
Abstract
Patient-matched implants were one of the first great applications of 3D printing in medicine (Mankovich et al. 1990; Stoker et al. 1992; Binder and Kaye 1994; Komori et al. 1994). Even preceding the advent of 3D printing, surgeons were using crude, more manually constructed models to aid in design of a patient-matched implant for some of the most complex reconstructive surgeries, surgeries such as for reconstruction of pelvic discontinuity following tumor removal. An anatomical model which clearly displays the deficit one is trying to reconstruct and is a perfect application. Reported benefits for prefabricated implants include surgical time savings, ease of adaptation in surgery, perfected shape or design, and an ability to reconstruct anatomical areas that have no other alternatives from an implant standpoint (Hamid et al. 2016; McAloon 1997; Erickson et al. 1999; Taunton et al. 2012). In many of the initial cases, 3D printing was not used to create the actual implant, but instead it helped to facilitate the design, workflow, or manufacturing of tools used to create these implants. Surgeon adaptation of plates using an anatomical model is also tangentially related to the topic of patient-matched implants. This very “manual” technique for personalizing an implant has been a mainstay of medical modeling since the earliest days (Eppley and Sadove 1998).
Access provided by CONRICYT-eBooks. Download chapter PDF
Similar content being viewed by others


9.1 Background
Patient-matched implants were one of the first great applications of 3D printing in medicine (Mankovich et al. 1990; Stoker et al. 1992; Binder and Kaye 1994; Komori et al. 1994). Even preceding the advent of 3D printing, surgeons were using crude, more manually constructed models to aid in design of a patient-matched implant for some of the most complex reconstructive surgeries, surgeries such as for reconstruction of pelvic discontinuity following tumor removal. An anatomical model which clearly displays the deficit one is trying to reconstruct is a perfect application. Reported benefits for prefabricated implants include surgical time savings, ease of adaptation in surgery, perfected shape or design, and an ability to reconstruct anatomical areas that have no other alternatives from an implant standpoint (Hamid et al. 2016; McAloon 1997; Erickson et al. 1999; Taunton et al. 2012). In many of the initial cases, 3D printing was not used to create the actual implant, but instead it helped to facilitate the design, workflow, or manufacturing of tools used to create these implants. Surgeon adaptation of plates using an anatomical model is also tangentially related to the topic of patient-matched implants. This very “manual” technique for personalizing an implant has been a mainstay of medical modeling since the earliest days (Eppley and Sadove 1998) (Figs. 9.1 and 9.2).

Stereolithography model of a patient with a left mandibular tumor which has eaten away the bone.Surgery will involve removing almost half of the mandible and replacing with a large reconstruction plate and bone graft. Courtesy 3D Systems, Rock Hill, South Carolina, USA

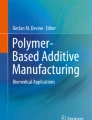
The surgical removal of the left mandible has been simulated and a titanium reconstruction plate has been pre-bent before surgery.Performing the bending before surgery both saves time in surgery and provides for a better aesthetic outcome for the patient. Courtesy 3D Systems, Rock Hill, South Carolina, USA
In the last 5 years, the direct output of implantable parts produced using 3D printing has become more common (Hamid et al. 2016; Di Prima et al. 2016). When 3D printing is directly used for output of a patient-matched implant, it takes advantage of the fact that one-off designs are suited very well to this manufacturing technique. Another benefit of 3D printing is that “complexity is free,” and many times the more complex the design is, the faster and more economical the design is to actually produce (Fig. 9.3). This is a major shift in terms of design thinking, where biomedical engineers and others who have produced implants traditionally using subtractive machining need to reorient and expand their design thinking, which often adds constraints imposed by manufacturing processes.

