
Abstract
Allergic contact dermatitis to chromium (Cr) is one of the most common and most severe metal allergies. Chromium-sensitized persons need to strictly avoid contact with chromium, which is a difficult task due to its main sources being nonmetals and non-labeled occupational or everyday life products. Regulations, work hygiene, and the decrease of hexavalent chromium sources can be effective measures to reduce the prevalence of allergic contact dermatitis. There are no inexpensive and simple analytical tools available that can detect released chromium with sufficient sensitivity to detect potential sources that should be avoided. Hexavalent chromium has significantly higher skin and cell penetration rates compared with trivalent chromium. Hexavalent chromium is therefore generally considered the more potent allergen compared with trivalent chromium. Anionic trivalent chromium species have the highest skin penetration rates among trivalent chromium species. The chromium release chemistry from potential sources, the chromium oxidation state and chemical form, skin penetration, and skin reactions depend all largely on pH and the presence of complexing and reducing species. Therefore, some environments and sources, especially alkaline ones, should be particularly avoided. A trivalent chromium-protein conjugate is the recognized antigen by cutaneous dendritic cells. Patch testing with potassium dichromate is the main diagnostic tool, but causes a relatively high percentage of irritant or doubtful reactions. Hypersensitivity to chromium released from metallic implants is rarer compared with allergic contact dermatitis. Allergic asthma to chromium has been reported for a few occupations.
Access provided by CONRICYT-eBooks. Download chapter PDF
Similar content being viewed by others


1 Prevalence of Allergy and Epidemiology
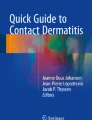
Chromium (Cr) has traditionally been the third most common metal allergen (after nickel and cobalt) [1, 2], but ranges from the first to the fifth most common metal allergen in different occupations and countries (Fig. 27.1). Its prevalence varies largely among different groups and countries and over time, closely related to occupations, exposure, different regulations, and work hygiene. Figure 27.1 shows the large variation in the percentage of positive patch test reactions among adults to potassium dichromate (0.25% or 0.5% in petrolatum) found in different studies after the year 2000. Studies on the prevalence of allergic Cr contact dermatitis before the year 2000 have been summarized in [3] and in [4].

Prevalence of Cr sensitization obtained through patch testing with 0.25% or 0.5% potassium dichromate (in petrolatum) in occupational (blue-collar workers), clinical (e.g., patients suspected to have contact dermatitis), and general population groups in different countries. The study country/region and number of tested persons in each study are noted above the bars, and the years during which the patch testing was conducted (two last numbers of the year only) can be found below the bars and reference letters—A [14], B [2], C [15], D [16], E [17], F [18], G [19], H [20], I [21], J [22], K [23], L [24], M [25], N [26], O [27], P [1], Q [28], R [29], S [30], T [31], U [32], V [33], W [34], X [35], Y [36]. Note that there are differences in patch testing, readings, statistical analysis, etc., among the studies. The reader is referred to the respective study for exact numbers and study details
Generally, prevalence of allergic Cr contact dermatitis is lower in North America and Western Europe compared with Eastern Europe and Asian countries (Fig. 27.1). This corresponds with a long-term decrease in allergic Cr contact dermatitis in Western Europe and North America, and a stagnant or increasing trend in Asia [4], and is believed mainly to be related to differences in exposure sources, occupations, and regulatory measures. Differences in referral patterns and false positive or false negative readings could be other possible explanations.
Generally, prevalence of allergic Cr contact dermatitis increases with age [4]. Although contact dermatitis to Cr is usually less common in children compared to adults, it remains an important contact allergen [5,6,7,8] and, in some studies and countries (e.g., Italy, Switzerland, India), represents one of the most common contact allergens for children [5].
Traditionally, allergic Cr contact dermatitis has been mostly found in men due to the high prevalence in construction workers [4]. This has, however, recently changed in many countries due to regulatory measures to limit the soluble hexavalent Cr (CrVI) content in cement in some countries, first implemented in Denmark in 1981 [4, 9, 10]. Other important regulations are the recently implemented restriction of CrVI released from leather [11] and the general attempt by industry and regulators to replace CrVI in processes and products, e.g., for electronic equipment [12] and chemicals [13].
2 Relevant Chromium Chemistry
Trivalent Cr (CrIII) is the hapten that is bound to a carrier (a protein), forming a conjugate (antigen) which causes Cr sensitization and elicitation [37, 38]. Both trivalent and hexavalent Cr species can be stable in aqueous solutions depending on the pH and solution redox potential [39, 40]. Figure 27.2 gives some examples of important trivalent and hexavalent Cr species in aqueous solutions such as patch test solutions. Generally, CrVI species cannot form cations and do not easily bind to organic species and proteins (unless they are first reduced to CrIII) [41, 42]. This, in addition to their negative charge (at neutral and alkaline pH), has been suggested to be the reason for their relatively high skin penetration [42,43,44]. CrIII, in contrast, forms a vast number of different cationic, anionic, and neutral charged species in aqueous solutions and binds easily to abundant blood and skin proteins [42, 45,46,47], but has a low skin penetration and is reported to be rejected by the skin [44].

Some examples of relevant cationic, anionic, and neutral hexavalent (top) and trivalent (bottom) Cr species in aqueous solutions of relevance for patch test solutions and clinical and laboratory studies. Species were analyzed for several patch test solutions (13% CrCl3 and 0.5% potassium dichromate in water) and for the most common leather tanning agent CrSO4OH in water, using the Medusa software [50], and drawn by the ChemSketch software (ACD/Labs Freeware 2012)
Metallic Cr, Cr0, is neither stable in air nor water due to its high oxygen affinity, and it rapidly forms a trivalent Cr oxide. This surface oxide or passive film is important for all corrosion-resistant Cr alloys such as stainless steel, Inconel (a common Ni-Cr alloy), and cobalt-chromium alloys (e.g., used for dental implants and artificial joint prostheses). This surface oxide of noncorroding Cr alloys and metal is very stable. It cannot be seen by the naked eye, because it is very thin (e.g., 2–5 nm in water or air) [48, 49].
