
Abstract
Glaucoma is one of the main causes of blindness in the world. Until it reaches an advanced stage, Glaucoma is asymptomatic, and an early diagnosis improves the quality of life of patients developing this illness.
In this paper we put forward an algorithmic solution for the diagnosis of Glaucoma. We approach the problem through a hybrid model of fuzzy and soft set based decision making techniques. Automated combination and analysis of information from structural and functional diagnostic techniques are used in order to obtain an enhanced Glaucoma detection in the clinic.
Access provided by Autonomous University of Puebla. Download conference paper PDF
Similar content being viewed by others


Keywords
1 Introduction
In this paper we take advantage of the theory of soft sets and fuzzy sets in order to design a procedure to diagnose Glaucoma risk.
Imprecise or uncertain data require the use of mathematical principles designed to capture these characteristics. The most successful approach in this regard is fuzzy set theory, which allows partial membership. In this position a property can be gradually verified and it can define sets in a non-traditional way. Fuzzy sets have been applied to many branches of science and technology since Zadeh’s seminal paper [42].
In a different vein, the theory of soft sets was initiated by Molodtsov [22]. Not only did he provide fundamental results, but he also proved that soft set theory was applicable to many fields. In particular, Molodtsov showed that soft set models encompass the fuzzy sets models.Footnote 1 Other references worth mentioning are Maji et al. [21], Aktaş and Çağman [1] and Maji, Biswas and Roy [19]. In the case of incomplete information, standard references that propose decision making criteria include Han et al. [15], Qin et al. [26] and Zou and Xiao [44].Footnote 2
The aim of this paper is to provide an application of fuzzy and soft set theory in ophthalmology which continues the research conducted by Hernández Galilea et al. [17]. Data from clinical examinations, standard perimetry and analysis of the nerve fibers of the retina with scanning laser polarimetry (NFAII;GDx) are combined to design an expert system that can be of avail to diagnose Glaucoma.
1.1 Glaucoma Diagnosis
Glaucoma is responsible for 20 % of blindness in Europe. It represents a public health problem all over the world (cf., [10]). It is an asymptomatic disease and early diagnosis represents an important objective. Glaucoma is an optic neuropathy characterized by progressive loss of retinal ganglion cells and by changes in the optic nerve head. It is associated with visual field loss. There are various risk factors of Glaucoma, the most important being intraocular pressure (IOP). Older patients who have a larger cup-disc ratio, greater elevation of IOP, or thinner corneas appear to be more likely to develop Glaucoma [13]. Pressure-independent factors that may predict the onset of Glaucoma or ocular hypertension may include genetic predisposition, altered optic-nerve microcirculation, systemic hypotension, race, or myopia (cf., [14]).
A number of studies show that structural and functional techniques often identify Glaucoma patients when Glaucoma severity is not too advanced (v. [5, 43]). A combination of both techniques can improve Glaucoma detection (v. [28, 34]).
The functional studies performed today in clinical practice with conventional computerized perimetry (static, threshold, white stimulus on white background), do not appear to be optimal and sensitive to detect early functional damage in many individuals. A significant number of patients with ocular hypertense and suspect of Glaucoma with normal standard visual fields present deficits of the visual function in other tests [31].
The single most effective method of Glaucoma diagnosis is direct examination of the optic nerve fibers, although essential in the diagnosis of Glaucoma, it is a non sensitive technique. In addition, normal eyes may have an optic nerve indistinguishable from incipient Glaucomatous eyes. The structural changes in the fiber layer of the retina and neuroretinal ring of the optic disk may occur before a deficit is determined in the visual field. Damage in the retinal nerve fibers layer (RNFL) or in the optic disk allows the identification of Glaucoma in the most incipient phase of clinical evolution even in absence of any kind of deficit in the visual field (cf., [39]).
The most universally accepted criterion to establish a definitive diagnosis of Glaucoma has usually been the loss of the visual field. Now it is commonly accepted that a significant loss of optic nerve fibers is needed to document the visual field loss (cf., [31]).
In optic neuropathy of Glaucoma a progressive loss of retinal ganglion cells occurs which brings about a decrease of RNFL thickness. Decrease of fibers can begin even five years before functional damage on the perimetry can be detected. Functional and structural damage in Glaucoma is present and the measurements of changes in the optic nerve could be correlated with damage observed in the visual field. The availability of devices that allow the analysis of fibers thickness of the layer is crucial [23, 37].
