
Abstract
Fine needle aspiration and small tissue biopsies have become a popular modality for an initial workup or to achieve a definitive diagnosis of a patient with lymphadenopathy. This chapter delineated cytologic and histologic features of common and rare neoplastic and nonneoplastic lesions of the lymph node. The utilities and pitfalls of commonly used diagnostic immunohistochemical (IHC) stains such as PAX5, LEF1, LMO2, and SOX11, and small diagnostic IHC panels, and flow cytometry were described. Multiple challenging and yet practical cases at the end of the chapter were used to re-emphasize important points illustrated throughout the chapter.
Access provided by CONRICYT-eBooks. Download chapter PDF
Similar content being viewed by others



Keywords
- Lymph node
- Suppurative lymphadenitis
- Infectious mononucleosis
- Rosai-Dorfman disease
- Granulomatous lymphadenitis
- T-cell lymphoma
- Anaplastic large cell lymphoma (ALCL)
- Myeloid sarcoma
- Lymphoblastic lymphoma
- Chronic lymphocytic leukemia/small lymphocytic lymphoma
- Splenic marginal zone lymphoma
- Nodal marginal zone lymphoma
- Follicular lymphoma
- Mantle cell lymphoma
- Diffuse large B-cell lymphoma (DLBCL)
- Plasmablastic lymphoma
- Hodgkin lymphoma
- Nodular lymphocyte-predominant Hodgkin lymphoma
- Nodular sclerosis classical Hodgkin lymphoma
- Lymphocyte-rich classical Hodgkin lymphoma
- Mixed cellularity classical Hodgkin lymphoma
- Lymphocyte-depleted classical Hodgkin lymphoma
- Histiocytic sarcoma
- Langerhans cell histiocytosis
- Langerhans cell sarcoma
- Interdigitating dendritic cell sarcoma
- Follicular dendritic cell sarcoma
- Sarcoma
- Carcinoma
- Melanoma
- Germ cell tumor
- t(8;14)(q24;q32)
- t(11;14)(q13;q32)
- t(14;18)(q32;q21)
- t(2;5)(p23;q35)
- CD20
- CD79a
- PAX5
- CD2
- CD3
- CD4
- CD5
- CD7
- CD8
- CD10
- CD15
- CD30
- EMA
- IMP3
- EBV
- MUM1
- MYC
- cCD3
- CD23
- BCL2
- BCL1 (cyclin D1)
- BCL6
- LEF1
- LMO2
- SOX11
- TdT
- ALK-1
- CD38
- CD138
- CD1a
- CD21
- CD35
- CD117
- CD43
- CD68
- Lysozyme
- CD34
- Granzyme
- MPO
- ZAP-70
- TIA
- BRAF
- MYD88
- EZH2
- GNA13
- STAT3
- IgH
-
Always attempt to get sufficient sample for flow cytometric study, molecular analysis, and cellblock preparation if a lymphoma is suspected.
-
A final diagnosis of lymphoma should not be based on cytomorphology alone. Ancillary tests such as flow cytometric study, immunohistochemistry (IHC), and cytogenetic analysis/fluorescence in situ hybridization (FISH) should be performed.
-
Cell block preparation for immunostains is highly recommended if large B-cell lymphoma (LBCL) is suspected, since a significant number of cases have an inconclusive diagnosis from flow cytometric analysis due to the breakdown of the cytoplasm of lymphoid cells.
-
Incisional or excisional biopsy is recommended for all cases suspicious for Hodgkin lymphoma , T-cell lymphoma , T-cell-rich B-cell lymphoma, transformation from a low-grade lymphoma into a high-grade non-Hodgkin lymphoma and unusual types of lymphoma.
-
Culture should be considered when acute inflammation and necrosis are present.
-
Mycobacterial infection should be considered when a granulomatous process and necrosis are present.
-
Cohesive sheets and groups of lymphoid cells are frequently seen in an LBCL that might be mistaken for metastatic carcinoma .
-
Noncaseating granulomas are frequently seen in Hodgkin lymphoma and T-cell lymphoma, in addition to benign conditions and metastatic tumors, such as seminoma.
-
In addition to Burkitt lymphoma (BL), cytoplasmic vacuoles can be seen in other high-grade lymphomas, rhabdomyosarcoma, seminoma, and carcinomas.
-
Lymphoglandular bodies are less frequently present in plasmacytoma or myeloid sarcoma .
-
HIV-associated follicular hyperplasia and mononucleosis are more likely to mimic a high-grade lymphoma.
-
Collision tumors, such as metastatic small cell carcinoma or melanoma in the background of small lymphocytic lymphoma (SLL), are infrequent, but can be seen.
-
Most low-grade lymphomas have a mindbomb homolog 1 (MIB-1, Ki-67) proliferative index less than 26%; in contrast, high-grade lymphoma usually has a MIB-1 proliferative index greater than 26%.
2017 WHO Classification of Mature Lymphoid , Histiocytic, and Dendritic Neoplasms
Used with permission from Arber et al. (Arber et al. 2016); and from Swerdlow et al. (Swerdlow et al. 2016a).
Mature B-Cell Neoplasms
-
Chronic lymphocytic leukemia /small lymphocytic lymphoma (CLL/SLL)
-
Monoclonal B-cell lymphocytosisFootnote 1
-
B-cell prolymphocytic leukemia
-
Splenic marginal zone lymphoma (MZL )
-
Hairy cell leukemia
-
Splenic B-cell lymphoma/leukemia, unclassifiable
-
Splenic diffuse red pulp small B-cell lymphoma
-
Hairy cell leukemia variant
-
-
Lymphoplasmacytic lymphoma (LPL)
-
Waldenström macroglobulinemia
-
-
Monoclonal gammopathy of undetermined significance (MGUS), IgM2
-
Mu heavy chain disease
-
Gamma heavy chain disease
-
Alpha heavy chain disease
-
MGUS, IgG/AFootnote 2
-
Plasma cell myeloma
-
Solitary plasmacytoma of the bone
-
Extraosseous plasmacytoma
-
Monoclonal immunoglobulin deposition diseases3
-
Extranodal MZL of mucosa-associated lymphoid tissue (MALT lymphoma)
-
Nodal MZL
-
Pediatric nodal MZL
-
-
Follicular lymphoma
-
In situ follicular neoplasia3
-
Duodenal-type follicular lymphoma3
-
-
Pediatric-type follicular lymphoma3
-
LBCL with interferon regulatory factor 4 (IRF4) rearrangement 3
-
Primary cutaneous follicle center lymphoma
-
Mantle cell lymphoma (MCL )
-
In situ mantle cell neoplasia3
-
-
Diffuse large B-cell lymphoma (DLBCL ), not otherwise specified (NOS)
-
Germinal center B-cell type3
-
Activated B-cell (ABC) type3
-
-
T-cell/histiocyte-rich LBCL
-
Primary DLBCL of the central nervous system (CNS)
-
Primary cutaneous DLBCL , leg type
-
Epstein-Barr virus (EBV )-positive DLBCL , NOSFootnote 3
-
EBV + mucocutaneous ulcer 4
-
DLBCL associated with chronic inflammation
-
Lymphomatoid granulomatosis
-
Primary mediastinal (thymic) LBCL
-
Intravascular LBCL
-
ALK-positive LBCL
-
Plasmablastic lymphoma
-
Primary effusion lymphoma
-
Human herpes virus 8 (HHV8)-positive DLBCL , NOS 4
-
Burkitt lymphoma
-
Burkitt-like lymphoma with 11q aberration 4
-
High-grade B-cell lymphoma (HGBCL), with MYC and BCL2 and/or BCL6 rearrangements4
-
HGBCL, NOS4
-
B-cell lymphoma, unclassifiable, with features intermediate between DLBCL and CHL
Mature T- and Natural Killer (NK)-Cell Neoplasms
-
T-cell prolymphocytic leukemia
-
T-cell large granular lymphocytic leukemia
-
Chronic lymphoproliferative disorder of NK cells
-
Aggressive NK-cell leukemia
-
Systemic EBV + T-cell lymphoma of childhoodFootnote 4
-
Hydroa vacciniforme-like lymphoproliferative disorder5
-
Adult T-cell leukemia/lymphoma
-
Extranodal NK/T-cell lymphoma , nasal type
-
Enteropathy-associated T-cell lymphoma
-
Monomorphic epitheliotropic intestinal T-cell lymphoma5
-
Indolent T-cell lymphoproliferative disorder of the gastrointestinal (GI) tract 5
-
Hepatosplenic T-cell lymphoma
-
Subcutaneous panniculitis-like T-cell lymphoma
-
Mycosis fungoides
-
Sézary syndrome
-
Primary cutaneous CD30 -positive T-cell lymphoproliferative disorders
-
Lymphomatoid papulosis
-
Primary cutaneous anaplastic large cell lymphoma
-
-
Primary cutaneous gamma-delta T-cell lymphoma
-
Primary cutaneous CD8 -positive aggressive epidermotropic cytotoxic T-cell lymphoma
-
Primary cutaneous acral CD8 -positive T-cell lymphoma 5
-
Primary cutaneous CD4 -positive small/medium T-cell lymphoproliferative disorder 5
-
Peripheral T-cell lymphoma, NOS
-
Angioimmunoblastic T-cell lymphoma
-
Follicular T-cell lymphoma Footnote 5
-
Nodal peripheral T-cell lymphoma with T follicular helper (TFH) phenotype 6
-
Anaplastic large cell lymphoma, ALK positive
-
Anaplastic large cell lymphoma, ALK negative6
-
Breast implant-associated ALCL 6
Hodgkin Lymphoma
-
Nodular lymphocyte-predominant Hodgkin lymphoma
-
Classical Hodgkin lymphoma (CHL)
-
Nodular sclerosis CHL
-
Lymphocyte-rich CHL
-
Mixed cellularity CHL
-
Lymphocyte-depleted CHL
-
Posttransplant Lymphoproliferative Disorders (PTLD )
-
Plasmacytic hyperplasia PTLD
-
Infectious mononucleosis PTLD
-
Florid follicular hyperplasia PTLD6
-
Polymorphic PTLD
-
Monomorphic PTLD (B- and T-/NK-cell types)
-
CHL PTLD
Histiocytic and Dendritic Cell Neoplasms
-
Histiocytic sarcoma
-
Langerhans cell histiocytosis (LCH )
-
Langerhans cell sarcoma
-
Indeterminate dendritic cell tumor
-
Interdigitating dendritic cell sarcoma
-
Follicular dendritic cell sarcoma
-
Fibroblastic reticular cell tumor
-
Disseminated juvenile xanthogranuloma
-
Erdheim-Chester diseaseFootnote 6
B Lymphoblastic Leukemia /Lymphoma
-
B lymphoblastic leukemia/lymphoma, NOS
-
B lymphoblastic leukemia/lymphoma with recurrent genetic abnormalities
-
B lymphoblastic leukemia/lymphoma with t(9;22)(q34.1;q11.2); BCR-ABL1B lymphoblastic leukemia/lymphoma with t(v;11q23.3); KMT2A rearranged
-
B lymphoblastic leukemia/lymphoma with t(12;21)(p13.2;q22.1); ETV6-RUNX1
-
B lymphoblastic leukemia/lymphoma with hyperdiploidy
-
B lymphoblastic leukemia/lymphoma with hypodiploidy
-
B lymphoblastic leukemia/lymphoma with t(5;14)(q31.1;q32.3) IL3-IGH
-
B lymphoblastic leukemia/lymphoma with t(1;19)(q23;p13.3); TCF3-PBX1
-
Provisional entity: B lymphoblastic leukemia/lymphoma, BCR-ABL1-like
-
Provisional entity: B lymphoblastic leukemia/lymphoma with iAMP21
T Lymphoblastic Leukemia/Lymphoma
Provisional entity: early T-cell precursor lymphoblastic leukemia
Provisional entity: NK-cell lymphoblastic leukemia/lymphoma
Nonneoplastic Lymph Nod es
Cytological Features (Fig. 4.1a, b)
-
High cellularity
-
Mixed population of lymphoid cells with small lymphocytes predominant
-
Plasma cells, plasmacytoid cells, and immunoblasts
-
Histiocytes and tingible-body macrophages

