
Abstract
Nickel is the most common skin sensitizer, affecting large proportions of the population. Nickel allergy is more prevalent among girls and women than boys and men, owing to differences in exposure patterns. There are large differences in prevalence between age groups, countries and occupations, over time. Skin exposure to nickel in various consumer articles results in nickel allergy and dermatitis on exposed body parts, including the hands. Occupational exposure to nickel is an important cause of occupational skin disease, particularly hand eczema. Nickel allergy has started to decline in some countries owing to the EU restriction of nickel.
Nickel is used in numerous products and materials, and it is difficult to avoid nickel. It is necessary to identify sources of exposure in the workplace, home and leisure environment for exposure reduction and prevention of dermatitis. The dimethylglyoxime (DMG) test is a useful tool. Nickel release can also be quantified by immersion in artificial sweat, and it is now possible to quantify nickel on the skin.
Patients with hand eczema and nickel allergy often have recurrent vesicular hand eczema. Occupational nickel exposure should be considered in nickel-allergic patients with hand eczema. Nickel sulphate 5% is used in the European baseline series. It is safe to use, patch test sensitization has not been reported, and the proportion of irritant and doubtful reactions is low. Patients with nickel allergy and contact dermatitis should be encouraged to use the DMG test to minimize nickel exposure from personal items, in the workplace and during leisure.
Access provided by CONRICYT-eBooks. Download chapter PDF
Similar content being viewed by others


1 Introduction
Nickel is the most common skin sensitizer, affecting large proportions of women, men and children. Nickel allergy is considerably more prevalent among girls and women than boys and men, owing to differences in exposure patterns. Skin exposure to nickel in various consumer articles results in nickel allergy and allergic contact dermatitis on exposed body parts, including the hands. Occupational exposure to nickel is an important cause of occupational skin disease, particularly hand eczema.
Nickel is used in numerous products and materials, many of which come in contact with the skin of consumers and workers. The use of nickel in steels and plating started around 1870, and nickel production has increased considerably since 1940 [1,2,3]. Today, approximately 65% of the nickel produced is used in stainless steels, 20% in other steels and alloys, and 15% in plating and also in chemical compounds (Nickel Institute https://www.nickelinstitute.org/).
Many of the products and materials intended for consumer and occupational use release nickel ions upon skin contact and contaminate the skin. It is thus difficult to avoid skin exposure to nickel in daily life and in the workplace.
2 Prevalence of Nickel Allergy
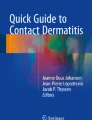
Results from some of the pioneering, largest and most recent studies on the prevalence of nickel allergy among dermatitis patients and the general population in Europe and North America are shown in Tables 32.1 and 32.2. Occupational groups affected by nickel allergy are shown in Table 32.3. There are large differences in the prevalence of nickel allergy between women and men and between age groups, countries and occupations, over time (Fig. 32.1). Most alarming is the persistent and high prevalence of nickel allergy and particularly the much higher prevalence among women compared with men.

Prevalence of nickel allergy among patch-tested dermatitis patients (a–c) and the general population (d–f) in Europe. Examples to display differences between countries, genders and age groups, over time. See also Tables 32.1 and 32.2. References: (a) [6]; (b) [7]; (c) [4]; (d) [15]; (e) [13, 14]; (f) [15,16,17, 19]. Country codes: CH Switzerland, DE Germany, DK Denmark, ES Spain, IT Italy, NL The Netherlands, PL Poland, PT Portugal, SE Sweden, SI Slovenia, UK United Kingdom. Colour codes: red/dots—women or girls, blue/stripes—men or boys, violet—all, pale red or blue—youngest, medium red or blue—middle, dark red or blue—oldest age group
2.1 Dermatitis Patients
Table 32.1 shows that nickel allergy is extremely common among patch-tested adult dermatitis patients (range 12–25%) and three to six times more frequent among women than men. The prevalence of nickel allergy in children is also very high; to what extent stricter selectivity in patch testing children as compared to adults affects the results is not known.
2.2 General Population
There are few large patch test studies among the general population, compared with dermatitis patients. Table 32.2 shows that nickel allergy is extremely common among the general population, adults (range 5–19%) as well as children including adolescents (range 8–10%). Nickel allergy is four to ten times more frequent among women than men among the general population, and the prevalence differs largely also between girls and boys.
2.3 Geographical Differences
Healthcare and social security systems, access to dermatology and selection for patch testing, patch test routines, etc., vary between countries, which contribute to difficulties in comparing the prevalence of nickel allergy between countries. The highest prevalence rates among dermatitis patients in 12 European countries (Table 32.1, Fig. 32.1) were reported for Italy, Poland and Spain (25–26%) and the lowest for Denmark and Germany (12–13%). In North America, the generally used patch test concentration of nickel is 2.5%, half the concentration of that used in the European baseline series. It is likely that this has resulted in some underestimation of nickel allergy among patch-tested patients in North America (Table 32.1).