Glaucomatous structural injury progresses and develops changes in the contour of the optic nerve. Different methods have been used to document the status of the optic nerve and RNFL [29, 38].
At present commercial versions of optical imaging techniques that discriminate between healthy eyes and eyes with glaucomatous visual field loss are available: scanning laser polarimetry with variable corneal compensation (GDx VCC), confocal scanning laser ophthalmoscopy (HRT II, Heidelberg Retina Tomograph), and optical coherence tomography (Cirrus OCT). The sensitivities at high specificities were similar among the best parameters provided by each instrument.

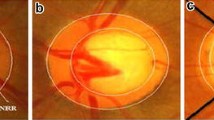
Analysis with laser polarimetry for the measurement of the RNFL thickness using the NFA-II, GDX fibers analyzer (patients with normal and terminal Glaucoma).
In order to classify the eyes in glaucomatous and non-glaucomatous eyes, besides studying IOP (Goldmann tonometry) and the ophthalmoscopic study of the optic disc by biometry using Volk aspheric lens [27], Dicon TKS 4000 autoperimetry is used for the analysis of the visual field, and the laser polarimetry for the measurement of the RNFL thickness using the NFA-II, GDX fiber analyzer (Fig. 1).
A classification was separately performed for each eye of each patient. According to [7], these groups present different stages: 0 (normal eye), 1 (ocular hypertension), 2 (early Glaucoma), 3 (established Glaucoma), 4 (advanced Glaucoma), and 5 (terminal Glaucoma). Based on these stages, a non-glaucomatous eye corresponds to normal eye or ocular hypertension stages. A glaucomatous eye corresponds to an early Glaucoma stage or higher.
1.2 Contribution and Organization of the Paper
According to the discussion above we use source data from five characteristics of the patients: age, IOP, cup-to-disc ratio, the mean of all the values of the visual field in four quadrants (the superior nasal, superior temporal, inferior nasal and inferior temporal), and an experimental number extracted from all the values obtained by an image (employing NFA-II, GDX). Through recourse to suitable fuzzifications of the raw data, soft sets are suitably associated in a way that permits to devise soft rules. On these grounds we produce a prediction system according to which the risk of Glaucoma can be assessed.
Our approach is inspired by earlier applications of soft computing techniques in diagnosis. Yuksel et al. [41] apply soft set theory to diagnose prostate cancer risk. Slowiński [35] contributes to the application of rough sets to the analysis of an information system containing 122 patients (described by 12 attributes) with duodenal ulcer treated by highly selective vagotomy. Our approach differs from the method used by Yuksel et al. [41] in different respects. We introduce validation, which is missing in [41], and use our set of data in order to estimate the predictive power of our proposal. As to methodology, we avoid some technically controversial steps in the algorithm suggested by [41].
This paper is organized as follows. Section 2 recalls some terminology and definitions. Section 3 contains a review of the solution proposed by Yuksel et al. [41] as well as our own proposal. Finally, our conclusions are presented in Sect. 4.
2 Definition of Fuzzy Set and Soft Set
A fuzzy subset A of a set S is a function \(\mu _A: S\rightarrow [0,1]\) where \(\mu _A(x)\) is called the degree of membership of x in A. Henceforth FS(S) denotes the fuzzy subsets (FSs) of the set S. We can embed \(\mathcal {P}(S)\), the set of all subsets of S, into FS(S) through the standard identification of \(A\subseteq S\) with its characteristic function \(\chi _A\).
The usual description and terminology for soft sets refers to a universe of objects U and a universal set of parameters E. The fundamental reference for soft set based decision making draws on Maji, Biswas and Roy [20]. The main concept we use is the following:
Definition 1
(Molodtsov [22]). A pair (F, A) is a soft set over U when \(A\subseteq E\) and \( F: A \longrightarrow \mathcal{P}(U). \)
A soft set over U is regarded as a parameterized family of subsets of the universe U, the set A being the parameters. For each parameter \(e\in A\), F(e) is the subset of U approximated by e, that is, the set of e-approximate elements of the soft set. This concept has been investigated e.g., by Maji, Bismas and Roy [21] and by Feng and Li [12]. While [21] define concepts like soft subsets and supersets, soft equalities, intersections and unions of soft sets, et cetera, [12] give an extensive study of several types of soft subsets and soft equal relations.
