
Abstract
The purpose of this paper is to compare the relevance of four resource indicators (inputs), in regard to six mortality indicators (outputs) within healthcare systems in 27 East European countries.
The correlation between the following input indicators, number of GPs/100,000 population, health expenditure as % of GDP, total health expenditure PPP $/capita, pharmaceutical expenditure PPP $/capita, and the following demographic and output indicators, life expectancy at birth; reduction of life expectancy through death before 65 years; estimated infant mortality/1000 live births; maternal deaths/100,000 live births; SDR diabetes mellitus, all ages/100,000; and SDR tuberculosis, all ages/100,000, was analyzed.
WHO data was used, for the following East European countries: Albania, Armenia, Azerbaijan, Belarus, Bosnia and Herzegovina, Bulgaria, Croatia, Cyprus, Czech Republic, Estonia, Georgia, Greece, Hungary, Latvia, Lithuania, FYROM, Moldova, Montenegro, Poland, Romania, Russia, Serbia, Slovakia, Slovenia, Turkey, and Ukraine. Data from 2011 was used.
The various degrees of correlation between the input and output indicators were analyzed using scatter diagrams and calculating Pearson linear correlation coefficient.
This type of study can be extended to other health outcome indicators as it can be also tried with other healthcare system resource indicators.
The research shows the importance of real data (money) as compared to percentage data.
Many reform projects as well as policy evaluations are based on “weak” indicators, misleading public perception, hiding policy mistakes, and ultimately leading focus to unimportant things.
The paper tries to shed light on indicators which are really significant from the point of view of policymakers. It might be also of particular interest to students who can understand better the use of indicators.
This paper will be presented as PPT.
Access provided by CONRICYT-eBooks. Download conference paper PDF
Similar content being viewed by others