Likewise, there are large differences between countries in the prevalence of nickel allergy among the general population (Table 32.2 and Fig. 32.1).
2.4 Time Trends
Studies where nickel allergy has been monitored over several years, or reevaluated under similar conditions, show convincingly that nickel allergy has started to decline in some countries. For dermatitis patients in Europe (Table 32.1), a significant decrease in nickel allergy has been noted among younger women (below age 30 or 40) in Denmark, Germany, Italy, Sweden and the UK, and an increase has been noted among women and men above this age in some of the countries (Fig. 32.1) [4, 5]. The reduced prevalence of nickel allergy in the younger age groups has been interpreted to be a result of the EU restriction of nickel and the increase in a cohort effect (see Chap. 5).
Only few studies allowing for trend analysis have been performed among the general population (Table 32.2, Fig. 32.1). A decrease in nickel allergy among the younger women was noted in Denmark between 1990/1991 and 2006; Denmark introduced a nickel restriction in 1991, 10 years before the EU [14].
For dermatitis patients in North America (Table 32.1), a significantly higher prevalence of nickel allergy has been recorded for the period 2013–2014 compared with 2001–2012 [8]. In a systematic review of peer-reviewed publications from the USA in 1961–2015, more than 18,000 adult nickel dermatitis cases were identified [29]. The number of published cases and articles had increased exponentially; suggested explanations for this were previous underdiagnosis and underreporting and increasing nickel exposure and sensitization. There is no nickel regulation in North America, and the North American Contact Dermatitis Group (NACDG) has suggested that regulations restricting release of nickel should be introduced also in North America.
Time trends in nickel exposure are discussed below.
3 Occupational Groups
Occupational nickel exposure is still an important risk factor for nickel allergy and related hand eczema, and certain occupational groups are affected more often than the general population [2, 3, 20]. Examples of occupational groups with a high frequency of nickel allergy are listed in Table 32.3.
More than a hundred years ago, nickel dermatitis was identified as an occupational skin disease among nickel platers. Until the 1930s nickel allergy was predominantly a male occupational disease. Improved industrial hygiene and technical development have decreased the risk, but safety standards vary significantly between workplaces, industries and countries. Outbreaks of nickel allergy are still reported in industrial settings involving platers, metalworkers and electronics industry workers. In such industries, the use of nickel or nickel chemicals is generally obvious and unavoidable (Table 32.3).
Many occupations in the construction industry or involving repair and maintenance work are associated with high exposure to nickel, resulting in occupational nickel allergy and nickel dermatitis (Table 32.3). Car mechanics, electricians, locksmiths, plumbers and other groups are exposed to nickel from intense contact with work materials, tools and other equipment, sometimes in conjunction with exposure to skin irritants.
The prevalence of nickel allergy and hand eczema is high in many occupations in the service and healthcare sectors (Table 32.3). Exposure to nickel in these occupations is often not as obvious as in the other groups. Exposure may be caused by repeated contact of short duration with various commonly occurring items, including coins, handles, keys and utensils (Table 32.4). Exposure to wet work and other irritant factors in many of these occupations impairs the skin barrier function, which facilitates penetration of nickel, sensitization and dermatitis. It has, however, sometimes been questioned whether or not the high rate of nickel allergy in female-dominated occupations such as hairdressing, cleaning and nursing is work related.
Two large studies in the UK in the 1990s assessed occupational contact dermatitis and nickel exposure. In 23% of 368 nickel-allergic patients, nickel was considered to be an occupational or possibly occupational allergen. The main workers were hairdressers, retail clerks, caterers, cleaners and metalworkers. Hand eczema was more prevalent in the occupational than nonoccupational group [21]. National occupational surveillance data was examined, and it was estimated that up to 12% of occupational contact dermatitis cases were associated with nickel exposure. Hairdressers, bar staff and chefs or cooks had the highest incidence rates [22].
Exposure assessments of the work environment are generally required to identify and validate the relevance of occupational nickel exposure (see Chap. 6).
4 Exposure
4.1 Sources of Skin Exposure
It is necessary to identify sources of nickel exposure in the workplace, home and leisure environment for exposure reduction and prevention of dermatitis. The dimethylglyoxime (DMG) test indicates the presence of nickel ions by a pink colour. For decades, it has been the most valuable tool that has been used in dermatology in testing for nickel release. It is used in the clinic, market surveys and workplace studies, and it has been standardized and validated in relation to the limit value (0.5 μg/cm2/week) of the EU nickel restriction [31, 32] (see Chap. 6).