(a, b) Reactive lymph node with a mixed population of lymphoid cells with small lymphocytes predominant on Diff-Quik (a) and Pap stain (b)
Suppurative Lymphadenitis
Cytological Features (Fig. 4.2a, b)
-
Mixed population of lymphoid cells with a variable number of neutrophils.
-
Degenerated lymphoid cells, histiocytes, neutrophils, and necrotic debris.
-
Bacteria or fungus may be seen.
-
Etiologies could include cat-scratch disease, bacterial infection, lupus, and less commonly Hodgkin lymphoma and metastatic carcinomas.

(a, b) Suppurative lymphadenitis with degenerated lymphoid cells, histiocytes, neutrophils, and necrotic debris on Diff-Quik (a) and Pap stain (b)
Histologic Features
-
Preserved nodal architecture with lymphoid follicular hyperplasia (Fig. 4.3).
Fig. 4.3 
Suppurative lymphadenitis showing preserved nodal architecture with reactive lymphoid follicles and focal abscess formation
-
Hyperplastic lymphoid follicles show polarity with tingible-body macrophages (Fig. 4.4).
Fig. 4.4 
Reactive lymphoid follicles with polarity and tingible-body macrophages
-
Increased neutrophilic infiltrate, abscess formation, and perilymphadenitis (Fig. 4.5).
Fig. 4.5 
Suppurative lymphadenitis with focal abscess formation and necrosis



Infectious Mononucleosis
Cytological Features
-
Highly cellular specimen
-
Mixed population of lymphoid cells with many immunoblasts and plasmacytoid cells.
-
Large atypical lymphoid cells are frequently present; some may mimic Hodgkin cells.
-
Flow cytometry reveals an abundance of CD8 -positive T cells and only a small population of B cells.
Histologic Features
-
Preserved nodal architecture with paracortical expansion composed of mixed mature lymphocytes, plasma cells, immunoblasts, and histiocytes in a mottled pattern (Figs. 4.6 and 4.7)
Fig. 4.6 
Infectious mononucleosis with reactive lymphoid follicles and perifollicular expansion
Fig. 4.7 
Infectious mononucleosis with lymphoblasts and immunoblasts showing prominent nucleoli
-
Lymphoid follicular hyperplasia
-
EBV -positive by in situ hybridization stain (Fig. 4.8)
Fig. 4.8 
Infectious mononucleosis with positive EBV by in situ hybridization stain



Differential Diagnosis
-
HGBCL
-
Hodgkin lymphoma
Rosai-Dorfman Diseas e
Cytological Features
-
Mixed population of lymphoid cells.
-
A large number of histiocytes with pale cytoplasm.
-
Many histiocytes contain lymphoid cells or red blood cells.
-
These histiocytes are positive for S100, but negative for CD1a .
-
Tissue biopsy should be recommended for a final diagnosis.
Histologic Features
-
Marked sinus dilatation with sheets of foamy histiocytes (Figs. 4.9 and 4.10).
Fig. 4.9 
Lymph node with Rosai-Dorfman disease shows marked sinus dilation
Fig. 4.10 
Lymph node with Rosai-Dorfman disease shows sheets of histiocytes
-
Some histiocytes may contain lymphocytes, plasma cells, or red blood cells.


Granulomatous Lymphadenitis
Cytological Features (Fig. 4.11a–c)
-
Mixed population of lymphoid cells.
-
Epithelioid histiocytes in aggregates with or without multinucleated giant cells.
-
Necrotic debris and acute inflammatory cells may or may not be present.
-
Etiologies could include foreign body reaction, sarcoidosis, fungus, mycobacteria, and toxoplasmic lymphadenitis.
-
Culture should be submitted.