3 Skin Deposition
The skin deposition of Cr from different items is not necessarily similar to the amount and chemical form that is released from these items in different simulants, such as artificial sweat. There are two major reasons: (1) most skin contact includes wear processes which are often not considered in laboratory testing, such as in artificial sweat according to the EN 1811 standard [51], and (2) the chemical reactions in skin contact are thin-film reactions and not necessarily comparable to bulk solution conditions [49,50,51,52]. It has been shown that the skin deposition on the index finger after touching different metal and alloy surfaces is higher compared with the amount released into artificial sweat [53]. Skin deposition of Cr from different items and in certain occupations has been investigated using acid wipe sampling [54,55,56] and wipe sampling [57]. The recovery of Cr was between 90% and 102% [58] in acid wipe sampling, however, not tested for CrVI, which is not possible to distinguish from CrIII using this technique. The skin deposition of Cr has been found to be larger for Cr-tanned leather compared with Cr-containing metal discs [54], which is in accordance with release data (see Use and Sources of Exposure below). It has been highlighted in these studies that even brief skin contact results in significant amounts of deposited metals. This is also true for release processes in bulk solutions, which mostly take place in the first seconds to minutes for passive metals [49, 59] and Cr-tanned leather [60]. With both metals [53] and Cr-tanned leather [61], it was found that surfaces previously stored in air can release more metals compared with previously touched [53] or immersed [61] surfaces. Unpublished results of Cr skin deposition from leather bracelets suggest that Cr is deposited from Cr-tanned leather bracelets (Y. Hedberg, B. Erfani, M. Matura, C. Lidén, unpublished data).
4 Skin Penetration
Penetration of Cr through human skin is governed by (1) pH, (2) Cr concentration, and (3) chemical speciation of Cr, as well as biological factors such as the skin barrier (Table 27.1). Since the Cr chemical speciation (Fig. 27.2) is governed by the solution pH, solution composition, and Cr concentration, systematic studies comparing the skin penetration of different Cr compounds are difficult to conduct and interpret. Table 27.1 summarizes several skin penetration studies, with a focus on the comparison of different Cr compounds and solution pH values. Since CrVI species are generally more soluble at alkaline pH, and CrIII species at acidic pH, they cannot be compared directly without affecting their solubility and ionic charge. It is, however, clear from Table 27.1 and [62] that anionic species of both CrVI and CrIII penetrate the skin to a larger extent compared with cationic or neutral species. The solution pH affects not only the Cr speciation (which Cr species exist) but also the skin permeability [43] and skin charge [42]. At alkaline pH, both the skin membrane and CrVI species are negatively charged (CrIII species are not soluble at this pH), which results in electrostatic repulsion and hence no binding. The consequence of the equal skin membrane and CrVI species charge, as well as the higher skin permeability to water, is that CrVI species at alkaline pH show the highest Cr skin penetration compared with CrIII species and acidic pH.
5 Immunology
In order to be a sensitizer, Cr must bind to a protein (a carrier) to form an antigen [66, 67]. It is now generally accepted that the antigen is a CrIII-protein conjugate and that any CrVI first needs to be reduced before it binds to a protein [37, 38, 41]. The fact that CrVI is a stronger sensitizer compared to CrIII (Tables 27.2 and 27.3), even if skin penetration is excluded (e.g., by intra-/subdermal injection or in in vitro assays), may be explained by (1) the strong binding of CrIII to proteins compared with CrVI and (2) the ability of CrVI to penetrate the cell membrane and bind to proteins after reduction inside the cell [37, 38, 68]. It has been suggested that Cr (and metal cations in general) changes protein structure upon binding and that this structurally modified protein is processed and presented to T cells by cutaneous dendritic cells (Langerhans cells) [67] (sensitization step) or recognized by circulating hapten-specific T cells (elicitation step) [66, 67, 69, 70]. Activation of human monocyte-derived dendritic cells through direct ligation with human Toll-like receptor (TLR)-4, shown to be important for nickel, palladium, and cobalt, has not been found to be important for Cr [71]. It is well known that CrIII can modify protein structure, or even strongly aggregate proteins, such as normally pure serum albumin [45,46,47, 72]. Whether this structural modification or any other reaction is responsible for the antigenic properties is unclear. Several CrIII-protein conjugates have been identified that are able to be recognized as antigen by Cr-sensitized persons (investigated by different methods), in decreasing order: human serum albumin [73,74,75,76], heparin [75, 76], hyaluronic acid from human umbilical cord [76], undefined skin proteins [73], and γ-globulin [74, 75].
Generally, due to the strong effect of skin penetration (for all Cr species) and protein binding (in the case of CrIII only), allergic responses are greater for sub- or intracutaneous testing relative to epicutaneous testing, as well as irritated or stripped skin relative to intact skin (Table 27.2). Furthermore, skin penetration largely determines the wide variation among the different Cr solutions summarized in Table 27.2. However, for anionic CrIII solutions, such as CrIII-oxalate, the difference from CrVI solutions is smaller (Table 27.2). Several minimum elicitation threshold values for CrIII and CrVI are summarized in Table 27.3, and other studies are summarized in [77]. These were obtained via occluded patch testing, and it has been argued that more realistic methods such as repeated open application tests (ROAT), where the test solution is applied for brief discontinuous periods on non-occluded skin, are needed. ROAT tests have been conducted for aqueous potassium dichromate solutions, where comparable threshold values were obtained as in occluded patch tests [78, 79].
Concomitant reactivity to other haptens may occur, possibly due to cross-reactivity or co-sensitization. For example, concomitant reactivity to Cr and Co has been observed [80]. A recent study on 656 consecutive dermatitis patients, of which 200 patients reacted positively to either Co, Cr, or Ni, demonstrated that reactivity to each of these metals can either exist independently or for one or several more metals, suggesting co-sensitization rather than cross-reactivity to be the reason behind concomitant reactivity [81].
6 Use and Sources of Exposure
Cr is used or present in a large variety of articles, products, and alloys. In contrast to other metal allergens, the most important sources of skin exposure, both occupationally and environmentally, are nonmetals: Cr-containing cement, Cr-tanned leather [86, 91], and different fluids and chemicals, such as detergents and bleaching chemicals [92]. Table 27.4 summarizes amounts of released CrIII and CrVI from different sources into select environments. Generally, the release of Cr from noncorroding metals and alloys is significantly lower compared with Cr-tanned leather (Table 27.4). The release of Cr from noncorroding metals is not proportional to their Cr content, which is also illustrated in Table 27.4. Corroding metals and alloys can, however, release a significant amount of CrIII. Corroding metals and alloys without any chromate-containing coatings can only release significant amounts of CrVI if a high voltage is applied (Table 27.4), which does not occur in ambient environments, skin contact, or the human body, but might be important in certain manufacturing processes, electrical applications, or implants that make use of high pulsed voltage. Chromate coatings have been used as anti-fingerprint coating on metal surfaces during transport and storage, such as roof sheets, screws, and other metal products [93]. These coating types can result in CrVI release upon skin contact when a product is new or has been stored at dry conditions, and they are increasingly replaced by manufacturers with alternative coatings [93]. Cr-releasing particles include welding fume from Cr-containing alloys and cement particles (Table 27.4). Since ultrafine particles can be inhaled and reach the alveolar region in the lung [94], special protection is required. Certain combinations of exposure factors and source chemistry should also be avoided. These include for Cr-tanned leather (Table 27.4): (1) alkaline fluids such as wet cement contact or detergents, (2) dry storage in low humidity followed by wet skin exposure, and (3) frequent skin contact with Cr-tanned leather that was not treated with antioxidants.