Patient-matched acetabular cup produced by 3D printing shown during surgical insertion. Courtesy P. James Burn, MD and Paul Morrison, Ossis Ltd., Christchurch, New Zealand
In the 1990s, early uses for patient-matched implants centered around craniomaxillofacial (CMF) applications ; and these are still likely the most prevalent by percentage of total cases in any one anatomical area (Chepelev et al. 2017). Based on the intrinsic complexity of the face and the need for not only functional but aesthetic reconstruction, CMF applications continue to be solid users of patient-matched implant technology (Erickson et al. 1999; Powers et al. 1998; Müller et al. 2003). The technology matured in other areas of the body for large reconstructive surgery cases, many of which were oncology cases (Mulford et al. 2016). Over time, many more applications arose such as limb salvage procedures where complexity is created with defects that are not easily reconstructed with off-the-shelf sizes or shapes of implants. 3D printing is advantageous for the creation of patient-matched implants due to its accurate shape and scale, as well as the ability to print contralateral anatomy to use as a reference for anatomical reconstruction.
Currently, there is a major shift away from patient-matched implants being used solely for the extreme, massive reconstructive surgery cases toward these technologies being used for more “everyday” types of surgical cases. For example, one area that is now largely patient-matched is cranioplasty for repair of large cranial defects. For a defect over a couple of inches in diameter, a very large number of these neurosurgery cases worldwide involve prefabrication of a cranioplasty implant powered by 3D printing technology (Roberson and Rosenberg 1997; Eppley and Sadove 1998). Other even more common areas such as knee replacement are now also beginning to catch on, with patient-matched implant workflows being more commonly offered for partial or total knee arthroplasty (Slamin and Parsley 2012).
9.2 Terminology
From a regulatory standpoint, the terminology used to describe a patient-specific implant is important. Historically, the word “custom” has been used to describe 3D printed implants made for a specific patient using medical image data. However, from the US FDA’s perspective, the term “custom” is closely affiliated with the Custom Device Exemption (FDA 2014), a very specific, defined regulatory path for use of a singular device in the treatment of a singular patient. Such devices have many restrictions, the most major of which is that no other commercially available device is available to treat the patient’s condition. Other major drawbacks to using the Custom Device Exemption for provision of an implant, from a device manufacturer’s standpoint, are related to the fact that there is a strict five units per year limit and that no marketing may be performed, both which severely hinder the ability to provide implants on a widespread basis under the Custom Device Exemption.
The FDA has recommended the use of the terminology “patient-matched” in an effort to make more clear the delineation between devices which go through a rigorous marketing clearance process such as a 510(k) or Premarket Approval (PMA) , patient-matched, and those which are used on more of a one-off basis for a truly unique surgical situation, custom devices (FDA 2016). Patient-matched implants going through the FDA’s traditional regulatory pathways for marketing clearance are much like regular, off-the-shelf-sized implants; however, instead of the FDA clearing the implant size, shape, etc., the FDA is clearing the “system” of design which leads to the final design. The system concept would talk about the inputs such as medical imaging studies and design constraints. The final design must fit into a bounding box that the company determines up front, allowing for testing at the extents of thickness, size, expanse, and material, among other considerations.
9.3 Medical Imaging and Digital Design of Patient-Matched Implants
Modern volumetric medical imaging studies can produce high-quality images that are usable for patient-matched implants. Most implants made for reconstruction of bony anatomy are designed with the aid of preoperative computed tomography (CT) scans. Typical workflows for medical image processing to extract the exact area of anatomy in question are performed by qualified technicians using specialized software tools. When the anatomy in question has been segmented, the workflow can proceed in a number of different ways depending on the patient-matched implant needs. This could look as simple as an anatomical model being 3D printed or as complex as a manufacturing mold being output or even direct output of the implant via 3D printing in a biocompatible material.
Although medical imaging has long been ready to support patient-matched implants, the software tools for digital design of the implants themselves have not always been robust enough for these tasks. It was only following the year 2000 that software tools which would allow for precise manipulation of very organic shapes became available. Many of those tools are still widely used today for implant design, tools such as Geomagic Freeform (3D Systems, Rock Hill, SC). Freeform is somewhat unique in that it combines organic manipulation software with haptic feedback, so the user can actually “feel” the model they are working on in digital space (Fig. 9.4). For many patient-specific implants which are anatomically designed (i.e., meant to mimic the shape of the anatomy they are replacing), this tool has been incredibly powerful. Other design tasks in different industries like the footwear industry also rely heavily on organic modeling software, which can be used to design very complex geometries for things like shoe soles. Digital design is most powerful in designing net-shape (final, perfect design) designs which can be directly built using digital fabrication techniques like 3D printing. In addition, digital design can also be used to design near-net-shape (close to final design) parts for surgeon input, further design, and rough design iterations.

