
Abstract
The paper presents the results of clinical trials using dynamic hip screw (DHS) for the treatment of fractures of the proximal femur and the results of numerical simulation of the model of femoral fixation using stabilizer DHS for the fixations most commonly occurring in clinical cases. The simulation results constituted the basis for the selection of mechanical properties and allowed to define the zones most vulnerable to mechanical failure of both the implant and bone tissue. Furthermore, designated zones of maximum stress enable the identification and assessment of corrosion processes in the areas of the damaged surface layer of the metal biomaterial.
Access provided by CONRICYT-eBooks. Download conference paper PDF
Similar content being viewed by others


Keywords
- Dynamic hip screw
- DHS
- Finite element analysis
- Treatment of proximal femoral fracture
- Treatment of intertrochanteric fracture
- Osteoporosis
1 Introduction
Majority of proximal femur fractures occur among the elderly as a result of low-energy trauma - e.g. fall from own height (fall from stending height or less). Less fractures of this type is caused by high energy trauma or neoplastic lesions. In Poland, every year, there are around 16–20 thousand inter- or pertrochanteric fractures. Most of the cases involve older patients with more severe osteoporosis than in the case of femoral neck fractures [1, 2]. According to the literature, over 50 years old the incidence of fractures of the proximal femur doubles every 6 years. Because of the concomitant osteoporosis fractures are more likely to occur among women than men. Fracture of the proximal femur is one of the most dangerous complications of osteoporosis. It is associated with high mortality (fracture of the femoral neck - approximately 8–11 %), what is more leads to temporary or permanent loss of independence. Risk factors of proximal femur fractures include: age, sex, alcohol abuse, rheumatoid arthritis, impaired ability to walk, impaired brain function, dementia, use of psychotropic drugs and peripheral neuropathies [1–6]. The aim of the surgical treatment of trochanteric fractures is stable fixation, restoration of limb function and as soon as possible walking, which protects against general and local complications [1, 2]. One of the methods used for osteosynthesis of proximal femur fractures, including the treatment of femoral neck fractures and intertrochanteric fractures is DHS (Dynamic Hip Screw) also known as Sliding Screw Fixation. DHS method includes three components: appropriate lenght lag screw (inserted into the neck of the femur) which is connected with sideplate and cortical screws (fixated into the proximal femoral shaft corticales). It is recommended to insert lag screw in longitudinal axis of femoral neck approx. 10 mm below bony surface of the femoral head. Rotational stabilization is achieved by introducing lag screw into sideplate (with special internal antirotational notch). Mechanism of dynamic osteosynthesis is a result of possible movement of lag screw into sleeve of sideplate. To carry out such a procedure it is necessary to have adequate instruments and variety of implants (screws and plates) of different geometry and size [1, 2]. Biomechanical numerical analysis preceding implantation of the stabilizing system performed to determine the state of displacements and stresses occurring in the implant during the stabilization and in bones, and on the implant - bone interface is important due to the selection of biomechanical characteristics of the stabilizer and metal biomaterial, and modification of the surface layer structure of applied implants [7–13]. On the basis of the literature review, it may be said that the authors [14–19] attempt at the numerical analysis of the system: femur - dynamic hip screw system (DHS). In each case, the simulated fracture was an intertrochanteric fracture. The results of their analyses are based on the models of various degrees of simplification: from very simple models in which the plate is fixed with four screws [16] (made as one element), to sophisticated models with up to eight screws presented as separate elements [19]. However, in all of the cases, there is a simplification that the bolts are not threaded and the diameter of the cortical screws and thread geometry are not taken into consideration. The analyses resulted in determining the values of displacements, von Misses strains and stresses. Taking into consideration the simplifications applied by other authors, the study involved the biomechanical analysis using finite element method supplemented by clinical observations. DHS screw of thread diameter equal to \(G = 12.5\) mm (standard DHS screw used for cancellous healthy bone), and standard cortical screws of \(BS = 4.5\) mm diameter were used. The analysis was performed for the most frequent DHS fixations with the use of the plate intended for use with three cortical screws.