Cr can also be released from Cr-containing alloys (nearly all implant materials that require wear and corrosion resistance) inside the human body, such as from different stainless steel and cobalt-chromium-alloy dental or artificial joint prostheses. The released form is ionic CrIII or wear particles including Cr0 or CrIII in the form of Cr2O3 [95, 96].
Other sources vary largely among countries and occupations and depend on prevailing safety procedures, technologies, and regulations. Industrial/professional use includes chromate containing anticorrosion inhibitors or coatings, catalysts (CrIII based and converted to other oxidation states during the process), electroplating (CrO3) and anodization agents, pigments (green Cr2O3, decreasingly yellow/orange chromates) for the production of glass or ceramics, chromates in paints, mordant dyes of textiles, CrVI-containing wood preservatives that are converted to CrIII during the process, CrVI-containing oxidative bleaching chemicals, and wet cement [4, 97, 98].
Green pigments in cosmetics and tattoo ink (Cr2O3); Cr-containing ash, e.g., due to combustion of Cr-tanned leather and preserved wood; and dry/wet cement are examples of other sources that are not necessarily an occupational exposure [4, 70, 92, 97, 98]. A more detailed summary of different sources, including older technology and processes, can be found in [4].
7 Clinical Manifestations
7.1 Contact Dermatitis
Contact dermatitis to Cr is often located on the hands and feet [86, 113]. Cr dermatitis is associated with greater severity of hand eczema [114], a lower quality of life [115], and higher prevalence of sick leave [115], compared to other dermatitis patients. Cr contact dermatitis is very persistent [116, 117] and has a poor prognosis [113,114,115, 118,119,120]. It has been suggested that this might be due to the multitude of different Cr sources and/or an ability of Cr to remain absorbed in the skin [116, 117]. However, it has been shown that strict allergen avoidance, mainly by a change of workplace or early retirement, resulted in the improvement of 72% of Cr contact dermatitis patients’ symptoms within a few years [121]. Systemic contact dermatitis is not very common and of minor importance, except in the setting of a high oral intake of CrVI [97] and CrIII food supplements [122].
7.2 Hypersensitivity to Implant Materials and Their Wear Debris
In regard to the general prevalence of metal contact dermatitis, nickel and cobalt are more commonly reported to cause hypersensitivity reactions compared with Cr [123]. However, Cr is an alloying element in many biomedical metallic implant materials and might be released in nano-sized wear particles [95] or as ionic species (CrIII) [96]. Cr ions or Cr-containing wear debris released from implant materials can cause cutaneous allergic reactions [123,124,125], peri-implant inflammation [123, 126], and other reactions [127]. Large aggregates of Langerhans cells have been found in the lymph nodes of a patient with high cobalt and Cr serum ion levels [124], suggesting a type IV (cell-mediated) reaction. Complications for patients with articulating implants, especially knee arthroplasty, are associated with a higher rate of metal sensitization [123]. It is, however, unclear whether the metal sensitization caused complications or vice versa [123]. Symptomatic relief and/or disappearance of associated eczema has been reported after replacement of the implant, but the role of metal allergy is still not clear for several other complicating conditions (e.g., persistent pain, aseptic loosening, pseudotumors) [123]. Two studies concluded that the overall risk of knee arthroplasty failure is not increased due to metal hypersensitivity [128, 129]. It was also shown (in 52 patients) that, despite higher serum ion levels as compared to metal-on-polymer implants, having cobalt- and Cr-releasing metal-on-metal hip implants did not increase the prevalence of Cr or cobalt contact dermatitis after a 5-year follow-up [130]. This was confirmed in a Danish registry-based study, where it was, however, found that the prevalence of cobalt and Cr contact dermatitis was increased for patients having two or more episodes of revision surgery [131].
7.3 Allergic Asthma
Asthma is a common disease worldwide, with a physician-diagnosed prevalence rate of 4.3%, ranging from 0.19% (China) to 21% (Australia) [132]. Its prevalence is not declining [133]. The incidence of allergic asthma is approximately equal to that of non-allergic asthma, but dependent upon age [134]. Cr-induced allergic asthma has been reported relatively scarcely [135] for some occupations, such as welding, electroplating/metal plating, and cement work [136,137,138,139]. It has been suggested that the metal sensitivity involved in allergic asthma may be IgE mediated without a clear association with allergic contact dermatitis to the same metal [135, 138, 140] or may be IgE mediated in some cases, but not in others [136, 139]. Thus, there is some evidence for both delayed and immediate types of allergic asthma to Cr.
8 Patch Testing, Spot Testing, and Other Testings
For patch testing, potassium dichromate 0.5% in petrolatum (e.g., baseline series for Europe) or 0.25% in petrolatum (e.g., North America) is most often used [97]. These CrVI patch test allergens can cause irritant reactions that are sometimes difficult to distinguish from allergic reactions without retesting. However, lower concentrations of CrVI, shorter patch test durations than 48 h, or the use of CrIII salts may instead result in a large percentage of false negatives (Tables 27.2 and 27.3) [90]. A recent study found that Cr was associated with a significantly higher percentage of potentially irritant reactions for at least one patch test reading (day 3 or days 6–7 after the start of patch test placement for 48 h), in comparison to cobalt and nickel [81]. It seems, therefore, particularly important that two readings be conducted when patch testing to Cr [81]. Of note, the number of irritant reactions for Cr patch testing increased with lower temperature and lower humidity [141], probably related to an impaired skin barrier under these conditions. For children, the same patch test concentration as for adults (0.5% potassium dichromate in petrolatum) was recommended, if there was a history of reactions to shoe allergens [142]. In addition to patch testing, less commonly used tests are immersion tests [143] and repeated open application or prolonged tests [79, 91].
In order to identify potential sources of Cr in a simple and inexpensive way, CrVI spot testing using diphenylcarbazide (DPC) has been suggested and conducted [4, 144, 145]. The test is, however, more challenging to interpret and conduct correctly, as compared to other spot tests such as for nickel and cobalt. This is due to its specificity to CrVI, relatively high detection limit of 0.5 mg/L CrVI [145], and the potential loss of specificity to CrVI upon oxidation in air, facilitated by illumination [146]. CrVI is easily reduced to CrIII on many surfaces, including leather and metal surfaces, at a sufficiently high relative humidity in air [61, 93, 109]. The DPC spot test can hence miss CrVI that has been reduced to CrIII, but may be oxidized again on leather surfaces when the relative humidity is low [61, 109]. The DPC spot test may furthermore miss lower CrVI concentrations and all CrIII, which are also able to cause positive reactions (Tables 27.2 and 27.3). Despite these limitations, the DPC spot test might be a reasonable initial rapid screening tool, and contact with items that test positive should be avoided for a Cr-sensitive person.