In applications both U and A are usually finite, thus soft sets can be represented either by matrices or in tabular form (cf., Yao [40]). All cells are either 0 or 1. Rows are attached with objects in U, and columns are attached with parameters in A. It is also customary to give an abbreviated representation as shown in Example 1 below:
Example 1
Let \(U = \{u_1, ... ,u_5\}\) and \(A = E = \{e_1, e_2, e_3, e_4\}\). A soft set (F, A) over U can be described as \(F(e_1)=\{u_1, u_4\}\), \(F(e_2)=\{u_3\}\), \(F(e_3)=\varnothing \), and \(F(e_4)=\{u_1, u_2, u_5\}\); or also in tabular or matrix form (see Table 1).
In order to design adequate soft rules for our expert system we make use of the following notion:
Definition 2
(Maji et al. [21]). Let (F, A) and (G, B) be two soft sets. Then (F, A) AND (G, B), henceforth denoted by \((F,A)\wedge (G,B)\), is defined as \((H,A \times B)\) where \(H(a,b) = F(a) \cap G(b)\) for each \((a,b)\in A\times B\).
3 The Problem: Antecedents and a New Proposal
3.1 Antecedents
In this section we explore the problem of applying soft sets in decision making practice in medicine. Several AI techniques have been suggested as tools for the interpretation of automated visual field test results in patients with Glaucoma [18, 33]. Using the optic disc topography parameters of the Heidelberg Retina Tomograph, neural network techniques can improve differentiation between glaucomatous and non-glaucomatous eyes [16, 24, 33]. Other types of machine learning classifiers, such as support vector machines, have also been reported to interpret visual fields adequately [4, 6, 14].
We can cite many antecedents of the use of soft computing techniques in medicine. Slowiński [35] applied rough sets in the analysis of duodenal ulcer to provide assessment in the treatment of new duodenal ulcer patients by HSV. This is in continuation of earlier applications of rough sets to this medical issue by Pawlak et al. [25]. Stefanowski and Slowiński [36] discuss problems connected with applications of rough set theory to identify the most important attributes and connected with induction of decision rules from the medical data set. [36] show that the causal relevancy of particular pre-therapy attributes can be determined by specifying the accuracy with which patients are assigned to particular recovery classes. Sanchez [32] pioneered the use of fuzzy techniques in medical diagnosis, an approach later extended by e.g., De et al. [11] to the setting of intuitionistic fuzzy sets; Saikia et al. [30] to the setting of intuitionistic fuzzy soft sets; and Chetia and Das [9] to the setting of interval-valued fuzzy soft sets, etc. Our main inspiration is Yuksel et al. [41], who use soft set theory to diagnose prostate cancer risk. Nevertheless, we can cite related uses of even fuzzy soft set theory in medical diagnosis (cf., Çelik and Yamak [8]).
3.2 Proposal of a New Soft Expert System for Glaucoma Diagnosis
We use a set of available data on five variables: (1) age; (2) intraocular pressure (IOP, expressed in millimeters of mercury); (3) cup-to-disc ratio (abbr. CDR, results were assigned as following: 0 for less than 0.4; 1 between 0.4–0.5; 2 between 0.5–0.6; 3 between 0.7–0.9); (4) visual field mean (abbr. VFM, mean of all the values of the visual field in superior nasal, superior temporal, inferior nasal, and inferior temporal quadrants); and (5) polarimetry nerve fiber (abbr. PNF, experimental number extracted from all the values on acquiring an image employing NFA-II, GDX).
Diagnosis of Glaucoma is known for all patients and corresponds to a total of 106 eyes. 53 eyes were randomly selected among the total set of available data in order to configure our expert system. The remaining eyes were used for validation purposes. In this section we proceed to explain the crucial part of the test, which is our algorithm for diagnosis.
Following the suggestion in [41], we first transform these data into fuzzy sets. Afterwards, by taking advantage of the standard inclusion of fuzzy sets into soft sets (cf., Molodtsov [22]), these fuzzy sets are transformed into suitable soft sets. Contrary to the spirit of [41] we do not invoke any parameter reduction of these soft sets, for which we find neither justification nor need. The crucial step is the construction of soft rules, which are subsequently analyzed in order to assess the Glaucoma risk. For this purpose each of the obtained rules yields a percentage.
Thus, for the diagnosis of Glaucoma we advance the following algorithm and give illustrative examples for each phase.
Algorithm - Setting up the Expert System
-
Step 1. Fuzzyfication of our data set with five variables (except for the CDR variable).
