, Quinn JA, Resnick MB, Giri D, DeLellis RA, Steinhoff MM, Sabo E. Distribution of GPR30, a seven membrane-spanning estrogen receptor, in primary breast cancer and its association with clinicopathologic determinants of tumor progression. Clin Cancer Res. 2006;12(21):6359–66. https://doi.org/10.1158/1078-0432.ccr-06-0860.
Luo HJ, Luo P, Yang GL, Peng QL, Liu MR, Tu G. G-protein coupled estrogen receptor 1 expression in primary breast cancers and its correlation with clinicopathological variables. J Breast Cancer. 2011;14(3):185–90. https://doi.org/10.4048/jbc.2011.14.3.185.
Sjostrom M, Hartman L, Grabau D, Fornander T, Malmstrom P, Nordenskjold B, Sgroi DC, Skoog L, Stal O, Leeb-Lundberg LM, Ferno M. Lack of G protein-coupled estrogen receptor (GPER) in the plasma membrane is associated with excellent long-term prognosis in breast cancer. Breast Cancer Res Treat. 2014;145(1):61–71. https://doi.org/10.1007/s10549-014-2936-4.
Samartzis EP, Noske A, Meisel A, Varga Z, Fink D, Imesch P. The G protein-coupled estrogen receptor (GPER) is expressed in two different subcellular localizations reflecting distinct tumor properties in breast cancer. PLoS One. 2014;9(1):e83296. https://doi.org/10.1371/journal.pone.0083296.
Ignatov A, Ignatov T, Weissenborn C, Eggemann H, Bischoff J, Semczuk A, Roessner A, Costa SD, Kalinski T. G-protein-coupled estrogen receptor GPR30 and tamoxifen resistance in breast cancer. Breast Cancer Res Treat. 2011;128(2):457–66. https://doi.org/10.1007/s10549-011-1584-1.
Marjon NA, Hu C, Hathaway HJ, Prossnitz ER. G protein-coupled estrogen receptor regulates mammary tumorigenesis and metastasis. Mol Cancer Res. 2014;12(11):1644–54. https://doi.org/10.1158/1541-7786.mcr-14-0128-t.
Liu Q, Li JG, Zheng XY, Jin F, Dong HT. Expression of CD133, PAX2, ESA, and GPR30 in invasive ductal breast carcinomas. Chin Med J. 2009;122(22):2763–9.
Steiman J, Peralta EA, Louis S, Kamel O. Biology of the estrogen receptor, GPR30, in triple negative breast cancer. Am J Surg. 2013;206(5):698–703. https://doi.org/10.1016/j.amjsurg.2013.07.014.
Konecny G, Pauletti G, Pegram M, Untch M, Dandekar S, Aguilar Z, Wilson C, Rong HM, Bauerfeind I, Felber M, Wang HJ, Beryt M, Seshadri R, Hepp H, Slamon DJ. Quantitative association between HER-2/neu and steroid hormone receptors in hormone receptor-positive primary breast cancer. J Natl Cancer Inst. 2003;95(2):142–53.
Rakha EA, El-Sayed ME, Green AR, Lee AH, Robertson JF, Ellis IO. Prognostic markers in triple-negative breast cancer. Cancer. 2007;109(1):25–32. https://doi.org/10.1002/cncr.22381.
Girgert R, Emons G, Grundker C. Inactivation of GPR30 reduces growth of triple-negative breast cancer cells: possible application in targeted therapy. Breast Cancer Res Treat. 2012;134(1):199–205. https://doi.org/10.1007/s10549-012-1968-x.
Mo Z, Liu M, Yang F, Luo H, Li Z, Tu G, Yang G. GPR30 as an initiator of tamoxifen resistance in hormone-dependent breast cancer. Breast Cancer Res. 2013;15(6):R114. https://doi.org/10.1186/bcr3581.
Yuan J, Liu M, Yang L, Tu G, Zhu Q, Chen M, Cheng H, Luo H, Fu W, Li Z, Yang G. Acquisition of epithelial-mesenchymal transition phenotype in the tamoxifen-resistant breast cancer cell: a new role for G protein-coupled estrogen receptor in mediating tamoxifen resistance through cancer-associated fibroblast-derived fibronectin and beta1-integrin signaling pathway in tumor cells. Breast Cancer Res. 2015;17:69. https://doi.org/10.1186/s13058-015-0579-y.
Weissenborn C, Ignatov T, Poehlmann A, Wege AK, Costa SD, Zenclussen AC, Ignatov A. GPER functions as a tumor suppressor in MCF-7 and SK-BR-3 breast cancer cells. J Cancer Res Clin Oncol. 2014;140(4):663–71. https://doi.org/10.1007/s00432-014-1598-2.
Weissenborn C, Ignatov T, Nass N, Kalinski T, Dan Costa S, Zenclussen AC, Ignatov A. GPER promoter methylation controls GPER expression in breast cancer patients. Cancer Investig. 2017;35(2):100–7. https://doi.org/10.1080/07357907.2016.1271886.
Poola I, Abraham J, Liu A, Marshalleck JJ, Dewitty RL. The cell surface estrogen receptor, G protein-coupled receptor 30 (GPR30), is markedly down regulated during breast tumorigenesis. Breast Cancer. 2008;1:65–78.
Weissenborn C, Ignatov T, Ochel HJ, Costa SD, Zenclussen AC, Ignatova Z, Ignatov A. GPER functions as a tumor suppressor in triple-negative breast cancer cells. J Cancer Res Clin Oncol. 2014;140(5):713–23. https://doi.org/10.1007/s00432-014-1620-8.
Chen ZJ, Wei W, Jiang GM, Liu H, Wei WD, Yang X, Wu YM, Liu H, Wong CK, Du J, Wang HS. Activation of GPER suppresses epithelial mesenchymal transition of triple negative breast cancer cells via NF-kappaB signals. Mol Oncol. 2016. https://doi.org/10.1016/j.molonc.2016.01.002.
Plante BJ, Lessey BA, Taylor RN, Wang W, Bagchi MK, Yuan L, Scotchie J, Fritz MA, Young SL. G protein-coupled estrogen receptor (GPER) expression in normal and abnormal endometrium. Reprod Sci. 2012;19(7):684–93. https://doi.org/10.1177/1933719111431000.