An engineer uses Geomagic Freeform software to design a patient-matched cranioplasty. The tool in his left hand provides force feedback, giving the designer the sensation of “touching” the design he is working on. Courtesy 3D Systems, Rock Hill, South Carolina, USA
This is an exciting time for patient-matched implants from a design software standpoint. In the past, only very “one-off” implants were created with 3D printing, and these were primarily designed by hand, even when a designer would do this work digitally. Today the tools exist to almost totally automate many of these design tasks, taking what has been labor intensive and making it effortless once the system is developed. In addition to saving time and money on labor, other benefits of automation of design include reproducibility and standardization, both of which are much more predictable with automation of design. Watch this space for the coming 5 years to see automation totally change the economics and timeframes and accessibility of truly personalized, patient-matched design.
9.4 How 3D Printing Fits In
There is no single tool or method that fits the needs for all types of patient-matched implants. 3D printing supports the creation of patient-matched implants in a variety of ways including:
-
1.
Anatomical model as a baseline for a design which is performed manually (i.e., with wax or clay)
-
2.
Anatomical model as a template for preparing an off-the shelf implant by hand during or before surgery
-
3.
Different types of models as manufacturing tools following digital design of the implant (molds for forming materials or sacrificial wax patterns)
-
4.
Digital design and 3d printed fabrication of these implants directly in an implantable biomaterial
-
1.
Anatomical Models as Baseline for Manual Design
In this scenario, the anatomical model is 3D printed and is used for the surgeon and engineer to develop an implant design. Many bone reconstructive, implantable devices have been designed in this way, allowing the surgeon to visualize the anatomy clearly in hand and to make needed modifications to the anatomy such as removing bone spurs and existing implants before design of a patient-matched implant (Fig. 9.5). The design of the implant could be as simple as creating a wax pattern of the implant on the model. Later this design could be investment cast into metal, machined by tracer mill, or digitized for computer numerical control (CNC) machining. Historically, without digital design tools, this has been the most common method to create a patient-matched implant; however, given the tools today available for digital design, this method has been surpassed by these more digital techniques.
-
2.
Intraoperative or Immediately Preoperative Bending/Fitting by Surgeons
Many times models or templates are used to create patient-matched implants by the surgeon doing the fabrication using the model and the implant (think of a reconstruction plate being bent). This is also very common for personalizing implant hardware which is fairly straightforward and easy for the surgeon to modify in fitting to the patient’s anatomy.
-
3.
Models as a Manufacturing Tool/Pattern
If implant design is carried out digitally, there will be a need to output that design into physical form. Many methods exist, but the two main methods include (a) the digital design of the implant is produced as a sacrificial pattern for investment casting and (b) the digital design is subtracted from a box and output as a two-part mold for injection molding of the implant.
-
(a)
Sacrificial Pattern 3D Printing of the Implant Design. In this scenario, one could imagine a proximal total knee component being digitally designed with the target material being cobalt-chrome (Co-Cr) alloy. Co-Cr is typically investment cast for these applications using a sacrificial wax pattern invested in plaster. In this case, the digitally designed, patient-matched implant is 3D printed in wax or another investment casting-friendly material. Once printed, the pattern is used in the more traditional workflow for investment casting and subsequent finishing and polishing of the implant.
-
(b)
3D Printing of a Mold for Injection Molding. In this scenario, the implant may be polymeric and in a material that is not yet easy to directly 3D print. The net-shape designed implant would be digitally subtracted from a box, which would then be cut to form a two-part mold, with a cavity inside where the implant would be formed. Sprues and channels can be added to the digital model before being 3D printed in a material conducive to injection molding of the final implant material. Once the mold is 3D printed, the injection molding (i.e., injecting material into the mold to form the shape of the implant) is completed, and the implant is finished, packaged, and readied for use. This method is common for implant materials which are not yet suited for direct 3D printing.
-
(a)
-
4.
Digital Design and 3D Printing of Implants Directly in an Implantable Material
The most direct route to production of a patient-matched implant would be to directly 3D print it in a suitable biomaterial. Today there exist 3D printing techniques to produce implantable parts in various biocompatible metals and plastics. Most common direct metal applications are produced by powder bed fusion techniques (EBM, DMLS, SLM, DMP) in titanium, titanium alloys, and cobalt-chrome alloy. In polymers, most of the implantable work to date has been performed using laser sintering of polyether ether ketone (PEEK) and polyether ketone ketone (PEKK) materials , with others like silicone and polyethylene being researched. 3D printing of titanium and other implant biomaterials has been going on for the last 10+ years with the first FDA clearance for a titanium, 3D printed implant in 2010 (FDA 2010), and the first FDA clearance for a polymeric, 3D printed implant in 2013 (FDA 2013). Regardless of these approvals, many of the patient-matched implants created today are still produced by machining, investment casting, or injection molding versus 3D printing.