2 Materials and Methods
2.1 Clinical Studies
422 patients between years 2009–1013 were treated because of intertrochanteric fracture in the Janusz Daab Provincial Hospital of Orthopaedics and Traumatology in Piekary Śląskie. Clinical and radiological outcomes were analyzed. 369 patients were treated with open reduction and internal fixation with DHS method. Patients group consists of 272 (73.7 %) women and 97 (26.3 %) men. The average age of all treated patients was 78.4 years (mean age of women - \(73\pm 26\) years, men - \(60\pm 37\) years. The structure of patients gender, age, circumstances of the injury, time, method and results of treatment were analyzed.
2.2 FEM Analysis
Numerical simulation of loading of the femoral fixation model, with the use of dynamic hip screw DHS, was performed in Ansys Workbench 15 environment. The fixation of intertrochanteric femoral fractures of the type I according to the classification of trochanteric fractures of femur by Evans and Jensen modifications was analyzed [20]. Preliminary tests included evaluation of a non-fractured femur. The generated finite element mesh (element type SOLID 187) was characterized by the skewness parameter of mean value equal to \(0.4 \pm 0.2\) providing its good match to the geometry of the analyzed system. The geometric model of the femur was prepared in the Mimics Innovation Suite software based on CT images with the following parameters: The size of the pixel in the lateral plane: 0.684 mm, The imaging field width: 171.68 mm, Distance between sections: 1.5 mm, The number of sections: 331. In order to segment bones, thresholding operation was performed with the lower threshold value of 226HU and upper threshold value of 1613HU. It included both the cortical and the cancellous part of the femur. In the numerical analysis the DHS system was analyzed. The geometry of the system has been commonly used in the Provincial Hospital of Orthopaedics and Traumatology in Piekary Śląskie. The fixation was performed using the DHS plate of neck length of \(Ls = 38\) mm, plate length of \(L = 105\,\)mm and the angle \(135^{\circ }\). DHS screws with a thread diameter \(G = 12.5\) mm and three cortical screws of diameter \(BS = 4.5\) mm were used. The width of the fracture gap was \(d = 0.2\,\)mm. A callus forming in the gap was simulated. In order to perform numerical calculations, the mechanical properties shown in Table 1 were assumed.
On the basis of the developed geometric models, numerical models were prepared. Because of the complex shapes and in particular the threads of the cortical screws and the irregular geometry of the bone, in order to reduce the number of finite elements and speed up the calculations a simplification omitting the threads in the cortical screws, as in works [14–19] was done. However, the thread of the DHS screw was taken into account in the analyses. The following were assumed for the needs of the analysis:
-
distal part of femur was immobilized by depriving the nodes situated along the plane of all the freedom degrees,
-
the bone was loaded following Będziński model [23].
The values of forces assumed for the test corresponded to peak values reached when carrying a load with one limb by a walking person of 70 kg bodyweight - Table 2.
Furthermore, friction between the thread of the DHS bolt and the cancellous bone in the femoral head was assumed. An asymmetric friction coefficient of \(\eta = 0.3\) [15, 17] was assumed. The contacting surfaces were described as automatically adjusting to one another, and the calculations were made with Augmented Lagrange equations. Friction contact and geometry correction corresponding to M4 thread geometry were also applied between the compressive bolt and the DHS bolt. In the remaining contact areas between the elements of the DHS system and the model femur, a standard bonded contact was applied in order to simulate the connections between the cortical screws and the bone, and between the DHS plate and the bone. The stresses and strains obtained in the analysis are the values reduced in accordance with the Huber–Hencky–von Misses theory.