Samartzis N, Samartzis EP, Noske A, Fedier A, Dedes KJ, Caduff R, Fink D, Imesch P. Expression of the G protein-coupled estrogen receptor (GPER) in endometriosis: a tissue microarray study. Reprod Biol Endocrinol. 2012;10:30. https://doi.org/10.1186/1477-7827-10-30.
He YY, Cai B, Yang YX, Liu XL, Wan XP. Estrogenic G protein-coupled receptor 30 signaling is involved in regulation of endometrial carcinoma by promoting proliferation, invasion potential, and interleukin-6 secretion via the MEK/ERK mitogen-activated protein kinase pathway. Cancer Sci. 2009;100(6):1051–61. https://doi.org/10.1111/j.1349-7006.2009.01148.x.
Skrzypczak M, Schuler S, Lattrich C, Ignatov A, Ortmann O, Treeck O. G protein-coupled estrogen receptor (GPER) expression in endometrial adenocarcinoma and effect of agonist G-1 on growth of endometrial adenocarcinoma cell lines. Steroids. 2013;78(11):1087–91. https://doi.org/10.1016/j.steroids.2013.07.007.
Tica AA, Tica OS, Georgescu CV, Pirici D, Bogdan M, Ciurea T, Mogoanta SS, Georgescu CC, Comanescu AC, Balseanu TA, Ciurea RN, Osiac E, Buga AM, Ciurea ME. GPER and ERalpha expression in abnormal endometrial proliferations. Romanian J Morphol Embryol. 2016;57(2):413–8.
Krakstad C, Trovik J, Wik E, Engelsen IB, Werner HM, Birkeland E, Raeder MB, Oyan AM, Stefansson IM, Kalland KH, Akslen LA, Salvesen HB. Loss of GPER identifies new targets for therapy among a subgroup of ERalpha-positive endometrial cancer patients with poor outcome. Br J Cancer. 2012;106(10):1682–8. https://doi.org/10.1038/bjc.2012.91.
Huang GS, Gunter MJ, Arend RC, Li M, Arias-Pulido H, Prossnitz ER, Goldberg GL, Smith HO. Co-expression of GPR30 and ERbeta and their association with disease progression in uterine carcinosarcoma. Am J Obstet Gynecol. 2010;203(3):242.e241–5. https://doi.org/10.1016/j.ajog.2010.04.046.
Parker LP, Taylor DD, Kesterson S, Gercel-Taylor C. Gene expression profiling in response to estradiol and genistein in ovarian cancer cells. Cancer Genomics Proteomics. 2009;6(3):189–94.
Heublein S, Mayr D, Friese K, Jarrin-Franco MC, Lenhard M, Mayerhofer A, Jeschke U. The G-protein-coupled estrogen receptor (GPER/GPR30) in ovarian granulosa cell tumors. Int J Mol Sci. 2014;15(9):15161–72. https://doi.org/10.3390/ijms150915161.
Francois CM, Wargnier R, Petit F, Goulvent T, Rimokh R, Treilleux I, Ray-Coquard I, Zazzu V, Cohen-Tannoudji J, Guigon CJ. 17beta-estradiol inhibits spreading of metastatic cells from granulosa cell tumors through a non-genomic mechanism involving GPER1. Carcinogenesis. 2015;36(5):564–73. https://doi.org/10.1093/carcin/bgv041.
Smith HO, Arias-Pulido H, Kuo DY, Howard T, Qualls CR, Lee SJ, Verschraegen CF, Hathaway HJ, Joste NE, Prossnitz ER. GPR30 predicts poor survival for ovarian cancer. Gynecol Oncol. 2009;114(3):465–71. https://doi.org/10.1016/j.ygyno.2009.05.015.
Long L, Cao Y, Tang LD. Transmembrane estrogen receptor GPR30 is more frequently expressed in malignant than benign ovarian endometriotic cysts and correlates with MMP-9 expression. Int J Gynecol Cancer. 2012;22(4):539–45. https://doi.org/10.1097/IGC.0b013e318247323d.
Ghazarian AA, Trabert B, Devesa SS, McGlynn KA. Recent trends in the incidence of testicular germ cell tumors in the United States. Andrology. 2015;3(1):13–8. https://doi.org/10.1111/andr.288.
Chevalier N, Paul-Bellon R, Camparo P, Michiels JF, Chevallier D, Fenichel P. Genetic variants of GPER/GPR30, a novel estrogen-related G protein receptor, are associated with human seminoma. Int J Mol Sci. 2014;15(1):1574–89. https://doi.org/10.3390/ijms15011574.
Franco R, Boscia F, Gigantino V, Marra L, Esposito F, Ferrara D, Pariante P, Botti G, Caraglia M, Minucci S, Chieffi P. GPR30 is overexpressed in post-puberal testicular germ cell tumors. Cancer Biol Ther. 2011;11(6):609–13.
Rago V, Romeo F, Giordano F, Maggiolini M, Carpino A. Identification of the estrogen receptor GPER in neoplastic and non-neoplastic human testes. Reprod Biol Endocrinol. 2011;9:135. https://doi.org/10.1186/1477-7827-9-135.
Chieffi P. An overview on predictive biomarkers of testicular germ cell tumors. J Cell Physiol. 2017;232(2):276–80. https://doi.org/10.1002/jcp.25482.
Liu C, Liao Y, Fan S, Tang H, Jiang Z, Zhou B, Xiong J, Zhou S, Zou M, Wang J. G protein-coupled estrogen receptor (GPER) mediates NSCLC progression induced by 17beta-estradiol (E2) and selective agonist G1. Med Oncol. 2015;32(4):104. https://doi.org/10.1007/s12032-015-0558-2.
Mau M, Mielenz M, Sudekum KH, Obukhov AG. Expression of GPR30 and GPR43 in oral tissues: deriving new hypotheses on the role of diet in animal physiology and the development of oral cancers. J Anim Physiol Anim Nutr. 2011;95(3):280–5. https://doi.org/10.1111/j.1439-0396.2010.01052.x.
Tang C, Yang L, Wang N, Li L, Xu M, Chen GG, Liu ZM. High expression of GPER1, EGFR and CXCR1 is associated with lymph node metastasis in papillary thyroid carcinoma. Int J Clin Exp Pathol. 2014;7(6):3213–23.
Zhao L, Zhu XY, Jiang R, Xu M, Wang N, Chen GG, Liu ZM. Role of GPER1, EGFR and CXCR1 in differentiating between malignant follicular thyroid carcinoma and benign follicular thyroid adenoma. Int J Clin Exp Pathol. 2015;8(9):11236–47.