Currently, other tests cannot be performed as easily and inexpensively. X-ray fluorescence can detect the total Cr content of a product, but does not give information on its potential Cr release, which often differs (Table 27.4). Release tests can be very relevant and should ideally be able to distinguish between CrIII and CrVI (speciation testing). Candidates for speciation testing are the DPC test by means of spectrophotometry (UV-vis), testing by means of stripping voltammetry (polarography), and distinction by chromatography techniques, before/in conjunction with analytical techniques for total Cr such as atomic absorption spectroscopy and inductively coupled plasma spectroscopy [147]. The DPC spectrophotometry test is used both in standard CrVI testing in cement [148] and in leather [149]. More details on the testing of CrVI in leather can be found in Chap. 4.
References
Warshaw EM, Maibach HI, Taylor JS, Sasseville D, DeKoven JG, Zirwas MJ, et al. North American contact dermatitis group patch test results: 2011–2012. Dermatitis. 2015;26(1):49–59.
Uter W, Larese Filon F, Rui F, Balato A, Wilkinson M, Kręcisz B, et al. ESSCA results with nickel, cobalt and chromium, 2009–2012. Contact Dermatitis. 2016;75(2):117–21. doi:10.1111/cod.12582.
Proctor DM, Fredrick MM, Scott PK, Paustenbach DJ, Finley BL. The prevalence of chromium allergy in the United States and its implications for setting soil cleanup: a cost-effectiveness case study. Regul Toxicol Pharmacol. 1998;28(1):27–37.
Bregnbak D, Johansen JD, Jellesen MS, Zachariae C, Menné T, Thyssen JP. Chromium allergy and dermatitis: prevalence and main findings. Contact Dermatitis. 2015;73(5):261–80. doi:10.1111/cod.12436.
Zug KA, Pham AK, Belsito DV, DeKoven JG, DeLeo VA, Fowler JF Jr, et al. Patch testing in children from 2005 to 2012: results from the North American contact dermatitis group. Dermatitis. 2014;25(6):345–55.
Simonsen AB, Deleuran M, Mortz CG, Johansen JD, Sommerlund M. Allergic contact dermatitis in Danish children referred for patch testing–a nationwide multicentre study. Contact Dermatitis. 2014;70:104–11.
Lagrelius M, Wahlgren C-F, Matura M, Kull I, Lidén C. High prevalence of contact allergy in adolescence: results from the population-based BAMSE birth cohort. Contact Dermatitis. 2016;74(1):44–51.
Belloni Fortina A, Cooper SM, Spiewak R, Fontana E, Schnuch A, Uter W. Patch test results in children and adolescents across Europe. Analysis of the ESSCA network 2002–2010. Pediatr Allergy Immunol. 2015;26(5):446–55.
Stocks SJ, McNamee R, Turner S, Carder M, Agius RM. Has European Union legislation to reduce exposure to chromate in cement been effective in reducing the incidence of allergic contact dermatitis attributed to chromate in the UK? Occup Environ Med. 2012;69(2):150–2. doi:10.1136/oemed-2011-100220.
Uter W, Rühl R, Pfahlberg A, Geier J, Schnuch A, Gefeller O. Contact allergy in construction workers: results of a multifactorial analysis. Ann Occup Hyg. 2004;48(1):21–7.
Thyssen JP, Menné T, Johansen JD. Hexavalent chromium in leather is now regulated in European Union member states to limit chromium allergy and dermatitis. Contact Dermatitis. 2014;70(1):1–2. doi:10.1111/cod.12182.
Directive 2011/65/EU of the European Parlaiment and of the Council of 8 June 2011 on the restriction of the use of certain hazardous substances in electrical and electronic equipment (recast). 2011.
REACH - Registration, Evaluation, Authorisation and Restriction of Chemicals. 2007.
Schwensen JF, Menné T, Veien NK, Funding AT, Avnstorp C, Østerballe M, et al. Occupational contact dermatitis in blue-collar workers: results from a multicentre study from the Danish contact dermatitis group (2003–2012). Contact Dermatitis. 2014;71(6):348–55.
Fall S, Bruze M, Isaksson M, Lidén C, Matura M, Stenberg B, et al. Contact allergy trends in Sweden – a retrospective comparison of patch test data from 1992, 2000, and 2009. Contact Dermatitis. 2015;72(5):297–304. doi:10.1111/cod.12346.
Mahler V, Geier J, Schnuch A. Current trends in patch testing–new data from the German contact dermatitis research group (DKG) and the information network of departments of dermatology (IVDK). J Dtsch Dermatol Ges. 2014;12(7):583–92.
Fida M, Topi G, Qirko E, Kellici S, Shehu E, Dervishi O, et al. The use of patch testing for the diagnosis of contact dermatitis: an Albanian experience. J Health Sci. 2015;5(2):65–71.
Machovcová A, Dastychová E, Kostalova D, Vojtechovska A, Reslova J, Smejkalova D, et al. Common contact sensitizers in the Czech Republic. Patch test results in 12,058 patients with suspected contact dermatitis. Contact Dermatitis. 2005;53(3):162–6.
Tichy M, Karlova I. Allergic contact dermatitis and changes in the frequency of the causative allergens demonstrated with patch testing in 2008-2012. Biomed Pap Med Fac Univ Palacky Olomouc Czech Repub. 2015;159(3):480–8.
Reduta T, Bacharewicz J, Pawłoś A. Patch test results in patients with allergic contact dermatitis in the Podlasie region. Postepy Dermatol Alergol. 2013;30:350–7.
Beliauskiene A, Valiukeviciene S, Uter W, Schnuch A. The European baseline series in Lithuania: results of patch testing in consecutive adult patients. J Eur Acad Dermatol Venereol. 2011;25(1):59–63.
Rui F, Bovenzi M, Prodi A, Belloni Fortina A, Romano I, Corradin MT, et al. Nickel, chromium and cobalt sensitization in a patch test population in north-eastern Italy (1996–2010). Contact Dermatitis. 2013;68(1):23–31.
García-Gavín J, Armario-Hita J, Fernández-Redondo V, Fernández-Vozmediano J, Sánchez-Pérez J, Silvestre J, et al. Epidemiology of contact dermatitis in Spain. Results of the Spanish surveillance system on contact allergies for the year 2008. Actas Dermosifiliogr. 2011;102(2):98–105.
Aguilar-Bernier M, Bernal-Ruiz A, Rivas-Ruiz F, Fernández-Morano M, de Troya-Martín M. Contact sensitization to allergens in the Spanish standard series at hospital costa del sol in Marbella, Spain: a retrospective study (2005–2010). Actas Dermosifiliogr. 2012;103(3):223–8.