(a–c) Granulomatous lymphadenitis with epithelioid histiocytes in aggregates with or without multinucleated giant cells and a mixed population of lymphoid cells on Diff-Quik (a), Pap stain (b), and cellblock preparation (c)
Histologic Features
-
Granulomas with necrosis in infection of mycobacteria (Figs. 4.12, 4.13, and 4.14)
Fig. 4.12 
Lymph node with caseating granulomas in tuberculosis
Fig. 4.13 
Lymph node with caseating granulomas showing necrosis and giant cells
Fig. 4.14 
Special stain (acid-fast bacilli [AFB], acid-fast Fite) reveals mycobacteria in caseating granulomas
-
Granulomas surrounded by few or no lymphocytes (naked granuloma) in sarcoidosis (Figs. 4.15, 4.16, 4.17, and 4.18)
Fig. 4.15 
Sarcoidosis in lymph node with noncaseating granulomas
Fig. 4.16 
Sarcoidosis in lymph node with “naked” noncaseating granulomas
Fig. 4.17 
Sarcoidosis in the spleen with noncaseating granulomas
Fig. 4.18 
Sarcoidosis in the spleen with “naked” noncaseating granulomas
-
Epithelioid granuloma and sheets of monocytoid lymphocytes in infection of Toxoplasma (Figs. 4.19 and 4.20)
Fig. 4.19 
Lymph node with toxoplasma shows reactive lymphoid follicles and expanded perifollicular area in a “mottled” appearance
Fig. 4.20 
Lymph node with toxoplasma shows cluster of epithelioid histiocytes and monocytoid lymphocytes
-
Multinucleated cells with foreign body in foreign body granuloma (Fig. 4.21)
Fig. 4.21 
Foreign body granuloma with giant cells containing foreign body (arrow)










Non-Hodgkin Lymphoma s
Cytological Features
-
Hypercellular specimen
-
A relatively uniform population of lymphoid cells
-
Can be divided into three groups
-
Group 1 – small lymphoid cells (smaller than histiocytes), such as small lymphocytic lymphoma (SLL), grade I follicular lymphoma, MZL , LPL
-
Group 2 –intermediate lymphoid cells (same size as histiocytes), such as MCL , grade II follicular lymphoma, BL, lymphoblastic lymphoma
-
Group 3 – large lymphoid cells (larger than histiocytes), such as LBCL, grade III follicular lymphoma, ALCL , some T-cell lymphomas
-
Immunophenotypes of B-cell lymphoma (Table 4.1) and frequent chromosomal translocations and gene mutations (Tables 4.2 and 4.3)
Table 4.1 Immunophenotype of B-cell lymphomas Table 4.2 Summary of chromosomal translocation-associated lymphomas and the affected genes Table 4.3 Most common gene mutations in non-Hodgkin lymphomas
Small Lymphocytic Lymphoma (SLL)
Clinical Features
-
Rare before 40 years of age
-
General lymphadenopathy
-
Bone marrow involvement
Cytological Features (Fig. 4.22a, b)
-
Highly cellular
-
Monotonous population of small lymphocytes
-
Smooth nuclear membrane, “clock face” nuclear chromatin, small to invisible nucleoli, and scant cytoplasm

(a, b) Small lymphocytic lymphoma with monotonous population of small lymphocytes on Diff-Quik (a) and Pap stain (b)
Histologic Features
-
Effaced nodal architecture in a vaguely nodular (pseudofollicular) pattern (Fig. 4.23).
Fig. 4.23 
Small lymphocytic lymphoma with effaced nodal architecture in a vaguely nodular (pseudofollicular) pattern
-
Sheets of neoplastic lymphocytes with hypercondensed chromatin and round to slightly irregular nuclear contour (Fig. 4.24).
Fig. 4.24 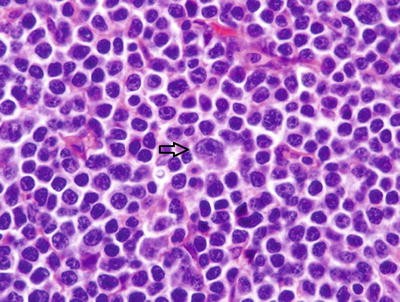
Small lymphocytic lymphoma cells with hypercondensed chromatin and round nuclear contour; admixed prolymphocytes (arrow) with nucleolus and larger in size
-
Admixed with prolymphocytes.
-
Adenopathy <1.5 cm by computed tomography (CT) scan is called tissue-based monoclonal B-cell lymphocytosis.


Immunohistochemistry and Ancillary Studies
-
Flow cytometry studies: CD19+, CD20 + (low intensity), CD5 +, CD23 +, CD43 +, FMC7- (Fig. 4.25a–d); CD38 and zeta-chain-associated protein kinase 70 (ZAP-70 ) to evaluate the prognosis: both negative, most favorable; one positive and one negative, intermediate; and both positive, least favorable prognosis
Fig. 4.25 
(a–d) Flow cytometry studies in small lymphocytic lymphoma shows CD19+ lymphoma cells with coexpression of CD5 and CD23 , positive for CD43 and negative for FMC7
-
IHC: CD20 +, PAX5 + (especially important after Rituxan treatment that cause CD20 negativity on IHC), CD5 +, CD23 +, lymphoid enhancer-binding factor 1 (LEF1 )+ (Fig. 4.26)
Fig. 4.26 
Small lymphocytic lymphoma positive for LEF1
-
FISH: deletion of 13q14 in 50% of cases, trisomy 12 in 20% of cases (Figs. 4.27 and 4.28)
Fig. 4.27 
FISH in small lymphocytic lymphoma with deletion of 13q14 (IR2G2A) in 50% of cases
Fig. 4.28 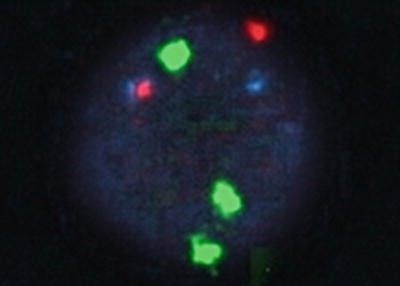
FISH in small lymphocytic lymphoma with trisomy 12 (2R3G2A) in 20% of cases




Differential Diagnosis
-
Reactive lymph node
-
Other low-grade lymphoma
Follicular Lymphoma
Clinical Features
-
Accounts for 35% of adult non-Hodgkin lymphomas in the USA and 22% worldwide.
-
Accounts for 70% of “low-grade” lymphomas in the USA.
-
Affecting mainly adults, median age of 59 years, rarely occurs before age 20 years.
-
40% of patients have bone marrow involvement at the initial diagnosis.
Cytological Features (Fig. 4.29a–d)
-
Usually cellular.
-
Small lymphocytes with cleaved nuclei.
-
Papanicolaou (Pap) stain better shows nuclear membrane irregularities.
-
Small to inconspicuous nucleoli and scant cytoplasm.
-
Increased numbers of large atypical lymphoid cells (centroblasts) in grade 2 and grade 3 follicular lymphoma.
-
Grading of follicular lymphoma in a fine needle aspiration (FNA) specimen is similar to that of a histological specimen by counting the number of centroblasts at 40x high-power field (HPF); i.e., grade 1, 0–5 centroblasts/HPF; grade 2, 6–15 centroblasts/HPF; and grade 3, >15 centroblasts/HPF.
-
MIB-1 (Ki-67) is a useful marker to differentiate most grade 1 and grade 2 from grade 3.
-
In situ follicular neoplasia with a low rate of progression can be detected by flow cytometry studies in half of the cases. Careful interpretation of FNA specimens is recommended.

(a–d) Follicular lymphoma with increased numbers of large atypical lymphoid cells (centroblasts) in grade 1 (a, b), grade 2 (c), and grade 3 (d) follicular lymphoma
Histologic Features
-
Effaced nodal architecture in follicular pattern, follicles >75% (Fig. 4.30); in follicular and diffuse pattern, follicles 25–75%; in focally follicular pattern, follicles <25%; and in diffuse pattern, follicles 0%.
Fig. 4.30 
Follicular lymphoma with effaced nodal architecture in a follicular pattern as “balls in a bag”
-
Neoplastic follicles are usually round, surrounded by decreased mantle zone and composed of centrocytes and centroblasts without tingible-body macrophages.
-
Centrocytes have mature chromatin and folded nuclear membrane; centroblasts show prominent nucleolus and round nuclear contour (Fig. 4.31).
Fig. 4.31 
Neoplastic cells (centrocytes) with folded nuclear contour and mature chromatin; admixed centroblasts (arrow) with smooth nuclear membrane and vesicular chromatin
-
Grades 1–2 (low grade) with similar clinical prognosis
-
Grade 1: <5 centroblasts/HPF
-
Grade 2: 6–15 centroblasts/HPF
-
-
Grade 3 (high grade): >15 centroblasts/HPF
-
Grade 3A: centroblasts separated by centrocytes
-
Grade 3B: sheets of centroblasts
-


Immunohistochemistry and Ancillary Studies
-
Flow cytometry: CD19+, CD20 +, CD10 + (Fig. 4.32a–d)
Fig. 4.32 
(a–d) Flow cytometry studies of follicular lymphoma with coexpression of CD10 , high intensity of CD20 , and immunoglobulin light chain restriction
-
IHC: CD20 +, CD10 +, BCL2 +, BCL6 + and LIM-only transcription factor-2 (LMO2 )+ (Fig. 4.33)
Fig. 4.33 
Follicular lymphoma with LMO2 positivity
-
FISH: positive for t(14;18)(q32;q21) (IGH;BCL2) (Fig. 4.34)
Fig. 4.34 
FISH in follicular lymphoma with t(14;18) ( IGH; BCL2 ) (1R1G2A, arrow)