3 Results and Discussion
3.1 Clinical Studies
Hip fractures occurred as a result of fall from own height (standing height or less) in 325 (88.1 %) patients; as a result of other circumstances in 41 (11.1 %) patients, including fall from a higher altitude, e.g. ladders, chairs, stairs, roof, scaffolding, etc. 3 (0.8 %) patients had a traffic accident. 309 (83.7 %) reported to the hospital immediately after the injury, 30 (8.13 %) patients reported within 48 h after injury, 30 (8.13 %) more than 48 h after injury. In the Emergency Room after diagnosis in 237 (64.2 %) patients proximal tibial skeletal traction was applied, 132 (35.8 %) patients did not have skeletal traction. In 70 (19 %) patients underwent surgery immediately after admission, 59 (16 %) patients had surgery on the next day. 240 (65 %) patients had surgery later due to additional general conditions, other diseases or need to perform additional tests and consultations. Among analyzed cases 12.5 mm diameter DHS lag screw was used. The shortest lag screw length used was \(60\,\)mm, the longest - 135 mm (average - 94.24 mm). Side-plate used for surgery had angle of 135\(\circ \), 2 to 12 hole (average 3.75) with cortical screws 4.5 mm diameter and a length adapted to the anatomical characteristics of the femur. In 4 (1,1 %) cases 2 holes plate was used, 3-hole - in 174 cases (47.2 %), 4-hole - 133 (36 %), 5-hole - 13 (3.5 %), 6-hole - 14 (3.8 % ), 8-hole - 4 (1.1 %), 10-hole - 5 (1.4 %), 12-hole - 1 (0.3 %). Compression screw was used in 287 cases (77.8 %). Additional stabilization devices were necessary in 28 (7.6 %) patients (metal loops, spongy and cortical screws). 176 (47.7 %) patients who underwent surgical treatment in outpatient clinic control showed complete radiographic bone union. This group consisted of 129 women (47.4 %) and 47 men (48.5 %). 94 (25.5 %) patients did not report at all for clinical control after surgery. In the group of patients treated with 2-hole plate bone union was achieved in 2 (50 %) cases, 3-hole - 78 (44.8 %), 4-hole - 69 (51.9 %), 5-hole - 8 (61.5 %), 6-hole - 4 (28.6 %), 8-hole - 3 (75 %), 10-hole - 4 (80 %), 12-hole - 1 (100 %).
3.2 FEM Analysis
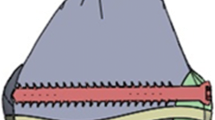
The results of the analysis of the displacements, von Misses strains and equivalent stress for all femur - DHS system models are presented in Table 3 and Fig. 1.

Stress distribution in DHS system and femur elements, MPa
In the presented work taking into account the results of the clinical evaluation of the DHS stabilizer the numerical analysis of the DHS system with three cortical screws with a diameter of 4.5 mm was performed. The DHS stabilizer was placed in the femur in accordance with the recommendations of the implantation technique. Placement of the implant corresponded to the one used in the Provincial Hospital of Orthopaedics and Traumatology in Piekary Śląskie and at the same time was in accordance with the works [15, 17]. Calculations were carried out for bone models both non-fractured and with the intertrochanteric fracture. For the non-fractured model of the femur, wherein the implant was not used, a displacement of the proximal section of the femur \(L = 6.5\) mm was observed, which resulted in stresses in the cortical bone equal to \(\sigma = 34\) MPa. The values of displacements of the femur - DHS stabilizer system were higher than those obtained for the non-fractured bone and were equal to \(L = 7.9\) mm. Reduction in stiffness of bone after use of the DHS with three cortical screws can contribute to a reduction of treatment efficiency (44.8 % of full bone union according to clinical trials) compared to stabilization using more cortical screws for example 5 - 61.5 % efficiency. The results indicate that in the analyzed model, the maximum stress do not exceed the yield strength of the metal biomaterial - Table 3. Furthermore, the strength of both cortical and cancellous bone was not exceeded as well. The maximum stresses in the parts of the stabilizer were observed in the contact zones between the DHS screw and the neck of the DHS plate and cortical screw slots of the DHS plate. Furthermore, in the cortical screws an accumulation of stress in the transition zone between the shaft to the head was observed - Fig. 1. Taking into account the results of the analysis can be concluded that for the implant made of the austenitic stainless steel results obtained by authors [14–19, 24] are similar, and on this basis threats related to the application of the DHS system in intertrochanteric femur fractures can be concluded. Maximum stress areas are vulnerable to mechanical failure of the implant, leading to its destruction. At the same time damage of passive layer in the contact zones may lead to initiation of corrosion processes. These zones will be exposed to the initiation and development of crevice, pitting and fatigue corrosion [24].