Yamasaki M, Mukai A, Ohba M, Mine Y, Sakakibara Y, Suiko M, Morishita K, Nishiyama K. Genistein induced apoptotic cell death in adult T-cell leukemia cells through estrogen receptors. Biosci Biotechnol Biochem. 2010;74(10):2113–5. https://doi.org/10.1271/bbb.100359.
Huang W, Chen Y, Liu Y, Zhang Q, Yu Z, Mou L, Wu H, Zhao L, Long T, Qin D, Gui Y. Roles of ERbeta and GPR30 in proliferative response of human bladder cancer cell to estrogen. Biomed Res Int. 2015;2015:251780. https://doi.org/10.1155/2015/251780.
Glass JP, Parasher G, Arias-Pulido H, Donohue R, Prossnitz ER, Cerilli LA. Mesothelin and GPR30 staining among a spectrum of pancreatic epithelial neoplasms. Int J Surg Pathol. 2011;19(5):588–96. https://doi.org/10.1177/1066896911409575.
Zhang Q, Wu YZ, Zhang YM, Ji XH, Hao Q. Activation of G-protein coupled estrogen receptor inhibits the proliferation of cervical cancer cells via sustained activation of ERK1/2. Cell Biochem Funct. 2015;33(3):134–42. https://doi.org/10.1002/cbf.3097.
Guan BZ, Yan RL, Huang JW, Li FL, Zhong YX, Chen Y, Liu FN, Hu B, Huang SB, Yin LH. Activation of G protein coupled estrogen receptor (GPER) promotes the migration of renal cell carcinoma via the PI3K/AKT/MMP-9 signals. Cell Adhes Migr. 2015. https://doi.org/10.4161/19336918.2014.990781.
Watson CS, Jeng YJ, Hu G, Wozniak A, Bulayeva N, Guptarak J. Estrogen- and xenoestrogen-induced ERK signaling in pituitary tumor cells involves estrogen receptor-alpha interactions with G protein-alphai and caveolin I. Steroids. 2012;77(5):424–32. https://doi.org/10.1016/j.steroids.2011.12.025.
Scaling AL, Prossnitz ER, Hathaway HJ. GPER mediates estrogen-induced signaling and proliferation in human breast epithelial cells and normal and malignant breast. Horm Cancer. 2014;5(3):146–60. https://doi.org/10.1007/s12672-014-0174-1.
Luo H, Yang G, Yu T, Luo S, Wu C, Sun Y, Liu M, Tu G. GPER-mediated proliferation and estradiol production in breast cancer-associated fibroblasts. Endocr Relat Cancer. 2014;21(2):355–69. https://doi.org/10.1530/erc-13-0237.
Lappano R, Maggiolini M. GPER is involved in the functional liaison between breast tumor cells and cancer-associated fibroblasts (CAFs). J Steroid Biochem Mol Biol. 2017. https://doi.org/10.1016/j.jsbmb.2017.02.019.
He YY, Du GQ, Cai B, Yan Q, Zhou L, Chen XY, Lu W, Yang YX, Wan XP. Estrogenic transmembrane receptor of GPR30 mediates invasion and carcinogenesis by endometrial cancer cell line RL95-2. J Cancer Res Clin Oncol. 2012;138(5):775–83. https://doi.org/10.1007/s00432-011-1133-7.
Du GQ, Zhou L, Chen XY, Wan XP, He YY. The G protein-coupled receptor GPR30 mediates the proliferative and invasive effects induced by hydroxytamoxifen in endometrial cancer cells. Biochem Biophys Res Commun. 2012;420(2):343–9. https://doi.org/10.1016/j.bbrc.2012.02.161.
Jiang X, Ye X, Ma J, Li W, Wu R, Jun L. G protein-coupled estrogen receptor 1 (GPER 1) mediates estrogen-induced, proliferation of leiomyoma cells. Gynecol Endocrinol. 2015;31(11):894–8. https://doi.org/10.3109/09513590.2015.1092022.
Imesch P, Samartzis EP, Dedes KJ, Fink D, Fedier A. Histone deacetylase inhibitors down-regulate G-protein-coupled estrogen receptor and the GPER-antagonist G-15 inhibits proliferation in endometriotic cells. Fertil Steril. 2013;100(3):770–6. https://doi.org/10.1016/j.fertnstert.2013.05.008.
Zhang H, Wang X, Chen Z, Wang W. MicroRNA-424 suppresses estradiol-induced cell proliferation via targeting GPER in endometrial cancer cells. Cell Mol Biol (Noisy-le-Grand). 2015;61(7):96–101.
Liu H, Yan Y, Wen H, Jiang X, Cao X, Zhang G, Liu G. A novel estrogen receptor GPER mediates proliferation induced by 17beta-estradiol and selective GPER agonist G-1 in estrogen receptor alpha (ERalpha)-negative ovarian cancer cells. Cell Biol Int. 2014;38(5):631–8. https://doi.org/10.1002/cbin.10243.
Sirianni R, Chimento A, Ruggiero C, De Luca A, Lappano R, Ando S, Maggiolini M, Pezzi V. The novel estrogen receptor, G protein-coupled receptor 30, mediates the proliferative effects induced by 17beta-estradiol on mouse spermatogonial GC-1 cell line. Endocrinology. 2008;149(10):5043–51. https://doi.org/10.1210/en.2007-1593.
Vivacqua A, Bonofiglio D, Albanito L, Madeo A, Rago V, Carpino A, Musti AM, Picard D, Ando S, Maggiolini M. 17beta-estradiol, genistein, and 4-hydroxytamoxifen induce the proliferation of thyroid cancer cells through the g protein-coupled receptor GPR30. Mol Pharmacol. 2006;70(4):1414–23. https://doi.org/10.1124/mol.106.026344.
Rudelius M, Rauert-Wunderlich H, Hartmann E, Hoster E, Dreyling M, Klapper W, Ott G, Rosenwald A. The G protein-coupled estrogen receptor 1 (GPER-1) contributes to the proliferation and survival of mantle cell lymphoma cells. Haematologica. 2015;100(11):e458–61. https://doi.org/10.3324/haematol.2015.127399.
Pupo M, Pisano A, Lappano R, Santolla MF, De Francesco EM, Abonante S, Rosano C, Maggiolini M. Bisphenol A induces gene expression changes and proliferative effects through GPER in breast cancer cells and cancer-associated fibroblasts. Environ Health Perspect. 2012;120(8):1177–82. https://doi.org/10.1289/ehp.1104526.