Differential Diagnosis
-
Reactive lymph node
-
Other low-grade lymphoma
Marginal Zone Lymphoma (MZL )
Clinical Features
-
Involving nodal and extranodal sites
-
Commonly in women
-
Usually in the elderly
Cytological Features (Fig. 4.35a–f)
-
Cellular smear
-
A heterogeneous population of cells, including plasmacytoid cells, plasma cells, scattered immunoblasts, centrocyte-like cells
-
Monocytoid B cells

(a–f) Marginal zone lymphoma with a heterogeneous population of cells, including plasmacytoid cells, plasma cells, scattered immunoblasts, centrocyte-like cells on Diff-Quik (S), and Pap stain (b). Note that immunostain performed on the direct FNA smears showed CD20 positivity (c), Kappa light chain restriction (d), lack of Lambda light chain (e), and low Ki-67 proliferative index (f)
Histologic Features
-
Expanded marginal zone (Fig. 4.36)
Fig. 4.36 
Marginal zone lymphoma with effaced nodal architecture and marked marginal zone expansion
-
Neoplastic cells may appear as monocytoid, plasmacytoid, or centrocyte-like cells (Fig. 4.37).
Fig. 4.37 
Neoplastic marginal zone cells show round nuclear contour and mature chromatin with monocytoid or plasmacytoid appearance


Immunohistochemistry and Ancillary Studies
-
Flow cytometry: CD19+, CD20 +, CD5 -, CD10 -, CD23 -
-
IHC: CD20 +, CD43 + (50% of cases), immunoglobulin superfamily receptor translocation associated 1(IRTA1)+ (Fig. 4.38)
Fig. 4.38 
Neoplastic marginal zone cells positive for IRTA1

Differential Diagnosis
-
Reactive lymph node
-
Other low-grade lymphoma
Mantle Cell Lymphoma (MCL )
Clinical Features
-
3–10% of non-Hodgkin lymphomas.
-
Median age of 60 and male predominance.
-
Involvement of the lymph nodes, spleen, and bone marrow.
-
Up to 30% with GI involvement.
-
Up to 25% with peripheral blood involvement.
-
Two types: sex-determining region Y box (SOX)11-positive/immunoglobulin heavy chain variable (IGHV)-unmutated MCL typically involves lymph nodes and other extranodal sites with an aggressive clinical behavior; SOX11 -negative/IGHV-mutated MCL usually involves the peripheral blood, bone marrow, and spleen with an indolent clinical course.
Cytological Features (Fig. 4.39a, b)
-
Cellular smear.
-
Homogeneous population of small- to intermediate-size lymphocytes
-
Slightly cleft nuclear membrane.
-
Condensed chromatin.
-
Inconspicuous nucleoli.
-
Many large cells are seen in a blastoid variant (resembling lymphoblasts) with a high mitotic index (>10/10 HPF).
-
Positive for CD20 , CD5 , and negative for CD23 and CD10 .
-
FISH showing nearly 100% of cases with the t(11;14) translocation.
-
Cyclin D1 overexpression by immunostain.

(a, b) Mantle cell lymphoma with a homogeneous population of small to intermediate-size lymphocytes with slightly cleft nuclear membranes on Diff-Quik (a) and Pap stain (b)
Histologic Features
-
Nodular pattern with expanded mantle zone and may show a diffuse pattern (Fig. 4.40).
Fig. 4.40 
Mantle cell lymphoma with effaced nodal architecture and mantle zone expansion in a vaguely nodular pattern
-
Neoplastic cells with mature chromatin and irregular nuclear contour (Fig. 4.41).
Fig. 4.41 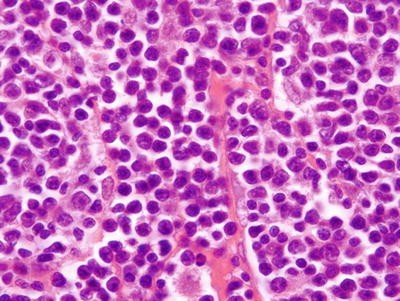
Neoplastic mantle cells with irregular nuclear contour and mature chromatin
-
Capillary proliferation (Fig. 4.42).
Fig. 4.42 
Mantle cell lymphoma with capillary proliferation
-
Aggressive variants:
-
Blastoid variant with lymphoblasts
-
Pleomorphic variant with oval to irregular nuclear contour and prominent nucleolus
-
-
Other variants:
-
Small cell variant mimicking SLL
-
Marginal zone-like variant with monocytoid cells
-
-
In situ mantle cell neoplasia with a low rate of progression and indolent clinical course. Careful interpretation of FNA specimen is recommended.



Immunohistochemistry and Ancillary Studies
-
Flow cytometry: CD19+, CD20 +, CD5 +, FMC7+, CD43 - (Fig. 4.43a–d)
Fig. 4.43 
(a–d) Flow cytometry studies of mantle cell lymphoma with coexpression of CD5 , positivity of FMC7, and immunoglobulin light chain restriction
-
IHC: CD20 +, CD5 +, BCL1+, SOX11 + (Figs. 4.44 and 4.45)
Fig. 4.44 
Immunohistochemical study of SOX11 in mantle cell lymphoma shows mantle zone expansion
Fig. 4.45 
Immunohistochemical study in mantle cell lymphoma shows mantle cells positive for SOX11
-
FISH: t(11;14) (CCND1;IGH) (Fig. 4.46)
Fig. 4.46 
FISH in mantle cell lymphoma with t(14;18) (CCND1;IGH) (1R1G2F)




Differential Diagnosis
-
Reactive lymph node
-
Other low-grade lymphoma
Plasmacytoma/Multiple Myeloma
Cytological Features (Fig. 4.47a, b)
-
Mature or immature plasma cells.
-
Binucleation or multinucleation.
-
Intranuclear bodies (Dutcher body) or intracytoplasmic bodies (Russell body).
-
Positive for CD38 and CD138 and negative for CD20 .
-
May be positive for epithelial membrane antigen (EMA ), but negative for cytokeratin.
-
IgM MGUS is more closely related to LPL.

(a, b) Plasmacytoma on Diff-Quik (a) and Pap stain (b)
Histologic Features
-
Sheets of plasma cells in tissue or lymph node (Figs. 4.48 and 4.49).
Fig. 4.48 
Plasmacytoma with sheets of plasma cells
Fig. 4.49 
Neoplastic plasma cells with less mature chromatin, nucleolus, and scattered binucleation
-
Multiple myeloma in bone marrow biopsy: monotypic plasma cells represent >30% of marrow cellularity.


Immunohistochemistry and Ancillary Studies
-
IHC: CD138 + (Fig. 4.50) used to evaluate volume of plasma cells and kappa and lambda for clonality; some neoplastic plasma cells show aberrant expression of CD56, BCL1, and CD117 .
Fig. 4.50 
Plasmacytoma with sheets of CD138 positive plasma cells

Large B-Cell Lymphom a (LBCL)
Clinical Features
-
Accounts for 30%–40% of adult non-Hodgkin lymphomas in western countries.
-
Nodal or extranodal disease.
-
Forty percent with initial extranodal presentation, GI tract most common.
-
HIV or other immunodeficiency is a risk factor.
-
Many morphologic variants, including centroblastic, immunoblastic, and anaplastic, and subtypes, such as T-cell/histiocytes-rich, primary DLBCL of the CNS, primary cutaneous DLBCL leg type and EBV -positive DLBCL, NOS, et al.
-
t(14;18) chromosomal translocation in 30% of cases.
-
Two major patterns of gene expression in DLBCL : germinal center (GC)-B cell type DLBCL and activated B-cell (ABC)-type DLBCL. GC-type DLBCL has a much better prognosis than ABC-type DLBCL.
Cytological Features (Fig. 4.51a–g)
-
Highly cellular specimen.
-
Dispersed large uniform to variable-size lymphoid cells.
-
Numerous lymphoglandular bodies in the background.
-
Large pleomorphic nuclei, irregular nuclear contour, and prominent nucleoli.
-
Multinucleated giant cells can be seen.
-
Variable nuclear-to-cytoplasmic ratio.
-
Cohesive groups of large atypical lymphoid cells may mimic other malignant tumors, such as carcinoma , melanoma, and sarcoma .
-
Tumor necrosis and mitosis are usually present.