Examples of typical items known to release nickel and cause nickel allergy and dermatitis are given in Table 32.4. Numerous market surveys have been performed with the DMG test and only a few by nickel release in artificial sweat. Most studies have examined jewellery or earrings; others have assessed coins, clothes, electronic devices, tools, toys and other articles. See Chaps. 13, 14, 15, and 16.
4.2 Nickel Release in Artificial Sweat
Nickel release from materials and items is of large interest for risk assessment, and it can be quantified by immersion in artificial sweat according to EN 1811, the reference test method for nickel restriction [33]. The rate (speed) of release of nickel from materials is initially very high and declines rapidly, and samples should preferably be taken at several time points: after minutes, hours, days and a week. The release rate is important for understanding why contact with coins, handles, tools and other items can result in deposition of significant amounts of nickel on the skin [34,35,36].
4.3 Trends in Exposure
Fashion varies over time, and fashion items, including suspenders, ear clips, jeans buttons and piercing jewellery, have been important for widespread nickel sensitization. Technical development in material design and introduction of new types of consumer articles, including electronic devices such as mobile phones, laptops, play stations, activity bracelets and electronic cigarettes, have been highlighted as new sources of nickel exposure and dermatitis among children, consumers and workers (Table 32.4 and Chap. 13).
Three consecutive surveys in Sweden show significant adaptation to the requirements of the Nickel Directive that entered into full force in 2001 (Table 32.4) [37,38,39]. In 1999, 25% of 725 articles were DMG test-positive, in 2002 8%, and in 2010 9% were DMG test-positive. Only 4% of the earrings were DMG test-positive in 1999 and 2010, and 0% in 2002, considerably lower than recorded in other countries (15–31%) [40]. Sweden introduced a restriction on the nickel concentration (0.05%) in piercing posts used during epithelization in 1990, corresponding to former part 1 of the Nickel Directive, and a nationwide information campaign about the Nickel Directive was launched in Sweden in 1999.
Notwithstanding the relatively good compliance to the restriction in Sweden, the prevalence of nickel allergy was high among 16-year-old girls (9.8%) and boys (4.9%) born in 1994–1996 [19]. Sources of exposure other than piercing, jewellery, etc., likely contributed significantly to their sensitization.
4.4 Sharpening of the EU Nickel Restriction
Owing to the slow decrease of nickel allergy in the EU despite the restriction, the European Chemicals Agency (ECHA) was requested to define what should be interpreted as “prolonged contact” in the regulation. In 2014, ECHA published this definition (Table 32.4). ECHA has also been requested to prepare a list of examples of articles covered by the definition, as a guideline. Many of the items in Tables 32.3 and 32.4 should fit the definition.
The most pragmatic approach for manufacturers, retailers and employers, as well as for control of compliance with the regulation, would be that DMG test-positive items should not be used in contact with the skin.
4.5 Skin Exposure Assessment
It is now possible to quantify nickel and other metals deposited onto the skin. Acid wipe sampling, finger rinsing and tape stripping are methods that have been used in occupational, clinical and experimental studies [20, 41,42,43]. It is also possible to visualize nickel on the skin by the DMG test [44]. Skin exposure assessments of nickel and other metals will contribute important information for risk assessment, assessment of occupational dermatitis and prevention efforts (see Chaps. 6 and 28).
4.6 Systemic Exposure
The role of nickel in the diet, surgical implants and dental materials remains partly controversial and is reviewed in Chaps. 17, 19 and 22.
5 Genetic Susceptibility
It is well known that skin exposure to nickel is the main risk factor for sensitization to nickel and nickel dermatitis. It is obvious that also endogenous factors are of importance for sensitization and allergic contact dermatitis. During recent years, efforts have been made to identify genetic factors associated with nickel allergy and nickel dermatitis. Most interest has concerned atopic dermatitis and filaggrin gene mutations.
Several studies have been performed to elucidate associations between genetic factors and nickel allergy or nickel dermatitis. A number of review articles have discussed recent developments [45,46,47,48,49]. Studies have been performed by various methodologies, including population-based studies among families, twins and the general population; studies in patients with atopic dermatitis, hand eczema or nickel allergy; and experimental studies in patients and animals and in vitro studies. To summarize some current positions that may be of particular relevance to clinicians:
-
The prevalence of nickel sensitization is increased in patients with atopic dermatitis.
-
Multiple factors affect the association between atopic dermatitis and skin sensitization.
-
Filaggrin gene mutations increase the risk of atopic dermatitis and likely the risk of sensitization to nickel due to compromised chelation of nickel in the stratum corneum.
-
Filaggrin null mutations have been associated with nickel allergy and self-reported jewellery dermatitis.
-
Some epidemiological filaggrin studies on nickel have been stratified for piercing.
-
Epigenetic regulation likely has a role in nickel dermatitis.