-
Step 2. The fuzzy sets corresponding to our data are transformed into soft sets via standard identification.
-
Step 3. The soft rules associated with our expert system are defined by the application of the AND operator (Definition 2) to the soft sets obtained above. 15, 552 rules were obtained. We observe which patients satisfy each rule.
-
Step 4. We calculate the Glaucoma risk percentage for each given particular soft rule as follows: the set of patients for this rule is determined in Step 3. The number of patients with Glaucoma in this set is compared with the total number of patients associated with this rule.
Algorithm - Application for Diagnosis. Based on the five parameters of a newly arrived patient suspected of suffering from Glaucoma, the risk of actually presenting Glaucoma is calculated as the maximum of the risks of all the rules that the patient verifies (Step 4).
This is a detailed description of these steps illustrated with examples from our data set.
Description of Step 1. In order to fuzzyficate our input data set we use several membership functions for each variable described in medical literature (Fig. 2).

Membership functions for our input variables.
The following linguistic variables are used: (1) for age: Y (young), M (medium), and O (old); (2) for IOP: N (normal), H (high), and VH (very high hypertension); (3) for CDR: N (normal), S (slight), M (moderate), and H (high excavation); (4) for VFM: H (high), M (medium), L (low), and N (normal deficit); and (5) for PNF: N (normal), L (limit), and A (altered number of fibers).
Considering the width of the intervals associated to each linguistic variable that the literature provides us, we define trapezoidal or triangular membership functions. Although final results achieved were similar, sigmoid functions were used in some cases.
In the case of the cup-to-disc ratio variable, the first two steps of fuzzification/defuzzification are omitted since the possible values for this variable are 0, 1, 2 and 3. Thus, initial values of the CDR variable are maintained.
As an illustration we show the membership degrees of the following sample of input variables, where superindexes indicate the number of the variable:
Description of Step 2. In order to apply techniques from soft set theory, we resort to Molodtsov’s procedure of transformation of fuzzy sets into soft sets.
We must be aware that Molodtsov’s procedure considers soft sets on the universe [0, 1]. In order to conduct a practical study we need to select a subset of this infinite parameter set. The analysis of each membership function obtained in Step 1 suggests this selected set of parameters. Since the number of patients is limited, the parameter set must consist of a small number of elements (2 or 3).
In each of the newly defined soft sets, the universe of objects U coincides with the set of patients for whom data are employed. Hence, for example (\(u_1\) is 97 years old, \(u_{35}\) is 72 y.o., and \(u_{24}\) is 67 y.o.): associated with the fuzzy set \(\mathrm {AGE}(\mathrm {O})\), \(A_{\mathrm {AGE}(\mathrm {O})}=\{0.16, 0.49, 0.83 \}\) is a pertinent parameter set; the soft set corresponding to \(\mathrm {AGE}(\mathrm {O})\) and \(A_{\mathrm {AGE}(\mathrm {O})}\) is \(F: A_{\mathrm {AGE}(\mathrm {O})} \longrightarrow \mathcal{P}(U) \), where \(F(e_1) =\{ u_1, u_{10}, u_{21}, u_{24}, u_{28}, u_{30}, u_{35}, u_{40}, u_{41}, u_{45}, u_{47} \}\), \(F(e_2) =\{ u_1, u_{10}, u_{28}, u_{30}, u_{35}, u_{40}, u_{45}, u_{47} \}\), \(F(e_3) =\{ u_1, u_{10}, u_{28}, u_{30}, u_{40}, u_{47} \}\). In this example, an element x of \(F(e_1)\) (resp. \(e_2\) and \(e_3\)) is an element \(x\in U\) such that \(\mathrm {AGE}(\mathrm {O})(x) \ge 0.16\) (resp. 0.49 and 0.83).
Description of Step 3. All the feasible soft rules are obtained by combining the soft sets in Step 2 through the AND operator. In this way, a total of 15, 552 rules are obtained for which we determine the patients who verify them. For example:
Description of Step 4. The output of Step 3 allows us to associate each rule with a risk of Glaucoma as follows. For each of these rules, the ratio of patients with Glaucoma within the total of patients who verify each rule is computed. For example, the rule described by (1) presents a Glaucoma risk of \(100\,\% \) because 3 out of the 3 patients listed suffer, in fact, from Glaucoma.