Keywords
1 Introduction
Within the public space, the media, and academics, we hear many times that health systems need to be reformed, that performance needs to be improved, and that things need to change for the better. In order to demonstrate the truthfulness of the above, many outcome indicators are called forth. Not all of them are very specific and some are quite broad (to be more understandable). Naturally, there are various ideas about the necessary inputs to achieve good results. The purpose of this paper is to shed some light on this issue, namely, to see what are the correlations between four input indicators and six outcome indicators. A lot of money is put in projects related to healthcare reforms. Important resources are allocated to tackle the issues and improve health outcomes. Policies are debated and adopted based on assumptions that certain input increase will lead to certain good outcomes. The only way to find out how valid these assumptions are is to study the correlation between certain input indicators and outcome indicators.
2 Body of the Paper
2.1 Data
The input indicators used are the following:
The number of the general practitioners per 100,000 population (no. of GPs/100,000). It is assumed that the greater this number, the better healthcare is delivered.
The second input indicator is the total health expenditure as % of GDP. The gross domestic product (GDP) is defined as the monetary value of all goods and services produced in an economy over a certain period of time (Market House Books Ltd. 1990a). So the indicator, “total health expenditure as percentage of GDP,” is merely an indicator of the size of the health sector within the economy of a country, in monetary terms.
The third financial input indicator was the total healthcare expenditure in PPP $/capita. The indicator total health expenditure/capita is adjusted in the data used with purchasing power parity (PPP) which is parity between two currencies that will give each currency exactly the same purchasing power in its own country (Market House Books Ltd. 1990b).
Finally, the fourth indicator was pharmaceutical expenditure in PPP $/capita. Again the raw indicator, pharmaceutical expenditure/capita, is adjusted with purchasing power parity for adjusting the purchasing power of various currencies.
The six outcome indicators used for as pairs for the correlation assessment were:
Life expectancy at birth. This is a widely used indicator estimating the life length of a new born if mortality patterns remain the same all its life (World Bank indicators 2016).
The second outcome indicator was the reduction of life expectancy through death before 65 years. This is also a more general indicator but not very frequently used.
The third outcome indicator was estimated infant mortality/1000 live births. It explores the mortality at a very vulnerable age.
The fourth outcome indicator was maternal deaths/100,000 live births, also a mortality indicator of a vulnerable group.
The fifth outcome indicator was SDR diabetes mellitus, all ages/100,000. It explores the standardized mortality rate for a serious chronic disease with large prevalence and deadly complications.
The sixth outcome indicator was SDR tuberculosis, all ages/100,000, exploring the standardized mortality rate of a mortal infectious disease, with high prevalence in certain countries.
All these outcome indicators are measures of multifactorial processes, comprising activities in the healthcare sector. In case of existing Pearson linear correlation, an assessment of the proportion to which input influenced the outcome was conducted, by calculating r2.
The data used is from the WHO European Health for All database HFA-DB (WHO 2016) from 2011.
This study comprised data from the following East European, Central European, Balkan, and Caucasus countries: Albania, Armenia, Azerbaijan, Belarus, Bosnia and Herzegovina, Bulgaria, Croatia, Cyprus, Czech Republic, Estonia, Georgia, Greece, Hungary, Latvia, Lithuania, FYROM, Moldova, Montenegro, Poland, Romania, Russia, Serbia, Slovakia, Slovenia, Turkey, and Ukraine. Unfortunately the data was not available for all countries and for all indicators, but using Pearson linear correlation analysis, the validity thresholds were clear, and the degree of correlation was obvious.
2.2 Methods
Every input indicator was paired successively with each one of the six outcome indicators, and Pearson linear correlation coefficient (r) was calculated (Triola and Triola 2006a). For the interpretation of the significance of (r), a table with critical values of α was used, for α = 0.05 and for α = 0.01, respectively (Triola and Triola 2006b). In other words, a value of r exceeding the value of α = 0.05 means 95% chance of linear correlation, and a value of r exceeding α = 0.01 means a 99% chance of a linear correlation.
For the data pairs which show a Pearson linear correlation, r2 was also calculated, which is the proportion in variation of one variable which can be attributed to the linear association between the two variables (Triola and Triola 2006c).
2.3 Results
The first input indicator, number of GPs/100,000 population, was paired successively with all the outcome indicators: life expectancy at birth; reduction of life expectancy through death before 65 years; estimated infant mortality/1000 live births; maternal deaths/100,000 live births; SDR diabetes mellitus, all ages/100,000; and SDR tuberculosis, all ages/100,000. Then r was calculated for each pair, and the degree of significance of the Pearson linear correlation coefficient was assessed. This is shown in Table 1.
As we could see, no correlation was found between the number of GPs/100,000 population and the six outcome indicators. An example of no linear correlation is shown in Fig. 1.

The Pearson linear correlation coefficient (0.429) between number of GPs/100,000 population and maternal deaths/100,000 live births
The second input indicator—health expenditure as % of GDP—was paired successively with all the six outcome indicators: life expectancy at birth; reduction of life expectancy through death before 65 years; estimated infant mortality/1000 live births; maternal deaths/100,000 live births; SDR diabetes mellitus, all ages/100,000; and SDR tuberculosis, all ages/100,000. Then r was calculated for each pair, and the degree of significance of the Pearson linear correlation coefficient was assessed. This is shown in Table 2.
This is showing no correlation whatsoever between the health expenditure as % of GDP input indicator and the six outcome indicators: life expectancy at birth; reduction of life expectancy through death before 65 years; estimated infant mortality/1000 live births; maternal deaths/100,000 live births; SDR diabetes mellitus, all ages/100,000; and SDR tuberculosis, all ages/100,000.

The correlations of the third input indicator—total health expenditure in PPP $/capita—with the six outcome indicators are more interesting. Following the same method, it was paired successively with the outcome indicators: life expectancy at birth; reduction of life expectancy through death before 65 years; estimated infant mortality/1000 live births; maternal deaths/100,000 live births; SDR diabetes mellitus, all ages/100,000; and SDR tuberculosis, all ages/100,000. Then r was calculated for each pair, and the degree of significance of the Pearson linear correlation coefficient was assessed. This is shown in Table 3.
We can notice the following results:
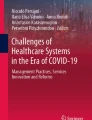
A strong Pearson linear correlation between total health expenditure PPP $/capita and life expectancy at birth. The r value (0.716) exceeds α = 0.01 (0.575). This is shown Fig. 2.