-
Results from epidemiological studies concerning genetic predisposition to nickel allergy have sometimes been conflicting.
-
More studies are needed to determine the role of genetics in the development of nickel allergy and nickel dermatitis.
Ongoing and future research is expected to contribute with further knowledge as to the role of genetic factors in nickel allergy. This may be of high relevance for diagnosis, treatment and prevention.
6 Potency, Cross-Reactivity and Concomitant Reactivity
It is sometimes assumed that nickel is a potent skin sensitizer, as it is a very frequent sensitizer. Based on results from predictive testing in animals by the guinea pig maximization test (GPMT) and the local lymph node assay (LLNA) in mice, however, it has been concluded that nickel is a moderate or weak sensitizer. Negative LLNA results are considered false negative, and mice have been sensitized to nickel by other test methods [50,51,52].
Although the sensitizing potency of nickel is moderate in animal experiments, the dose required for elicitation of nickel dermatitis in humans is very low (see “Dose-Response Studies”).
Concomitant reactivity to nickel and other metals is seen relatively often in dermatitis patients. It is generally difficult to tell if concomitant reactions to commonly occurring skin sensitizers are related to cross-reactivity, co-reactivity or increased susceptibility. Cross-challenge experiments in guinea pigs indicate cross-reactivity for nickel and palladium, but not nickel and cobalt or nickel and chromium [53,54,55].
Patch test results among dermatitis patients and adolescents in the general population have been analysed concerning concomitant and solitary reactivity to nickel, chromium and cobalt [19, 56, 57]. Of particular interest is that cobalt allergy without nickel allergy is relatively frequent, compared with the general assumption that cobalt allergy is coupled to nickel allergy owing to assumed concomitant exposure or cross-reactivity. It should also be noted that cobalt often is used in other forms and products than nickel (see Chap. 28).
7 Clinical Picture
Skin lesions in nickel-allergic persons may be transient or more persistent, localized to skin contact with certain items, to the hands, or more widespread. When localized to the skin under jewellery, buttons, a belt buckle, spectacle frames, a wristwatch and other personal items, it may be relatively easy to identify and avoid the causative exposure. It may, however, be difficult to identify the exposure(s) causing or contributing to hand eczema.
Historically, jewellery, suspenders, hooks, zippers and buttons in clothes and spectacle frames have often been reported to cause the first noted lesion (primary eruption). During recent decades, when ear and body piercing has been increasingly popular, dermatitis from jewellery for pierced holes has been common. The picture is dependent on fashion, which varies, and to the properties of the materials used, i.e. nickel release.
Nickel-allergic individuals run an increased risk of developing hand eczema [3]. Approximately 30–40% of nickel-allergic individuals report that they ever have experienced hand eczema, compared with 15–20% among non-nickel-allergic individuals [12, 58, 59]. Patients with hand eczema and nickel allergy often have recurrent vesicular hand eczema [60]. Occupational nickel exposure should be considered in nickel-allergic patients with hand eczema. In some countries, the association between nickel allergy and hand eczema in young women may have weakened (see “Severity and Prognosis”).
Systemic exposure to nickel by ingestion, implants and dental materials is reviewed in Chaps. 17, 19 and 22.
7.1 Severity and Prognosis
Many mild cases of nickel dermatitis will clear with avoidance of nickel exposure and with topical treatment. Hand eczema in nickel-sensitive patients has often been considered to have a poor prognosis and may in some cases be resistant to treatment and persist for years [2, 3, 61].
Severe hand eczema occurs in nickel-allergic patients, particularly in work-related cases when the exposure may be massive or difficult to avoid, and when combined with exposure to wet work and other skin irritants that impair the skin barrier function. Other well-known factors that contribute to severe symptoms or poor prognosis of nickel allergy are multiple sensitization and a history of atopic dermatitis [3, 47, 62].
Some studies among the general population indicate that the prognosis of nickel allergy has become more favourable. The association has weakened between nickel allergy and hand eczema among young women in Denmark, although not among older women, following the Danish nickel restriction of 1991 [63]. In a 20-year follow-up of patch-tested schoolgirls in Sweden, the prognosis of hand eczema in relation to nickel allergy was more favourable than previously reported [64]. The participants had, however, been patch tested with nickel and informed about any nickel allergy in the first study, and it is unknown if they had avoided nickel exposure since then.
8 Diagnosis and Prevention in the Clinic
8.1 Patch Test
Nickel sulphate 5% (2.0 mg/cm2) in petrolatum is used in the European baseline series, while 2.5% (1.0 mg/cm2) is used in the North American series [8, 65]. The ready-to-use patch test system TRUE Test® contains a nickel patch (0.20 mg/cm2). Active patch test sensitization from nickel sulphate 5% in petrolatum has not been reported. The proportion of irritant and doubtful patch test reactions to nickel is low, compared with that to cobalt, chromium and most other baseline patch test substances [57, 66, 67]. Poor reproducibility of patch test reactions to nickel among infants has been reported [68] (see Chap. 37).