A 3D printed trial implant (blue green) on a patient-specific bone model for a patient-matched hip reconstruction case. Courtesy P. James Burn, MD and Paul Morrison, Ossis Ltd., Christchurch, New Zealand
9.5 Patient-Matched Implant Examples
A few examples of patient-matched implants are included below for illustration of the scope of procedures benefitted and general use of 3D printing technology.
-
1.
Facial Augmentation with Silicone Implant . Patients requiring augmentation of soft tissue or bony deformities of the face can benefit from the use of patient-matched silicone implants (Fig. 9.6). These implants may be designed by hand or digitally against the patient-matched bone model.
-
2.
Hemi-Pelvis Reconstruction with 3D Printed Titanium Implant . Oncology patients often require substantial reconstruction following removal of large sections of cancerous tissue. Directly 3D printed titanium alloy implants (EBM, Powder Bed Fusion) combined with fully digital design take advantage of the ability of 3D printing to produce complex, organic shapes. Notice the porous section of the flange, specifically designed for greater muscle adhesion (Fig. 9.7).
-
3.
Revision Hip Arthroplasty . Roughly 15% of all total hip arthroplasty procedures performed annually are revision procedures, with an increasing number of patients on their second or third revision. Each revision removes more of the good, baseline bone that is required for optimal fixation of the acetabular cup. When extensive bone loss is encountered, a patient-matched implant may be an optimal solution, designed for contact with the patient’s anatomy in optimal locations. Direct production by 3D printing in titanium alloy (EBM, Powder Bed Fusion) is accomplished after the implant is digitally designed (Figs. 9.8 and 9.9).
-
4.
Directly 3D Printed Cranioplasty in PEKK . Direct output of implantable polymers with FDA clearance has only been available since 2013. Oxford Performance Materials using their unique PEKK (polyether ketone ketone) biomaterial have paved the way in this area. In this example of a cranioplasty implant, the patient has a large defect in the skull, likely due to trauma or previous surgical intervention (Fig. 9.10). Digital design of the implant is carried out and direct 3D printing of the implant in PEKK biomaterial is performed (Laser Sintering, Powder Bed Fusion).
-
5.
TMJ and Mandibular Reconstruction . One of the early, most common applications for patient-matched implants was in the area of total temporomandibular joint (TMJ) reconstruction (Worford et al. 2015). Many times the implants will be produced traditionally (i.e., CNC machined or formed without 3D printing), but the 3D printed anatomical model will be key to the process of personalizing the design (Fig. 9.11).
-
6.
Machined PEEK Zygoma Implants . Personalized reconstructive facial prostheses like this zygoma plus orbital floor implant are gaining popularity in the plastic surgery and oral and maxillofacial surgical communities. Patients that have had a traumatic injury many times will require some augmentation to the bony structures to again regain their normal appearance. For some of these cases, the globe of the eye may also be in a suboptimal position. Using digital design and machining of PEEK (polyether ether ketone), these implants can be output utilizing a “puzzle-piece” design to allow for optimal stability after implantation (Fig. 9.12).
-
7.
Directly 3D Printed Titanium Mandibular Reconstruction Plate . A fairly common application for digital planning and patient-matched implants are for mandibular reconstruction. In this case, the titanium plate is 3D printed in titanium (Laser Sintering, Powder Bed Fusion) for precise adaptation to the desired shape of the mandible following resection of a portion of the mandible (Fig. 9.13).
-
8.
Patient-Matched Orbital Floor Implant . Many times in facial fracture cases, the patient will suffer an orbital floor “blowout” whereby the thin bone of the floor of the orbit fractures and is displaced into the maxillary sinus, causing the globe to displace inferiorly. A patient-matched implant such as this 3D printed titanium (Laser Sintering, Powder Bed Fusion) implant will be used to perfectly repair the orbital floor while not impinging on other areas that are sensitive, such as the optic nerve (Fig. 9.14).
-
9.
Salvage Ankle Fusion Cage Directly 3D Printed in Titanium (Hamid et al. 2016 ). There are many times that large defects threaten the viability of a limb from a stability and vascularity standpoint. Limb salvage procedures are there to save the limb from the possibility of amputation. In this case, the patient presented with a comminuted fracture of the ankle and was given several options, including amputation of the foot (Fig. 9.15). A patient-matched 3D printed titanium (EBM, Powder Bed Fusion) cage was designed to allow her to keep her foot and to be used in conjunction with adjacent hardware (rod, screws).
-
10.
Distal Humeral Resurfacing Implant Directly 3D Printed in Titanium (Fig. 9.16 ).
-
11.
3D Printed, Bioresorbable Tracheal Splint for Tracheobronchomalacia (Morrison et al. 2015 ). A patient-matched, 3D printed tracheal splint was developed by the University of Michigan to treat young children with a rare condition called tracheobronchomalacia (TBM), a collapse of the airway. The splint is designed from the patient’s CT scan of the airway using Materialise Mimics software and 3D printed out of a bioresorbable material. The intent is the splint will support the bronchus locally preventing airway collapse and will eventually resorb once the patient’s airway has remodeled. The company Materialise and the University of Michigan are partnered to bring this breakthrough device and technology--> through to commercialization (Fig. 9.17).