(a–g) Large B-cell lymphoma with large uniform to variable-size lymphoid cells on Diff-Quik (a, b) and Pap stain (c). Note that LBCL may mimic other malignant tumors, such as carcinoma , as shown in (d), on cellblock preparation (e), positive for CD20 (f) and increased Ki-67 proliferative index (g)
Histologic Features
-
Effaced nodal architecture in a diffuse pattern by medium to large neoplastic lymphocytes
-
Neoplastic cells in sheets or a scattered pattern, depending on the subtype (Figs. 4.52 and 4.55)
Fig. 4.52 
Diffuse large B-cell lymphoma with effaced nodal architecture in a diffuse pattern by sheets of large cells showing vesicular chromatin and prominent nucleolus

Immunohistochemistry and Ancillary Studies
-
IHC: positive for the B-cell markers CD20 (Figs. 4.53 and 4.56), paired box gene (PAX)5 (Fig. 4.54), B-cell Oct binding protein 1 (BOB1), octamer-binding transcription factor 2 (Oct2); MIB evaluates the proliferation rate.
Fig. 4.53 
Diffuse large B-cell lymphoma with sheets of CD20 -positive neoplastic cells
Fig. 4.54 
Diffuse large B-cell lymphoma with sheets of PAX5 -positive neoplastic cells
Fig. 4.55 
Diffuse large B-cell lymphoma with effaced nodal architecture in a diffuse pattern by scattered large cells showing pleomorphism
Fig. 4.56 
The large pleomorphic cells in diffuse large B-cell lymphoma with CD20 positivity
-
Subclassification:
-
GCB-type DLBCL : CD10 +, BCL6 +, multiple myeloma 1 (MUM1 )-
-
ABC-type DLBCL : CD10 -, BCL6 -, MUM1 +
-
-
Other types include double-hit or triple-hit HGBCL with rearrangements of MYC and BCL2 and/or BCL6 , and double-expresser HGBCL with immunostain of MYC (>40%) and BCL2 (>50%) but lack MYC and BCL2 chromosomal alteration.




Differential Diagnosis
-
Reactive lymph node
-
High-grade lymphoma and Hodgkin lymphoma
-
Melanoma
-
Carcinoma
-
Sarcoma
Burkitt Lymphoma (BL)
Clinical Features
-
Endemic BL, sporadic BL, and immunodeficiency-related BL.
-
Extranodal involvement frequent in the jaw, facial bone, abdominal organs, and breast.
-
EBV plays an important role in endemic BL.
-
Transcription factor 3 (TCF3) mutation in 40% of endemic BLs and 70% of sporadic BLs and immunodeficiency-related BLs.
Cytological Features (Fig. 4.57)
-
Cellular smear.
-
Monotonous population of medium-size lymphoid cells.
-
Usually smooth nuclear membrane, small notched or indented, may be seen.
-
Finely stippled nuclear chromatin.
-
Multiple conspicuous nucleoli.
-
Moderate amount, deeply basophilic cytoplasm with tiny vacuoles.
-
CD20 , CD10 , BCL6 positive.
-
All cases positive for the t(8;14) translocation, involving MYC .

Burkitt lymphoma with a monotonous population of medium-size lymphoid cells. Note the deeply basophilic cytoplasm with tiny vacuoles
Histologic Features
-
Effaced nodal architecture with a “starry sky” pattern and composed of sheets of neoplastic lymphocytes and scattered tingible-body histiocytes (Fig. 4.58)
Fig. 4.58 
Burkitt lymphoma with sheets of lymphoma cells admixed with histiocytes as a “starry sky” pattern
-
Neoplastic lymphocytes are medium in size with a round to slightly irregular nuclear contour and small nucleoli with a “snake head” appearance (Fig. 4.59).
Fig. 4.59 
Burkitt lymphoma cells with round nuclear contour and small nucleoli as a “snake head” appearance


Immunohistochemistry and Ancillary Studies
-
IHC: strongly positive for CD20 , CD10 , BCL6 , c-MYC and negative for BCL2 with proliferation rate of 100% by MIB-1 stain (Fig. 4.60)
Fig. 4.60 
Burkitt lymphoma cells with 100% of proliferation rate by Ki67 (MIB) immunohistochemical stain
-
FISH: MYC translocation (Fig. 4.61)
Fig. 4.61 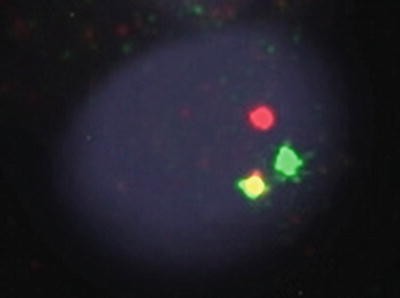
FISH in Burkitt lymphoma with MYC rearrangement (break-apart, 1R1G1F)
-
A subset lacking MYC rearrangement called “Burkitt-like lymphoma with 11q aberration” shows the same morphology and similar clinical course.


Differential Diagnosis
-
LBCL
-
Viral infection with reactive change
-
Lymphoblastic lymphoma
T-Cell Lymphoma
Clinical Features
-
Relatively uncommon lymphoid neoplasm, accounting for less than 12% of non-Hodgkin lymphomas , including peripheral T-cell lymphoma (PTCL), unspecified T-cell lymphoma, NK-cell lymphoma, ALCL , and nodal T-cell lymphoma with TFH phenotype
-
More common in Asia
Cytological Features (Fig. 4.62a, b)
-
Polymorphous population of a spectrum of small, medium, and large lymphocytes.
-
Convoluted nuclear membranes, vesicular or coarse chromatin, and prominent nucleoli.
-
Binucleation and multinucleation can be seen.
-
Cytoplasm ranging from scant to abundant, pale to basophilic.
-
Histiocytes, eosinophils, plasma cells and neutrophils can be seen.
-
Granulomas can be seen.

(a, b) T-cell lymphoma with a polymorphous population of a spectrum of small, medium, and large lymphocytes on Diff-Quik (a) and Pap stain (b)
Histologic Features
-
Effaced nodal architecture with perifollicular (T-cell zone) expansion (Fig. 4.63).
Fig. 4.63 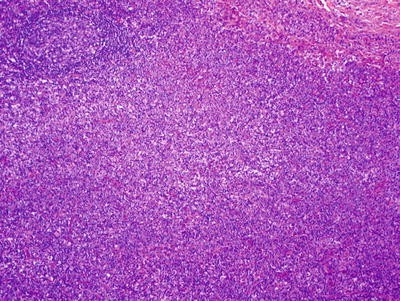
Peripheral T-cell lymphoma with effaced nodal architecture and perifollicular expansion
-
Neoplastic lymphocytes are medium in size with irregular nuclear contour, vesicular chromatin, and prominent nucleoli; they form sheets or a scattered pattern (Fig. 4.64).
Fig. 4.64 
Neoplastic T cells are medium in size with vesicular chromatin and nucleolus; there is a background of mature lymphocyte and scattered eosinophils


Immunohistochemistry and Ancillary Studies
-
Positive for, but often loss of one or more of, the T-cell markers CD2 , CD3 , CD5 and CD7 with either CD4 or CD8 .
-
Angioimmunoblastic T-cell lymphoma (Fig. 4.65) and two new subtypes – follicular center T-cell lymphoma and nodal PTCL with TFH type – show the follicular center markers CD279/programmed death 1 (PD1), CD10 , BCL6 , chemokine (C-X-C motif) ligand 13 (CXCL13), inducible T-cell co-stimulator (ICOS), serum amyloid P (SAP), and chemokine receptor type 5 (CCR5).
Fig. 4.65 
Angioimmunoblastic T-cell lymphoma with effaced nodal architecture and perifollicular expansion by monocytoid lymphocytes and capillary proliferation

Anaplastic Large Cell Lymphoma (ALCL )
Clinical Features
-
Three percent of adult non-Hodgkin lymphomas.
-
ALK+ ALCL represents 10–20% of childhood lymphomas; ALK- ALCL peaks in adults (40–65 years).
-
CD30 -positve T-cell lymphoma.
-
70–80% with t(2;5) translocation and ALK expression.
-
ALK-positive cases frequently involve both nodal and extranodal sites and have a better prognosis.
Cytological Features (Fig. 4.66a–d)
-
Cellular smear.
-
Pleomorphic cells with variable sizes.
-
Binucleation or multinucleation or bizarre cells can be seen.
-
Large nuclei with indentation and lobulation.
-
Variable amount of cytoplasm.
-
Heterogeneous population in the background, including small lymphoid cells, histiocytes, and plasma cells.
-
CD2 and CD4 are the more sensitive markers.
-
More than 75% of cases are negative for CD3 .
-
CD30 positive in all cases, usually in large lymphoid cells; most cases are positive for EMA .
-
Seventy percent of cases show ALK expression (either nuclear or cytoplasmic staining).
-
EBV is negative.