Patch testing with serial dilutions of nickel is performed to assess an individual’s degree of sensitivity or to confirm that a reaction is allergic. Patch testing with metal discs of various nickel-containing materials gives information about the ability of materials to cause allergic contact dermatitis (Chap. 6) [69,70,71]. Such testing is sometimes used when patients are evaluated in relation to implants (see Chap. 24).
8.2 Dose-Response Studies
Compilations of dose-response results give important information on elicitation thresholds [72]. Dose-response studies have been performed with serial dilutions of nickel by patch testing and repeated open application testing (ROAT) [73]. The patch test dose to which 10% of nickel-allergic individuals reacted (ED10) was 0.78 μg nickel/cm2. The reactivity to the accumulated dose per unit area by ROAT was similar to that by patch test. Knowledge about elicitation thresholds is important for understanding that low doses of nickel are able to cause allergic contact dermatitis by prolonged contact and that nickel deposited onto the skin by short and repeated contact likewise is able to cause allergic contact dermatitis. See further Chap. 6 concerning measured levels of skin exposure to nickel in various occupations.
8.3 DMG Test
The DMG test presents a cheap, simple and powerful tool for prevention of nickel dermatitis by exposure reduction. All patients with nickel allergy and contact dermatitis should be encouraged to use the DMG test to minimize nickel exposure from personal items, in the workplace and during leisure. It may be necessary for the patient to get support by the occupational health service, safety representative or employer to reduce exposure in the workplace.
8.4 Exposure Assessment
In the case of suspected work-related nickel allergy, it may be of high importance to make a thorough assessment of the patient’s exposure to nickel, other skin sensitizers and skin irritants. This is essential for diagnosis, rehabilitation and medicolegal purposes [65]. The assessment should preferably include a systematic investigation with the DMG test to identify sources of nickel exposure in the workplace. Nickel on the skin should also be assessed qualitatively by the DMG test or quantitatively if chemical analysis is available (see “Exposure” and Chap. 6).
References
Flint GN. A metallurgical approach to metal contact dermatitis. Contact Dermatitis. 1998;39:213–21.
Lidén C. Nickel. In: Rustemeyer T, Elsner P, John SM, Maibach HI, editors. Kanerva’s occupational dermatology. 2nd ed. Berlin/Heidelberg: Springer; 2012. p. 485–94. (chapter 43).
Lidén C, Bruze M, Thyssen JP, Menné T. Metals. In: Johansen JD, Frosch P, Lepoittevin J-P, editors. Contact dermatitis. 5th ed. Berlin: Springer; 2011. p. 643–80.
Garg S, Thyssen JP, Uter W, Schnuch A, Johansen JD, Menné T, Belloni Fortina A, Statham B, Gawkrodger DJ. Nickel allergy following European Union regulation in Denmark, Germany, Italy and the U.K. Br J Dermatol. 2013;169:854–8.
Fall S, Bruze M, Isaksson M, Lidén C, Matura M, Stenberg B, Lindberg M. Contact allergy trends in Sweden - a retrospective comparison of patch test data from 1992, 2000, and 2009. Contact Dermatitis. 2015;72:297–304.
Uter W, Gefeller O, Gimenez-Arnau A, Frosch P, Johansen JD, Schuttelaar ML, Rustemeyer T, Filon FL, Dugonik A, Bircher A, Wilkinson M. Characteristics of patients patch tested in the European Surveillance System on Contact Allergies (ESSCA) network, 2009-2012. Contact Dermatitis. 2015;73:82–90.
Uter W, Filon FL, Rui F, Balato A, Wilkinson M, Ecisz BK, Chomiczewska-Skora D, Kiec-Swierczynska M, Schuttelaar MLA, Frosch PJ, Bircher AJ. ESSCA results with nickel, cobalt and chromium, 2009-2012. Contact Dermatitis. 2016;75:117–U186.
DeKoven JG, Warshaw EM, Belsito DV, Sasseville D, Maibach HI, Taylor JS, Marks JG, Fowler JF Jr, Mathias CG, DeLeo VA, Pratt MD, Zirwas MJ, Zug KA. North American Contact Dermatitis Group patch test results: 2013–2014. Dermatitis. 2016;28:33–46.
Simonsen AB, Deleuran M, Mortz CG, Johansen JD, Sommerlund M. Allergic contact dermatitis in Danish children referred for patch testing - a nationwide multicentre study. Contact Dermatitis. 2014;70:104–11.