Silicone genial implant for a patient requiring augmentation of the chin. Courtesy of Implantech Associates, Ventura, California, USA

Hemi-pelvic reconstruction using a patient-matched 3D printed titanium alloy implant. Note areas of the design which are porous for planned adhesion of tissue. Courtesy P. James Burn MD and Paul Morrison, Ossis Ltd., Christchurch, New Zealand

Patient-matched design of a revision acetabular component allows for precise locating of screw trajectory and placement (yellow). Courtesy P. James Burn MD and Paul Morrison, Ossis Ltd., Christchurch, New Zealand

Patient-matched 3D printed titanium implant for a patient requiring revision hip arthroplasty. Courtesy P. James Burn MD and Paul Morrison, Ossis Ltd., Christchurch, New Zealand

Cranioplasty implant 3D printed in PEKK biomaterial for a patient with a large cranial defect. Courtesy Oxford Performance Materials, South Windsor, Connecticut, USA

Patient-matched total temporomandibular joint (TMJ) replacement with temporal extension covering a larger than normal defect. 3D printed model integral to the design and manufacturing process. Courtesy TMJ Concepts, Ventura, California, USA

Machined PEEK implants are produced by milling from a digital design. 3D printed anatomical models form a basis for the design and quality control of these components. Courtesy KLS Martin, Jacksonville, Florida, USA

3D Printed mandibular reconstruction plate (gray) following a resection of the left mandible. Precise screw locations and contour can be achieved by the combination of digital design and digital output. Courtesy KLS Martin, Jacksonville, Florida, USA

A patient-matched orbital floor plate (gray) which has been designed based on the patient’s CT scan and digitally output by 3D printing in titanium. Courtesy KLS Martin, Jacksonville, Florida, USA

(a) and (b) Large 3D printed titanium cage that was packed with bone graft to augment a missing area of anatomy in the lower leg just at the ankle. Courtesy 4WEB Medical, Frisco, Texas, USA

(a) and (b) Distal humeral resurfacing implant produced by 3D printing in titanium with additional titanium nitride coating. Note the porous area for bone ingrowth and the highly polished joint surface area for articulation against the opposing, native bone. Courtesy 4WEB Medical, Frisco, Texas, USA