Bordel-Gómez MT, Miranda-Romero A, Castrodeza-Sanz J. Isolated and concurrent prevalence of sensitization to transition metals in a Spanish population. J Eur Acad Dermatol Venereol. 2008;22(12):1452–7.
Kridin K, Bergman R, Khamaisi M, Weltfriend S. Chromate allergy in northern Israel in relation to exposure to cement and detergents. Dermatitis. 2016;27(3):131–6.
Ertam I, Turkmen M, Alper S. Patch-test results of an academic Department in Izmir, Turkey. Dermatitis. 2008;19(4):213–5.
Wentworth AB, Yiannias JA, Keeling JH, Hall MR, Camilleri MJ, Drage LA, et al. Trends in patch-test results and allergen changes in the standard series: A Mayo Clinic 5-year retrospective review (January 1, 2006, to December 31, 2010). J Am Acad Dermatol. 2014;70(2):269–75.e4. doi:10.1016/j.jaad.2013.09.047.
Toholka R, Wang YS, Tate B, Tam M, Cahill J, Palmer A, et al. The first Australian baseline series: recommendations for patch testing in suspected contact dermatitis. Aust J Dermatol. 2015;56(2):107–15.
Boonchai W, Iamtharachai P. Risk factors for common contact allergens and patch test results using a modified European baseline series in patients tested during between 2000 and 2009 at Siriraj Hospital. Asian Pac J Allergy Immunol. 2014;32(1):60.
Goon AT, Goh C. Metal allergy in Singapore. Contact Dermatitis. 2005;52(3):130–2.
Bajaj A, Saraswat A, Mukhija G, Rastogi S, Yadav S. Patch testing experience with 1000 patients. Indian J Dermatol Venereol Leprol. 2007;73(5):313.
Yin R, Huang XY, Zhou XF, Hao F. A retrospective study of patch tests in Chongqing, China from 2004 to 2009. Contact Dermatitis. 2011;65(1):28–33.
Dou X, Zhao Y, Ni C, Zhu X, Liu L. Prevalence of contact allergy at a dermatology clinic in China from 1990-2009. Dermatitis. 2011;22(6):324–31.
Bilcha KD, Ayele A, Shibeshi D, Lovell C. Patch testing and contact allergens in Ethiopia–results of 514 contact dermatitis patients using the European baseline series. Contact Dermatitis. 2010;63(3):140–5.
Diepgen T, Ofenloch R, Bruze M, Bertuccio P, Cazzaniga S, Coenraads PJ, et al. Prevalence of contact allergy in the general population in different European regions. Br J Dermatol. 2016;174(2):319–29.
Siegenthaler U, Laine A, Polak L. Studies on contact sensitivity to chromium in the guinea pig. The role of valence in the formation of the antigenic determinant. J Invest Dermatol. 1983;80(1):44–7.
Polak L, Frey JR. Studies on contact hypersensitivity to chromium in the Guinea pig. Int Arch Allergy Appl Immunol. 1973;44(1):51–61.
Shupack SI. The chemistry of chromium and some resulting analytical problems. Environ Health Perspect. 1991;92:7.
Rollinson CL. The chemistry of chromium, molybdenum, and tungsten. Oxford: Robert Maxwell, M.C.; 1975.
Samitz M, Katz S. A study of the chemical reactions between chromium and skin. J Invest Dermatol. 1964;43(1):35–42.
Mali JWH, Van Kooten WJ, Van Neer FCJ. Some aspects of the behavior of chromium compounds in the skin. J Invest Dermatol. 1963;41(3):111–22. doi:10.1038/jid.1963.83.
Gammelgaard B, Fullerton A, Avnstorp C, Menné T. Permeation of chromium salts through human skin in vitro. Contact Dermatitis. 1992;27(5):302–10.
Van Lierde V, Chéry CC, Roche N, Monstrey S, Moens L, Vanhaecke F. In vitro permeation of chromium species through porcine and human skin as determined by capillary electrophoresis-inductively coupled plasma-sector field mass spectrometry. Anal Bioanal Chem. 2006;384(2):378–84.
Yang J, Black J. Competitive binding of chromium, cobalt and nickel to serum proteins. Biomaterials. 1994;15(4):262–8. doi:10.1016/0142-9612(94)90049-3.
Hedberg YS, Pettersson M, Pradhan S, Odnevall Wallinder I, Rutland MW, Persson C. Can cobalt(II) and chromium(III) ions released from joint prostheses influence the friction coefficient? ACS Biomater Sci Eng. 2015;1(8):617–20. doi:10.1021/acsbiomaterials.5b00183.
Österberg R, Sjöberg B, Persson D. Cr (III)-induced polymerization of human albumin. Biol Trace Elem Res. 1981;3(3):157–67.
Lundin M, Hedberg Y, Jiang T, Herting G, Wang X, Thormann E, et al. Adsorption and protein-induced metal release from chromium metal and stainless steel. J Colloid Interface Sci. 2012;366:155–64.
Hedberg YS, Odnevall Wallinder I. Metal release from stainless steel in biological environments: a review. Biointerphases. 2016;11(1):018901-1–17. doi:10.1116/1.4934628.
Puigdomenech I. Hydra/Medusa chemical equilibrium database and plotting software. KTH Royal Institute of Technology. 2015. https://www.kth.se/polopoly_fs/1.369371!/Eq-Calcs_32.zip.
CEN. Reference test method for release of nickel from all post assemblies which are inserted into pierced parts of the human body and articles intended to come into direct and prolonged contact with the skin, EN-1811:2011. 2011.
Leygraf C, Wallinder IO, Tidblad J, Graedel T. Atmospheric corrosion. Hoboken: Wiley; 2016.
Erfani B, Lidén C, Midander K. Short and frequent skin contact with nickel. Contact Dermatitis. 2015;73(4):222–30. doi:10.1111/cod.12426.
Bregnbak D, Thyssen JP, Jellesen MS, Zachariae C, Johansen JD. Experimental skin deposition of chromium on the hands following handling of samples of leather and metal. Contact Dermatitis. 2016;75(2):89–95. doi:10.1111/cod.12605.
Julander A, Skare L, Mulder M, Grander M, Vahter M, Lidén C. Skin deposition of nickel, cobalt, and chromium in production of gas turbines and space propulsion components. Ann Occup Hyg. 2010;54(3):340–50. doi:10.1093/annhyg/meq002.
Lidén C, Skare L, Nise G, Vahter M. Deposition of nickel, chromium, and cobalt on the skin in some occupations - assessment by acid wipe sampling. Contact Dermatitis. 2008;58(6):347–54. doi:10.1111/j.1600-0536.2008.01326.x.
Day GA, Virji MA, Stefaniak AB. Characterization of exposures among cemented tungsten carbide workers. Part II: assessment of surface contamination and skin exposures to cobalt, chromium and nickel. J Expo Sci Environ Epidemiol. 2009;19(4):423–34.