(a–d) Anaplastic large cell lymphoma with pleomorphic cells with variable sizes on Diff-Quik (a, b), cellblock (c), positive for CD30 (d)
Histologic Features
-
Effaced nodal architecture with expanded perifollicular areas (Fig. 4.67).
Fig. 4.67 
Anaplastic large cell lymphoma with effaced nodal architecture and perifollicular expansion
-
Neoplastic cells are pleomorphic and hallmark cells with horseshoe-like nucleus (Fig. 4.68).
Fig. 4.68 
Neoplastic T cells are pleomorphic and some with horseshoe-like nucleus – hallmark cells


Immunohistochemistry and Ancillary Studies
-
Positive for T-cell markers, CD30 (Fig. 4.69), and ALK1 (Fig. 4.70) and negative for CD15
Fig. 4.69 
Neoplastic T cells positive for CD30
Fig. 4.70 
Neoplastic T cells positive for ALK1
-
ALK1+ and ALK1- types share a similar molecular Janus kinase/signal transducer and activator of transcription 3 (JAK/STAT3 ) pathway.
-
New type: ALK-negative ALCL arising in association with breast implants shows similar morphological features, but neoplastic cells are confined to the seroma fluid without invasion of the capsule. Treatment is removal of the implant and capsule.


Differential Diagnosis
-
Hodgkin lymphoma
-
Other high-grade lymphoma
-
Carcinoma
-
Melanoma
-
Sarcoma
Hodgkin Lymphoma
Clinical Features
-
Cervical, mediastinal, or axillary mass
-
Bimodal age curve with a peak in young adults (15–35 years) and a second in the elderly
Cytological Features (Fig. 4.71a–h)
-
Low to moderate cellularity.
-
Polymorphous population of small lymphoid cells, plasma cells, histiocytes, and eosinophils.
-
Classic multinucleated Reed-Sternberg cells and mononuclear Hodgkin cells.
-
Fibrosis and crushed cellular components are frequently seen.
-
Excisional biopsy should be suggested for further classification.


(a–h) Hodgkin lymphoma with classic Reed-Sternberg cells and mononuclear or multinucleated Hodgkin cells in the background of a polymorphous population of small lymphoid cells, plasma cells, histiocytes, and eosinophils (a–e), and small tissue section (f), Hodgkin cells positive for CD15 (g), and CD30 (h)
Histologic Features
-
Effaced nodal architecture in a nodular or diffuse pattern with two types: CHL (nodular sclerosis, mixed cellularity, lymphocyte rich, and lymphocyte depleted) (Figs. 4.72a–d and 4.73a–c) and nodular lymphocyte-predominant Hodgkin lymphoma (NLPHL) (Figs. 4.74 and 4.75a–d)
Fig. 4.72 
(a–d) Classical Hodgkin lymphoma with nodular sclerosis (a), mixed cellularity (b), lymphocyte rich (c), and lymphocyte depleted (d)
Fig. 4.73 
(a–c) High-power view of classical Hodgkin lymphoma with Reed-Stenberg cells in a background of mixed lymphocytes, plasma cells, and eosinophils in nodular sclerosis and mixed cellularity (a), neoplastic cells with background of lymphocytes in lymphocyte-rich (b) and neoplastic cells with background of hypocellularity in lymphocyte depleted (c)
Fig. 4.74 
Nodular lymphocytic-predominant Hodgkin lymphoma with large nodular pattern
Fig. 4.75 
(a–d) Nodular lymphocytic-predominant Hodgkin lymphoma with scattered lymphocyte-predominant cells in a background of mature lymphocytes
-
Large neoplastic cells including Reed-Sternberg cells, Hodgkin cells, lacunar cells, and popcorn cells (Fig. 4.76a–d)
Fig. 4.76 
(a–d) Hodgkin lymphoma with Reed-Sternberg cells (a), Hodgkin cells (b), lacunar cells (c), and popcorn cells (d)





Immunohistochemistry and Ancillary Studies
-
Reed-Sternberg cells in CHL are positive for CD15 , CD30 , and K homology domain-containing protein overexpressed in cancer 1 (KOC1) (Fig. 4.77a–c) and negative for CD3 and CD20 .
Fig. 4.77 
(a–c ) Reed-Sternberg cells in classical Hodgkin lymphoma with positive CD15 (a), positive CD30 (b), and positive KOC1 (c)
-
NLPHL is a monoclonal B-cell neoplasm that is CD45 positive, CD20 positive, PAX5 positive, CD15 negative, and CD30 negative (Fig. 4.78a–e).
Fig. 4.78 
(a–e) Lymphocyte-predominant cells in nodular lymphocytic-predominant Hodgkin lymphoma with positive CD45 (a), positive CD20 (b), negative CD3 (c), negative CD15 (d), and negative CD30 (e)
-
Lymphocyte-rich CHL has features intermediate between CHL and NLPHL .


Differential Diagnosis
-
Poorly differentiated carcinoma
-
Melanoma
-
Sarcoma
-
Reactive lymph node with many immunoblasts
Others
Langerhans Cell Histiocytosis (LCH )
Cytological Features (Fig. 4.79a–e)
-
Langerhans histiocytes and eosinophils.
-
Nuclear grooves or linear folds are seen in Langerhans cells.
-
Immunostain shows positivity for both S100 and CD1a .
-
Multinucleated giant cells may be present.
-
Some of these neoplasms may have transdifferentiation to follicular lymphoma, CLL, B- or T-lymphoblastic neoplasms carrying the same IGHV, or T-cell receptor (TCR) gene rearrangement.

(a–e) Langerhans cell histiocytosis with Langerhans histiocytes and eosinophils in (a) and (b), prominent nuclear grooves or linear folds seen in Langerhans histiocytes (c), on cellblock (d) and positive for CD1a (e)
Histologic Features
-
Effaced nodal architecture with expanded sinus and pericortex by large neoplastic Langerhans cells
-
In early stage, Langerhans cells prominent admixed with eosinophils and neutrophils; in late stage, the number of Langerhans cells is decreased with fibrosis and increased foamy macrophages.
Myeloid Sarcoma
Cytological Features (Fig. 4.80a–e)
-
Myeloid cells in various stages of differentiation
-
Can be mainly blasts or a mixed population of myeloid cells in different stages
-
Eosinophilic myelocytes may be seen.

(a–e) Myeloid sarcoma on Diff-Quik (a, b), Pap stain (c), positive for CD34 (d) and CD43 (e) on cellblock sections
Histologic Features
-
Effaced nodal or tissue architecture with sheets of myeloblasts (Figs. 4.81 and 4.82), rarely, of erythroid precursors or megakaryoblasts
Fig. 4.81 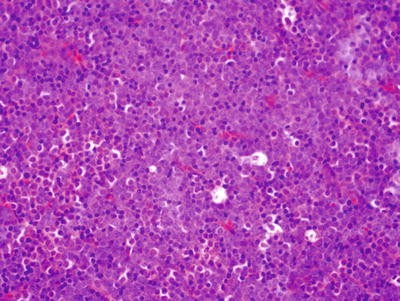
Myeloid sarcoma with sheets of blasts
Fig. 4.82 
Myeloblasts with fine chromatin, round nuclear contour, and frequent mitotic figures
-
May present de novo, with peripheral and bone marrow involvement, relapse of acute myeloid leukemia (AML) or progression of a prior myelodysplastic syndrome (MDS), myeloproliferative neoplasm (MPN), or MDS/MPN. Recommend clinical correlation.