3.3 Testing the Performance of the Algorithm
The implementation of the model has been carried out by means of the scientific computation platform R2014a Matlab, using the toolbox of Fuzzy Logic.
The performance of classification of the designed model was validated with the remainder of the data of the other \(50\,\%\) of the patients of the database. A correct classification of each eye in the diagnosis of Glaucoma (glaucomatous versus non-glaucomatous patient) has been achieved with an accuracy of \(96.2\,\%\). Specificity and sensitivity yield 1 and 0.95, respectively. Several statistical characteristics were calculated out of 53 total patients: true positive rate (39), false positive rate (0), true negative rate (12), false negative rate (2), precision (1), and F1-score (0.97).
4 Final Comments and Conclusion
Glaucoma constitutes a pathology of multifactorial etiology. Precocious diagnoses entail therapeutic actions which in a fundamental way affect the prognosis of the illness. Despite the increase of specificity and sensitivity of the diagnostic tests which are applied to detect Glaucoma, none stands alone a diagnostic criterion. Clinical judgment by an expert evaluator in Glaucoma remains the primary element for diagnosis.
In the present paper, an analysis of 106 eyes (including normal and glaucomatous patients in diverse stages) is used to develop an expert system. The expert system inputs 5 variables (age, intraocular pressure, cup-to-disc ratio, visual field mean, and polarimetry nerve fiber number) and outputs the diagnosis. The risk model is set up with half the data and contrasted with the diagnoses by a Glaucoma expert ophthalmologist. The performance of classification of the designed model is validated by the remaining data from our database. A correct classification of each eye has been achieved with an accuracy of \(96.2\,\%\). Specificity and sensitivity were 1 and 0.95, respectively. Hence, this method provides an efficient and accurate tool for the diagnosis of Glaucoma by means of soft computing techniques.
We contribute the inclusion of fuzzy soft sets in the diverse systems of clinical examination, standard perimetry, and analysis of the nerve fibers of the retina with scanning laser polarimetry (NFAII;GDx). Our proposal provides a new criterion for soft set based decision making that aims at facilitating the adequate diagnosis in a rapid and automated way.
References
Aktaş, H., Çağman, N.: Soft sets and soft groups. Inf. Sci. 177, 2726–2735 (2007)
Alcantud, J.C.R.: Some fundamental relationships among soft sets, fuzzy sets, and their extensions. Mimeo (2015)
Alcantud, J.C.R., Santos-García, G.: A new criterion for soft set based decision making problems under incomplete information. Mimeo (2015)
Bowd, C., Hao, J., Tavares, I.M., Medeiros, F.A., Zangwill, L.M., Lee, T.W., Sample, P.A., Weinreb, R.N., Goldbaum, M.H.: Bayesian machine learning classifiers for combining structural and functional measurements to classify healthy and glaucomatous eyes. Invest. Ophthalmol. Vis. Sci. 49(3), 945–953 (2008)
Bowd, C., Zangwill, L.M., Berry, C.C., Blumenthal, E.Z., Vasile, C., Sánchez-Galeana, C., Bosworth, C.F., Sample, P.A., Weinreb, R.N.: Detecting early Glaucoma by assessment of retinal nerve fiber layer thickness and visual function. Invest. Ophthalmol. Vis. Sci. 42(9), 1993–2003 (2001)
Burgansky-Eliash, Z., Wollstein, G., Chu, T., Ramsey, J.D., Glymour, C., Noecker, R.J., Ishikawa, H., Schuman, J.S.: Optical coherence tomography machine learning classifiers for Glaucoma detection: a preliminary study. Invest. Ophthalmol. Vis. Sci. 46(11), 4147–4152 (2005)
Caprioli, J.: Discrimination between normal and glaucomatous eyes. Invest. Ophthalmol. Vis. Sci. 33(1), 153–159 (1992)