Fortina AB, Cooper SM, Spiewak R, Fontana E, Schnuch A, Uter W. Patch test results in children and adolescents across Europe. Analysis of the ESSCA Network 2002-2010. Pediatr Allergy Immunol. 2015;26:446–55.
Zug KA, Pham AK, Belsito DV, DeKoven JG, DeLeo VA, Fowler JF, Fransway AF, Maibach HI, Marks JG, Mathias CGT, Pratt MD, Sasseville D, Storrs FJ, Taylor JS, Warshaw EM, Zirwas MJ. Patch testing in children from 2005 to 2012: Results from the North American Contact Dermatitis Group. Dermatitis. 2014;25:345–55.
Peltonen L. Nickel sensitivity in the general population. Contact Dermatitis. 1979;5:27–32.
Nielsen NH, Menné T. Allergic contact sensitization in an unselected Danish population. The Glostrup Allergy Study, Denmark. Acta Derm Venereol. 1992;72:456–60.
Thyssen JP, Linneberg A, Menné T, Nielsen NH, Johansen JD. Contact allergy to allergens of the TRUE-test (panels 1 and 2) has decreased modestly in the general population. Br J Dermatol. 2009;161:1124–9.
Diepgen TL, Ofenloch RF, Bruze M, Bertuccio P, Cazzaniga S, Coenraads PJ, Elsner P, Goncalo M, Svensson A, Naldi L. Prevalence of contact allergy in the general population in different European regions. Br J Dermatol. 2016;174:319–29.
Mortz CG, Lauritsen JM, Bindslev-Jensen C, Andersen KE. Prevalence of atopic dermatitis, asthma, allergic rhinitis, and hand and contact dermatitis in adolescents. The odense adolescence cohort study on atopic diseases and dermatitis. Br J Dermatol. 2001;144:523–32.
Fors R, Persson M, Bergström E, Stenlund H, Stymne B, Stenberg B. Nickel allergy–prevalence in a population of Swedish youths from patch test and questionnaire data. Contact Dermatitis. 2008;58:80–7.
Krecisz B, Chomiczewska D, Palczynski C, Kiec-Swierczynska M. Contact allergy to metals in adolescents. Nickel release from metal accessories 7 years after the implementation of the EU Nickel Directive in Poland. Contact Dermatitis. 2012;67:270–6.
Lagrelius M, Wahlgren CF, Matura M, Kull I, Lidén C. High prevalence of contact allergy in adolescence: results from the population-based BAMSE birth cohort. Contact Dermatitis. 2016;74:44–51.
Gawkrodger DJ, McLeod CW, Dobson K. Nickel skin levels in different occupations and an estimate of the threshold for reacting to a single open application of nickel in nickel-allergic subjects. Br J Dermatol. 2012;166:82–7.
Shah M, Lewis FM, Gawkrodger DJ. Nickel as an occupational allergen - a survey of 368 nickel-sensitive subjects. Arch Dermatol. 1998;134:1231–6.
Shum KW, Meyer JD, Chen Y, Cherry N, Gawkrodger DJ. Occupational contact dermatitis to nickel: experience of the British dermatologists (EPIDERM) and occupational physicians (OPRA) surveillance schemes. Occup Environ Med. 2003;60:954–7.
Richardson C, Hamann CR, Hamann D, Thyssen JP. Mobile phone dermatitis in children and adults: a review of the literature. Pediatr Allergy Immunol Pulmonol. 2014;27:60–9.
Thyssen JP, Gawkrodger DJ, White IR, Julander A, Menné T, Lidén C. Coin exposure may cause allergic nickel dermatitis: a review. Contact Dermatitis. 2013;68:3–14.
Jensen P, Hamann D, Hamann CR, Jellesen MS, Jacob SE, Thyssen JP. Nickel and cobalt release from children’s toys purchased in Denmark and the United States. Dermatitis. 2014;25:356–65.
Kickinger-Lorsch A, Bruckner T, Mahler V. Nickel and cobalt release from metal alloys of tools-a current analysis in Germany. Contact Dermatitis. 2015;73:289–95.
Lidén C, Röndell E, Skare L, Nalbanti A. Nickel release from tools on the Swedish market. Contact Dermatitis. 1998;39:127–31.
Ringborg E, Lidén C, Julander A. Nickel on the market: a baseline survey of articles in ‘prolonged contact’ with skin. Contact Dermatitis. 2016;75:77–81.
Goldenberg A, Vassantachart J, Lin EJ, Lampel HP, Jacob SE. Nickel allergy in adults in the U.S.: 1962 to 2015. Dermatitis. 2015;26:216–23.
Thyssen JP, Menné T, Johansen JD. Identification of metallic items that caused nickel dermatitis in Danish patients. Contact Dermatitis. 2010;63:151–6.