Immunohistochemistry and Ancillary Studies
-
Myeloblasts positive for myeloperoxidase (MPO , Fig. 4.83), CD117 , lysozyme (Fig. 4.84), CD68 , CD99, and CD34
Fig. 4.83 
Myeloblasts with positive myeloperoxidase
Fig. 4.84 
Myeloblasts with positive lysozyme


Lymphoblastic Lymphoma
Clinical Features
-
A childhood disease
-
90% precursor T-lymphoblastic cells and 10% precursor B lymphoblastic cells.
-
A designation of lymphoma is given when a patient presents as a mass lesion and less than 25% blasts in bone marrow.
-
T-lymphoblastic lymphoma frequently present with a mediastinal mass.
-
Indolent T-lymphoblastic proliferation may mimic T-lymphoblastic lymphoma. It typically involves lymphoid tissue of the upper aerodigestive tract without systemic dissemination and also no clonality detected.
Cytological Features (Fig. 4.85a–c)
-
Cellular smear
-
Relatively uniform population of medium-size lymphoid cells
-
Fine, delicate, and powdery nuclear chromatin
-
Small to conspicuous nucleoli
-
Nuclear membrane variable from smooth to convoluted
-
Scant to small amount of cytoplasm
-
Cytoplasmic vacuoles can be seen

(a–c) Lymphoblastic lymphoma with relatively uniform population of medium-size lymphoid cells, with fine, delicate, and powdery nuclear chromatin on Diff-Quik (a, b) and Pap stain (c)
Histologic Features
-
Effaced nodal architecture with sheets of blasts (Fig. 4.86) and may have a “starry sky” pattern.
Fig. 4.86 
Lymphoblastic lymphoma with effaced nodal architecture in a diffuse pattern by sheets of neoplastic cells
-
Neoplastic cells are medium in size with vesicular chromatin and small nucleolus (Fig. 4.87).
Fig. 4.87 
Neoplastic cells with round nuclear contour, vesicular chromatin, and small nucleoli; in a background of mature lymphocytes and eosinophils
-
New type: Early T-precursor (ETP) lymphoblastic leukemia shows blasts positive for CD2 , CD7 , cytoplasmic CD3 , and CD4 and negative for CD1a , CD5 (or weak expression) and CD8 with one or more of the myeloid/stem cell markers CD34 , CD117 , CD13, CD33, CD11b, or CD65 (Figs. 4.88 and 4.89a, b). It has a very poor outcome.
Fig. 4.88 
Flow cytometry studies of lymphoblast positive for cCD3 and CD34 , and low intensity of CD5 and negative for sCD3, CD8 , and MPO (a few blasts expressing MPO in low intensity) with aberrant expression of CD33
Fig. 4.89 
Neoplastic cells positive for cCD3 (a) and negative for CD1a (b)
-
New provisional entity: Indolent T-lymphoblastic proliferation belongs to nonneoplastic entity and may mimic T-lymphoblastic lymphoma. IHC: TdT +, no aberrant phenotype, and not clonal. It mostly occurs in lymphoid tissue of upper aerodigestive tract with good prognosis.




Immunohistochemistry and Ancillary Studies
-
Terminal deoxynucleotidyl transferase (TdT )-positive in both T and B lymphoblasts.
-
T lymphoblasts are positive for CD7 and cytoplasmic CD3 with coexpression of CD4 and CD8 and also positive for other T-cell markers, such as CD1a and CD2 .
-
B lymphoblasts are positive for CD19, CD79a , CD10 , and CD34 .
Tumors Mimicking Lymphomas
Melanoma
Cytological Features
-
Loosely cohesive groups and single cells
-
Binucleation and multinucleation
-
Intranuclear inclusions
-
Plasmacytoid cells with abundant cytoplasm
-
Prominent nucleoli
-
Dusty pigments
Small Cell Undifferentiated Carcinoma
Cytological Features
-
Cohesive and single neoplastic cells.
-
Very high nuclear-to-cytoplasmic ratio.
-
Neuroendocrine chromatin.
-
Inconspicuous nucleoli.
-
Single cell necrosis and many mitosis.
-
Blue bodies in the background may resemble lymphoglandular bodies.
Undifferentiated Carcinoma
-
Nasopharyngeal carcinoma
-
Poorly differentiated squamous cell carcinoma
-
Basaloid squamous cell carcinoma
-
Merkel cell carcinoma
Small Round Cell Tumors
-
Rhabdomyosarcoma
-
Ewing’s sarcoma /primitive neuroectodermal tumor (PNET)
-
Neuroblastoma
-
Desmoplastic small round cell tumor
Seminoma
Cytological Features
-
Two populations of cells: large neoplastic tumor cells and small benign lymphoid cells.
-
The neoplastic cells are large and relatively uniform in size.
-
Single prominent nucleoli.
-
Cytoplasmic vacuoles can be seen.
Thymoma
Cytological Features
-
Two populations of cells: epithelial cells and lymphoid cells.
-
Can be predominately lymphoid cells.
-
Lymphoid cells are CD3 -positve and TdT -positive cortical thymocytes.
-
Epithelial cells are positive for p63.