Chevalier N, Bouskine A, Fenichel P. Bisphenol A promotes testicular seminoma cell proliferation through GPER/GPR30. Int J Cancer. 2012;130(1):241–2. https://doi.org/10.1002/ijc.25972.
Bouskine A, Nebout M, Brucker-Davis F, Benahmed M, Fenichel P. Low doses of bisphenol A promote human seminoma cell proliferation by activating PKA and PKG via a membrane G-protein-coupled estrogen receptor. Environ Health Perspect. 2009;117(7):1053–8. https://doi.org/10.1289/ehp.0800367.
Wei W, Chen ZJ, Zhang KS, Yang XL, Wu YM, Chen XH, Huang HB, Liu HL, Cai SH, Du J, Wang HS. The activation of G protein-coupled receptor 30 (GPR30) inhibits proliferation of estrogen receptor-negative breast cancer cells in vitro and in vivo. Cell Death Dis. 2014;5:e1428. https://doi.org/10.1038/cddis.2014.398.
Lv X, He C, Huang C, Hua G, Wang Z, Remmenga SW, Rodabaugh KJ, Karpf AR, Dong J, Davis JS, Wang C. G-1 inhibits breast cancer cell growth via targeting colchicine-binding site of tubulin to interfere with microtubule assembly. Mol Cancer Ther. 2017. https://doi.org/10.1158/1535-7163.mct-16-0626.
Wang C, Lv X, He C, Hua G, Tsai MY, Davis JS. The G-protein-coupled estrogen receptor agonist G-1 suppresses proliferation of ovarian cancer cells by blocking tubulin polymerization. Cell Death Dis. 2013;4:e869. https://doi.org/10.1038/cddis.2013.397.
Holm A, Baldetorp B, Olde B, Leeb-Lundberg LM, Nilsson BO. The GPER1 agonist G-1 attenuates endothelial cell proliferation by inhibiting DNA synthesis and accumulating cells in the S and G2 phases of the cell cycle. J Vasc Res. 2011;48(4):327–35. https://doi.org/10.1159/000322578.
Duarte-Guterman P, Lieblich SE, Chow C, Galea LA. Estradiol and GPER activation differentially affect cell proliferation but not GPER expression in the hippocampus of adult female rats. PLoS One. 2015;10(6):e0129880. https://doi.org/10.1371/journal.pone.0129880.
Correia S, Cardoso HJ, Cavaco JE, Socorro S. Oestrogens as apoptosis regulators in mammalian testis: angels or devils? Expert Rev Mol Med. 2015;17. https://doi.org/10.1017/erm.2014.25.
Lawen A. Apoptosis-an introduction. BioEssays. 2003;25(9):888–96. https://doi.org/10.1002/bies.10329.
Royer C, Lucas TF, Lazari MF, Porto CS. 17Beta-estradiol signaling and regulation of proliferation and apoptosis of rat Sertoli cells. Biol Reprod. 2012;86(4):108. https://doi.org/10.1095/biolreprod.111.096891.
Li WL, Xiang W, Ping Y. Activation of novel estrogen receptor GPER results in inhibition of cardiocyte apoptosis and cardioprotection. Mol Med Rep. 2015;12(2):2425–30. https://doi.org/10.3892/mmr.2015.3674.
Bopassa JC, Eghbali M, Toro L, Stefani E. A novel estrogen receptor GPER inhibits mitochondria permeability transition pore opening and protects the heart against ischemia-reperfusion injury. Am J Phys Heart Circ Phys. 2010;298(1):H16–23. https://doi.org/10.1152/ajpheart.00588.2009.
Sbert-Roig M, Bauza-Thorbrugge M, Galmes-Pascual BM, Capllonch-Amer G, Garcia-Palmer FJ, Llado I, Proenza AM, Gianotti M. GPER mediates the effects of 17beta-estradiol in cardiac mitochondrial biogenesis and function. Mol Cell Endocrinol. 2016;420:116–24. https://doi.org/10.1016/j.mce.2015.11.027.
Chen J, Hu R, Ge H, Duanmu W, Li Y, Xue X, Hu S, Feng H. G-protein-coupled receptor 30-mediated antiapoptotic effect of estrogen on spinal motor neurons following injury and its underlying mechanisms. Mol Med Rep. 2015;12(2):1733–40. https://doi.org/10.3892/mmr.2015.3601.
Zekas E, Prossnitz ER. Estrogen-mediated inactivation of FOXO3a by the G protein-coupled estrogen receptor GPER. BMC Cancer. 2015;15:702. https://doi.org/10.1186/s12885-015-1699-6.
Calnan DR, Brunet A. The FoxO code. Oncogene. 2008;27(16):2276–88. https://doi.org/10.1038/onc.2008.21.
Broselid S, Cheng B, Sjostrom M, Lovgren K, Klug-De Santiago HL, Belting M, Jirstrom K, Malmstrom P, Olde B, Bendahl PO, Hartman L, Ferno M, Leeb-Lundberg LM. G protein-coupled estrogen receptor is apoptotic and correlates with increased distant disease-free survival of estrogen receptor-positive breast cancer patients. Clin Cancer Res. 2013;19(7):1681–92. https://doi.org/10.1158/1078-0432.ccr-12-2376.
Chimento A, Casaburi I, Bartucci M, Patrizii M, Dattilo R, Avena P, Ando S, Pezzi V, Sirianni R. Selective GPER activation decreases proliferation and activates apoptosis in tumor Leydig cells. Cell Death Dis. 2013;4:e747. https://doi.org/10.1038/cddis.2013.275.
Mori T, Ito F, Matsushima H, Takaoka O, Tanaka Y, Koshiba A, Kusuki I, Kitawaki J. G protein-coupled estrogen receptor 1 agonist G-1 induces cell cycle arrest in the mitotic phase, leading to apoptosis in endometriosis. Fertil Steril. 2015;103(5):1228–1235.e1221. https://doi.org/10.1016/j.fertnstert.2015.01.026.
Kurt AH, Celik A, Kelleci BM. Oxidative/antioxidative enzyme-mediated antiproliferative and proapoptotic effects of the GPER1 agonist G-1 on lung cancer cells. Oncol Lett. 2015;10(5):3177–82. https://doi.org/10.3892/ol.2015.3711.