CEN. Screening tests for nickel release from alloys and coatings in items that come into direct and prolonged contact with the skin. CEN/CR 12471:2002. European Committee for Standardisation; 2002.
Thyssen JP, Skare L, Lundgren L, Menné T, Johansen JD, Maibach HI, Lidén C. Sensitivity and specificity of the nickel spot (dimethylglyoxime) test. Contact Dermatitis. 2010;62:279–88.
CEN. Reference test method for release of nickel from all post assemblies which are inserted into pierced parts of the human body and articles intended to come into direct and prolonged contact with the skin. EN 1811:2011+A1:2015. European Committee for Standardisation; 2015.
Erfani B, Lidén C, Midander K. Short and frequent skin contact with nickel. Contact Dermatitis. 2015;73:222–30.
Julander A, Midander K, Herting G, Thyssen JP, White IR, Odnevall Wallinder I, Lidén C. New UK nickel-plated steel coins constitute an increased allergy and eczema risk. Contact Dermatitis. 2013;68:323–30.
Lidén C, Carter S. Nickel release from coins. Contact Dermatitis. 2001;44:160–5.
Biesterbos J, Yazar K, Lidén C. Nickel on the Swedish market: follow-up 10 years after entry into force of the EU Nickel Directive. Contact Dermatitis. 2010;63:333–9.
Lidén C, Johnsson S. Nickel on the Swedish market before the Nickel Directive. Contact Dermatitis. 2001;44:7–12.
Lidén C, Norberg K. Nickel on the Swedish market. Follow-up after implementation of the Nickel Directive. Contact Dermatitis. 2005;52:29–35.
Thyssen JP, Menné T, Lidén C, White IR, White J, Spiewak R, Johansen JD. Excessive nickel release from earrings purchased from independent shops and street markets–a field study from Warsaw and London. J Eur Acad Dermatol Venereol. 2011;25:1021–6.
Jensen P, Thyssen JP, Johansen JD, Skare L, Menné T, Lidén C. Occupational hand eczema caused by nickel and evaluated by quantitative exposure assessment. Contact Dermatitis. 2011;64:32–6.
Julander A, Boman A, Johanson G, Lidén C Occupational skin exposure to chemicals. With focus on skin exposure assessment, skin sensitisation and prevention by exposure reduction. The Nordic Expert Group for Criteria Documentation of Health Risks from Chemicals. Arbete och Hälsa (in press). 2017.
Lidén C, Skare L, Nise G, Vahter M. Deposition of nickel, chromium, and cobalt on the skin in some occupations - assessment by acid wipe sampling. Contact Dermatitis. 2008;58:347–54.
Julander A, Skare L, Vahter M, Lidén C. Nickel deposited on the skin-visualization by DMG test. Contact Dermatitis. 2011;64:151–7.
Friedmann PS, Sanchez-Elsner T, Schnuch A. Genetic factors in susceptibility to contact sensitivity. Contact Dermatitis. 2015;72:263–74.
Martin SF. New concepts in cutaneous allergy. Contact Dermatitis. 2015;72:2–10.
Schram SE, Warshaw EM, Laumann A. Nickel hypersensitivity: a clinical review and call to action. Int J Dermatol. 2010;49:115–25.
Thyssen JP, Menné T. Metal allergy--A review on exposures, penetration, genetics, prevalence, and clinical implications. Chem Res Toxicol. 2010;23:309–18.
Thyssen JP, McFadden JP, Kimber I. The multiple factors affecting the association between atopic dermatitis and contact sensitization. Allergy. 2014;69:28–36.
Basketter DA, Scholes EW, Kimber I. The performance of the local lymph-node assay with chemicals identified as contact allergens in the human maximization test. Food Chem Toxicol. 1994;32:543–7.
Vennegaard MT, Dyring-Andersen B, Skov L, Nielsen MM, Schmidt JD, Bzorek M, Poulsen SS, Thomsen AR, Woetmann A, Thyssen JP, Johansen JD, Odum N, Menné T, Geisler C, Bonefeld CM. Epicutaneous exposure to nickel induces nickel allergy in mice via a MyD88-dependent and interleukin-1-dependent pathway. Contact Dermatitis. 2014;71:224–32.
Wahlberg JE. Nickel: Animal sensitization assays. In: Maibach HI, Menné T, editors. Nickel and the skin: immunology and toxicology. Boca Raton: CRC Press; 1989.
Lidén C, Wahlberg JE. Cross-reactivity to metal compounds studied in guinea pigs induced with chromate or cobalt. Acta Derm Venereol. 1994;74:341–3.
Wahlberg JE, Boman AS. Cross-reactivity to palladium and nickel studied in the guinea-pig. Acta Derm Venereol. 1992;72:95–7.