The Pearson linear correlation coefficient (0.716) between total health expenditure PPP $/capita and life expectancy at birth
It is obvious that low expenditure in PPP $ /capita is correlated with low life expectancy at birth, whereas high expenditure in PPP $/capita is correlated with high life expectancy at birth; r2 was 0.51, suggesting that 51% of the variation of the life expectancy at birth can be attributed to the total expenditure on health in PPP $/capita.
The next pair—PPP $/capita and reduction of life expectancy through death before 65 years—shows a negative correlation. Thus r value (−0.574) exceeds α = 0.05 (0.456) and is very close to α = 0.01 (0.575). This shows a negative correlation between the two indicators and is presented in Fig. 3.

The Pearson linear correlation coefficient (−0.574) between total health expenditure PPP $/capita and reduction of life expectancy through death before 65 years
It is obvious that high expenditure in PPP $/capita is correlated with low reduction of life expectancy through death before 65 years, whereas low expenditure in PPP/capita is correlated with high reduction of life expectancy through death before 65 years. r2 was 0.33, suggesting that only 33% of the variation of the reduction of life expectancy through death before 65 years can be attributed to the expenditure in PPP $/capita.
The third pair—PPP $/capita and estimated infant mortality/1000 live births—shows a strong negative Pearson linear correlation between total health expenditure PPP $ $/capita and estimated infant mortality/1000 live births. The r value (−0.621) exceeds α = 0.01 (0.505). This is shown Fig. 4.

The Pearson linear correlation coefficient (−0.621) between total health expenditure PPP $/capita and estimated infant mortality/1000 live births
High expenditure in PPP $/capita is correlated with low estimated infant mortality/1000 live births, whereas low expenditure in PPP $/capita is correlated with high estimated infant mortality/1000 live births. r2 was 0.39, suggesting that only 39% of the variation of the estimated infant mortality/1000 live births can be attributed to the expenditure in PPP $/capita.
The pair—PPP $/capita and maternal deaths/100,000 live births—shows a negative linear correlation. Thus, r value (−0.455) exceeds α = 0.05 (0.396) but does not exceed α = 0.01 (0.505). This shows a negative correlation between the two indicators and is presented in Fig. 5.

The Pearson linear correlation coefficient (−0.454) between total health expenditure in PPP $/capita and maternal deaths/100,000 live births
High expenditure in PPP $/capita is correlated with low maternal deaths/100,000 live births, whereas low expenditure in PPP/capita is correlated with high maternal deaths/100,000 live births; r2 was 0.21, suggesting that only 21% of the variation of the maternal deaths/100,000 live births can be attributed to the expenditure in PPP $/capita.
For the next pair—total health expenditure in PPP $/capita and SDR diabetes mellitus, all ages/100,000—r value (0.074) does not exceed α = 0.05 (0.456). Thus, it shows no correlation.
The last pair —total health expenditure in PPP $/capita and SDR tuberculosis, all ages/100,000—shows a negative correlation. Thus r value (−0.539) exceeds α = 0.05 (0.456), but does not exceed α = 0.01 (0.575). This shows a negative correlation between the two indicators and is presented in Fig. 6.

The Pearson linear correlation coefficient (−0.539) between total health expenditure PPP $/capita and SDR tuberculosis, all ages/100,000
High expenditure in PPP $/capita is correlated with low SDR tuberculosis, all ages/100,000, whereas low expenditure in PPP/capita is correlated with high SDR tuberculosis, all ages/100,000; r2 was 0.29, suggesting that only 29% of the variation of the SDR tuberculosis, all ages/100,000, can be attributed to the expenditure in PPP $/capita.
The fourth input indicator, pharmaceutical expenditure PPP $/capita, was paired successively with all the outcome indicators: life expectancy at birth; reduction of life expectancy through death before 65 years; estimated infant mortality/1000 live births; maternal deaths/100,000 live births; SDR diabetes mellitus, all ages/100,000; and SDR tuberculosis, all ages/100,000. Then r was calculated for each pair, and the degree of significance of the Pearson linear correlation coefficient was assessed. This is shown in Table 4.
No correlation was found between pharmaceutical expenditure PPP $/capita and the six outcome indicators. However for one of them—SDR tuberculosis, all ages/100,000—the degree of correlation is the highest among them pretty close to significance especially with the latter: maternal death/100,000 live births. For this set of indicators, there was not enough data, and the number of pairs was limited; therefore, the significance level of α was very high. This is shown in Fig. 7.