Chimento A, Sirianni R, Casaburi I, Ruggiero C, Maggiolini M, Ando S, Pezzi V. 17beta-Estradiol activates GPER- and ESR1-dependent pathways inducing apoptosis in GC-2 cells, a mouse spermatocyte-derived cell line. Mol Cell Endocrinol. 2012;355(1):49–59. https://doi.org/10.1016/j.mce.2012.01.017.
Altmann JB, Yan G, Meeks JF, Abood ME, Brailoiu E, Brailoiu GC. G protein-coupled estrogen receptor-mediated effects on cytosolic calcium and nanomechanics in brain microvascular endothelial cells. J Neurochem. 2015;133(5):629–39. https://doi.org/10.1111/jnc.13066.
Yue J, Zhang Y, Li X, Gong S, Tao J, Jiang X. Activation of G-protein-coupled receptor 30 increases T-type calcium currents in trigeminal ganglion neurons via the cholera toxin-sensitive protein kinase A pathway. Pharmazie. 2014;69(11):804–8.
Hao J, Bao X, Jin B, Wang X, Mao Z, Li X, Wei L, Shen D, Wang JL. Ca2+ channel subunit alpha 1D promotes proliferation and migration of endometrial cancer cells mediated by 17beta-estradiol via the G protein-coupled estrogen receptor. FASEB J. 2015;29(7):2883–93. https://doi.org/10.1096/fj.14-265603.
Ji Y, Han Z, Shao L, Zhao Y. Ultrasound-targeted microbubble destruction of calcium channel subunit alpha 1D siRNA inhibits breast cancer via G protein-coupled receptor 30. Oncol Rep. 2016;36(4):1886–92. https://doi.org/10.3892/or.2016.5031.
Okegawa T, Pong RC, Li Y, Hsieh JT. The role of cell adhesion molecule in cancer progression and its application in cancer therapy. Acta Biochim Pol. 2004;51(2):445–57. doi: 035001445
Mehlen P, Puisieux A. Metastasis: a question of life or death. Nat Rev Cancer. 2006;6(6):449–58.
Jiang QF, Wu TT, Yang JY, Dong CR, Wang N, Liu XH, Liu ZM. 17beta-estradiol promotes the invasion and migration of nuclear estrogen receptor-negative breast cancer cells through cross-talk between GPER1 and CXCR1. J Steroid Biochem Mol Biol. 2013;138:314–24. https://doi.org/10.1016/j.jsbmb.2013.07.011.
Xie K. Interleukin-8 and human cancer biology. Cytokine Growth Factor Rev. 2001;12(4):375–91.
Ohshiro K, Schwartz AM, Levine PH, Kumar R. Alternate estrogen receptors promote invasion of inflammatory breast cancer cells via non-genomic signaling. PLoS One. 2012;7(1):e30725. https://doi.org/10.1371/journal.pone.0030725.
Yu T, Liu M, Luo H, Wu C, Tang X, Tang S, Hu P, Yan Y, Wang Z, Tu G. GPER mediates enhanced cell viability and motility via non-genomic signaling induced by 17beta-estradiol in triple-negative breast cancer cells. J Steroid Biochem Mol Biol. 2014;143:392–403. https://doi.org/10.1016/j.jsbmb.2014.05.003.
Li Y, Chen Y, Zhu ZX, Liu XH, Yang L, Wan L, Lei TW, Wang XD. 4-Hydroxytamoxifen-stimulated processing of cyclin E is mediated via G protein-coupled receptor 30 (GPR30) and accompanied by enhanced migration in MCF-7 breast cancer cells. Toxicology. 2013;309:61–5. https://doi.org/10.1016/j.tox.2013.04.012.
De Marco P, Lappano R, De Francesco EM, Cirillo F, Pupo M, Avino S, Vivacqua A, Abonante S, Picard D, Maggiolini M. GPER signalling in both cancer-associated fibroblasts and breast cancer cells mediates a feedforward IL1beta/IL1R1 response. Sci Rep. 2016;6:24354. https://doi.org/10.1038/srep24354.
Liu Y, Du FY, Chen W, Fu PF, Yao MY, Zheng SS. G15 sensitizes epithelial breast cancer cells to doxorubicin by preventing epithelial-mesenchymal transition through inhibition of GPR30. Am J Transl Res. 2015;7(5):967–75.
Ruan SQ, Wang SW, Wang ZH, Zhang SZ. Regulation of HRG-beta1-induced proliferation, migration and invasion of MCF-7 cells by upregulation of GPR30 expression. Mol Med Rep. 2012;6(1):131–8. https://doi.org/10.3892/mmr.2012.874.
Chen Y, Li Z, He Y, Shang D, Pan J, Wang H, Chen H, Zhu Z, Wan L, Wang X. Estrogen and pure antiestrogen fulvestrant (ICI 182 780) augment cell-matrigel adhesion of MCF-7 breast cancer cells through a novel G protein coupled estrogen receptor (GPR30)-to-calpain signaling axis. Toxicol Appl Pharmacol. 2014;275(2):176–81. https://doi.org/10.1016/j.taap.2014.01.005.
Castillo Sanchez R, Gomez R, Perez Salazar E. Bisphenol A induces migration through a GPER-, FAK-, Src-, and ERK2-dependent pathway in MDA-MB-231 breast cancer cells. Chem Res Toxicol. 2016;29(3):285–95. https://doi.org/10.1021/acs.chemrestox.5b00457.
Yan Y, Liu H, Wen H, Jiang X, Cao X, Zhang G, Liu G. The novel estrogen receptor GPER regulates the migration and invasion of ovarian cancer cells. Mol Cell Biochem. 2013;378(1–2):1–7. https://doi.org/10.1007/s11010-013-1579-9.
Yan Y, Jiang X, Zhao Y, Wen H, Liu G. Role of GPER on proliferation, migration and invasion in ligand-independent manner in human ovarian cancer cell line SKOV3. Cell Biochem Funct. 2015;33(8):552–9. https://doi.org/10.1002/cbf.3154.
Siesser PM, Hanks SK. The signaling and biological implications of FAK overexpression in cancer. Clin Cancer Res. 2006;12(11 Pt 1):3233–7. https://doi.org/10.1158/1078-0432.ccr-06-0456.
Tsai CL, Wu HM, Lin CY, Lin YJ, Chao A, Wang TH, Hsueh S, Lai CH, Wang HS. Estradiol and tamoxifen induce cell migration through GPR30 and activation of focal adhesion kinase (FAK) in endometrial cancers with low or without nuclear estrogen receptor alpha (ERalpha). PLoS One. 2013;8(9):e72999. https://doi.org/10.1371/journal.pone.0072999.