Lidén C, Skare L, Lind B, Nise G, Vahter M. Assessment of skin exposure to nickel, chromium and cobalt by acid wipe sampling and ICP-MS. Contact Dermatitis. 2006;54(5):233–8.
Hedberg Y, Midander K. Size matters: mechanism of metal release from 316L stainless steel particles is governed by size-dependent properties of the surface oxide. Mater Lett. 2014;122:223–6. doi:10.1016/j.matlet.2014.02.034.
Hedberg Y, Lidén C, Odnevall Wallinder I. Chromium released from leather – I: exposure conditions that govern the release of chromium(III) and chromium(VI). Contact Dermatitis. 2015;72(4):206–15. doi:10.1111/cod.12329.
Hedberg YS, Lidén C. Chromium(III) and chromium(VI) release from leather during 8 months simulated use. Contact Dermatitis. 2016;75(2):82–8. doi:10.1111/cod.12581.
Samitz M, Katz S, Shrager JD. Studies of the diffusion of chromium compounds through skin. J Invest Dermatol. 1967;48(6):514–20.
Wahlberg J. Percutaneous absorption from chromium (51Cr) solutions of different pH, 1.4–12.8. Dermatology. 1968;137(1):17–25.
Spruit D, van Neer FCJ. Penetration rate of Cr (III) and Cr (VI). Dermatology. 1966;132(2):179–82.
Lidén S, Lundberg E. Penetration of chromium in intact human skin in vivo. J Invest Dermatol. 1979;72(1):42–5. doi:10.1111/1523-1747.ep12530184.
Lepoittevin J-P. Molecular aspects in allergic and irritant contact dermatitis. In:Contact dermatitis. Berlin: Springer; 2011. p. 91–110.
Saint-Mezard P, Rosieres A, Krasteva M, Berard F, Dubois B, Kaiserlian D, et al. Allergic contact dermatitis. Eur J Dermatol. 2004;14(5):284–95.
Rytter M, Haustein UF. Hapten conjugation in the leukocyte migration inhibition test in allergic chromate eczema. Br J Dermatol. 1982;106(2):161–8. doi:10.1111/j.1365-2133.1982.tb00925.x.
Sinigaglia F. The molecular basis of metal recognition by T cells. J Invest Dermatol. 1994;102(4):398–401. doi:10.1111/1523-1747.ep12372149.
Forte G, Petrucci F, Bocca B. Metal allergens of growing significance: epidemiology, immunotoxicology, strategies for testing and prevention. Inflamm Allergy Drug Targets. 2008;7(3):145–62. doi:10.2174/187152808785748146.
Rachmawati D, Bontkes HJ, Verstege MI, Muris J, von Blomberg BME, Scheper RJ, et al. Transition metal sensing by toll-like receptor-4: next to nickel, cobalt and palladium are potent human dendritic cell stimulators. Contact Dermatitis. 2013;68(6):331–8.
Friedberg F. Effects of metal binding on protein structure. Q Rev Biophys. 1974;7(01):1–33. doi:10.1017/S0033583500001335.
Thulin H, Zachariae H. The leucocyte migration test in chromium hypersensitivity. J Invest Dermatol. 1972;58(2):55–8. doi:10.1111/1523-1747.ep12551476.
Cohen HA. Carrier specificity of tuberculin-type reaction to trivalent chromium. Arch Dermatol. 1966;93(1):34–40.
Cohen HA. Tuberculin-type reaction to heparin-chromium complex: heparin—a specific carrier of chromium sensitivity. Arch Dermatol. 1966;94(4):409–12. doi:10.1001/archderm.1966.01600280027005.
Cohen HA. Hyaluronic acid: a specific carrier of chromium sensitivity. Arch Dermatol. 1968;98(2):148–51. doi:10.1001/archderm.1968.01610140046010.
Hansen MB, Rydin S, Menné T, Johansen JD. Quantitative aspects of contact allergy to chromium and exposure to chrome-tanned leather. Contact Dermatitis. 2002;47(3):127–34.
Basketter D, Horev L, Slodovnik D, Merimes S, Trattner A, Ingber A. Investigation of the threshold for allergic reactivity to chromium. Contact Dermatitis. 2001;44(2):70–4. doi:10.1034/j.1600-0536.2001.440202.x.
Nielsen N, Kristiansen J, Borg L, Christensen J, Poulsen L, Menne T. Repeated exposures to cobalt or chromate on the hands of patients with hand eczema and contact allergy to that metal. Contact Dermatitis. 2000;43(4):212–5.
Albert MR, Chang Y, González E. Concomitant positive reactions to allergens in a patch testing standard series from 1988-1997. Dermatitis. 1999;10(4):219–23.
Lidén C, Andersson N, Julander A, Matura M. Cobalt allergy: suitable test concentration, and concomitant reactivity to nickel and chromium. Contact Dermatitis. 2016;74(6):360–7. doi:10.1111/cod.12568.
Samitz M, Shrager J. Patch test reactions to hexavalent and trivalent chromium compounds. Arch Dermatol. 1966;94(3):304–6.
Fregert S, Rorsman H. Allergy to trivalent chromium. Arch Dermatol. 1964;90(1):4.
Fregert S, Rorsman H. Allergic reactions to trivalent chromium compounds. Arch Dermatol. 1966;93(6):711–3.
Hansen MB, Johansen JD, Menné T. Chromium allergy: significance of both Cr(III) and Cr(VI). Contact Dermatitis. 2003;49(4):206–12. doi:10.1111/j.0105-1873.2003.0230.x.
Hansen MB, Menné T, Johansen JD. Cr(III) reactivity and foot dermatitis in Cr(VI) positive patients. Contact Dermatitis. 2006;54(3):140–4. doi:10.1111/j.0105-1873.2006.00802.x.
Allenby C, Goodwin B. Influence of detergent washing powders on minimal eliciting patch test concentrations of nickel and chromium. Contact Dermatitis. 1983;9(6):491–9.
Fregert S, Rorsman H. Patch test reactions to basic chromium (III) sulfate. Arch Dermatol. 1965;91(3):233–4.
Nethercott J, Paustenbach D, Adams R, Fowler J, Marks J, Morton C, et al. A study of chromium induced allergic contact dermatitis with 54 volunteers: implications for environmental risk assessment. Occup Environ Med. 1994;51(6):371–80. doi:10.1136/oem.51.6.371.
Kosann MK, Brancaccio RR, Shupack JL, Franks AG Jr, Cohen DE. Six-hour versus 48-hour patch testing with varying concentrations of potassium dichromate. Dermatitis. 1998;9(2):92–5.
Hansen MB, Menné T, Johansen JD. Cr(III) and Cr(VI) in leather and elicitation of eczema. Contact Dermatitis. 2006;54(5):278–82. doi:10.1111/j.0105-1873.2006.00824.x.