4 Conclusion
On the basis of the performed treatment analyses of intertrochanteric fractures stabilized with the DHS system in the Provincial Hospital of Orthopaedics and Traumatology in Piekary Śląskie in 2009–2013 it can be concluded that:
-
pertrochanteric fractures occur more often among older females and are a result of low Energy trauma,
-
DHS system is the most often used implant for trochanteric fractures stabilization in the hospital,
-
DHS osteosynthesis is an effective method of treatment,
-
better results of DHS surgical treatment were observed among men than women.
Moreover, summarizing the numerical analysis of displacements and stresses in the elements of the DHS dynamic hip stabilizer, in particular taking into account the stresses in the femoral shaft and cancellous bone, one can conclude that the maximum stress in the analyzed models do not exceed the assumed yield strength of the biomaterial \(R_{p0.2} = 690\) MPa and the established compression strength of bone \(R_c = 180\) MPa. The analysis allows the determination of potentially dangerous areas, vulnerable to damage due to overload. Furthermore, the analysis identifies the areas of initiation and development of crevice, pitting and fatigue corrosion.
References
Canale, T.S., Beaty, J.H.: Campbellś Operative Orthopaedics, 12nd edn. Chapter 1: 58–59, Chapter 55: 2725–2776 (2013)
Standard, J.P., Schmidt, A.H., Kregor, P.O.: Leczenie operacyjne obrażeń narządu ruchu. wyd.1, 2010, tom.3, rozdział 23 (in Polish)
Kenzora, J.E., McCarthy, R.E., Lowell, O.D., Sledge, C.B.: Hip fracture mortality: relation to age, treatment preoperative illness, time of surgery and complications. Clin. Orthop. Relat. Res. 186, 45–56 (1984)
Ring, P.A.: Treatment of trochanteric fractures of the femur. Br. Med. J. 1(5331), 654–656 (1963)
McNeill, D.H.: Hip fractures: influence of delay in surgery on mortality. Wis. Med. J. 74(12), 129–138 (1975)
Griffiths, R., Alper, J., Beckingsale, A., Goldhill, D., Heyburn, G., Holloway, J., Leaper, E., Parker, M., Ridgway, S., White, S., Wiese, M., Wilson, I.: Management of proximal femoral fractures 2011 Association of Anaesthetists of Great Britain and Ireland. Anaesthesia 67(1), 85–98 (2012)
Özkan, A., Atmaca, H., Mutlu, İ., Çelik, T., Uğur, L., Kiioğlu, Y.: Stress distribution comparisons of foot bones in patient with tibia vara: a finite element study. Acta Bioeng. Biomech. 15(4), 67–72 (2013). doi:10.5277/abb130409
Świeczko-Źurek, B., Serbiński, W., Szumlański, A.: Analisys of the failure of fixator used in bone surgery. Adv. Mater. Sci. 8(2), 84–88 (2008)
Ziębowicz, A., Bączkowski, B.: Numerical analysis of the implant – abutment system. In: Piętka, E., Kawa, J. (eds.) ITIB 2012. LNCS, vol. 7339, pp. 341–350. Springer, Heidelberg (2012)
Kajzer, W., Kajzer, A., Gzik-Zroska, B., Wolański, W., Janicka, I., Dzielicki, J.: Comparison of numerical and experimental analysis of plates used in treatment of anterior surface deformity of chest. In: Piętka, E., Kawa, J. (eds.) ITIB 2012. LNCS, vol. 7339, pp. 319–330. Springer, Heidelberg (2012). doi:10.1007/978-3-642-31196-3_32