Abbreviations List
Abbreviation | Full text |
|---|---|
ABC | Activated B-cell |
ABL | Abelson murine leukemia viral oncogene homolog 1 |
ALCL | Anaplastic large cell lymphoma |
ALK | Anaplastic lymphoma kinase |
ALL | Acute lymphoblastic leukemia |
AML | Acute myeloid leukemia |
B-ALL | B-cell acute lymphoblastic leukemia |
BCL | B-cell lymphoma (BCL1, BCL2, BCL6) |
BCR | Breakpoint cluster region |
BL | Burkitt lymphoma |
BM | Bone marrow |
BOB1 | B-cell Oct binding protein 1 |
BRAF | v-raf murine sarcoma viral oncogene homolog B1 |
CARD11 | Caspase recruitment domain-containing protein 11 |
cCD3 | Cytoplasmic CD3 |
CCND1 | Cyclin D1 |
CCR5 | Chemokine receptor type 5 |
CD | Cluster of differentiation |
CHL | Classical Hodgkin lymphoma |
CLL | Chronic lymphocytic leukemia |
CNS | Central nervous system |
CT | Computed tomography |
CXCL13 | Chemokine (C-X-C motif) ligand 13 |
DLBCL | Diffuse large B-cell lymphoma |
EBV | Epstein-Barr virus |
EMA | Epithelial membrane antigen |
ETP | Early T precursor |
ETV6 | ETS variant 6 |
EZH2 | Enhancer of zeste homolog 2 |
FISH | Fluorescence in situ hybridization |
FL | Follicular lymphoma |
FMC7 | A monoclonal antibody and an epitope of CD20 |
FNA | Fine needle aspiration |
GC | Germinal center |
GI | Gastrointestinal |
GNA13 | Guanine nucleotide-binding protein subunit alpha-13 |
HGBCL | High-grade B-cell lymphoma |
HHV8 | Human herpes virus 8 |
HPF | High-power field |
iAMP2 | Intrachromosomal amplification of chromosome 21 |
ICOS | Inducible T-Cell co-stimulator |
IgG/A | Immunoglobulin G/A |
IGH | Immunoglobulin heavy chain |
IGHV | Immunoglobulin heavy-chain variable |
IgM | Immunoglobulin M |
IHC | Immunohistochemistry |
IL3 | Interleukin 3 |
IRF4 | Interferon regulatory factor 4 |
IRTA1 | Immunoglobulin superfamily receptor translocation associated 1 |
JAK/STAT3 | Janus kinase/signal transducer and activator of transcription |
KMT2A | Lysine methyltransferase 2A |
KOC1 | K homology domain-containing protein overexpressed in cancer |
L256P | Leucine to proline mutation at amino acid position 256 |
LBCL | Large B-cell lymphoma |
LCH | Langerhans cell histiocytosis |
LEF1 | Lymphoid enhancer-binding factor 1 |
LMO2 | LIM-only transcription factor-2 |
LN | Lymph node |
LPL | Lymphoplasmacytic lymphoma |
MALT | Mucosa-associated lymphoid tissue |
MCL | Mantle cell lymphoma |
MDS | Myelodysplastic syndrome |
MGUS | Monoclonal gammopathy of undetermined significance |
MIB-1 | Mindbomb homolog 1 |
MLL | Mixed-lineage leukemia |
MPN | Myeloproliferative neoplasm |
MPO | Myeloperoxidase |
MUM1 | Multiple myeloma 1 |
MYC/c-MYC | A regulator gene that codes for a transcription factor |
MYD88 | Myeloid differentiation primary response gene 88 |
MZL | Marginal zone lymphoma |
N/C | Nuclear to cytoplasmic |
NK | Natural killer |
NOS | Not otherwise specified |
NPM | Nucleophosmin |
Oct2 | Octamer-binding transcription factors |
Pap | Papanicolaou |
PAX | Paired box gene |
PB | Peripheral blood |
PBX1 | Pre-B-cell leukemia homeobox 1 |
PD1 | Programmed death 1 |
PNET | Primitive neuroectodermal tumor |
PTCL | Peripheral T-cell lymphoma |
PTLD | Posttransplant lymphoproliferative disorders |
RUNX1 | Rnt-related transcription factor 1 |
SAP | Serum amyloid P |
sCD3 | Surface CD3 |
SLL | Small lymphocytic lymphoma |
SOX | Sex-determining region Y box |
STAT3 | Signal transducer and activator of transcription 3 |
T-ALL | T-cell acute lymphoblastic leukemia |
TCF3 | Transcription factor 3 |
TCR | T-cell receptor |
TdT | Terminal deoxynucleotidyl transferase |
TFH | T follicular helper |
TIA | T-cell intracellular antibody |
TNFAIP3 | Tumor necrosis factor, alpha-induced protein 3 |
US, USA | United States (not spelled out in chapter) |
WHO | World Health Organization |
ZAP-70 | Zeta-chain-associated protein kinase 70 |
Notes
- 1.
Changes from the 2008 classification.
Provisional entities are listed in italics.
- 2.
See footnote 2.
- 3.
See footnote 2.
- 4.
See footnote 2.
- 5.
See footnote 2.
- 6.
See footnote 2.
References
Alikhan M, Song JY, Sohani AR, Moroch J, Plonquet A, Duffield AS, et al. Peripheral T-cell lymphomas of follicular helper T-cell type frequently display an aberrant CD3−/dimCD4+ population by flow cytometry: an important clue to the diagnosis of a Hodgkin lymphoma mimic. Mod Pathol. 2016;29:1173–82.
Arber DA, Orazi A, Hasserjian R, Thiele J, Borowitz MJ, Le Beau MM, et al. The 2016 revision to the World Health Organization classification of myeloid neoplasms and acute leukemia. Blood. 2016;127(20):2391–405.
Arcaini L, Rossi D, Paulli M. Splenic marginal zone lymphoma: from genetics to management. Blood. 2016;127(17):2072–81.
Berndt SI, Skibola CF, Joseph V, Camp NJ, Nieters A, Wang Z, et al. Genome-wide association study identifies multiple risk loci for chronic lymphocytic leukemia. Nat Genet. 2013;45(8):868–76.
Bigras G, Dong WF, Canil S, Lai R, Morel D, Swanson PE, et al. New MYC IHC classifier integrating quantitative architecture parameters to predict MYC gene translocation in diffuse large B-cell lymphoma. Appl Immunohistochem Mol Morphol. 2016.; Epub 2016 May 20.
Bob R, Falini B, Marafioti T, Paterson JC, Pileri S, Stein H. Nodal reactive and neoplastic proliferation of monocytoid and marginal zone B cells: an immunoarchitectural and molecular study highlighting the relevance of IRTA1 and T-bet as positive markers. Histopathology. 2013;63(4):482–98.
Bogusz AM, Bagg A. Genetic aberrations in small B-cell lymphomas and leukemias: molecular pathology, clinical relevance and therapeutic targets. Leuk Lymphoma. 2016;27:1–23.
Burotto M, Berkovits A, Dunleavy K. Double hit lymphoma: from biology to therapeutic implications. Expert Rev Hematol. 2016:1–10.
de Jonge AV, Roosma TJ, Houtenbos I, Vasmel WL, van de Hem K, de Boer JP, et al. Diffuse large B-cell lymphoma with MYC gene rearrangements: current perspective on treatment of diffuse large B-cell lymphoma with MYC gene rearrangements; case series and review of the literature. Eur J Cancer. 2016;55:140–6.
DeMay RM. Lymph node. In:The art and science of cytopathology. 2nd ed. Chicago: ASCP Press; 2010. p. 966–1028.
Dunleavy K. Aggressive B cell lymphoma: optimal therapy for MYC-positive, double-hit, and triple-hit DLBCL. Curr Treat Options in Oncol. 2015;16(12):58.
Dyhdalo KS, Lanigan C, Tubbs RR, Cook JR. Immunoarchitectural patterns of germinal center antigens including LMO2 assist in the differential diagnosis of marginal zone lymphoma vs follicular lymphoma. Am J Clin Pathol. 2013;140(2):149–54.
Falini B, Agostinelli C, Bigerna B, Pucciarini A, Pacini R, Tabarrini A, et al. IRTA1 is selectively expressed in nodal and extranodal marginal zone lymphomas. Histopathology. 2012;61(5):930–41.
Freedman A. Follicular lymphoma: 2015 update on diagnosis and management. Am J Hematol. 2015;90(12):1171–8.
Ioachim HL, Medeiros LJ, editors. Ioachim’s lymph node pathology. 4th ed. Philadelphia: Lippincott William & Wilkins; 2009. p. 1–291.
Jain N, Lamb AV, O'Brien S, Ravandi F, Konopleva M, Jabbour E, et al. Early T-cell precursor acute lymphoblastic leukemia/lymphoma (ETP-ALL/LBL) in adolescents and adults: a high-risk subtype. Blood. 2016;127(15):1863–9.
Karnik T, Ozawa MG, Lefterova M, Luna-Fineman S, Alvarez E, Link M, et al. The utility of IgM, CD21, HGAL and LMO2 in the diagnosis of pediatric follicular lymphoma. Hum Pathol. 2015;46(4):629–33.
Menter T, Dirnhofer S, Tzankov A. LEF1: a highly specific marker for the diagnosis of chronic lymphocytic B cell leukaemia/small lymphocytic B cell lymphoma. J Clin Pathol. 2015a Jun;68(6):473–8.
Menter T, Gasser A, Juskevicius D, Dirnhofer S, Tzankov A. Diagnostic utility of the germinal center-associated markers GCET1, HGAL, and LMO2 in hematolymphoid neoplasms. Appl Immunohistochem Mol Morphol. 2015b;23(7):491–8.
Nakashima MO, Durkin L, Bodo J, Lin J, Quintanilla-Martinez L, Fu K, et al. Utility and diagnostic pitfalls of SOX11 monoclonal antibodies in mantle cell lymphoma and other lymphoproliferative disorders. Appl Immunohistochem Mol Morphol. 2014;22(10):720–7.
Swerdlow SH. Diagnosis of 'double hit' diffuse large B-cell lymphoma and B-cell lymphoma, unclassifiable, with features intermediate between DLBCL and Burkitt lymphoma: when and how, FISH versus IHC. Hematology Am Soc Hematol Educ Program. 2014;2014(1):90–9.
Swerdlow SH, Campo E, Pileri SA, Harris NL, Stein H, Siebert R, et al. The 2016 revision of the World Health Organization classification of lymphoid neoplasms. Blood. 2016a;127(20):2375–90.
Swerdlow SH, Campo E, Pileri SA, Harris NL, Stein H, Siebert R, et al. WHO classification of tumours of hematopoietic and lymphoid tissues. 4th ed. Lyon: IARC; in press; expected Spring 2017.
Swerdlow SH, Kuzu I, Dogan A, Dirnhofer S, Chan JK, Sander B, et al. The many faces of small B cell lymphomas with plasmacytic differentiation and the contribution of MYD88 testing. Virchows Arch. 2016b;468(3):259–75.
Tandon B, Peterson L, Gao J, Nelson B, Ma S, Rosen S, et al. Nuclear overexpression of lymphoid-enhancer-binding factor 1 identifies chronic lymphocytic leukemia/small lymphocytic lymphoma in small B-cell lymphomas. Mod Pathol. 2011;24(11):1433–43.
Vose JM. Mantle cell lymphoma: 2015 update on diagnosis, risk-stratification, and clinical management. Am J Hematol. 2015;90(8):739–45.
Zhang YH, Liu J, Dawlett M, Guo M, Sun X, Gong Y. The role of SOX11 immunostaining in confirming the diagnosis of mantle cell lymphoma on fine-needle aspiration samples. Cancer Cytopathol. 2014;122(12):892–7.
Zucca E, Bertoni F. The spectrum of MALT lymphoma at different sites: biological and therapeutic relevance. Blood. 2016;127(17):2082–92.
Author information
Authors and Affiliations
Rights and permissions
Copyright information
© 2018 Springer International Publishing AG
About this chapter
Cite this chapter
Zhang, X.(., Lin, F. (2018). Lymph Nodes. In: Handbook of Practical Fine Needle Aspiration and Small Tissue Biopsies. Springer, Cham. https://doi.org/10.1007/978-3-319-57386-1_4
Download citation
DOI: https://doi.org/10.1007/978-3-319-57386-1_4
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-57384-7
Online ISBN: 978-3-319-57386-1
eBook Packages: MedicineMedicine (R0)