Çelik, Y., Yamak, S.: Fuzzy soft set theory applied to medical diagnosis using fuzzy arithmetic operations. J. Inequal. Appl. 2013(1), 82 (2013)
Chetia, B., Das, P.K.: An application of interval valued fuzzy soft sets in medical diagnosis. Int. J. Contemp. Math. Sci. 38(5), 1887–1894 (2010)
Cook, C., Foster, P.: Epidemiology of Glaucoma: what’s new? Can. J. Ophthalmol. 47(3), 223–226 (2012)
De, S.K., Biswas, R., Roy, A.R.: An application of intuitionistic fuzzy sets in medical diagnosis. Fuzzy Sets Syst. 117(2), 209–213 (2001)
Feng, F., Li, Y.: Soft subsets and soft product operations. Inf. Sci. 232, 44–57 (2013)
Fingeret, M., Medeiros, F.A., Susanna, R.J., Weinreb, R.N.: Five rules to evaluate the optic disc and retinal nerve fiber layer for Glaucoma. Optometry 76(11), 661–668 (2005)
Gordon, M.O., Beiser, J.A., Brandt, J.D., Heuer, D.K., Higginbotham, E.J., Johnson, C.A., Keltner, J.L., Miller, J.P., Parrish, R.K., Wilson, M.R., Kass, M.A.: The ocular hypertension treatment study: baseline factors that predict the onset of primary open-angle Glaucoma. Arch. Ophthalmol. 120(6), 714–720 (2002). discussion 829–30
Han, B.H., Li, Y., Liu, J., Geng, S., Li, H.: Elicitation criterions for restricted intersection of two incomplete soft sets. Knowl. Based Syst. 59, 121–131 (2014)
Henson, D.B., Spenceley, S.E., Bull, D.R.: Artificial neural network analysis of noisy visual field data in Glaucoma. Artif. Intell. Med. 10(2), 99–113 (1997)
Hernández-Galilea, E., Santos-García, G., Suárez-Bárcena, I.: Identification of Glaucoma stages with artificial neural networks using retinal nerve fibre layer analysis and visual field parameters. In: Corchado, E., Corchado, J., Abraham, A. (eds.) Innovations in Hybrid Intelligent Systems. Advances in Soft Computing, vol. 44, pp. 418–424. Springer, Heidelberg (2007)
Lietman, T., Eng, J., Katz, J., Quigley, H.A.: Neural networks for visual field analysis: how do they compare with other algorithms? J. Glaucoma 8(1), 77–80 (1999)
Maji, P., Biswas, R., Roy, A.: Fuzzy soft sets. J. Fuzzy Math. 9, 589–602 (2001)
Maji, P., Biswas, R., Roy, A.: An application of soft sets in a decision making problem. Comput. Math. Appl. 44, 1077–1083 (2002)
Maji, P., Biswas, R., Roy, A.: Soft set theory. Comput. Math. Appl. 45, 555–562 (2003)
Molodtsov, D.: Soft set theory - first results. Comput. Math. Appl. 37, 19–31 (1999)
Nukada, M., Hangai, M., Mori, S., Takayama, K., Nakano, N., Morooka, S., Ikeda, H.O., Akagi, T., Nonaka, A., Yoshimura, N.: Imaging of localized retinal nerve fiber layer defects in preperimetric Glaucoma using spectral-domain optical coherence tomography. J. Glaucoma 23(3), 150–159 (2014)
Oddone, F., Centofanti, M., Iester, M., Rossetti, L., Fogagnolo, P., Michelessi, M., Capris, E., Manni, G.: Sector-based analysis with the heidelberg retinal tomograph 3 across disc sizes and Glaucoma stages. Ophthalmology 116(6), 1106–11.e3 (2009)
Pawlak, Z., Slowiński, K., Slowiński, R.: Rough classification of patients after highly selective vagotomy for duodenal ulcer. Int. J. Man Mach. Stud. 24(5), 413–433 (1986)
Qin, H., Ma, X., Herawan, T., Zain, J.M.: Data filling approach of soft sets under incomplete information. In: Nguyen, N.T., Kim, C.-G., Janiak, A. (eds.) ACIIDS 2011, Part II. LNCS, vol. 6592, pp. 302–311. Springer, Heidelberg (2011)
Quigley, H.A., Enger, C., Katz, J., Sommer, A., Scott, R., Gilbert, D.: Risk factors for the development of glaucomatous visual field loss in ocular hypertension. Arch. Ophthalmol. 112(5), 644–649 (1994)
Quigley, H.A., Cone, F.E.: Development of diagnostic and treatment strategies for Glaucoma through understanding and modification of scleral and lamina cribrosa connective tissue. Cell Tissue Res. 353(2), 231–244 (2013)