The Pearson linear correlation coefficient (−0.691) between pharmaceutical expenditure PPP $/capita and SDR tuberculosis, all ages/100,000
2.4 Discussion
This study was limited by the availability of data especially about the pharmaceutical expenditure PPP $/capita. Another limitation is a methodological one. It explores only the Pearson linear correlation coefficient and not other types of correlations. Within this type of statistical analysis, one should know that a correlation does not necessarily imply causality. In this case, it is just a hint for further studies.
Firstly, this study showed there was no Pearson linear correlation between the number of GPs/100,000 population and the six outcome indicators: life expectancy at birth; reduction of life expectancy through death before 65 years; estimated infant mortality/1000 live births; maternal deaths/100,000 live births; SDR diabetes mellitus, all ages/100,000; and SDR tuberculosis, all ages/100,000. Several reasons should be looked for in this case. There might be other non-healthcare system-related factors which can influence these indicators. GPs play a lesser role than hospitals in medical activities to which these indicators pertain. There social behaviors, genetics, and poverty are also factors influencing the outcome of services rendered for the treatment of these diseases. These hypotheses need to be explored further. However for maternal death/100,000 live births, the degree of correlation is pretty close to significance: maternal death/100,000 live births; r = 0.429 while α = 0.05 was 0.444. In other words, it is closed to show a conceptual paradox; a higher number of GPs is close to be correlated with a higher number of maternal deaths. This is intriguing and needs to be explored in depth.
Secondly, the study showed no correlation whatsoever between health expenditure as % of GDP and the six outcome indicators: life expectancy at birth; reduction of life expectancy through death before 65 years; estimated infant mortality/1000 live births; maternal deaths/100,000 live births; SDR diabetes mellitus, all ages/100,000; and SDR tuberculosis, all ages/100,000. This suggests that this indicator is not useful in describing the health system but merely in describing the size of the health sector within a country’s economy, the attitude of the public, and the attitude of the government toward the health sector. This is quite stunning considering the exceptional wide use of this indicator. A search of this indicator on the internet on April 16, 2016, returned 494,000 results. This indicator is widely used by many international organizations, governments, statisticians, scholars, industry, and unions. Policies are designed based on this indicator. Many projects and investments are set forth based on this indicator. Yet we could see no correlation with important and also widely used health indicators.
By comparison to the above, the third indicator used—total health expenditure in PPP $/capita—has shown a strong correlation between this indicator and life expectancy at birth and estimated infant mortality/1000 live births, a correlation with reduction of life expectancy through death before 65 years, with maternal deaths/100,000 live births, and with SDR tuberculosis, all ages/100,000. No correlation was found between total health expenditure in PPP $/capita and SDR diabetes mellitus, all ages/100,000. The latter might be explained by the fact that diabetes mellitus is a disease that can’t be cured like TB. Of course, good treatments postpone the death of a patient with diabetes mellitus but never cure the disease. The fact that patients with this disease live longer if the expenditure/capita is higher is supported by the correlation of this input indicator with the other indicators: life expectancy at birth and reduction of life expectancy through death before 65 years.
The fourth input indicator pharmaceutical expenditure in PPP/capita was not correlated with any of the outcome indicators. As said before for this indicator data was scarce, and therefore significance levels were very high.