Basketter DA, Angelini G, Ingber A, Kern PS, Menné T. Nickel, chromium and cobalt in consumer products: revisiting safe levels in the new millennium. Contact Dermatitis. 2003;49(1):1–7. doi:10.1111/j.0105-1873.2003.00149.x.
Lindström D, Hedberg Y, Odnevall Wallinder I. Chromium(III) and chromium(VI) surface treated galvanized steel for outdoor constructions: environmental aspects. Environ Sci Technol. 2010;44(11):4322–7. doi:10.1021/es1003022.
Oberdörster G, Oberdörster E, Oberdörster J. Nanotoxicology: an emerging discipline evolving from studies of ultrafine particles. Environ Health Perspect. 2005;113(7):823–39. doi:10.1289/ehp.7339.
Keegan GM, Learmonth ID, Case C. A systematic comparison of the actual, potential, and theoretical health effects of cobalt and chromium exposures from industry and surgical implants. Crit Rev Toxicol. 2008;38(8):645–74. doi:10.1080/10408440701845534.
Hedberg Y, Odnevall Wallinder I. Metal release and speciation of released chromium from a biomedical CoCrMo alloy into simulated physiologically relevant solutions. J Biomed Mater Res B Appl Biomater. 2014;102(4):693–9. doi:10.1002/jbm.b.33048.
Liden C, Bruze M, Thyssen JP, Menné T, editors. Metals. Contact dermatitis. Berlin Heidelberg: Springer; 2011.
Kleban M. Lanxess Deutschland GmbH, personal communication. 2016.
Wass U, Wahlberg JE. Chromated steel and contact allergy. Contact Dermatitis. 1991;24(2):114–8.
Hedberg Y, Gustafsson J, Karlsson HL, Möller L, Odnevall Wallinder I. Bioaccessibility, bioavailability and toxicity of commercially relevant iron- and chromium-based particles: in vitro studies with an inhalation perspective. Part Fibre Toxicol. 2010;7:23. doi:10.1186/1743-8977-7-23.
Hedberg Y, Midander K, Odnevall Wallinder I. Particles, sweat, and tears: a comparative study on bioaccessibility of ferrochromium alloy and stainless steel particles, the pure metals and their metal oxides, in simulated skin and eye contact. Integr Environ Assess Manag. 2010;6(3):456–68. doi:10.1002/ieam.66.
Midander K, de Frutos A, Hedberg Y, Darrie G, Odnevall Wallinder I. Bioaccessibility studies of ferro-chromium alloy particles for a simulated inhalation scenario: a comparative study with the pure metals and stainless steel. Integr Environ Assess Manag. 2010;6(3):441–55. doi:10.1002/ieam.32.
Hedberg YS, Herting G, Latvala S, Elihn K, Karlsson HL, Odnevall Wallinder I. Surface passivity largely governs the bioaccessibility of nickel-based powder particles at human exposure conditions. Regul Toxicol Pharmacol. 2016;81:162–70. doi:10.1016/j.yrtph.2016.08.013.
Hedberg Y, Wang X, Hedberg J, Lundin M, Blomberg E, Odnevall Wallinder I. Surface-protein interactions on different stainless steel grades – effects of protein adsorption, surface changes and metal release. J Mater Sci Mater Med. 2013;24(4):1015–33. doi:10.1007/s10856-013-4859-8.
Hedberg Y, Mazinanian N, Odnevall Wallinder I. Metal release from stainless steel powders and massive sheet – comparison and implication for risk assessment of alloys. Environ Sci Process Impacts. 2013;15(2):381–92. doi:10.1039/C2EM30818E.
Flint G, Carter S, Fairman B. Skin allergy from exposure to alloys of chromium. Contact Dermatitis. 1998;39(6):315–6.
Keane M, Stone S, Chen B, Slaven J, Schwegler-Berry D, Antonini J. Hexavalent chromium content in stainless steel welding fumes is dependent on the welding process and shield gas type. J Environ Monit. 2009;11(2):418–24.
Hedberg Y, Lidén C, Odnevall Wallinder I. Correlation between bulk- and surface chemistry of Cr-tanned leather and the release of Cr(III) and Cr(VI). J Hazard Mater. 2014;280:654–61. doi:10.1016/j.jhazmat.2014.08.061.
Mathiason F, Lidén C, Hedberg Y. Chromium released from leather – II: the importance of environmental parameters. Contact Dermatitis. 2015;72(5):275–85. doi:10.1111/cod.12334.
Hedberg YS, Lidén C, Lindberg M. Chromium dermatitis in a metal worker due to leather gloves and alkaline coolant. Acta Derm Venereol. 2016;96(1):104–6. doi:10.2340/00015555-2160.
Hedberg YS, Gumulka M, Lind M-L, Matura M, Lidén C. Severe occupational chromium allergy despite cement legislation. Contact Dermatitis. 2014;70(5):321–3. doi:10.1111/cod.12203.
Odler I. The BET-specific surface area of hydrated Portland cement and related materials. Cem Concr Res. 2003;33(12):2049–56. doi:10.1016/S0008-8846(03)00225-4.
Dooms-Goossens A, Ceuterick A, Vanmaele N, Degreef H. Follow-up study of patients with contact dermatitis caused by chromates, nickel, and cobalt. Dermatology. 1980;160(4):249–60.
Hald M, Agner T, Blands J, Ravn H, Johansen JD. Allergens associated with severe symptoms of hand eczema and a poor prognosis. Contact Dermatitis. 2009;61(2):101–8. doi:10.1111/j.1600-0536.2009.01577.x.
Bregnbak D, Thyssen JP, Zachariae C, Johansen JD. Characteristics of chromium-allergic dermatitis patients prior to regulatory intervention for chromium in leather: a questionnaire study. Contact Dermatitis. 2014;71(6):338–47.
Avnstorp C. Follow-up of workers from the prefabricated concrete industry after the addition of ferrous sulphate to Danish cement. Contact Dermatitis. 1989;20(5):365–71. doi:10.1111/j.1600-0536.1989.tb03174.x.
Thormann J, Jespersen N, Joensen H. Persistence of contact allergy to chromium. Contact Dermatitis. 1979;5(4):261–4.
Bang Pedersen N. Chapter 11—the effects of chromium on the skin. In: Langård S, editor. Biological and environmental aspects of chromium. Amsterdam: Elsevier Biomedical Press; 1982. p. 249–75.
Wall LM, Gebauer KA. A follow-up study of occupational skin disease in Western Australia. Contact Dermatitis. 1991;24(4):241–3.
Fregert S. Occupational dermatitis in a 10–year material. Contact Dermatitis. 1975;1(2):96–107.
Lips R, Rast H, Elsner P. Outcome of job change in patients with occupational chromate dermatitis. Contact Dermatitis. 1996;34(4):268–71.