Avino S, De Marco P, Cirillo F, Santolla MF, De Francesco EM, Perri MG, Rigiracciolo D, Dolce V, Belfiore A, Maggiolini M, Lappano R, Vivacqua A. Stimulatory actions of IGF-I are mediated by IGF-IR cross-talk with GPER and DDR1 in mesothelioma and lung cancer cells. Oncotarget. 2016;7(33):52710–28. 10.18632/oncotarget.10348.
Fraser SP, Ozerlat-Gunduz I, Onkal R, Diss JK, Latchman DS, Djamgoz MB. Estrogen and non-genomic upregulation of voltage-gated Na(+) channel activity in MDA-MB-231 human breast cancer cells: role in adhesion. J Cell Physiol. 2010;224(2):527–39. https://doi.org/10.1002/jcp.22154.
Henic E, Noskova V, Hoyer-Hansen G, Hansson S, Casslen B. Estradiol attenuates EGF-induced rapid uPAR mobilization and cell migration via the G-protein-coupled receptor 30 in ovarian cancer cells. Int J Gynecol Cancer. 2009;19(2):214–22. https://doi.org/10.1111/IGC.0b013e31819bcb75.
Zhu G, Huang Y, Wu C, Wei D, Shi Y. Activation of G-protein-coupled estrogen receptor inhibits the migration of human nonsmall cell lung cancer cells via IKK-beta/NF-kappaB signals. DNA Cell Biol. 2016;35(8):434–42. https://doi.org/10.1089/dna.2016.3235.
Sharma G, Hu C, Brigman JL, Zhu G, Hathaway HJ, Prossnitz ER. GPER deficiency in male mice results in insulin resistance, dyslipidemia, and a proinflammatory state. Endocrinology. 2013;154(11):4136–45. https://doi.org/10.1210/en.2013-1357.
Chakrabarti S, Davidge ST. G-protein coupled receptor 30 (GPR30): a novel regulator of endothelial inflammation. PLoS One. 2012;7(12):e52357. https://doi.org/10.1371/journal.pone.0052357.
Itoga M, Konno Y, Moritoki Y, Saito Y, Ito W, Tamaki M, Kobayashi Y, Kayaba H, Kikuchi Y, Chihara J, Takeda M, Ueki S, Hirokawa M. G-protein-coupled estrogen receptor agonist suppresses airway inflammation in a mouse model of asthma through IL-10. PLoS One. 2015;10(3):e0123210. https://doi.org/10.1371/journal.pone.0123210.
Okamoto M, Mizukami Y. GPER negatively regulates TNFalpha-induced IL-6 production in human breast cancer cells via NF-kappaB pathway. Endocr J. 2016. https://doi.org/10.1507/endocrj.EJ15-0571.
Hanahan D, Weinberg RA. Hallmarks of cancer: the next generation. Cell. 2011;144(5):646–74. https://doi.org/10.1016/j.cell.2011.02.013.
Warburg O, Wind F, Negelein E. The metabolism of tumors in the body. J Gen Physiol. 1927;8(6):519–30.
Martensson UE, Salehi SA, Windahl S, Gomez MF, Sward K, Daszkiewicz-Nilsson J, Wendt A, Andersson N, Hellstrand P, Grande PO, Owman C, Rosen CJ, Adamo ML, Lundquist I, Rorsman P, Nilsson BO, Ohlsson C, Olde B, Leeb-Lundberg LM. Deletion of the G protein-coupled receptor 30 impairs glucose tolerance, reduces bone growth, increases blood pressure, and eliminates estradiol-stimulated insulin release in female mice. Endocrinology. 2009;150(2):687–98. https://doi.org/10.1210/en.2008-0623.
Sharma G, Prossnitz ER. Mechanisms of estradiol-induced insulin secretion by the G protein-coupled estrogen receptor GPR30/GPER in pancreatic beta-cells. Endocrinology. 2011;152(8):3030–9. https://doi.org/10.1210/en.2011-0091.
Xie BY, Lv QY, Ning CC, Yang BY, Shan WW, Cheng YL, Gu C, Luo XZ, Zhang ZB, Chen XJ, Xi XW, Feng YJ. TET1-GPER-PI3K/AKT pathway is involved in insulin-driven endometrial cancer cell proliferation. Biochem Biophys Res Commun. 2017;482(4):857–62. https://doi.org/10.1016/j.bbrc.2016.11.124.
Yu T, Yang G, Hou Y, Tang X, Wu C, Wu XA, Guo L, Zhu Q, Luo H, Du YE, Wen S, Xu L, Yin J, Tu G, Liu M. Cytoplasmic GPER translocation in cancer-associated fibroblasts mediates cAMP/PKA/CREB/glycolytic axis to confer tumor cells with multidrug resistance. Oncogene. 2016. https://doi.org/10.1038/onc.2016.370.
Altman BJ, Stine ZE, Dang CV. From Krebs to clinic: glutamine metabolism to cancer therapy. Nat Rev Cancer. 2016;16(10):619–34. https://doi.org/10.1038/nrc.2016.71.
Rothstein JD, Dykes-Hoberg M, Pardo CA, Bristol LA, Jin L, Kuncl RW, Kanai Y, Hediger MA, Wang Y, Schielke JP, Welty DF. Knockout of glutamate transporters reveals a major role for astroglial transport in excitotoxicity and clearance of glutamate. Neuron. 1996;16(3):675–86.
Lee E, Sidoryk-Wegrzynowicz M, Wang N, Webb A, Son DS, Lee K, Aschner M. GPR30 regulates glutamate transporter GLT-1 expression in rat primary astrocytes. J Biol Chem. 2012;287(32):26817–28. https://doi.org/10.1074/jbc.M112.341867.
Tiano JP, Delghingaro-Augusto V, Le May C, Liu S, Kaw MK, Khuder SS, Latour MG, Bhatt SA, Korach KS, Najjar SM, Prentki M, Mauvais-Jarvis F. Estrogen receptor activation reduces lipid synthesis in pancreatic islets and prevents beta cell failure in rodent models of type 2 diabetes. J Clin Invest. 2011;121(8):3331–42. https://doi.org/10.1172/jci44564.