Wahlberg JE, Lidén C. Cross-reactivity patterns of cobalt and nickel studied with repeated open applications (ROATS) to the skin of guinea pigs. Am J Contact Dermat. 2000;11:42–8.
Hegewald J, Uter W, Pfahlberg A, Geier J, Schnuch A. A multifactorial analysis of concurrent patch-test reactions to nickel, cobalt, and chromate. Allergy. 2005;60:372–8.
Lidén C, Andersson N, Julander A, Matura M. Cobalt allergy: suitable test concentration, and concomitant reactivity to nickel and chromium. Contact Dermatitis. 2016;74:360–7.
Meding B, Lidén C, Berglind N. Self-diagnosed dermatitis in adults - Results from a population survey in Stockholm. Contact Dermatitis. 2001;45:341–5.
Menné T, Borgan O, Green A. Nickel allergy and hand dermatitis in a stratified sample of the Danish female population: an epidemiological study including a statistic appendix. Acta Derm Venereol. 1982;62:35–41.
Boonstra MB, Christoffers WA, Coenraads PJ, Schuttelaar MLA. Patch test results of hand eczema patients: relation to clinical types. J Eur Acad Dermatol Venereol. 2015;29:940–7.
Fregert S. Occupational dermatitis in a 10-year material. Contact Dermatitis. 1975;1:96–107.
Hald M, Agner T, Blands J, Ravn H, Johansen JD. Allergens associated with severe symptoms of hand eczema and a poor prognosis. Contact Dermatitis. 2009;61:101–8.
Thyssen JP, Linneberg A, Menné T, Nielsen NH, Johansen JD. The association between hand eczema and nickel allergy has weakened among young women in the general population following the Danish nickel regulation: results from two cross-sectional studies. Contact Dermatitis. 2009;61:342–8.
Josefson A, Färm G, Magnuson A, Meding B. Nickel allergy as risk factor for hand eczema: a population-based study. Br J Dermatol. 2009;160:828–34.
Johansen JD, Aalto-Korte K, Agner T, Andersen KE, Bircher A, Bruze M, Cannavo A, Gimenez-Arnau A, Goncalo M, Goossens A, John SM, Lidén C, Lindberg M, Mahler V, Matura M, Rustemeyer T, Serup J, Spiewak R, Thyssen JP, Vigan M, White IR, Wilkinson M, Uter W. European Society of Contact Dermatitis guideline for diagnostic patch testing - recommendations on best practice. Contact Dermatitis. 2015;73:195–221.
Geier J, Uter W, Lessmann H, Schnuch A. The positivity ratio--another parameter to assess the diagnostic quality of a patch test preparation. Contact Dermatitis. 2003;48:280–2.
Warshaw EM, Nelsen DD, Sasseville D, Belsito DV, Maibach HI, Zug KA, Fowler JF Jr, Taylor JS, DeLeo VA, Marks JG Jr, Storrs FJ, Mathias CG, Pratt MD, Rietschel RL. Positivity ratio and reaction index: patch-test quality-control metrics applied to the north american contact dermatitis group database. Dermatitis. 2010;21:91–7.
Mortz CG, Kjaer HF, Eller E, Osterballe M, Norberg LA, Host A, Bindslev-Jensen C, Andersen KE. Positive nickel patch tests in infants are of low clinical relevance and rarely reproducible. Pediatr Allergy Immunol. 2013;24:84–7.
Haudrechy P, Mantout B, Frappaz A, Rousseau D, Chabeau G, Faure M, Claudy A. Nickel release from stainless steels. Contact Dermatitis. 1997;37:113–7.
Lidén C, Menné T, Burrows D. Nickel-containing alloys and platings and their ability to cause dermatitis. Br J Dermatol. 1996;134:193–8.
Menné T, Brandup F, Thestrup-Pedersen K, Veien NK, Andersen JR, Yding F, Valeur G. Patch test reactivity to nickel alloys. Contact Dermatitis. 1987;16:255–9.
Fischer LA, Menné T, Voelund A, Johansen JD. Can exposure limitations for well-known contact allergens be simplified? An analysis of dose-response patch test data. Contact Dermatitis. 2011;64:337–42.
Fischer LA, Johansen JD, Menné T. Nickel allergy: relationship between patch test and repeated open application test thresholds. Br J Dermatol. 2007;157:723–9.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2018 Springer International Publishing AG, part of Springer Nature
About this chapter

Cite this chapter
Lidén, C. (2018). Metal Allergy: Nickel. In: Chen, J., Thyssen, J. (eds) Metal Allergy. Springer, Cham. https://doi.org/10.1007/978-3-319-58503-1_32
Download citation
DOI: https://doi.org/10.1007/978-3-319-58503-1_32
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-58502-4
Online ISBN: 978-3-319-58503-1
eBook Packages: MedicineMedicine (R0)