The fact that only one of the input indicators—total health expenditure in PPP $/capita—has been correlated with outcome indicators raises few questions. Where does this money go, if other input indicators (resources) are not correlated with the outcomes? The answer to this question is that further studies should be made involving other input indicators. Another hypothesis to explain this is that this indicator—total health expenditure in PPP $/capita—does not only show the power of money to buy resources but is an indicator of wealth by itself. Countries with high expenditures/capita are richer than others. It is also well known that poor people are sicker than others; or maybe rich people know better how to preserve their health; or money are used more for prevention than to fight disease. Maybe for the pairs with strong correlations, the other factors contributing to the health outcomes like nutrition or hygiene or stress or pollution are better controlled by rich people. All these hypotheses need further studies to be validated or invalidated. It is to be noted that for pairs of indicators which are correlated, there is a consistency of correlation as it is between life expectancy at birth and reduction of life expectancy through death before 65 years or estimated infant mortality/1000 live births and maternal deaths/100,000 live births. These correlations might also suggest that this indicator can provide a better image about the health system. It is so because in any country, the needs for health services of the population are more or less the same. If less money are available to satisfy those needs, poorer resources will be used, and the health outcomes and performance of the system will be low. The health expenditures depend on two factors: the utilization of services and the price of services. The fact that low/capita expenditures are correlated with bad health outcomes suggests that either the utilization of services is inadequate (impaired access, allocative inefficiency) or human and material resources are underpriced and therefore ineffective or both. Indeed, especially prices of medical technology and drugs do not vary as much as per capita expenditure, and the best technology is not available in case of low expenditures (Sava 2014). It might be the case of technical inefficiency. These results suggest that in using indicators for supporting investment projects and improvement programs, one should be careful that bad outcome indicators are multifactorial, and they can only be addressed properly by taking into consideration all inputs. The mix of inputs and the relationships between them are equally important. One way of assessing this is to look for the correlation between many inputs and the specific outputs, as well as going beyond correlations and look for determinants and causalities.
3 Conclusion
In conclusion we can say that from the financial point of view, total health expenditure per capita is correlated better with the performance of the health sector than total health expenditure as % of GDP. The research shows the importance of using direct financial data than percentage data, which in this study proved to be irrelevant; this input hasn’t been correlated with the outcomes it has been paired with.
The paper tries to shed light on indicators which are really significant from the point of view of students and professionals in public health as well as policymakers.
References
Market House Books Ltd. (1990a). A concise dictionary of business (p. 167). Oxford: Oxford University Press.
Market House Books Ltd. (1990b). A concise dictionary of business (p. 312). Oxford: Oxford University Press.
Sava, D. (2014). The correlation between two financial policy indicators and several outcome indicators, a current perspective on health sciences (pp. 690–700). 1-st Balkan congress on health sciences, Edirne.
Triola, M. M., & Triola, M. F. (2006a). Correlation and regression. In Biostatistics for the biological and health sciences (p. 431). Boston: Pearson Education.
Triola, M. M., & Triola, M. F. (2006b). Correlation and regression. In Biostatistics for the biological and health sciences (p. 640). Boston: Pearson Education.
Triola, M. M., & Triola, M. F. (2006c). Correlation and regression. In Biostatistics for the biological and health sciences (p. 436). Boston: Pearson Education.
WHO. (2016, April). European health for all database. Available at http://data.euro.who.int/hfadb/
World Bank indicators. (2016, April). Available at http://data.worldbank.org/indicator/SP.DYN.LE00.IN
Acknowledgments
The author would like to thank the WHO and European Health for All database for maintaining and providing free access to a valuable database with public health indicators, pertaining to European countries.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2018 Springer International Publishing AG, part of Springer Nature
About this paper

Cite this paper
Sava, D. (2018). The Correlation Between Four Input Indicators and Six Demographic and Output Indicators Within the East European Healthcare Systems. In: Karasavvoglou, A., Goić, S., Polychronidou, P., Delias, P. (eds) Economy, Finance and Business in Southeastern and Central Europe. Springer Proceedings in Business and Economics. Springer, Cham. https://doi.org/10.1007/978-3-319-70377-0_29
Download citation
DOI: https://doi.org/10.1007/978-3-319-70377-0_29
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-70376-3
Online ISBN: 978-3-319-70377-0
eBook Packages: Economics and FinanceEconomics and Finance (R0)