Szewczenko, J., Pochrząst, M., Walke, W.: Evaluation of electrochemical properties of modified Ti–6Al–4V ELI alloy. Przeglad Elektrotechniczny 87(12b), 177–180 (2011)
Basiaga, M., Jendruś, R., Walke, W., Paszenda, Z., Kaczmarek, M., Popczyk, M.: Influence of surface modification on properties of stainless steel used for implants. Arch. Metall. Mater. 60(4), 2965–2969 (2015)
Walke, W., Paszenda, Z., Basiaga, M., Karasinski, P., Kaczmarek, M.: EIS study of SiO\(_2\) oxide film on 316L stainless steel for cardiac implants. In: Piętka, E.,; Kawa, J., Wieclawek, W. (eds.) Information Technologies in Biomedicine, vol. 4. Book Series: Advances in Intelligent Systems and Computing, vol. 284, pp. 403–410 (2014)
Hrubina, M., Skotak, M., Behounek, J.: Complications of dynamic hip screw treatment for proximal femoral factures. Acta Chir. Orthop. Traumatol. Cachoslovaca 77, 140–142 (2010)
Horák, Z., Hrubina, M., Dzupa, V.: Biomechanical analyses of proximal femur osteosynthesis by DHS system. Bull. Appl. Mech. 7(27), 60–65 (2011)
Taheri, N.S., Blicblau, A.S., Singh, M.: Effect of different load conditions on a DHS implanted human femur. Int. J. Eng Technol. 1(1), 141–146 (2012)
Hrubina, M., Horák, Z., Bartoška, R., Navrátil, L., Rosina, J.: Computational modeling in the prediction of Dynamic Hip Screw failure in proximal femoral fractures. J. Appl. Biomed. 11, 143–151 (2013)
Rooppakhun, S., Chantarapanich, N., Chernchujit, B., Mahaisavariya, B., Sucharitpwatskul, S., Sitthiseripratip, K.: Mechanical evaluation of dynamic hip screwfor trochanteric fracture. Int. Sch. Sci. Res. Innov. 4(9), 576–579 (2010)
Siamnuai, K., Rooppakhun, S.: Influence of plate length on the mechanical performance of dynamic hip screw. IACSIT Press, 23 Singapore (2012)
Bednarenko, M.: Classification systems for trochaneric fractures of the femur. Kwart. Ortop. 1, 1–9 (2011)
Keaveny, T.M., Morgan, E.F., Yeh, O.C.: Bone mechanics. Standard book of biomedical engineering and design. Chapter 8 (2004)
Standard: ISO 5832-1: Implants for surgery - Metallic materials - Part 1: Wrought stainless steel
Będziński, R.: Biomechanika Inźynierska. Zagadnienia Wybrane. Oficyna Wydawnicza Politechniki Wrocławskiej (1997) (in Polish)
Szewczenko, J., Marciniak, J., Kajzer, W., Kajzer, A.: Evaluation of corrosive resistance of titanium alloys used for medical implants. Arch. Metall. Mater. 61(2), 695–700 (2016). doi:10.1515/amm-2016-0118
Acknowledgements
The work has been financed from research Project No. \(BK-262/RIB2/2014\).
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2017 Springer International Publishing AG
About this paper
Cite this paper
Kajzer, W. et al. (2017). Application of Dynamic Hip Screw System in Treatment of Intertrochanteric Fracture. In: Gzik, M., Tkacz, E., Paszenda, Z., Piętka, E. (eds) Innovations in Biomedical Engineering. Advances in Intelligent Systems and Computing, vol 526. Springer, Cham. https://doi.org/10.1007/978-3-319-47154-9_15
Download citation
DOI: https://doi.org/10.1007/978-3-319-47154-9_15
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-47153-2
Online ISBN: 978-3-319-47154-9
eBook Packages: EngineeringEngineering (R0)