Cha JY, Repa JJ. The liver X receptor (LXR) and hepatic lipogenesis. The carbohydrate-response element-binding protein is a target gene of LXR. J Biol Chem. 2007;282(1):743–51. https://doi.org/10.1074/jbc.M605023200.
Repa JJ, Liang G, Ou J, Bashmakov Y, Lobaccaro JM, Shimomura I, Shan B, Brown MS, Goldstein JL, Mangelsdorf DJ. Regulation of mouse sterol regulatory element-binding protein-1c gene (SREBP-1c) by oxysterol receptors, LXRalpha and LXRbeta. Genes Dev. 2000;14(22):2819–30.
Uyeda K, Repa JJ. Carbohydrate response element binding protein, ChREBP, a transcription factor coupling hepatic glucose utilization and lipid synthesis. Cell Metab. 2006;4(2):107–10. https://doi.org/10.1016/j.cmet.2006.06.008.
Tiano JP, Mauvais-Jarvis F. Molecular mechanisms of estrogen receptors' suppression of lipogenesis in pancreatic beta-cells. Endocrinology. 2012;153(7):2997–3005. https://doi.org/10.1210/en.2011-1980.
Santolla MF, Lappano R, De Marco P, Pupo M, Vivacqua A, Sisci D, Abonante S, Iacopetta D, Cappello AR, Dolce V, Maggiolini M. G protein-coupled estrogen receptor mediates the up-regulation of fatty acid synthase induced by 17beta-estradiol in cancer cells and cancer-associated fibroblasts. J Biol Chem. 2012;287(52):43234–45. https://doi.org/10.1074/jbc.M112.417303.
Horton JD, Cohen JC, Hobbs HH. Molecular biology of PCSK9: its role in LDL metabolism. Trends Biochem Sci. 2007;32(2):71–7. https://doi.org/10.1016/j.tibs.2006.12.008.
Hussain Y, Ding Q, Connelly PW, Brunt JH, Ban MR, McIntyre AD, Huff MW, Gros R, Hegele RA, Feldman RD. G-protein estrogen receptor as a regulator of low-density lipoprotein cholesterol metabolism: cellular and population genetic studies. Arterioscler Thromb Vasc Biol. 2015;35(1):213–21. https://doi.org/10.1161/atvbaha.114.304326.
Wang A, Luo J, Moore W, Alkhalidy H, Wu L, Zhang J, Zhen W, Wang Y, Clegg DJ, Bin X, Cheng Z, McMillan RP, Hulver MW, Liu D. GPR30 regulates diet-induced adiposity in female mice and adipogenesis in vitro. Sci Rep. 2016;6:34302. https://doi.org/10.1038/srep34302.
Hall DA, Zhu H, Zhu X, Royce T, Gerstein M, Snyder M. Regulation of gene expression by a metabolic enzyme. Science (New York, NY). 2004;306(5695):482–4. https://doi.org/10.1126/science.1096773.
Zhuang Y, Xiang J, Bao W, Sun Y, Wang L, Tan M, He Y, Xi X. MDH2 stimulated by estrogen-GPR30 pathway down-regulated PTEN expression promoting the proliferation and invasion of cells in endometrial cancer. Transl Oncol. 2017;10(2):203–10. https://doi.org/10.1016/j.tranon.2017.01.009.
Siegel R, Ma J, Zou Z, Jemal A. Cancer statistics, 2014. CA. 2014;64(1):9–29. https://doi.org/10.3322/caac.21208.
Ribal MJ, Martínez-Salamanca JI, García Freire C (2015) Current patterns of management of advanced prostate cancer in routine clinical practice in Spain. Prostate Cancer. 2015:6. doi:https://doi.org/10.1155/2015/186740.
Karantanos T, Corn PG, Thompson TC. Prostate cancer progression after androgen deprivation therapy: mechanisms of castrate resistance and novel therapeutic approaches. Oncogene. 2013;32(49):5501–11. https://doi.org/10.1038/onc.2013.206.
Huggins C. Endocrine control of prostatic cancer. Science (New York, NY). 1943;97(2529):541–4. https://doi.org/10.1126/science.97.2529.541.
Ricke WA, McPherson SJ, Bianco JJ, Cunha GR, Wang Y, Risbridger GP. Prostatic hormonal carcinogenesis is mediated by in situ estrogen production and estrogen receptor alpha signaling. FASEB J. 2008;22(5):1512–20. https://doi.org/10.1096/fj.07-9526com.
Yang M, Wang J, Wang L, Shen C, Su B, Qi M, Hu J, Gao W, Tan W, Han B. Estrogen induces androgen-repressed SOX4 expression to promote progression of prostate cancer cells. Prostate. 2015;75(13):1363–75. https://doi.org/10.1002/pros.23017.
Denmeade S, Isaacs J. Androgen deprivation strategies in the treatment of advanced prostate cancer. In: Kufe DW, Pollock RE, Weichselbaum RR, et al., editors. Holland-Frei cancer medicine. Hamilton, ON: BC Decker; 2000.
Montgomery B, Nelson PS, Vessella R, Kalhorn T, Hess D, Corey E. Estradiol suppresses tissue androgens and prostate cancer growth in castration resistant prostate cancer. BMC Cancer. 2010;10:244. https://doi.org/10.1186/1471-2407-10-244.
Figueira MI, Correia S, Vaz CV, Cardoso HJ, Gomes IM, Marques R, Maia CJ, Socorro S. Estrogens down-regulate the stem cell factor (SCF)/c-KIT system in prostate cells: evidence of antiproliferative and proapoptotic effects. Biochem Pharmacol. 2016;99:73–87. https://doi.org/10.1016/j.bcp.2015.11.016.
Levin ER. Integration of the extranuclear and nuclear actions of estrogen. Mol Endocrinol. 2005;19(8):1951–9. https://doi.org/10.1210/me.2004-0390.
Nelson AW, Tilley WD, Neal DE, Carroll JS. Estrogen receptor beta in prostate cancer: friend or foe? Endocr Relat Cancer. 2014;21(4):T219–34. https://doi.org/10.1530/erc-13-0508.
Signoretti S, Loda M. Prostate stem cells: from development to cancer. Semin Cancer Biol. 2007;17(3):219–24. https://doi.org/10.1016/j.semcancer.2006.04.004.
Rago V, Romeo F, Giordano F, Ferraro A, Carpino A. Identification of the G protein-coupled estrogen receptor (GPER) in human prostate: expression site of the estrogen receptor in the benign and neoplastic gland. Andrology. 2016;4(1):121–7. https://doi.org/10.1111/andr.12131.