De Marchi S, Cecchin E, De Marchi SU. Systemic allergic dermatitis resulting from oral administration of chromium with a food supplement. Contact Dermatitis. 2014;70(2):123–5.
Thomas P, Summer B. Diagnosis and management of patients with allergy to metal implants. Expert Rev Clin Immunol. 2015;11(4):501–9. doi:10.1586/1744666x.2015.1016501.
Bizzotto N, Sandri A, Trivellin G, Magnan B, Micheloni GM, Zamò A, et al. Chromium-induced diffuse dermatitis with lymph node involvement resulting from Langerhans cell histiocytosis after metal-on-metal hip resurfacing. Br J Dermatol. 2015;172(6):1633–6. doi:10.1111/bjd.13517.
Hubler WR. Dermatitis from a chromium dental plate. Contact Dermatitis. 1983;9(5):377–83. doi:10.1111/j.1600-0536.1983.tb04432.x.
Lachiewicz PF, Watters TS, Jacobs JJ. Metal hypersensitivity and total knee Arthroplasty. J Am Acad Orthop Surg. 2016;24(2):106–12. doi:10.5435/jaaos-d-14-00290.
Thomas P. Clinical and diagnostic challenges of metal implant allergy using the example of orthopaedic surgical implants. Allergo J Int. 2014;23(6):179–85. doi:10.1007/s40629-014-0023-3.
Lützner J, Hartmann A, Dinnebier G, Spornraft-Ragaller P, Hamann C, Kirschner S. Metal hypersensitivity and metal ion levels in patients with coated or uncoated total knee arthroplasty: a randomised controlled study. Int Orthop. 2013;37(10):1925–31. doi:10.1007/s00264-013-2010-6.
Bravo D, Wagner ER, Larson DR, Davis MP, Pagnano MW, Sierra RJ. No increased risk of knee arthroplasty failure in patients with positive skin patch testing for metal hypersensitivity: a matched cohort study. J Arthroplast. 2016;31:1717.
Gustafson K, Jakobsen SS, Lorenzen ND, Thyssen JP, Johansen JD, Bonefeld CM, et al. Metal release and metal allergy after total hip replacement with resurfacing versus conventional hybrid prosthesis. Acta Orthop. 2014;85(4):348–54. doi:10.3109/17453674.2014.922730.
Münch HJ, Jacobsen SS, Olesen JT, Menné T, Søballe K, Johansen JD, et al. The association between metal allergy, total knee arthroplasty, and revision. Acta Orthop. 2015;86(3):378–83. doi:10.3109/17453674.2014.999614.
To T, Stanojevic S, Moores G, Gershon AS, Bateman ED, Cruz AA, et al. Global asthma prevalence in adults: findings from the cross-sectional world health survey. BMC Public Health. 2012;12(1):1.
Anandan C, Nurmatov U, Van Schayck O, Sheikh A. Is the prevalence of asthma declining? Systematic review of epidemiological studies. Allergy. 2010;65(2):152–67.
Leynaert B, Sunyer J, Garcia-Esteban R, Svanes C, Jarvis D, Cerveri I, et al. Gender differences in prevalence, diagnosis and incidence of allergic and non-allergic asthma: a population-based cohort. Thorax. 2012;67(7):625–31.
Nemery B. Metal toxicity and the respiratory tract. Eur Respir J. 1990;3(2):202–19.
Fernández-Nieto M, Quirce S, Carnés J, Sastre J. Occupational asthma due to chromium and nickel salts. Int Arch Occup Environ Health. 2006;79(6):483–6.
Hannu T, Piipari R, Tuppurainen M, Nordman H, Tuomi T. Occupational asthma caused by stainless steel welding fumes: a clinical study. Eur Respir J. 2007;29(1):85–90.
Novey HS, Habib M, Wells ID. Asthma and IgE antibodies induced by chromium and nickel salts. J Allergy Clin Immunol. 1983;72(4):407–12.
Keskinen H, Kalliomäki P-L, Alanko K. Occupational asthma due to stainless steel welding fumes. Clin Exp Allergy. 1980;10(2):151–9.
Shirakawa T, Kusaka Y, Fujimura N, Goto S, Kato M, Heki S, et al. Occupational asthma from cobalt sensitivity in workers exposed to hard metal dust. Chest J. 1989;95(1):29–37.
Hegewald J, Uter W, Kränke B, Schnuch A, Gefeller O, Pfahlberg A. Patch test results with metals and meteorological conditions. Int Arch Allergy Immunol. 2008;147(3):235–40.
de Waard-van der Spek FB, Darsow U, Mortz CG, Orton D, Worm M, Muraro A, et al. EAACI position paper for practical patch testing in allergic contact dermatitis in children. Pediatr Allergy Immunol. 2015;26(7):598–606.
Fowler JF Jr, Kauffman CL, Marks JG Jr, Proctor DM, Fredrick MM, Otani JM, et al. An environmental hazard assessment of low-level dermal exposure to hexavalent chromium in solution among chromium-sensitized volunteers. J Occup Environ Med. 1999;41(3):150–60.
Bregnbak D, Johansen JD, Hamann D, Hamann CR, Hamann C, Spiewak R, et al. Assessment of chromium(VI) release from 848 jewellery items by use of a diphenylcarbazide spot test. Contact Dermatitis. 2016;75(2):115–7. doi:10.1111/cod.12577.
Bregnbak D, Johansen JD, Jellesen MS, Zachariae C, Thyssen JP. Chromium(VI) release from leather and metals can be detected with a diphenylcarbazide spot test. Contact Dermatitis. 2015;73(5):281–8. doi:10.1111/cod.12406.
Pflaum RT, Howick LC. The chromium-diphenylcarbazide reaction. J Am Chem Soc. 1956;78(19):4862–6. doi:10.1021/ja01600a014.
Marques M, Salvador A, Morales-Rubio A, De la Guardia M. Chromium speciation in liquid matrices: a survey of the literature. Fresen J Anal Chem. 2000;367(7):601–13.
EN 196-10:2006. Methods of testing cement – Part 10: Determination of the water-soluble chromium (VI) content of cement. CEN. 2006.
ISO. ISO 17075, Leather - Chemical tests - Determination of chromium(VI) content. 2007.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2018 Springer International Publishing AG, part of Springer Nature
About this chapter

Cite this chapter
Hedberg, Y.S. (2018). Metal Allergy: Chromium. In: Chen, J., Thyssen, J. (eds) Metal Allergy. Springer, Cham. https://doi.org/10.1007/978-3-319-58503-1_27
Download citation
DOI: https://doi.org/10.1007/978-3-319-58503-1_27
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-58502-4
Online ISBN: 978-3-319-58503-1
eBook Packages: MedicineMedicine (R0)