A patient-matched, 3D printed tracheal splint was developed by the University of Michigan to treat young children with a rare condition called tracheobronchomalacia (TBM) , a collapse of the airway. The splint is designed from the patient’s CT scan of the airway using Materialise Mimics software and 3D printed out of a bioresorbable material. Courtesy Materialise USA, Plymouth, Michigan, USA and University of Michigan, Ann Arbor, Michigan, USA
Some of the examples shown are truly custom devices as discussed earlier when talking about terminology, and some are more commercially available, having gone through a more formal premarket clearance process [510(k) or PMA] with the US FDA.
9.6 Conclusions
Taking a survey today of the entire reconstructive implant industry spanning many specialties, one would find patient-matched implants being used more than ever before with applications spanning the entire body. There is a demonstrated utility for patient-matched implant technology when applying this to very uncommon and special reconstructive surgeries. Over time, though, a multitude of applications which are more common have arisen to make these personalized implants useful to a greater variety of patients. Mostly anecdotal reports of surgical time savings when using patient-matched implants have cemented their use for certain areas such as large oncologic reconstructions. Further study is ongoing to show that personalized implants applied to areas like total knee reconstruction can provide patient benefit in the long term, in addition to aiding the surgeon’s technical job during surgery.
Personalized surgery is a growing topic and will guide further growth and infiltration into many areas where traditionally the “one size fits all” approach has been used. Key to the further widespread adoption of patient-matched technology will be that it is not only better for the patient and the surgeon but also better for the hospital and the payer who is footing the cost. Today when one mentions “patient-matched implants” relative to cost, there is a thought that patient-matched means expensive. Further software automation and better direct implant output via 3D printing will be part of the solution to push the expense for these devices down which will push down their prices. The future is bright for further adoption of patient-matched implant technology in many different areas of the body.
References
Binder WJ, Kaye AH. Three-dimensional computer modeling. Facial Plast Surg Clin North Am. 1994;2:357.
Chepelev L, Giannopoulos A, Tang A, et al. Medical 3D printing: methods to standardize terminology and report trends. 3D Print Med. 2017;3:4. doi:10.1186/s41205-017-0012-5.
Di Prima M, Coburn J, Hwang D, Kelly J, Khairuzzaman A, Ricles L. Additively manufactured medical products – the FDA perspective. 3D Print Med. 2016;2:1. doi:10.1186/s41205-016-0005-9.
Eppley BL, Sadove AM. Computer generated patient models for reconstruction of cranial and facial deformities. J Craniofac Surg. 1998;6:548.
Erickson DM, Chance D, Schmitt S, et al. An opinion survey of reported benefits from the use of stereolithographic models. J Oral Maxillofac Surg. 1999;57:1040.