Rolle, T., Dallorto, L., Briamonte, C., Penna, R.R.: Retinal nerve fibre layer and macular thickness analysis with fourier domain optical coherence tomography in subjects with a positive family history for primary open angle Glaucoma. Br. J. Ophthalmol. 98(9), 1240–1244 (2014)
Saikia, B.K., Das, P.K., Borkakati, A.K.: An application of intuitionistic fuzzy soft sets in medical diagnosis. Bio. Sci. Res. Bull. 19(2), 121–127 (2003)
Sample, P.A., Taylor, J.D., Martinez, G.A., Lusky, M., Weinreb, R.N.: Short-wavelength color visual fields in Glaucoma suspects at risk. Am. J. Ophthalmol. 115(2), 225–233 (1993)
Sanchez, E.: Inverses of fuzzy relations: application to possibility distributions and medical diagnosis. Fuzzy Sets Syst. 2(1), 75–86 (1979)
Santos-García, G., Hernández-Galilea, E.: Using artificial neural networks to identify Glaucoma stages. In: Kubena, T. (ed.) The Mystery of Glaucoma, pp. 331–352. InTech, Rijeka (2011)
Shah, N.N., Bowd, C., Medeiros, F.A., Weinreb, R.N., Sample, P.A., Hoffmann, E.M., Zangwill, L.M.: Combining structural and functional testing for detection of Glaucoma. Ophthalmology 113(9), 1593–1602 (2006)
Slowiński, K.: Rough classification of HSV patients. In: Slowiński, R. (ed.) Intelligent Decision Support. Theory and Decision Library, pp. 77–93. Springer, The Netherlands (1992)
Stefanowski, J., Slowiński, K.: Rough set theory and rule induction techniques for discovery of attribute dependencies in medical information systems. In: Komorowski, Jan, Żytkow, Jan M. (eds.) PKDD 1997. LNCS, vol. 1263. Springer, Heidelberg (1997)
Suh, M.H., Yoo, B.W., Kim, J.Y., Choi, Y.J., Park, K.H., Kim, H.C.: Quantitative assessment of retinal nerve fiber layer defect depth using spectral-domain optical coherence tomography. Ophthalmology 121(7), 1333–1340 (2014)
Tatham, A.J., Weinreb, R.N., Zangwill, L.M., Liebmann, J.M., Girkin, C.A., Medeiros, F.A.: Estimated retinal ganglion cell counts in glaucomatous eyes with localized retinal nerve fiber layer defects. Am. J. Ophthalmol. 156(3), 578–87.e1 (2013)
Tjon-Fo-Sang, M.J., de Vries, J., Lemij, H.G.: Measurement by nerve fiber analyzer of retinal nerve fiber layer thickness in normal subjects and patients with ocular hypertension. Am. J. Ophthalmol. 122(2), 220–227 (1996)
Yao, Y.: Relational interpretations of neighbourhood operators and rough set approximation operators. Inf. Sci. 111, 239–259 (1998)
Yuksel, S., Dizman, T., Yildizdan, G., Sert, U.: Application of soft sets to diagnose the prostate cancer risk. J. Inequal. Appl. 2013(1), 229 (2013)
Zadeh, L.: Fuzzy sets. Inf. Control 8, 338–353 (1965)
Zangwill, L.M., Bowd, C., Berry, C.C., Williams, J., Blumenthal, E.Z., Sánchez-Galeana, C.A., Vasile, C., Weinreb, R.N.: Discriminating between normal and glaucomatous eyes using the Heidelberg Retina Tomograph, gdx nerve fiber analyzer, and optical coherence tomograph. Arch. Ophthalmol. 119(7), 985–993 (2001)
Zou, Y., Xiao, Z.: Data analysis approaches of soft sets under incomplete information. Knowl. Based Syst. 21(8), 941–945 (2008)
Acknowledgments
Alcantud acknowledges financial support from the Spanish Ministerio de Economía y Competitividad (Project ECO2012–31933). The research of Santos-García was partially supported by the Spanish project Strongsoft TIN2012–39391–C04–04.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2015 Springer International Publishing Switzerland
About this paper
Cite this paper
Alcantud, J.C.R., Santos-García, G., Hernández-Galilea, E. (2015). Glaucoma Diagnosis: A Soft Set Based Decision Making Procedure. In: Puerta, J., et al. Advances in Artificial Intelligence. CAEPIA 2015. Lecture Notes in Computer Science(), vol 9422. Springer, Cham. https://doi.org/10.1007/978-3-319-24598-0_5
Download citation
DOI: https://doi.org/10.1007/978-3-319-24598-0_5
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-24597-3
Online ISBN: 978-3-319-24598-0
eBook Packages: Computer ScienceComputer Science (R0)