Hu WY, Shi GB, Lam HM, Hu DP, Ho SM, Madueke IC, Kajdacsy-Balla A, Prins GS. Estrogen-initiated transformation of prostate epithelium derived from normal human prostate stem-progenitor cells. Endocrinology. 2011;152(6):2150–63. https://doi.org/10.1210/en.2010-1377.
Pisolato R, Lombardi AP, Vicente CM, Lucas TF, Lazari MF, Porto CS. Expression and regulation of the estrogen receptors in PC-3 human prostate cancer cells. Steroids. 2015. https://doi.org/10.1016/j.steroids.2015.12.021.
Chan QK, Lam HM, Ng CF, Lee AY, Chan ES, Ng HK, Ho SM, Lau KM. Activation of GPR30 inhibits the growth of prostate cancer cells through sustained activation of Erk1/2, c-jun/c-fos-dependent upregulation of p21, and induction of G(2) cell-cycle arrest. Cell Death Differ. 2010;17(9):1511–23. https://doi.org/10.1038/cdd.2010.20.
Zhang Z, Duan L, Du X, Ma H, Park I, Lee C, Zhang J, Shi J. The proliferative effect of estradiol on human prostate stromal cells is mediated through activation of ERK. Prostate. 2008;68(5):508–16. https://doi.org/10.1002/pros.20722.
Schade GR, Holt S, Zhang X, Song D, Wright JL, Zhao S, Kolb S, Lam HM, Levin L, Leung YK, Ho SM, Stanford JL. Prostate cancer expression profiles of cytoplasmic ERbeta1 and nuclear ERbeta2 are associated with poor outcomes following radical prostatectomy. J Urol. 2016. https://doi.org/10.1016/j.juro.2015.12.101.
Gan WD, Zhou M, Hu Y, Li DM, Jia RP. Low-dose nonylphenol promotes the proliferation of DU-145 cells and expression of membrane estrogen receptor GPR30 in DU-145 cells. Zhonghua Nan Ke Xue. 2014;20(5):405–9.
Lam HM, Ouyang B, Chen J, Ying J, Wang J, Wu CL, Jia L, Medvedovic M, Vessella RL, Ho SM. Targeting GPR30 with G-1: a new therapeutic target for castration-resistant prostate cancer. Endocr Relat Cancer. 2014;21(6):903–14. https://doi.org/10.1530/erc-14-0402.
Park II, Zhang Q, Liu V, Kozlowski JM, Zhang J, Lee C. 17Beta-estradiol at low concentrations acts through distinct pathways in normal versus benign prostatic hyperplasia-derived prostate stromal cells. Endocrinology. 2009;150(10):4594–605. https://doi.org/10.1210/en.2008-1591.
Koong LY, Watson CS. Direct estradiol and diethylstilbestrol actions on early- versus late-stage prostate cancer cells. Prostate. 2014;74(16):1589–603. https://doi.org/10.1002/pros.22875.
Lau KM, Ma FM, Xia JT, Chan QK, Ng CF, To KF. Activation of GPR30 stimulates GTP-binding of Galphai1 protein to sustain activation of Erk1/2 in inhibition of prostate cancer cell growth and modulates metastatic properties. Exp Cell Res. 2017;350(1):199–209. https://doi.org/10.1016/j.yexcr.2016.11.022.
Comeglio P, Morelli A, Cellai I, Vignozzi L, Sarchielli E, Filippi S, Maneschi E, Corcetto F, Corno C, Gacci M, Vannelli GB, Maggi M. Opposite effects of tamoxifen on metabolic syndrome-induced bladder and prostate alterations: a role for GPR30/GPER? Prostate. 2014;74(1):10–28. https://doi.org/10.1002/pros.22723.
Vaz CV, Alves MG, Marques R, Moreira PI, Oliveira PF, Maia CJ, Socorro S. Androgen-responsive and nonresponsive prostate cancer cells present a distinct glycolytic metabolism profile. Int J Biochem Cell Biol. 2012;44(11):2077–84. https://doi.org/10.1016/j.biocel.2012.08.013.
Vaz CV, Marques R, Alves MG, Oliveira PF, Cavaco JE, Maia CJ, Socorro S. Androgens enhance the glycolytic metabolism and lactate export in prostate cancer cells by modulating the expression of GLUT1, GLUT3, PFK, LDH and MCT4 genes. J Cancer Res Clin Oncol. 2016;142(1):5–16. https://doi.org/10.1007/s00432-015-1992-4.
Massie CE, Lynch A, Ramos-Montoya A, Boren J, Stark R, Fazli L, Warren A, Scott H, Madhu B, Sharma N, Bon H, Zecchini V, Smith DM, Denicola GM, Mathews N, Osborne M, Hadfield J, Macarthur S, Adryan B, Lyons SK, Brindle KM, Griffiths J, Gleave ME, Rennie PS, Neal DE, Mills IG. The androgen receptor fuels prostate cancer by regulating central metabolism and biosynthesis. EMBO J. 2011;30(13):2719–33. https://doi.org/10.1038/emboj.2011.158.
Correia S, Cardoso HJ, Cavaco JE, Socorro S. Oestrogens as apoptosis regulators in mammalian testis: angels or devils? Expert Rev Mol Med. 2015;17:e2. https://doi.org/10.1017/erm.2014.25.
Correia S, Alves MR, Cavaco JE, Oliveira PF, Socorro S. Estrogenic regulation of testicular expression of stem cell factor and c-kit: implications in germ cell survival and male fertility. Fertil Steril. 2014;102(1):299–306. https://doi.org/10.1016/j.fertnstert.2014.04.009.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2018 Springer International Publishing AG
About this chapter

Cite this chapter
Figueira, M.I., Cardoso, H.J., Socorro, S. (2018). The Role of GPER Signaling in Carcinogenesis: A Focus on Prostate Cancer. In: Fayyaz, S., Farooqi, A. (eds) Recent Trends in Cancer Biology: Spotlight on Signaling Cascades and microRNAs. Springer, Cham. https://doi.org/10.1007/978-3-319-71553-7_5
Download citation
DOI: https://doi.org/10.1007/978-3-319-71553-7_5
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-71552-0
Online ISBN: 978-3-319-71553-7
eBook Packages: Biomedical and Life SciencesBiomedical and Life Sciences (R0)