FDA. Exactech 510(k) K102975 Exactech Novation Crown Cup with InteGrip acetabular shell. November 5, 2010. https://www.accessdata.fda.gov/cdrh_docs/pdf10/K102975.pdf. Accessed 2017 Apr 30.
FDA. Oxford performance materials 510(k) K121818 OsteoFab™ patient-specific cranial device. Feb 7, 2013. https://www.accessdata.fda.gov/cdrh_docs/pdf12/K121818.pdf. Accessed 2017 Apr 30.
FDA. Custom device exemption guidance for industry and FDA staff. Document issued on September 24, 2014. https://www.fda.gov/downloads/medicaldevices/deviceregulationandguidance/guidancedocuments/ucm415799.pdf. Accessed 2017 Apr 30.
FDA. Technical considerations for additive manufactured devices, draft guidance for industry and FDA Staff. May 10, 2016. https://www.fda.gov/downloads/MedicalDevices/DeviceRegulationandGuidance/GuidanceDocuments/UCM499809.pdf. Accessed 2017 Apr 30.
Hamid KS, Parekh SG, Adams SB. Salvage of severe foot and ankle trauma with a 3D printed scaffold. Foot Ankle Int. 2016;37(4):433–9.
Komori T, Takato T, Akagawa T. Use of a laser-hardened three-dimensional replica for simulated surgery. J Oral Maxillofac Surg. 1994;52:516.
Mankovich NJ, Cheeseman AM, Stoker NJ. The display of three-dimensional anatomy with stereolithographic models. J Digit Imaging. 1990;3:200.
McAloon K. Rapid prototyping technology: a unique approach to the diagnosis and planning of medical procedures. Dearborn, MI: The Society of Manufacturing Engineers; 1997.
Morrison RJ, Hollister SJ, Niedner MF, et al. Mitigation of tracheobronchomalacia with 3D-printed personalized medical devices in pediatric patients. Sci Transl Med. 2015;7:285ra64.
Mulford JS, Babazadeh S, Mackay N. Three-dimensional printing in orthopaedic surgery: review of current and future applications. ANZ J Surg. 2016;86(9):648–53.
Müller A, Krishnan KG, Uhl E, Mast G. The application of rapid prototyping techniques in cranial reconstruction and preoperative planning in neurosurgery. J Craniofac Surg. 2003;14:899–914.
Powers DB, Edgin WA, Tabatchnick L. Stereolithography: a historical review and indications for use in the management of trauma. J Craniomaxillofac Trauma. 1998;4:16.
Roberson JB, Rosenberg WS. Traumatic cranial defects reconstructed with the HTR-PMI cranioplastic implant. J Craniomaxillofac Trauma. 1997;3(2):8–13.
Slamin J, Parsley B. Evolution of customization design for total knee arthroplasty. Curr Rev Muscoskelet Med. 2012;5(4):290–5.
Stoker NG, Mankovich NJ, Valentino D. Stereolithographic models for surgical planning. J Oral Maxillofac Surg. 1992;50:466.
Taunton MJ, et al. Pelvic discontinuity treated with custom triflange component: a reliable option. Clin Orthop Relat Res. 2012;470(2):428–34.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2017 Springer International Publishing AG
About this chapter
Cite this chapter
Christensen, A.M. (2017). 3D Printing and Patient-Matched Implants. In: Rybicki, F., Grant, G. (eds) 3D Printing in Medicine. Springer, Cham. https://doi.org/10.1007/978-3-319-61924-8_9
Download citation
DOI: https://doi.org/10.1007/978-3-319-61924-8_9
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-61922-4
Online ISBN: 978-3-319-61924-8
eBook Packages: MedicineMedicine (R0)